
Evaluation of 16S rDNA Heart Tissue PCR as a Complement to Blood Cultures for the Routine Etiological Diagnosis of Infective Endocarditis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Microbiological Cultures
2.3. 16S rDNA PCR Assays
2.4. Data Analysis
2.5. Ethics
3. Results
3.1. Patient Demographics and Clinical Features
3.2. Previous Antimicrobial Therapy and Its Effect on Microbiological Results
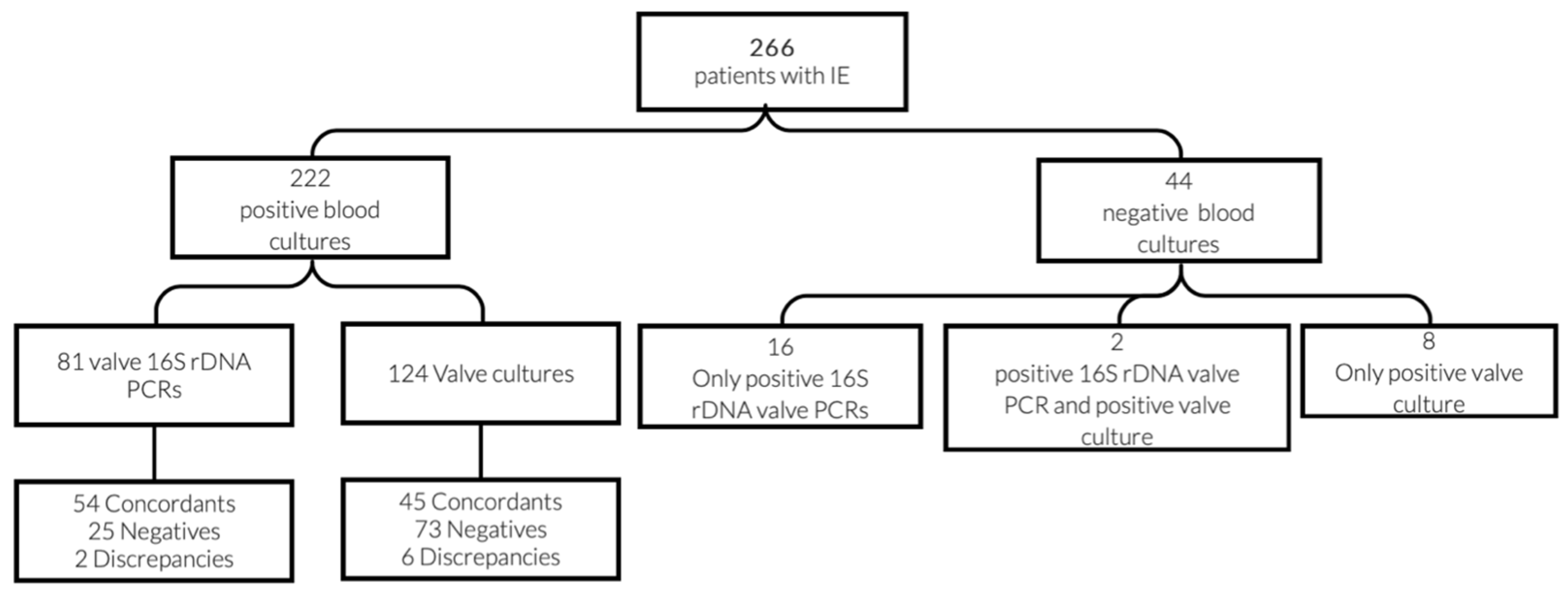
3.3. Microbiological Methods Results
3.4. Concordances and Discrepancies between the Different Evaluated Methods
3.5. Diagnostic Benefit from Valve PCR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: A prospective cohort study. Eur. Heart J. 2019, 40, 3222–3232. [Google Scholar] [CrossRef] [Green Version]
- Cahill, T.J.; Prendergast, B.D. Infective endocarditis. Lancet 2016, 387, 882–893. [Google Scholar] [CrossRef] [Green Version]
- Pettersson, G.B.; Hussain, S.T. Current AATS guidelines on surgical treatment of infective endocarditis. Ann. Cardiothorac. Surg. 2019, 8, 630–644. [Google Scholar] [CrossRef] [Green Version]
- Werner, M.; Andersson, R.; Olaison, L.; Hogevik, H.D. Swedish Society of Infectious Diseases Quality Assurance Study Group for Endocarditis. A 10-year survey of blood culture negative endocarditis in Sweden: Aminoglycoside therapy is important for survival. Scand. J. Infect. Dis. 2008, 40, 279–285. [Google Scholar] [CrossRef]
- Lamas, C.C.; Eykyn, S.J. Blood culture negative endocarditis: Analysis of 63 cases presenting over 25 years. Heart 2003, 89, 258–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fournier, P.; Thuny, F.; Richet, H.; Lepidi, H.; Casalta, J.; Arzouni, J.; Maurin, M.; Célard, M.; Mainardi, J.