
Comorbidity, Radiation Duration, and Pretreatment Body Muscle Mass Predict Early Treatment Failure in Taiwanese Patients with Locally Advanced Oral Cavity Squamous Cell Carcinoma after Completion of Adjuvant Concurrent Chemoradiotherapy

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
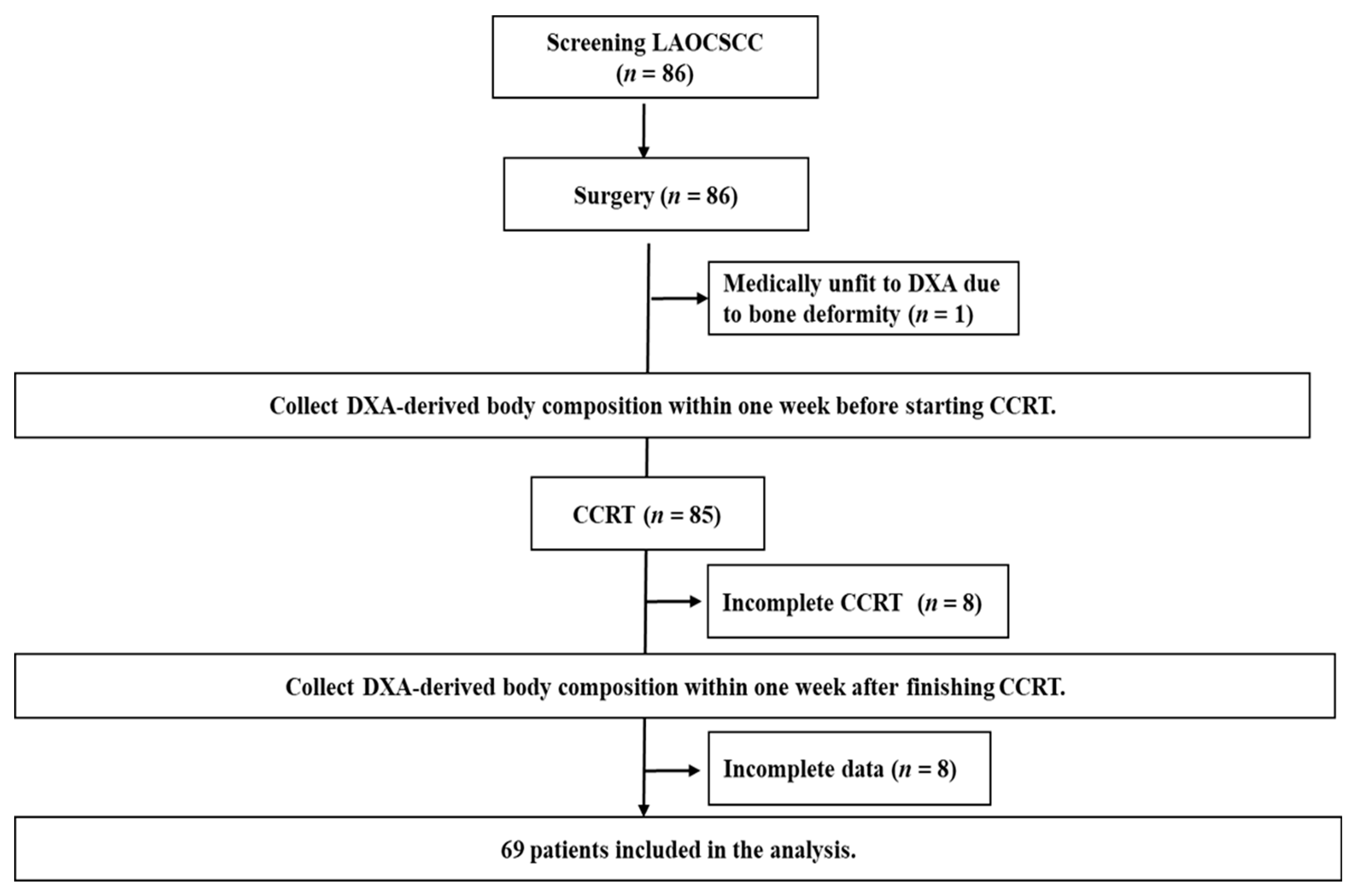
2.1. Enrollment
2.2. Treatment Schedule
2.3. Clinicopathological Data and NIMs
2.4. Body Composition Measurement
2.5. Follow-Up and Early Treatment Failure
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
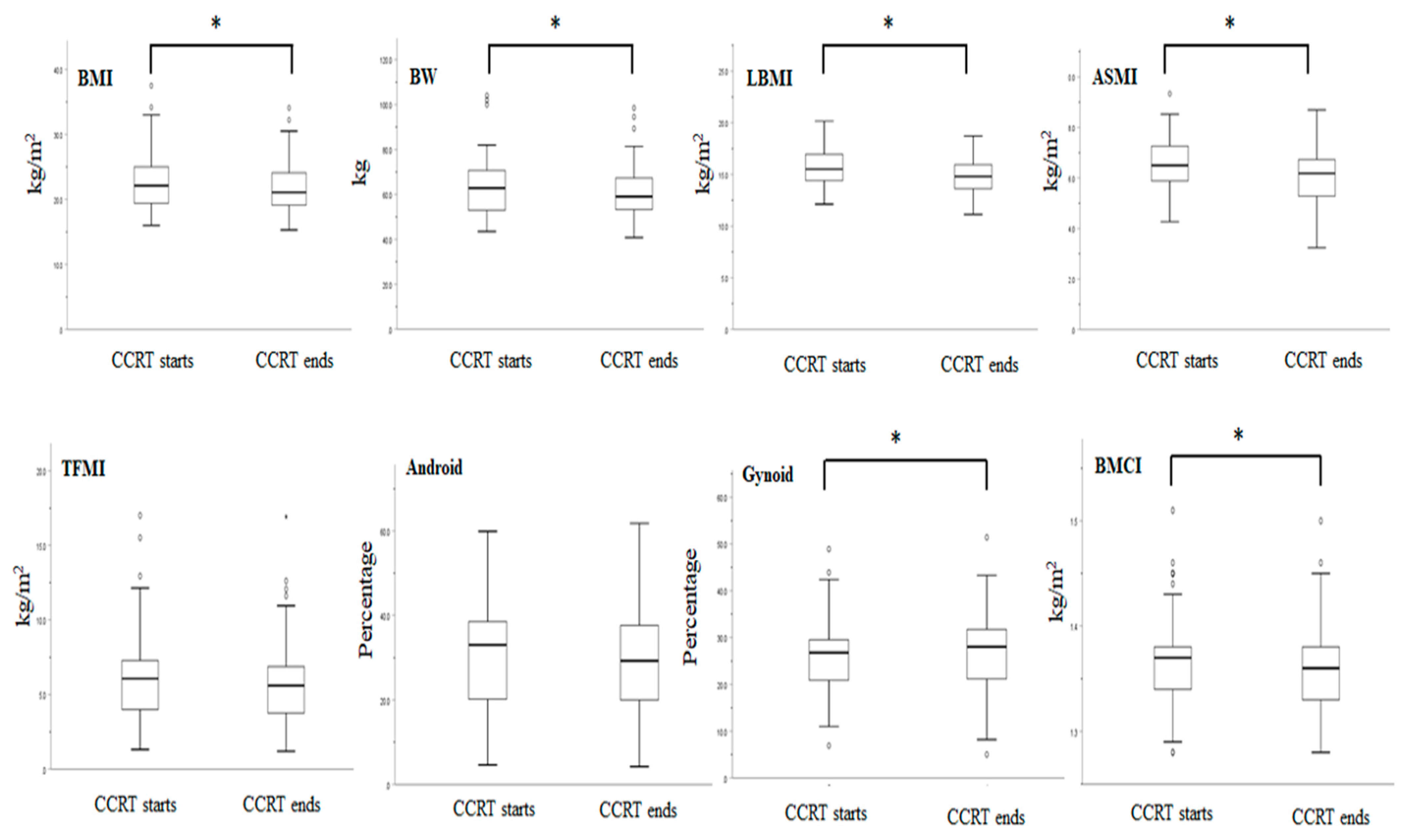
3.2. Anthropometric Data, NIMs, and DXA-Derived Parameters Before and after CCRT
3.3. Factor Analysis
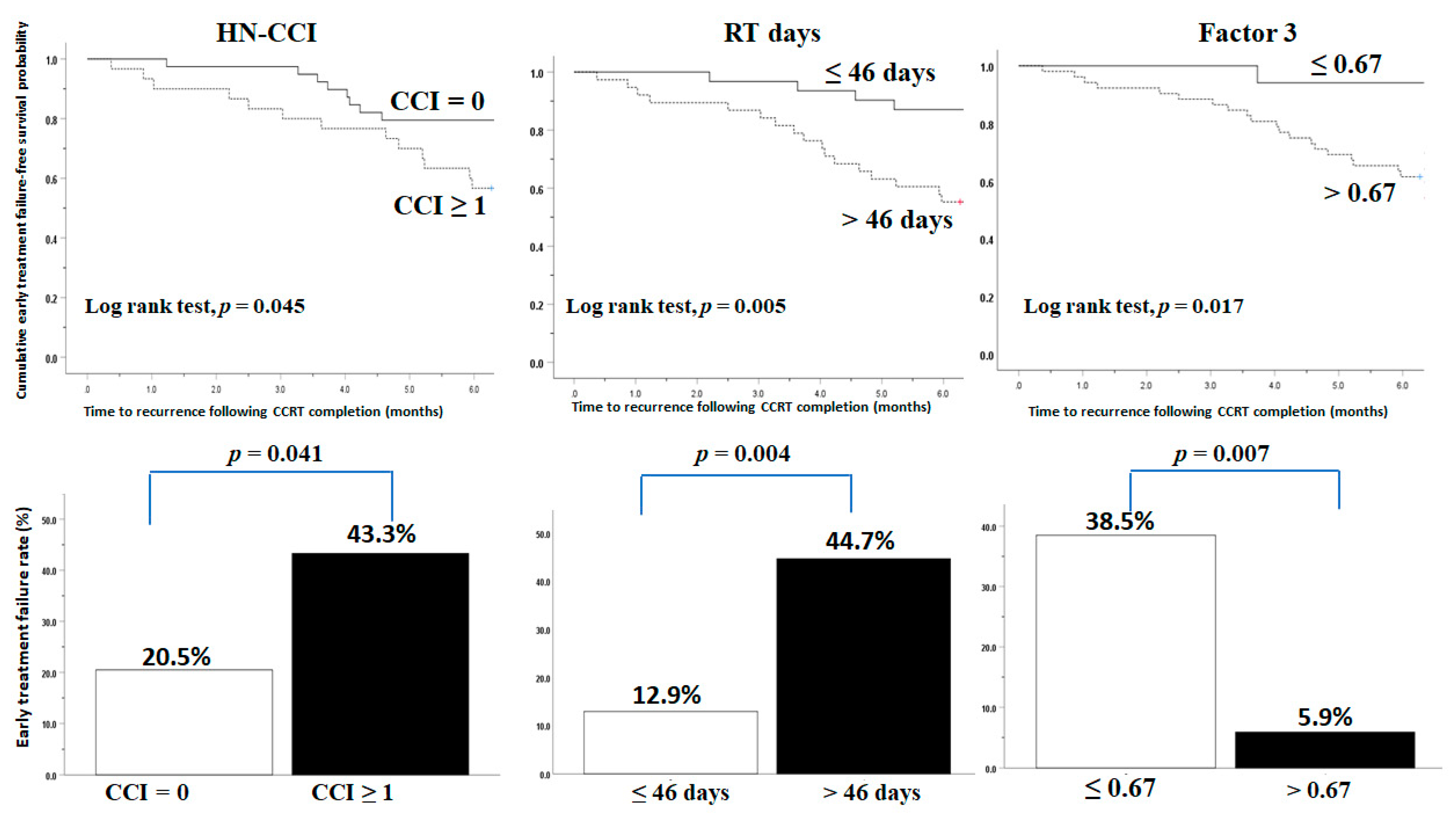
3.4. Comorbidity, Radiation Duration, and Pretreatment DXA-Derived Muscle Mass Predict Early Treatment Failure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haddad, R.I.; Shin, D.M. Recent advances in head and neck cancer. N. Engl. J. Med. 2008, 359, 1143–1154. [Google Scholar] [CrossRef] [Green Version]
- Le Tourneau, C.; Michiels, S.; Gan, H.K.; Siu, L.L. Reporting of time-to-event end points and tracking of failures in randomized trials of radiotherapy with or without any concomitant anticancer agent for locally advanced head and neck cancer. J. Clin. Oncol. 2009, 27, 5965–5971. [Google Scholar] [CrossRef] [PubMed]
- Posner, M.R. Adjuvant post-operative chemoradiotherapy in head and neck cancer: A standard of care? Oncologist 2005, 10, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Dixon, L.; Garcez, K.; Lee, L.W.; Sykes, A.; Slevin, N.; Thomson, D. Ninety Day Mortality After Radical Radiotherapy for Head and Neck Cancer. Clin. Oncol. R. Coll. Radiol. 2017, 29, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Pagh, A.; Grau, C.; Overgaard, J. Failure pattern and salvage treatment after radical treatment of head and neck cancer. Acta Oncol. 2016, 55, 625–632. [Google Scholar] [CrossRef] [Green Version]
- Capuano, G.; Grosso, A.; Gentile, P.C.; Battista, M.; Bianciardi, F.; Di Palma, A.; Pavese, I.; Satta, F.; Tosti, M.; Palladino, A.; et al. Influence of weight loss on outcomes in patients with head and neck cancer undergoing concomitant chemoradiotherapy. Head Neck 2008, 30, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.H.; Yeh, K.Y.; Huang, J.S.; Lai, C.H.; Wu, T.H.; Lan, Y.J.; Tsai, J.C.; Chen, E.Y.; Yang, S.W.; Wang, C.H. Pretreatment performance status and nutrition are associated with early mortality of locally advanced head and neck cancer patients undergoing concurrent chemoradiation. Eur. Arch. Otorhinolaryngol. 2013, 270, 1909–1915. [Google Scholar] [CrossRef] [PubMed]
- Kissun, D.; Magennis, P.; Lowe, D.; Brown, J.S.; Vaughan, E.D.; Rogers, S.N. Timing and presentation of recurrent oral and oropharyngeal squamous cell carcinoma and awareness in the outpatient clinic. Br. J. Oral. Maxillofac. Surg. 2006, 44, 371–376. [Google Scholar] [CrossRef]
- Schlumpf, M.; Fischer, C.; Naehrig, D.; Rochlitz, C.; Buess, M. Results of concurrent radio-chemotherapy for the treatment of head and neck squamous cell carcinoma in everyday clinical practice with special reference to early mortality. BMC Cancer 2013, 13, 610. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Garden, A.S.; Trotti, A.; Jones, C.U.; Carrascosa, L.; Cheng, J.D.; Spencer, S.S.; Forastiere, A.; Weber, R.S. Concomitant boost radiation plus concurrent cisplatin for advanced head and neck carcinomas: Radiation therapy oncology group phase II trial 99–14. J. Clin. Oncol. 2005, 23, 3008–3015. [Google Scholar] [CrossRef]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefebvre, J.L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef] [Green Version]
