1. Introduction
Oral cancer is one of the most frequent types of cancer worldwide, accounting for approximately 380,000 new cases annually, with oral squamous cell carcinoma (OSCC) being the most common type [
1]. Despite the achieved progress in treatment modalities, OSCC is associated with significant morbidity and mortality; despite geographic variations, the 5-year overall survival rate in general remains dismal, estimated at around 50% in most studies [
2]. Therefore, there is an urgent need for improvement though primary prevention (aiming at avoidance of exposure to known risk factors, such as smoking and alcohol), as well as secondary prevention with emphasis on early detection and proper management of OSCC precursor lesions [
3].
It is generally accepted that OSCC may arise either de novo or, most often, in the context of a preceding oral potentially malignant disorder (OPMD), most commonly oral leukoplakia (OL). According to the recent recommendation by the WHO Collaborating Centre for Oral Cancer, OPMDs can be defined as “any oral mucosal abnormality that is associated with a statistically increased risk of developing oral cancer.” [
4]. OPMDs encompass a spectrum of oral mucosal diseases (e.g., OL, erythroplakia, oral lichen planus, oral submucous fibrosis etc.) with a global prevalence of 4.47%, albeit with variable rates among different types of lesions and populations, as has been estimated in a recent systematic review [
5]. Among OPMDs, OL is the most common with a worldwide prevalence of 4.11% [
5]. Several definitions of OL have been used throughout the years; according to the WHO, “Leukoplakia is a clinical term used to describe white plaques of questionable risk, once other specific conditions and other OPMDs have been ruled out” [
6]. OL may undergo malignant transformation (MT) at a rate ranging widely in various studies between 0.13–34%, with an annual progression rate of 1–3% [
7,
8,
9]. Moreover, its co-existence in about 50% of OSCC cases at the time of diagnosis supports the necessity for early diagnosis and prevention of MT of OL, especially considering the dismal prognosis of OSCC [
10,
11]. Besides MT, OL recurrences, sometimes multiple, are generally regarded as common with a 5-year incidence of almost 50% [
12]. Although it is intuitive that OL recurrences pose a significant problem, indicating persistence and suggesting tendency for progression and also raising significant management concerns, they have not been studied as thoroughly so far.
Various sociodemographic factors (older age, female gender, non-smoking), clinical characteristics (increased size, non-homogeneous appearance, high risk sites such as lateral and ventral tongue and floor of mouth), and histopathologic features (higher grades of dysplasia) have been shown to correlate with risk of progression [
13]. Additionally, special attention has been given to the potential usefulness of molecular markers in predicting oral cancer development in OPMDs [
14,
15]. However, to this date, there are still important limitations, since no single marker that could estimate the precise malignant potential of OL has been corroborated yet, urging for further studies that may shed light on the molecular nature of OL [
14,
16,
17]. This is supported by a recent systematic review [
18] of biomarkers in OL failing to generate conclusive results due to the heterogeneity of studies. Most of the aforementioned studies have correlated these features with MT, while very few studies, as noted above, have specifically focused on OL recurrence, attempting to identify parameters that could determine the risk of relapse, following removal of the initial lesions [
12,
19].