-L.; Caus, T.; et al. Comprehensive Diagnostic Strategy for Blood Culture–Negative Endocarditis: A Prospective Study of 819 New Cases. Clin. Infect. Dis. 2010, 51, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Fournier, P.-E.; Gouriet, F.; Casalta, J.-P.; Lepidi, H.; Chaudet, H.; Thuny, F.; Collart, F.; Habib, G.; Raoult, D. Blood culture-negative endocarditis: Improving the diagnostic yield using new diagnostic tools. Medicine 2017, 96, e8392. [Google Scholar] [CrossRef]
- Fredricks, D.N.; Relman, D. Application of Polymerase Chain Reaction to the Diagnosis of Infectious Diseases. Clin. Infect. Dis. 1999, 29, 475–486. [Google Scholar] [CrossRef]
- Church, D.L.; Cerutti, L.; Gürtler, A.; Griener, T.; Zelazny, A.; Emler, S. Performance and Application of 16S rRNA Gene Cycle Sequencing for Routine Identification of Bacteria in the Clinical Microbiology Laboratory. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef]
- Marín, M.; Muñoz, P.; Sánchez, M.; del Rosal, M.; Alcalá, L.; Rodríguez-Créixems, M.; Bouza, E. Molecular Diagnosis of Infective Endocarditis by Real-Time Broad-Range Polymerase Chain Reaction (PCR) and Sequencing Directly From Heart Valve Tissue. Medicine 2007, 86, 195–202. [Google Scholar] [CrossRef]
- Vollmer, T.; Piper, C.; Horstkotte, D.; Körfer, R.; Kleesiek, K.; Dreier, J. 23S rDNA real-time polymerase chain reaction of heart valves: A decisive tool in the diagnosis of infective endocarditis. Eur. Heart J. 2010, 31, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G., Jr.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed Modifications to the Duke Criteria for the Diagnosis of Infective Endocarditis. Clin. Infect. Dis. 2000, 30, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.idsociety.org/practice-guideline/laboratory-diagnosis-of-infectious-diseases (accessed on 28 June 2021).