- Brizel, D.M.; Albers, M.E.; Fisher, S.R.; Scher, R.L.; Richtsmeier, W.J.; Hars, V.; George, S.L.; Huang, A.T.; Prosnitz, L.R. Hyperfractionated irradiation with or without concurrent chemotherapy for locally advanced head and neck cancer. N. Engl. J. Med. 1998, 338, 1798–1804. [Google Scholar] [CrossRef]
- Calais, G.; Alfonsi, M.; Bardet, E.; Sire, C.; Germain, T.; Bergerot, P.; Rhein, B.; Tortochaux, J.; Oudinot, P.; Bertrand, P. Randomized trial of radiation therapy versus concomitant chemotherapy and radiation therapy for advanced-stage oropharynx carcinoma. J. Natl. Cancer Inst. 1999, 91, 2081–2086. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Campbell, B.H.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Driessen, C.M.; de Boer, J.P.; Gelderblom, H.; Rasch, C.R.; de Jong, M.A.; Verbist, B.M.; Melchers, W.J.; Tesselaar, M.E.; van der Graaf, W.T.; Kaanders, J.H.; et al. Induction chemotherapy with docetaxel/cisplatin/5-fluorouracil followed by randomization to two cisplatin-based concomitant chemoradiotherapy schedules in patients with locally advanced head and neck cancer (CONDOR study) (Dutch Head and Neck Society 08-01): A randomized phase II study. Eur. J. Cancer 2016, 52, 77–84. [Google Scholar] [PubMed] [Green Version]
- Forastiere, A.A.; Goepfert, H.; Maor, M.; Pajak, T.F.; Weber, R.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.A.; Chao, C.; et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N. Engl. J. Med. 2003, 349, 2091–2098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staar, S.; Rudat, V.; Stuetzer, H.; Dietz, A.; Volling, P.; Schroeder, M.; Flentje, M.; Eckel, H.E.; Mueller, R.P. Intensified hyperfractionated accelerated radiotherapy limits the additional benefit of simultaneous chemotherapy--results of a multicentric randomized German trial in advanced head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2001, 50, 1161–1171. [Google Scholar] [CrossRef]
- Lazzari, G.; De Cillis, M.A.; Buccoliero, G.; Silvano, G. Competing Morbidities in Advanced Head and Neck Squamous Cell Carcinoma Concurrent Chemoradiotherapy: A Strong Implication of A Multidisciplinary Team Approach. Cancer Manag. Res. 2019, 11, 9771–9782. [Google Scholar] [CrossRef] [Green Version]
- Dechaphunkul, T.; Martin, L.; Alberda, C.; Olson, K.; Baracos, V.; Gramlich, L. Malnutrition assessment in patients with cancers of the head and neck: A call to action and consensus. Crit. Rev. Oncol. Hematol. 2013, 88, 459–476. [Google Scholar] [CrossRef]
- Fouladiun, M.; Korner, U.; Bosaeus, I.; Daneryd, P.; Hyltander, A.; Lundholm, K.G. Body composition and time course changes in regional distribution of fat and lean tissue in unselected cancer patients on palliative care—Correlations with food intake, metabolism, exercise capacity, and hormones. Cancer 2005, 103, 2189–2198. [Google Scholar] [CrossRef]
- Jackson, W.; Alexander, N.; Schipper, M.; Fig, L.; Feng, F.; Jolly, S. Characterization of changes in total body composition for patients with head and neck cancer undergoing chemoradiotherapy using dual-energy x-ray absorptiometry. Head Neck 2014, 36, 1356–1362. [Google Scholar] [CrossRef] [Green Version]