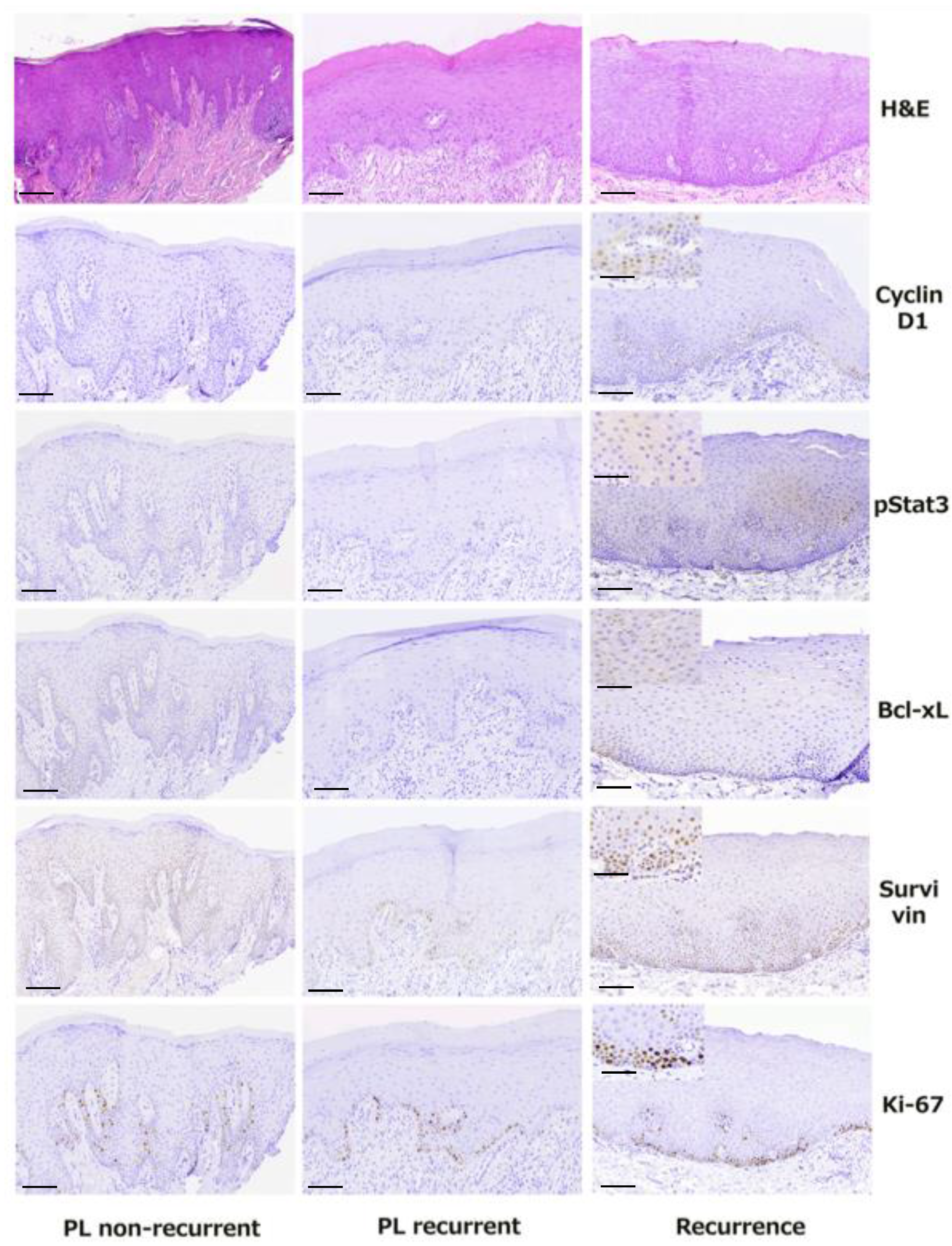
In the present study, we aimed to further investigate the phenomenon of recurrence in OL. Specifically, in a well-characterized cohort of 33 patients with one or more OL lesions, which were all subjected to excisional biopsy or incisional biopsy and laser ablation and then submitted to adequate follow-up, we first recorded all recurrences, new primary OL lesions (PLs) or OSCCs developing during follow-up. We also evaluated the demographic, clinical, and histopathologic characteristics of PLs and correlated them with their risk of recurrence after treatment. Further, we assessed the immunohistochemical (IHC) expression of selected cell cycle and apoptosis-related molecules (associated with the Stat3 oncogenic pathway, including pSTAT3, Bcl-xL, survivin, cyclin D1 and Ki-67) [
20] and correlated them with the presence and degree of epithelial dysplasia, as well as with the risk of OL recurrence. Finally, we compared the aforementioned clinical, microscopic, and IHC features between PLs and their respective recurrences observed during follow-up.