- Xu, J.; Millar, B.; Moore, J.; Murphy, K.; Webb, H.; Fox, A.; Cafferkey, M.; Crowe, M. Employment of broad-range 16S rRNA PCR to detect aetiological agents of infection from clinical specimens in patients with acute meningitis—Rapid separation of 16S rRNA PCR amplicons without the need for cloning. J. Appl. Microbiol. 2003, 94, 197–206. [Google Scholar] [CrossRef]
- Vondracek, M.; Sartipy, U.; Aufwerber, E.; Julander, I.; Lindblom, D.; Westling, K. 16S rDNA sequencing of valve tissue improves microbiological diagnosis in surgically treated patients with infective endocarditis. J. Infect. 2011, 62, 472–478. [Google Scholar] [CrossRef]
- Miller, R.J.H.; Chow, B.; Pillai, D.; Church, D. Development and evaluation of a novel fast broad-range 16S ribosomal DNA PCR and sequencing assay for diagnosis of bacterial infective endocarditis: Multi-year experience in a large Canadian healthcare zone and a literature review. BMC Infect. Dis. 2016, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, P.; Bouza, E.; Marín, M.; Alcalá, L.; Créixems, M.R.; Valerio, M.; Pinto, A.; on behalf of the Group for the Management of Infective Endocarditis of the Gregorio Marañón Hospital. Heart Valves Should Not Be Routinely Cultured. J. Clin. Microbiol. 2008, 46, 2897–2901. [Google Scholar] [CrossRef] [Green Version]
- Faraji, R.; Behjati-Ardakani, M.; Moshtaghioun, S.M.; Kalantar, S.M.; Namayandeh, S.M.; Soltani, M.; Emami, M.; Zandi, H.; Firoozabadi, A.D.; Kazeminasab, M.; et al. The diagnosis of microorganism involved in infective endocarditis (IE) by polymerase chain reaction (PCR) and real-time PCR: A systematic review. Kaohsiung J. Med. Sci. 2018, 34, 71–78. [Google Scholar] [CrossRef]
- Godfrey, R.; Curtis, S.; Schilling, W.; James, P.R. Blood culture negative endocarditis in the modern era of 16S rRNA sequencing. Clin. Med. 2020, 20, 412–416. [Google Scholar] [CrossRef]
- Armstrong, C.; Kuhn, T.C.; Dufner, M.; Ehlermann, P.; Zimmermann, S.; Lichtenstern, C.; Soethoff, J.; Katus, H.A.; Leuschner, F.; Heininger, A. The diagnostic benefit of 16S rDNA PCR examination of infective endocarditis heart valves: A cohort study of 146 surgical cases confirmed by histopathology. Clin. Res. Cardiol. 2020, 110, 332–342. [Google Scholar] [CrossRef]
- Voldstedlund, M.; Pedersen, L.N.; Baandrup, U.; Klaaborg, K.E.; Fuursted, K. Broad-range PCR and sequencing in routine diagnosis of infective endocarditis. APMIS 2008, 116, 190–198. [Google Scholar] [CrossRef]
- Rovery, C.; Greub, G.; Lepidi, H.; Casalta, J.-P.; Habib, G.; Collart, F.; Raoult, D. PCR Detection of Bacteria on Cardiac Valves of Patients with Treated Bacterial Endocarditis. J. Clin. Microbiol. 2005, 43, 163–167. [Google Scholar] [CrossRef] [Green Version]
- Barnes, P.; Crook, D. Culture negative endocarditis. J. Infect. 1997, 35, 209–213. [Google Scholar] [CrossRef]
- Dolmans, R.A.V.; Boel, C.H.E.; Lacle, M.M.; Kusters, J.G. Clinical Manifestations, Treatment, and Diagnosis of Tropheryma whipplei Infections. Clin. Microbiol. Rev. 2017, 30, 529–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karageorgou, I.; Kogerakis, N.; Labropoulou, S.; Hatzianastasiou, S.; Mentis, A.; Stavridis, G.; Angelakis, E. Q Fever Endocarditis and a New Genotype of Coxiella burnetii, Greece. Emerg. Infect. Dis. 2020, 26, 2527–2529. [Google Scholar] [CrossRef] [PubMed]