- Jager-Wittenaar, H.; Dijkstra, P.U.; Vissink, A.; Langendijk, J.A.; van der Laan, B.F.; Pruim, J.; Roodenburg, J.L. Changes in nutritional status and dietary intake during and after head and neck cancer treatment. Head Neck 2011, 33, 863–870. [Google Scholar] [CrossRef] [Green Version]
- Lonbro, S.; Dalgas, U.; Primdahl, H.; Johansen, J.; Nielsen, J.L.; Overgaard, J.; Overgaard, K. Lean body mass and muscle function in head and neck cancer patients and healthy individuals--results from the DAHANCA 25 study. Acta Oncol. 2013, 52, 1543–1551. [Google Scholar] [CrossRef] [Green Version]
- Silver, H.J.; Dietrich, M.S.; Murphy, B.A. Changes in body mass, energy balance, physical function, and inflammatory state in patients with locally advanced head and neck cancer treated with concurrent chemoradiation after low-dose induction chemotherapy. Head Neck 2007, 29, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.-L.; Yu, K.J.; Chiang, C.-J.; Chen, T.-C.; Wang, C.-P. Head and Neck Cancer Incidence Trends in Taiwan,1980~2014. Int. J. Head Neck Sci. 2017, 1, 180–189. [Google Scholar]
- Massano, J.; Regateiro, F.S.; Januario, G.; Ferreira, A. Oral squamous cell carcinoma: Review of prognostic and predictive factors. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2006, 102, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Vincent, N.; Dassonville, O.; Chamorey, E.; Poissonnet, G.; Pierre, C.S.; Nao, E.E.; Peyrade, F.; Benezery, K.; Viel, D.; Sudaka, A.; et al. Clinical and histological prognostic factors in locally advanced oral cavity cancers treated with primary surgery. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2012, 129, 291–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.H.; Wang, H.M.; Pang, Y.P.; Yeh, K.Y. Early nutritional support in non-metastatic stage IV oral cavity cancer patients undergoing adjuvant concurrent chemoradiotherapy: Analysis of treatment tolerance and outcome in an area endemic for betel quid chewing. Support. Care Cancer 2012, 20, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Baracos, V.; Bertz, H.; Bozzetti, F.; Calder, P.C.; Deutz, N.E.P.; Erickson, N.; Laviano, A.; Lisanti, M.P.; Lobo, D.N.; et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin. Nutr. 2017, 36, 1187–1196. [Google Scholar] [CrossRef] [Green Version]
- Boje, C.R.; Dalton, S.O.; Primdahl, H.; Kristensen, C.A.; Andersen, E.; Johansen, J.; Andersen, L.J.; Overgaard, J. Evaluation of comorbidity in 9388 head and neck cancer patients: A national cohort study from the DAHANCA database. Radiother. Oncol. 2014, 110, 91–97. [Google Scholar] [CrossRef]
- Bauer, J.; Capra, S.; Ferguson, M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur. J. Clin. Nutr. 2002, 56, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Hangartner, T.N.; Warner, S.; Braillon, P.; Jankowski, L.; Shepherd, J. The Official Positions of the International Society for Clinical Densitometry: Acquisition of dual-energy X-ray absorptiometry body composition and considerations regarding analysis and repeatability of measures. J. Clin. Densitom. 2013, 16, 520–536. [Google Scholar] [CrossRef] [PubMed]
- Moon, H.; Roh, J.L.; Lee, S.W.; Kim, S.B.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Prognostic value of nutritional and hematologic markers in head and neck squamous cell carcinoma treated by chemoradiotherapy. Radiother. Oncol. 2016, 118, 330–334. [Google Scholar] [CrossRef]