2. Materials and Methods
2.1. Patients’ Records
The clinical charts of 33 patients, managed at the Oral Medicine Clinic of the Department of Oral Medicine & Pathology and Hospital Dentistry, School of Dentistry, National and Kapodistrian University of Athens (NKUA), Greece, between January 2010 and March 2020, were reviewed. All patients had an initial clinical diagnosis of OL, which was submitted to biopsy and histopathologically confirmed as either epithelial hyperplasia or epithelial dysplasia of mild, moderate, or severe degree [
6,
21].
Inclusion criteria encompassed availability of demographic data, including age, gender, smoking habits, alcohol consumption, and complete medical history; detailed clinical information, including number, site, size and clinical appearance (homogeneous vs. heterogeneous) of lesions; biopsy (incisional or excisional) and histopathologic diagnosis with tissue availability; and close follow-up for at least 1 year.
Exclusion criteria were a previous diagnosis of head and neck SCC in the last 18 months before first visit and a history of previous chemo- or radiotherapy. White non-removable lesions consistent with frictional keratosis or other diagnoses (different than OL) were also excluded from the study.
According to our institutional regulations, this study was exempted from institutional review board approval.
2.2. Demographic Data
Data collected included epidemiologic characteristics, such as age and gender. Smoking and drinking habits were also recorded and patients were classified as either non-smokers (those who had never smoked) and ex-smokers (when a person had quit smoking at least 1 year prior to diagnosis), or as current smokers (those that are currently smoking or had stopped smoking <1 year prior to diagnosis) [
22]. Based on alcohol consumption, patients were classified as drinkers vs. non-drinkers, the latter category including never drinkers and social drinkers [
23].
2.3. Clinical Features
The available clinical parameters including number (uni- or multifocality), site and size of the lesions were recorded. Based on their clinical appearance, OL lesions were classified as homogeneous or non-homogeneous; the latter category included verrucous, speckled (erythro-leukoplakia) and nodular lesions [
6,
24]. Clinical photographs were available in all cases.
2.4. Biopsy and Histopathologic Features
All lesions included in our study had been submitted either to an excisional biopsy, when lesions were sized approximately ≤1 cm, or an incisional biopsy (size > 1 cm) with scalpel (performed under local anesthesia by an experienced clinician following similar technique). For excisional biopsies, a 3 mm margin of normal tissue was included.
Two oral and maxillofacial pathologists (N.N, A.L) re-evaluated the hematoxylin and eosin-stained (H&E) sections of all lesions for confirmation of the diagnosis. A microscopic diagnosis of epithelial hyperplasia or dysplasia of mild, moderate or severe degree was rendered according to the WHO classification [
6,
21]. For excisional biopsies, the status of the surgical margins, i.e., positive vs. negative, was also recorded.
2.5. Management
All cases removed by excisional biopsy were placed in follow-up. All cases first submitted to incisional biopsy were subsequently subjected to CO2 laser ablation with approximately 3 mm margin (beyond the clinically visible border of the residual OL in all directions). Small lesions were treated in one laser session; larger lesions needed two or more treatments.
The CO2 laser system was the Smart US20 D laser class 4 (DEKA M.E.L.A, Calenzano, Italy). The standard laser protocol, used in the Department of Oral & Maxillofacial Surgery, School of Dentistry, National and Kapodistrian University of Athens, Greece, was applied. Local anesthesia was administered peripherally to the borders of the lesion. The contour of the lesion was marked out in a pulsed mode with the laser, including an approximately 3 mm area of normal appearing mucosa peripherally to the lesion. The light ray of the laser during the sublimation was at a distance of about 1 mm, the wavelength ranged between 250–500 µm at 2–5 watts in continuous wave, and the pulse frequency was of about 100 Hz. All wounds caused by the laser were left open for secondary intention healing. All patients attended regular follow-up after treatment to evaluate the healing process.