- Raoult, D.; Tissot-Dupont, H.; Foucault, C.; Gouvernet, J.; Fournier, P.E.; Bernit, E.; Stein, A.; Nesri, M.; Harle, J.R.; Weiller, P.J. Q Fever 1985-1998: Clinical and Epidemiologic Features of 1,383 Infections. Medicine 2000, 79, 109–123. [Google Scholar] [CrossRef]
- Houpikian, P.; Raoult, D. Blood culture-negative endocarditis in a reference center: Etiologic diagnosis of 348 cases. Medicine 2005, 84, 162–173. [Google Scholar] [CrossRef]
- Subedi, S.; Jennings, Z.; Chen, S.-A. Laboratory Approach to the Diagnosis of Culture-Negative Infective Endocarditis. Heart Lung Circ. 2017, 26, 763–771. [Google Scholar] [CrossRef]
- Jang, Y.-R.; Song, J.S.; Jin, C.E.; Ryu, B.-H.; Park, S.Y.; Lee, S.-O.; Choi, S.-H.; Kim, Y.S.; Woo, J.H.; Song, J.-K.; et al. Molecular detection of Coxiella burnetii in heart valve tissue from patients with culture-negative infective endocarditis. Medicine 2018, 97, e11881. [Google Scholar] [CrossRef] [PubMed]
- Suardi, L.R.; de Alarcón, A.; García, M.V.; Ciezar, A.P.; Tenorio, C.H.; Martinez-Marcos, F.J.; Concejo-Martínez, E.; Lima, J.D.L.T.; García, D.V.; Márquez, R.L.; et al. Blood culture-negative infective endocarditis: A worse outcome? Results from a large multicentre retrospective Spanish cohort study. Infect. Dis. 2021, 1–9. [Google Scholar] [CrossRef]
- Oberbach, A.; Schlichting, N.; Feder, S.; Lehmann, S.; Kullnick, Y.; Buschmann, T.; Blumert, C.; Horn, F.; Neuhaus, J.; Neujahr, R.; et al. New insights into valve-related intramural and intracellular bacterial diversity in infective endocarditis. PLoS ONE 2017, 12, e0175569. [Google Scholar] [CrossRef]
- Chan, W.-S.; Au, C.-H.; Leung, H.C.-M.; Ho, D.N.; Li, D.; Chan, T.-L.; Lam, T.-W.; Ma, E.; Tang, B.S.-F. Potential utility of metagenomic sequencing for improving etiologic diagnosis of infective endocarditis. Futur. Cardiol. 2019, 15, 411–424. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, J.A.; Li, C.N.; Lamb, G.S.; Kane, D.A.; Stewart, M.K.; Mamedov, R.A.; Cookson, B.T.; Salipante, S.J. Case Report: Comparison of Plasma Metagenomics to Bacterial PCR in a Case of Prosthetic Valve Endocarditis. Front. Pediatr. 2021, 8, 575674. [Google Scholar] [CrossRef]
- Santibáñez, P.; Portillo, A.; Santibáñez, S.; García-Álvarez, L.; de Toro, M.; Oteo, J.A. What does 16S rRNA gene-targeted next generation sequencing contribute to the study of infective endocarditis in valve tissue? MedRxiv 2021. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | n (%) |
|---|---|
| Male sex | 171 (64.3) |
| Age mean ± SD (years) | 68 ± 13 |
| Medical history | |
| Native valve | 140 (52.6) |
| Prosthetic valve | 115 (43.2) |
| Intracardiac device | 18 (6.8) |
| Previous endocarditis | 20 (7.5) |
| Location | |
| Aortic | 138 (51.9) |
| Mitral | 65 (24.4) |
| Pulmonary | 2 (0.8) |
| Tricuspid | 3 (1.1) |
| Pacemaker | 15 (5.6) |
| Multiple valves | 40 (15.1) |
| Others | 3 (1.1) |
| Clinical course | |
| Surgical treatment | 154 (57.9) |
| Time of antimicrobial treatment before surgery (mean ± SD, days) | 10.3 ± 12.8 |
| Time of antimicrobial treatment after surgery (mean ± SD, days) * | 42.3 ± 19.5 |
| Time of total antimicrobial treatment (mean ± SD, days) * | 42.7 ± 22.5 |
| Deaths | 72 (27.1) |
| Number of Microorganisms Detected | ||||||||