- Wong, L.Y.; Wei, W.I.; Lam, L.K.; Yuen, A.P. Salvage of recurrent head and neck squamous cell carcinoma after primary curative surgery. Head Neck 2003, 25, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.H.; Wu, C.C.; Yuan, K.S.; Wu, A.T.H.; Wu, S.Y. Locoregionally recurrent head and neck squamous cell carcinoma: Incidence, survival, prognostic factors, and treatment outcomes. Oncotarget 2017, 8, 55600–55612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janot, F.; de Raucourt, D.; Benhamou, E.; Ferron, C.; Dolivet, G.; Bensadoun, R.J.; Hamoir, M.; Gery, B.; Julieron, M.; Castaing, M.; et al. Randomized trial of postoperative reirradiation combined with chemotherapy after salvage surgery compared with salvage surgery alone in head and neck carcinoma. J. Clin. Oncol. 2008, 26, 5518–5523. [Google Scholar] [CrossRef]
- Jung, Y.H.; Song, C.M.; Park, J.H.; Kim, H.; Cha, W.; Hah, J.H.; Kwon, T.K.; Kim, K.H.; Sung, M.W. Efficacy of current regular follow-up policy after treatment for head and neck cancer: Need for individualized and obligatory follow-up strategy. Head Neck 2014, 36, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Boje, C.R.; Dalton, S.O.; Gronborg, T.K.; Primdahl, H.; Kristensen, C.A.; Andersen, E.; Johansen, J.; Andersen, L.J.; Overgaard, J. The impact of comorbidity on outcome in 12 623 Danish head and neck cancer patients: A population based study from the DAHANCA database. Acta Oncol. 2013, 52, 285–293. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.J.; Tsai, M.H.; Chiang, C.J.; Tsai, S.T.; Liu, T.W.; Lou, P.J.; Liao, C.T.; Lin, J.C.; Chang, J.T.; Tsai, M.H.; et al. Adjuvant radiotherapy after curative surgery for oral cavity squamous cell carcinoma and treatment effect of timing and duration on outcome-A Taiwan Cancer Registry national database analysis. Cancer Med. 2018, 14, 3073–3083. [Google Scholar] [CrossRef]
- Qin, L.; Chen, T.M.; Kao, Y.W.; Lin, K.C.; Yuan, K.S.; Wu, A.T.H.; Shia, B.C.; Wu, S.Y. Predicting 90-Day Mortality in Locoregionally Advanced Head and Neck Squamous Cell Carcinoma after Curative Surgery. Cancers 2018, 10, 392. [Google Scholar] [CrossRef] [Green Version]
- Shaikh, T.; Handorf, E.A.; Murphy, C.T.; Mehra, R.; Ridge, J.A.; Galloway, T.J. The Impact of Radiation Treatment Time on Survival in Patients with Head and Neck Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 967–975. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Jiang, G.L.; Fu, X.L.; Wang, L.J.; Qian, H.; Chen, G.Y.; Zhao, S.; Liu, T.F. The impact of overall treatment time on outcomes in radiation therapy for non-small cell lung cancer. Lung Cancer 2000, 28, 11–19. [Google Scholar] [CrossRef]
- Kim, J.J.; Tannock, I.F. Repopulation of cancer cells during therapy: An important cause of treatment failure. Nat. Rev. Cancer 2005, 5, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Mazul, A.L.; Stepan, K.O.; Barrett, T.F.; Thorstad, W.L.; Massa, S.; Adkins, D.R.; Daly, M.D.; Rich, J.T.; Paniello, R.C.; Pipkorn, P.; et al. Duration of radiation therapy is associated with worse survival in head and neck cancer. Oral Oncol. 2020, 108, 104819. [Google Scholar] [CrossRef]