2.6. Follow-Up
Only patients seen at regular intervals for at least 1 year were included in the study. Patients were re-examined at least every 2 months until the end of the first year and subsequently on a 3-month basis. Clinical photographs of the PLs, taken with a graduated ruler in the vicinity, were available and compared in order to facilitate recognition of a clinical recurrence.
Local recurrence was defined as an OL lesion arising in the immediate vicinity of the treated area. In these cases, clinical parameters of the new lesion (size, site, homogeneity or not) were also carefully recorded and a new biopsy (incisional or excisional, according to size, similar to PLs) was performed under local anesthesia. Following histopathologic confirmation of the diagnosis (epithelial hyperplasia or dysplasia of various degrees), laser ablation (of the recurrent lesions first submitted to incisional biopsy) was performed, as described above.
In addition to local recurrences, all new PLs (i.e., at different sites compared to the original PLs) arising during the follow-up period were also detected and recorded according to their clinical features, submitted to biopsy (incisional or excisional, according to size) and histo-pathologically evaluated and managed, following the same protocol as for the original PLs noticed at first visit.
2.7. Immunohistochemistry Experiments
From each tissue block, four-µm-thick serial formalin-fixed paraffin-embedded tissue sections of biopsy specimens were deparaffinized and placed on charged slides. The slides were incubated in xylene and then immersed in ethanol 100% and 95% and heated for antigen retrieval in 0.01 M citrate buffer (C2488, Sigma-Aldrich, St. Louis, MO, USA) for 25 min in a pressure cooker inside a microwave oven. Endogenous peroxidase activity and non-specific protein reaction were then blocked. After dehydration in hydrogen peroxide, the sections were incubated with primary antibodies at room temperature for 1 h. The applied antibodies were all rabbit monoclonal against phospho-STAT3 (pSTAT3) (Tyr705) (CST, D3A7, #9145) (1:200), survivin (CST, 71G4B7, #2808) (1:300), cyclin D1 (CST, E3P5S, #55506) (1:300), Ki-67 (CST, D2H10, #9027) (1:250), and Bcl-xL (CST, 54H6, #2764) (1:200) (Cell Signaling Technology, Leiden, The Netherlands).
The standard streptavidin-biotin-peroxidase complex method was employed to bind to the primary antibody along with mouse anti-rabbit IgG as secondary antibody (1:2000) (CST#7074, Cell Signaling Technology, Leiden, The Netherlands). Reaction products were visualized by counterstaining with the 3,3V-diaminobenzidine reagent set (Kirkegaard and Perry Laboratories, Gaithersburg, MD, USA). Sections were counterstained with hematoxylin. As a negative control, sections were treated with phosphate-buffered saline (PBS) with omission of the primary antibody. Immunostains were reviewed by three evaluators (N.N., E.P., D.V.).
To validate the staining in all samples, positive controls of tissue sections known to express the five studied proteins were used (including breast cancer for phospho-STAT3, prostate cancer for survivin and Bcl-xL, papillary carcinoma of thyroid gland for cyclin D1, and small cell carcinoma of the bladder for Ki-67).
Positive and negative controls were included in every IHC run to ensure that technical variation did not affect the results.
Some samples were not evaluated, because of progressive depletion of the representative areas of the sample material.
2.8. Evaluation of Immunohistochemical Staining
The IHC staining was evaluated by three independent evaluators (N.N., E.P., D.V.). Sections were scored as positive if the epithelial cells showed immunoreactivity in the nucleus.