|---|---|---|---|---|---|---|---|---|
| Bacterial Species | Number of Cases | Only Positive Blood Culture | Only Positive Heart Tissue Culture | Only Positive Heart Tissue 16S rDNA PCR | Positive Blood Culture | Positive Heart Tissue Culture | Positive Heart Tissue 16S rDNA PCR | Positive in All Methods |
| Staphylococcus aureus | 48 | 32 | 2 | 1 | 45 | 9 | 8 | 1 |
| Coagulase-negative staphylococci (CoNS) | 69 | 41 | 3 | 2 | 64 | 19 | 15 | 6 |
| Staphylococcus epidermidis | 56 | 33 | 1 | 1 | 54 | 16 | 13 | 6 |
| Staphylococcus lugdunensis | 5 | 2 | 0 | 1 | 4 | 1 | 2 | 0 |
| Staphylococcus auricularis | 2 | 1 | 1 | 0 | 1 | 1 | 0 | 0 |
| Staphylococcus hominis | 2 | 2 | 0 | 0 | 2 | 0 | 0 | 0 |
| Staphylococcus haemolyticus | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 |
| Staphylococcus warneri | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 |
| Other CoNS | 2 | 2 | 0 | 0 | 2 | 0 | 0 | 0 |
| Viridans group streptococci | 49 | 28 | 0 | 3 | 46 | 3 | 18 | 0 |
| Streptococcus mitis | 3 | 0 | 0 | 2 | 1 | 0 | 3 | 0 |
| Streptococcus mutans | 3 | 0 | 0 | 1 | 2 | 0 | 3 | 0 |
| Streptococcus anginosus | 2 | 1 | 0 | 0 | 2 | 1 | 0 | 0 |
| Streptococcus constellatus | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| Streptococcus gallolyticus | 17 | 10 | 0 | 0 | 17 | 2 | 5 | 0 |
| Streptococcus gordonii | 6 | 4 | 0 | 0 | 6 | 0 | 2 | 0 |
| Streptococcus oralis | 6 | 3 | 0 | 0 | 6 | 0 | 3 | 0 |
| Streptococcus parasanguis | 2 | 2 | 0 | 0 | 2 | 0 | 0 | 0 |
| Streptococcus salivarius | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| Streptococcus sanguinis | 6 | 4 | 0 | 0 | 6 | 0 | 2 | 0 |
| Other | 2 | 2 | 0 | 0 | 2 | 0 | 0 | 0 |
| beta-hemolytic streptococci | 5 | 2 | 0 | 1 | 4 | 1 | 2 | 0 |
| Streptococcus dysgalactiae | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 |
| Streptococcus agalactiae | 4 | 2 | 0 | 1 | 3 | 0 | 2 | 0 |
| Enterobacterales and nonfermenting Gram-negative bacilli | 8 | 3 | 0 | 2 | 6 | 2 | 3 | 0 |
| Escherichia coli | 3 | 1 | 0 | 1 | 2 | 0 | 2 | 0 |
| Enterobacter cloacae | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| Chryseobacterium spp. | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 |
| Pseudomonas aeruginosa | 2 | 1 | 0 | 0 | 2 | 1 | 0 | 0 |
| Serratia marcescens | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 |
| Enterococci | 46 | 24 | 1 | 0 | 47 | 15 | 16 | 7 |
| Enterococcus faecalis | 43 | 21 | 1 | 0 | 42 | 14 | 15 | 7 |
| Enterococcus faecium | 3 | 2 | 0 | 0 | 3 | 0 | 1 | 0 |
| Candida spp. | 2 | 1 | 0 | 0 | 2 | 1 | 0 | 0 |
| Other | 17 | 6 | 1 | 7 | 7 | 3 | 10 | 0 |
| Abiotrophia defectiva | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| Aerococcus urinae | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| Agregatibacter actinomycetemcomitans | 2 | 2 | 0 | 0 | 2 | 0 | 0 | 0 |
| Listeria monocytogenes | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| Tropheryma whipplei | 2 | 0 | 0 | 2 | 0 | 0 | 2 | 0 |
| Coxiella burnetii | 4 | 0 | 0 | 4 | 0 | 0 | 4 | 0 |
| Cutibacterium acnes | 4 | 0 | 1 | 0 | 1 | 3 | 3 | 0 |
| Bartonella henselae | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 |
| Streptococcus pneumoniae | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| Polymicrobial infection | 4 | 0 | 1 | 0 | 3 | 3 | 2 | 0 |
| Blood Cultures | Heart Valve or Vegetation Cultures | 16S rDNA Heart Valves PCR |