- Sealy, M.J.; Dechaphunkul, T.; van der Schans, C.P.; Krijnen, W.; Roodenburg, J.L.N.; Walker, J.; Jager-Wittenaar, H.; Baracos, V.E. Low muscle mass is associated with early termination of chemotherapy related to toxicity in patients with head and neck cancer. Clin. Nutr. 2020, 39, 501–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Rijn-Dekker, M.I.; van den Bosch, L.; van den Hoek, J.G.; Bijl, H.P.; van Aken, E.S.M.; van der Hoorn, A.; Oosting, S.F.; Halmos, G.B.; Witjes, M.J.H.; van der Laan, H.P.; et al. Impact of sarcopenia on survival and late toxicity in head and neck cancer patients treated with radiotherapy. Radiother. Oncol. 2020, 147, 103–110. [Google Scholar] [CrossRef]
- Brown, J.C.; Schmitz, K.H. Weight lifting and appendicular skeletal muscle mass among breast cancer survivors: A randomized controlled trial. Breast Cancer Res. Treat. 2015, 151, 385–392. [Google Scholar] [CrossRef] [Green Version]
- Nishigori, T.; Okabe, H.; Tanaka, E.; Tsunoda, S.; Hisamori, S.; Sakai, Y. Sarcopenia as a predictor of pulmonary complications after esophagectomy for thoracic esophageal cancer. J. Surg. Oncol. 2016, 113, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Romanello, V.; Scalabrin, M.; Albiero, M.; Blaauw, B.; Scorrano, L.; Sandri, M. Inhibition of the Fission Machinery Mitigates OPA1 Impairment in Adult Skeletal Muscles. Cells 2019, 8, 597. [Google Scholar] [CrossRef] [Green Version]
- Kubrak, C.; Olson, K.; Jha, N.; Scrimger, R.; Parliament, M.; McCargar, L.; Koski, S.; Baracos, V.E. Clinical determinants of weight loss in patients receiving radiation and chemoirradiation for head and neck cancer: A prospective longitudinal view. Head Neck 2013, 35, 695–703. [Google Scholar] [CrossRef]
- Chang, P.H.; Wang, C.H.; Huang, J.S.; Lai, C.H.; Wu, T.H.; Lan, Y.J.; Tsai, J.C.; Chen, E.Y.; Yang, S.W.; Yeh, K.Y. Low body mass index at 3 months following adjuvant chemoradiation affects survival of postoperative locally advanced oral cavity cancer patients. Laryngoscope 2012, 122, 2193–2198. [Google Scholar] [CrossRef] [PubMed]
- Hardman, W.E. (n-3) fatty acids and cancer therapy. J. Nutr. 2004, 134, 3427S–3430S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, K.Y.; Wang, H.M.; Chang, J.W.; Huang, J.S.; Lai, C.H.; Lan, Y.J.; Wu, T.H.; Chang, P.H.; Wang, H.; Wu, C.J.; et al. Omega-3 fatty acid-, micronutrient-, and probiotic-enriched nutrition helps body weight stabilization in head and neck cancer cachexia. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2013, 116, 41–48. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Numbers (%) or Mean ± SD |
|---|---|
| Included patient number | 69 (100.0) |
| Age (years) | 53.2 ± 8.4 |
| Sex (male: female) | 69 (100.0):0 (0.0) |
| Tumor location | |
| Buccal mucosa | 20 (29.0) |
| Tongue | 28 (40.6) |
| Gingiva | 13 (18.8) |
| Mouth floor | 3 (4.3) |
| Retromolar | 2 (2.9) |
| Lip | 2 (2.9) |
| Hard palate | 1 (1.4) |
| TNM stage (III:IVA:IVB) | 4 (5.8):50 (72.5):15 (21.7) |
| Tumor size (T1:T2:T3:T4a: T4b) | 2 (2.9):6 (8.7):11 (15.9): 45 (65.3):5 (7.2) |
| Lymph node involvement (N0:N1:N2:N3) | 21 (30.5):9 (13.0):29 (42.0):10 (14.5) |
| Histological grade (1:2:3) | 8 (11.6):51 (73.9):10 (14.5) |
| Smoking (no:yes) | 6 (8.7):63 (91.3) |
| Alcohol (no:yes) | 18 (26.1):51 (73.9) |
| Betel nut (no:yes) | 16 (23.2):53 (76.8) |
| HN-CCI (0:1:2:≥3) | 29 (42.0):15 (21.7):6 (8.7):19 (27.5) |
| ECOG performance status (0:1:2) | 2 (2.9):61 (88.4):6 (8.6) |
| Tracheostomy (no:yes) | 23 (33.4):46 (66.6) |
| Adjuvant CCRT due to risk factor | |
| One major (positive surgical margin or ENE) | 42 (60.9) |
| ≥3 Minors | 27 (39.1) |
| Adjuvant CCRT | |
| Radiotherapy | |