The tissue sections were scored based on the percentage of positive cells in a semiquantitative manner: (0) <1%; (1) 1–25%; (2) 26–50%; (3) >50%. Sections were also scored on the basis of staining intensity as (0) no staining, (1) mild, (2) moderate, or (3) strong, compared with the positive control tissues, the intensity of which was classified as moderate. Lower intensity (light brown) compared to the brown staining of the positive control was classified as weak, while higher intensity (dark brown) compared to the positive control was classified as strong. Finally, a total score (0, 2–6) was obtained by adding the scores of percentage of cells positivity (0–3) and intensity (0–3). At least five random high-power magnification fields of view (of at least 100 total cells each) of selected areas (representative of the final diagnosis) of each specimen were analyzed independently and the average scores were calculated [
25]. In the limited number of cases that an initial disagreement among the independent evaluators was noticed, a consensus agreement was achieved by the use of a multi-observer microscope.
All images were scanned and photographed using the WSI software program (Microvisioneer, Germany) with an Olympus CX 23 microscope.
2.9. Data Comparison and Statistical Analysis
Comparative evaluation was performed as follows:
Recurrent vs. non-recurrent PLs were compared according to demographic data and patients’ habits (age, gender, smoking, and alcohol use), clinical features (site, size, homogeneity or not) and histopathologic features (epithelial hyperplasia vs. dysplasia of various degrees). For small lesions removed by surgical excisional biopsy, comparison was also made according to the histopathologic status of the surgical margins.
The IHC scores of the five molecules investigated were also compared between recurrent vs. non-recurrent primary OL lesions, as well as between lesions with different histopathologic diagnoses (epithelial hyperplasia vs. dysplasia of various degree).
For lesions developing recurrence, all the above parameters were also compared between PLs and their corresponding recurrent lesions.
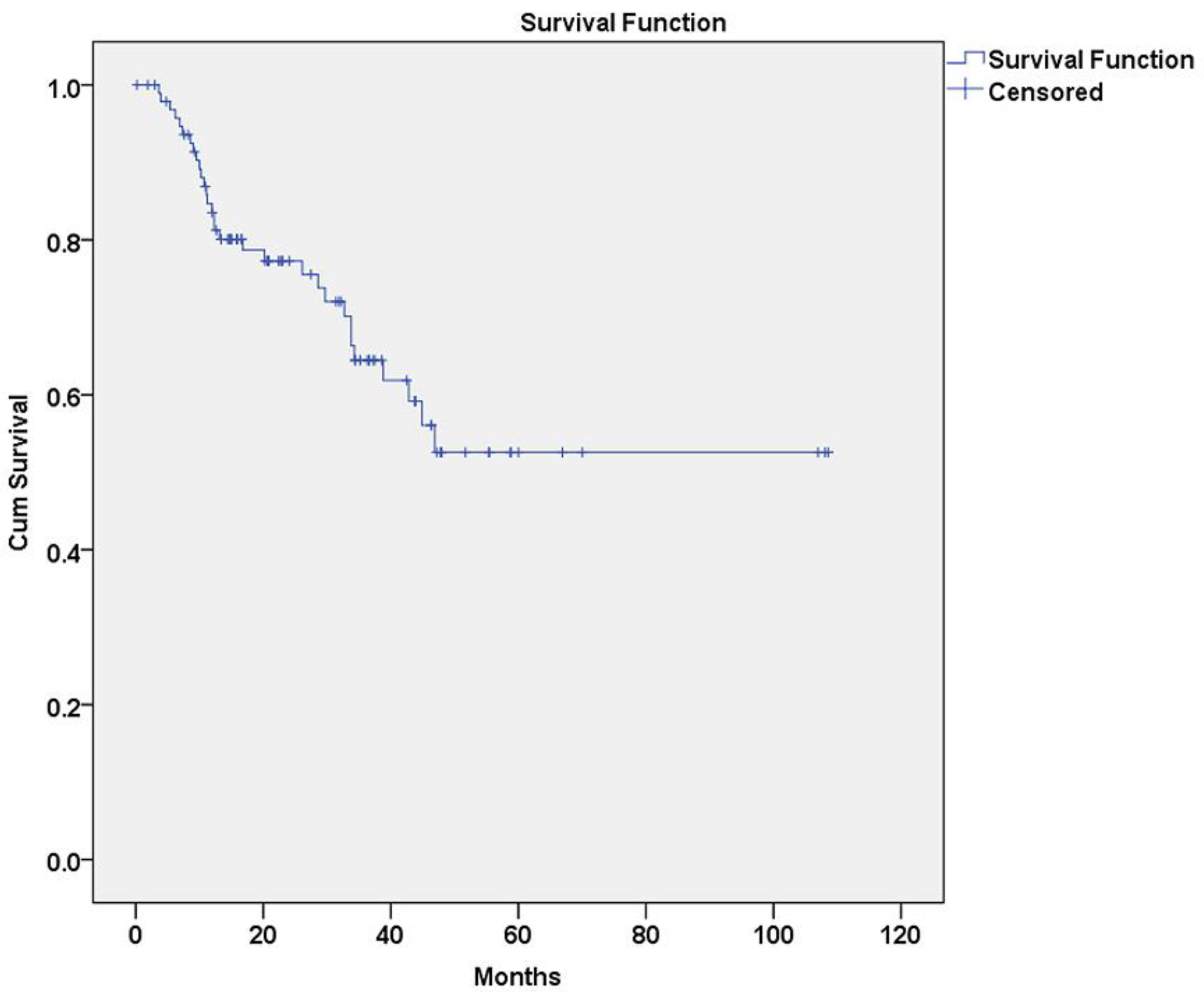
The baseline characteristics were summarized as absolute (n) and relative (%) frequencies in tables and relevant data were compared in terms of two tailed Fisher’s exact test. Statistical comparisons of molecular marker IHC scores were performed with Mann-Whitney U test, Kruskal-Wallis H test and Wilcoxon Signed Rank test. Disease free survival (DFS) curves were calculated according to the method of Kaplan and Meier. The significance of all parameters under study for DFS was analyzed by the Cox proportional hazards model. Statistical analyses were performed using the SPSS software application (version 21.0: SPSS, Chicago, IL, USA.) with p < 0.05 as the threshold of significance.