| Discrepancies between blood cultures and 16S rDNA heart valve PCR | ||
| Candida albicans | Candida albicans | Streptococcus dysgalactiae |
| Granulicatella adiacens | Negative | Staphylococcus epidermidis |
| Discrepancies between heart valve or vegetation cultures and the others | ||
| Streptococcus oralis | Cutibacterium acnes | Streptococcus oralis |
| Staphylococcus warneri | Staphylococcus warneri and Cutibacterium acnes | Negative |
| Streptococcus dysgalactiae | Streptococcus dysgalactiae and Staphylococcus aureus | Not performed |
| Agregatibacter actinomycetemcomitans | Klebsiella pneumoniae | Not performed |
| Enterococcus faecalis | Staphylococcus cohnii | Enterococcus faecalis |
| Staphylococcus aureus | Cutibacterium acnes | Negative |
| Streptococcus mutans | Staphylococcus haemolyticus | Streptococcus mutans |
| Blood Cultures | Heart Valve or Vegetation Cultures | 16S rDNA Heart Valves PCR | Number of Cases |
|---|---|---|---|
| Patients with only positive valve PCR | |||
| Negative | Negative | Coxiella burnetii | 4 |
| Negative | Negative | Tropheryma whipplei | 2 |
| Negative | Negative | Streptococcus mitis | 2 |
| Negative | Negative | Staphylococcus aureus | 1 |
| Negative | Negative | Staphylococcus epidermidis | 1 |
| Negative | Negative | Escherichia coli | 1 |
| Negative | Negative | Staphylococcus lugdunensis | 1 |
| Negative | Negative | Streptococcus agalactiae | 1 |
| Negative | Negative | Bartonella henselae | 1 |
| Negative | Negative | Streptococcus mutans | 1 |
| Negative | Negative | Chyseobacterium spp. | 1 |
| Patients with coagulase-negative staphylococci and skin commensals in blood cultures that are confirmed by concordant valve PCR | |||
| Staphylococcus epidermidis | Staphylococcus epidermidis | Staphylococcus epidermidis | 6 |
| Staphylococcus epidermidis | Negative | Staphylococcus epidermidis | 6 |
| Staphylococcus lugdunensis | Negative | Staphylococcus lugdunensis | 1 |
| Negative | Cutibacterium acnes | Cutibacterium acnes | 2 |
| Cutibacterium acnes | Negative | Cutibacterium acnes | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-García, R.; Rodríguez-Esteban, M.Á.; Fernández-Suárez, J.; Morilla, A.; García-Carús, E.; Telenti, M.; Morales, C.; Albaiceta, G.M.; Fernández, J. Evaluation of 16S rDNA Heart Tissue PCR as a Complement to Blood Cultures for the Routine Etiological Diagnosis of Infective Endocarditis. Diagnostics 2021, 11, 1372. https://doi.org/10.3390/diagnostics11081372
Rodríguez-García R, Rodríguez-Esteban MÁ, Fernández-Suárez J, Morilla A, García-Carús E, Telenti M, Morales C, Albaiceta GM, Fernández J. Evaluation of 16S rDNA Heart Tissue PCR as a Complement to Blood Cultures for the Routine Etiological Diagnosis of Infective Endocarditis. Diagnostics. 2021; 11(8):1372. https://doi.org/10.3390/diagnostics11081372
Chicago/Turabian StyleRodríguez-García, Raquel, María Ángeles Rodríguez-Esteban, Jonathan Fernández-Suárez, Ana Morilla, Enrique García-Carús, Mauricio Telenti, Carlos Morales, Guillermo Muñiz Albaiceta, and Javier Fernández. 2021. "Evaluation of 16S rDNA Heart Tissue PCR as a Complement to Blood Cultures for the Routine Etiological Diagnosis of Infective Endocarditis" Diagnostics 11, no. 8: 1372. https://doi.org/10.3390/diagnostics11081372