| Dose (Gy) | 64.3 ± 3.8 |
| Fractions | 32.0 ± 1.6 |
| Duration (days) | 48.0 ± 4.9 |
| Cisplatin dose (mg/m2) | 238.5 ± 20.5 |
| PG-SGA (well:moderate:severe) | 2 (2.9):32 (46.4):35 (50.7) |
| Anthropometric and biochemical data before CCRT | |
| BW (kg) | 63.6 ± 12.6 |
| BWL (%) | 1.0 ± 6.3 |
| BMI (kg/m2) | 22.8 ± 4.3 |
| <18.5:≥18.5 | 14 (20.3):55 (79.7) |
| Hb (g/dL, normal range: 12.0–16.0) | 11.7 ± 1.5 |
| WBC (×103 cells/mm3, normal range: 6.0–11.0) | 7.3 ± 2.5 |
| Platelet count (×103/mm3, normal range: 150–450) | 341.1 ± 148.4 |
| Albumin (g/dL, normal range: 3.5–4.5) | 3.9 ± 0.5 |
| CRP (mg/dL, normal range: <5.0) | 9.3 ± 13.7 |
| DXA-related parameters | |
| LBMI (kg/m2) before CCRT | 15.7 ± 1.6 |
| TFMI (kg/m2) before CCRT | 6.1 ± 3.1 |
| ASMI (kg/m2) before CCRT | 6.6 ± 1.0 |
| Android (%) before CCRT | 29.7 ± 13.4 |
| Gynoid (%) before CCRT | 25.7 ± 8.3 |
| BMCI (kg/m2) before CCRT | 1.4 ± 0.1 |
| ∆LBMI% * | −5.68 ± 0.72 |
| ∆TFMI% * | −2.22 ± 1.97 |
| ∆ASMI% * | −5.48 ± 0.52 |
| ∆Android% * | 0.34 ± 2.59 |
| ∆Gynoid% * | 4.37 ± 1.76 |
| ∆BMCI% * | −0.23 ± 0.12 |
| Mean daily calorie intake during CCRT (kcal/kg/day) | 28.6 ± 8.6 |
| CCRT | |
| Radiotherapy | |
| Dose (Gy) | 64.3 ± 3.8 |
| Fractions | 32.0 ± 1.6 |
| Duration (days) | 49.6 ± 6.6 |
| Cisplatin dose (mg/m2) | 238.5 ± 45.5 |
| Toxicity during CCRT | |
| Non-hematologic (any grade:grade 3/4) | |
| Dermatitis | 62 (89.9):3 (4.3) |
| Pharyngitis | 24 (34.8):5 (7.2) |
| Infection | 13 (18.8):10 (14.5) |
| Mucositis | 27 (39.1):16 (23.2) |
| Emesis | 33 (47.8):6 (8.7) |
| Hematologic (any grade:grade 3/4) | |
| Anemia | (95.7):5 (7.2) |
| Neutropenia | 57 (82.6):23 (33.3) |
| Thrombocytopenia | 42 (60.9):4 (5.8) |
| Early treatment failure (%) | 21(30.4) |
| Tumor progression (%) | 15 (21.7) |
| Death by cancer (%) | 4 (5.8) |
| Death by non-cancer (%) | 2 (2.9) |
| Factors | |||||
|---|---|---|---|---|---|
| Component | 1 | 2 | 3 | 4 | 5 |
| LBMI | 0.214 | −0.120 | 0.947 | −0.038 | 0.104 |
| ASMI | 0.226 | −0.126 | 0.943 | −0.108 | −0.024 |
| TFMI | 0.926 | −0.053 | 0.313 | −0.031 | −0.008 |
| Android | 0.931 | −0.076 | 0.207 | −0.071 | −0.120 |
| Gynoid | 0.970 | −0.064 | 0.031 | −0.054 | 0.011 |
| BMCI | −0.015 | −0.062 | 0.045 | 0.094 | 0.885 |
| ∆LBMI% | −0.055 | 0.011 | −0.129 | 0.931 | −0.096 |
| ∆ASMI% | −0.085 | 0.125 | −0.006 | 0.940 | −0.001 |
| ∆TFMI% | −0.095 | 0.901 | −0.206 | 0.283 | −0.031 |
| ∆Android% | −0.153 | 0.905 | −0.104 | 0.088 | 0.136 |
| ∆Gynoid% | 0.016 | 0.918 | 0.036 | −0.173 | 0.024 |
| ∆BMCI% | 0.089 | −0.248 | −0.025 | 0.340 | −0.645 |
| Eigenvalue | 4.04 | 2.24 | 1.99 | 1.39 | 1.04 |
| % of accumulative variances | 33.7 | 52.3 | 68.9 | 80.5 | 89.2 |
| Early Treatment Failure | |||
|---|---|---|---|
| Variables, Expressed as Numbers (%) or Mean ± SD | No | Yes | p-Value |
| Patient number | 48 | 21 | |
| Clinicopathologic | |||
| Age (years) | 53.3 ± 8.7 | 53.1 ± 8.1 | 0.954 |
| Tumor location | 0.298 | ||
| Buccal mucosa | 10 (20.8) | 10 (47.6) | |
| Tongue | 20 (41.6) | 8 (38.1) | |
| Gingiva | 11 (22.9) | 2 (9.5) | |
| Mouth floor | 2 (4.2) | 1 (4.8) | |
| Retromolar | 2 (4.2 ) | 0 (0.0) | |
| Lip | 2 (4.2 ) | 0 (0.0) | |
| Hard palate | 1 (2.1) | 0 (0.0) | |
| TNM stage (III vs. IVA vs. IVB) | 2 (4.2):35 (72.9):11 (22.9) | 2 (9.5):15 (71.4):4 (19.1) | 0.661 |
| T status (T0-2 vs. T3-4) | 7 (14.6):41 (85.4) | 1 (4.8):20 (95.2) | 0.241 |
| N status (N0-1 vs. N2-3) | 21 (43.8):27 (56.3) | 9 (42.9):12 (57.1) | 0.945 |
| Histological grade (1:2:3) | 2 (4.2):35 (72.9):11 (22.9) | 2 (9.5):15 (71.4):4 (19.1) | 0.065 |
| ECOG performance status (0:1:2) | 1 (2.1):46 (95.8):1 (2.1) | 1 (4.8):15 (71.4):5 (23.8) | 0.018 * |
| Smoking (no:yes) | 4 (8.3):44 (91.7) | 2 (9.5):19 (90.5) | 0.872 |
| Alcohol (no:yes) | 15 (31.3):33 (68.7) | 3 (14.3):18 (85.7) | 0.140 |
| Betel nut (no:yes) | 13 (27.1):35 (72.9) | 3 (14.3):18 (85.7) | 0.246 |
| HN-CCI (0 vs. 1 vs. 2 vs. ≥3) | 26 (54.2):10 (20.8):5 (10.5):7 (14.5) | 7 (33.3):5 (23.8):1 (4.8):8 (38.1) | 0.042 * |
| Tracheostomy (no:yes) | 16 (33.3):32 (66.7) | 7 (33.3):14 (66.7) | 1.000 |
| Adjuvant CCRT due to risk factor | 0.514 | ||
| One major (positive surgical margin or ENE) | 28 (58.3) | 14 (66.7) | |
| ≥3 Minors | 21 (41.7) | 7 (33.3) | |
| CCRT | |||
| RT dose (Gy) | 64.0 ± 3.3 | 64.9 ± 4.8 | 0.382 |
| RT duration (days) | 47.2 ± 4.6 | 50.0 ± 5.0 | 0.026 * |
| Cisplatin dose (mg/m2) | 237.8 ± 15.8 | 240.0 ± 28.9 | 0.687 |
| CCRT-induced grade 3/4 toxicity | |||
| Dermatitis | 1 (2.1) | 2 (9.5) | 0.163 |
| Pharyngitis | 2 (4.2) | 3 (14.3) | 0.136 |
| Mucositis | 9 (18.8) | 7 (33.3) | 0.253 |
| Infection | 6(12.5) | 4 (19.0) | 0.477 |
| Emesis | 5 (10.4) | 1 (4.8) | 0.443 |
| Anemia (%) | 4 (8.3) | 1 (4.8) | 0.599 |
| Neutropenia (%) | 16 (33.3) | 7 (33.3) | 1.000 |
| Thrombocytopenia (%) | 4 (8.3) | 0 (0.0) | 0.173 |
| Mean daily calorie intake during CCRT (kcal/kg/day) | 28.1 ± 8.1 | 29.8 ± 9.9 | 0.439 |
| Nutritional and inflammatory markers before CCRT | |||
| BMI (kg/m2) | 23.3 ± 4.5 | 21.4 ± 3.3 | 0.090 |
| BWL (kg) | 1.7 ± 22.3 | 4.5 ± 15.2 | 0.276 |
| Hb (mg/dL) | 11.9 ± 1.5 | 11.2 ± 1.4 | 0.082 |
| WBC (×103 cells/mm3) | 7.1 ± 2.1 | 7.7 ± 3.4 | 0.372 |
| Platelet count (×103/mm3) | 330.4 ± 150.6 | 365.3 ± 124.4 | 0.370 |
| Albumin (g/dL) | 3.9 ± 0.5 | 3.8 ± 0.5 | 0.526 |
| CRP (mg/dL) | 8.5 ± 10.4 | 17.9 ± 22.0 | 0.017 * |
| PG-SGA (well vs. moderate vs. severe) before CCRT | 2 (4.2):23 (47.9):23 (47.9) | 0 (0.0):9 (42.9):12 (57.1) | 0.549 |
| Body composition parameters | |||
| Factor 1 | 0.037 ± 1.037 | −0.085 ± 0.935 | 0.643 |
| Factor 2 | 0.045 ± 1.030 | −1.033 ± 0.943 | 0.574 |
| Factor 3 | 0.181 ± 0.979 | −0.415 ± 0.969 | 0.021 * |
| Factor 4 | −0.089 ± 0.942 | 0.205 ± 1.116 | 0.263 |
| Factor 5 | −0.005 ± 0.885 | 0.012 ± 1.247 | 0.940 |
| Time to treatment failure (months) | 30.9 ± 13.4 | 3.5 ± 1.6 | <0.001 * |
| Variables | Early Treatment Failure | ||
|---|---|---|---|
| Univariate | Multivariate | ||
| p-Value | Hazard Ratio (95% Confidence Interval) | p-Value | |
| Clinicopathologic | |||
| Age | 0.988 | ||
| TNM stage (ref: IV) | 0.620 | ||
| T status (ref: T3-4) | 0.285 | ||
| N status (ref: N2-3) | 0.423 | ||
| ECOG performance status (ref: 2) | 0.221 | ||
| Smoking (ref: yes) | 0.845 | ||
| Alcohol (ref: yes) | 0.176 | ||
| Betel nut (ref: yes) | 0.300 | ||
| HN-CCI (ref: no) | 0.047 * | 2.699 (1.005–7.193) | 0.044 * |
| Tracheostomy (ref: yes) | 0.920 | ||
| Risk factor for CCRT (ref: minor) | 0.505 | ||
| CCRT | |||
| RT dose | 0.254 | ||
| RT duration | 0.035 * | 1.092 (1.015–1.174) | 0.018 * |
| Cisplatin dose | 0.886 | ||
| CCRT-induced grade 3/4 toxicity | |||
| Dermatitis (ref: yes) | 0.030 * | 0.236 (0.040–1.383) | 0.180 |
| Pharyngitis (ref: yes) | 0.102 | ||
| Mucositis (ref: yes) | 0.495 | ||
| Infection (ref: yes) | 0.423 | ||
| Emesis (ref: yes) | 0.418 | ||
| Anemia (ref: yes) | 0.644 | ||
| Neutropenia (ref: yes) | 0.990 | ||
| Thrombocytopenia (ref: yes) | 0.416 | ||
| Mean daily calorie intake during CCRT (kcal/kg/day) | 0.108 | ||
| Nutritional and inflammatory markers before CCRT | |||
| BMI | 0.094 | ||
| BWL | 0.315 | ||
| Hb | 0.069 | ||
| WBC | 0.681 | ||
| Platelet count | 0.408 | ||
| Albumin | 0.433 | ||
| CRP | 0.012 * | 1.018 (0.995–1.041) | 0.130 |
| PG-SGA (well vs. moderate vs. severe) before CCRT | 0.976 | ||
| Body composition parameters | |||
| Factor 1 | 0.636 | ||
| Factor 2 | 0.570 | ||
| Factor 3 | 0.008 * | 0.578 (0.345–0.957) | 0.037 * |
| Factor 4 | 0.339 | ||
| Factor 5 | 0.772 | ||
| Study | Tumor Location | CCRT Type | Radiotherapy | Chemotherapy | Characteristics and Endpoint Assessment |
|---|---|---|---|---|---|
| Cooper et al., 2004 [14] | Oral cavity, oropharynx, hypopharynx, larynx | Adjuvant CCRT | 60 Gy, 6 weeks | Cisplatin (triweekly, 100 mg/m2) | Prospective, 206 patients, early treatment failure rate (within 30 days after CCRT): 3.4% (7 patients, 4 died of treatment toxicity, 1 died of cancer), no risk factor reported |
| Bernier et al., 2004 [11] | Oral cavity, oropharynx, hypopharynx, larynx | Adjuvant CCRT | 66 Gy, 5–6 weeks | Cisplatin (triweekly, 100 mg/m2) | Prospective, 167 patients, early mortality rate: 0.6% (one patient died of sepsis), no risk factor reported |
| Chang et al., 2013 [7] | Oral cavity, oropharynx, hypopharynx | Primary CCRT or adjuvant CCRT | 60–74 Gy, 6–8 weeks | cisplatin alone, cisplatin with oral UFT (tegafur plus uracil and calcium folinate) | Retrospective, 194 patients, early mortality rate (within 60 days after CCRT): 7.2% (14 patients, 11 died of sepsis); risk factors: performance status > 1, BMI < 19 kg/m2, and blood TLC < 700/mm3 |
| This study | Oral cavity | adjuvant CCRT | 64–72 Gy, 6–8 weeks | Cisplatin (weekly, 40 mg/m2) | Prospective, 69 patients, early treatment failure rate (within 180 days after CCRT): 30.4% (21 patients, 15 with tumor progression, 4 died of cancer, 2 died of sepsis): risk factors: comorbidity, RT duration, and muscle mass before CCRT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-C.; Ling, H.H.; Chang, P.-H.; Pan, Y.-P.; Wang, C.-H.; Chou, W.-C.; Chen, F.-P.; Yeh, K.-Y. Comorbidity, Radiation Duration, and Pretreatment Body Muscle Mass Predict Early Treatment Failure in Taiwanese Patients with Locally Advanced Oral Cavity Squamous Cell Carcinoma after Completion of Adjuvant Concurrent Chemoradiotherapy. Diagnostics 2021, 11, 1203. https://doi.org/10.3390/diagnostics11071203
Lin Y-C, Ling HH, Chang P-H, Pan Y-P, Wang C-H, Chou W-C, Chen F-P, Yeh K-Y. Comorbidity, Radiation Duration, and Pretreatment Body Muscle Mass Predict Early Treatment Failure in Taiwanese Patients with Locally Advanced Oral Cavity Squamous Cell Carcinoma after Completion of Adjuvant Concurrent Chemoradiotherapy. Diagnostics. 2021; 11(7):1203. https://doi.org/10.3390/diagnostics11071203
Chicago/Turabian StyleLin, Yu-Ching, Hang Huong Ling, Pei-Hung Chang, Yi-Ping Pan, Cheng-Hsu Wang, Wen-Chi Chou, Fang-Ping Chen, and Kun-Yun Yeh. 2021. "Comorbidity, Radiation Duration, and Pretreatment Body Muscle Mass Predict Early Treatment Failure in Taiwanese Patients with Locally Advanced Oral Cavity Squamous Cell Carcinoma after Completion of Adjuvant Concurrent Chemoradiotherapy" Diagnostics 11, no. 7: 1203. https://doi.org/10.3390/diagnostics11071203