4. Discussion
In this descriptive analysis of well-documented OL cases, we investigated key demographic, clinical, microscopic, and IHC parameters that could affect its biologic behavior. Malignant transformation (MT) is justifiably considered as the most important end point of the behavior of this entity and, as a result, several comparative studies have assessed various parameters affecting the risk of transition from OL to OSCC [
4,
26]. On the other hand, few studies have focused on OL recurrence, although it is evident that it represents an important factor affecting the outcome of these lesions [
12,
19], especially taking into consideration that development of OSCC (including progression of pre-existing OPMDs) does not usually occur abruptly, but involves a multistep process driven by the gradual accumulation of molecular defects [
14]. Hence, it is fundamental also to characterize OL recurrences, including their rate, pattern and potential predictors, since they could be intimately associated with a tendency towards MT [
12,
27]. The clinical significance of assessing the risk of recurrence and progression is its potential utility for developing individualized protocols of management and follow-up, based on the various clinicopathologic and IHC findings of each specific case.
In the present study, we closely followed-up 33 patients with OL, following lesions removal either by incisional biopsy and laser ablation or scalpel surgical excision. We defined recurrence as the development of a new lesion in the same anatomic location of a previously treated OL We separately assessed the lesions that developed subsequently during follow-up in other oral anatomic sites, also recording their potential recurrences. An alternative consideration could be to regard these new distant lesions as recurrences, since OPMDs could be construed as generalized disorders rather than localized lesions [
6]; however, we preferred to consider all lesions separately, acknowledging the possibility that multifocal lesions, developing synchronously or metachronously, could be also attributed to independent genetic events and not necessarily to a widespread field cancerization effect.
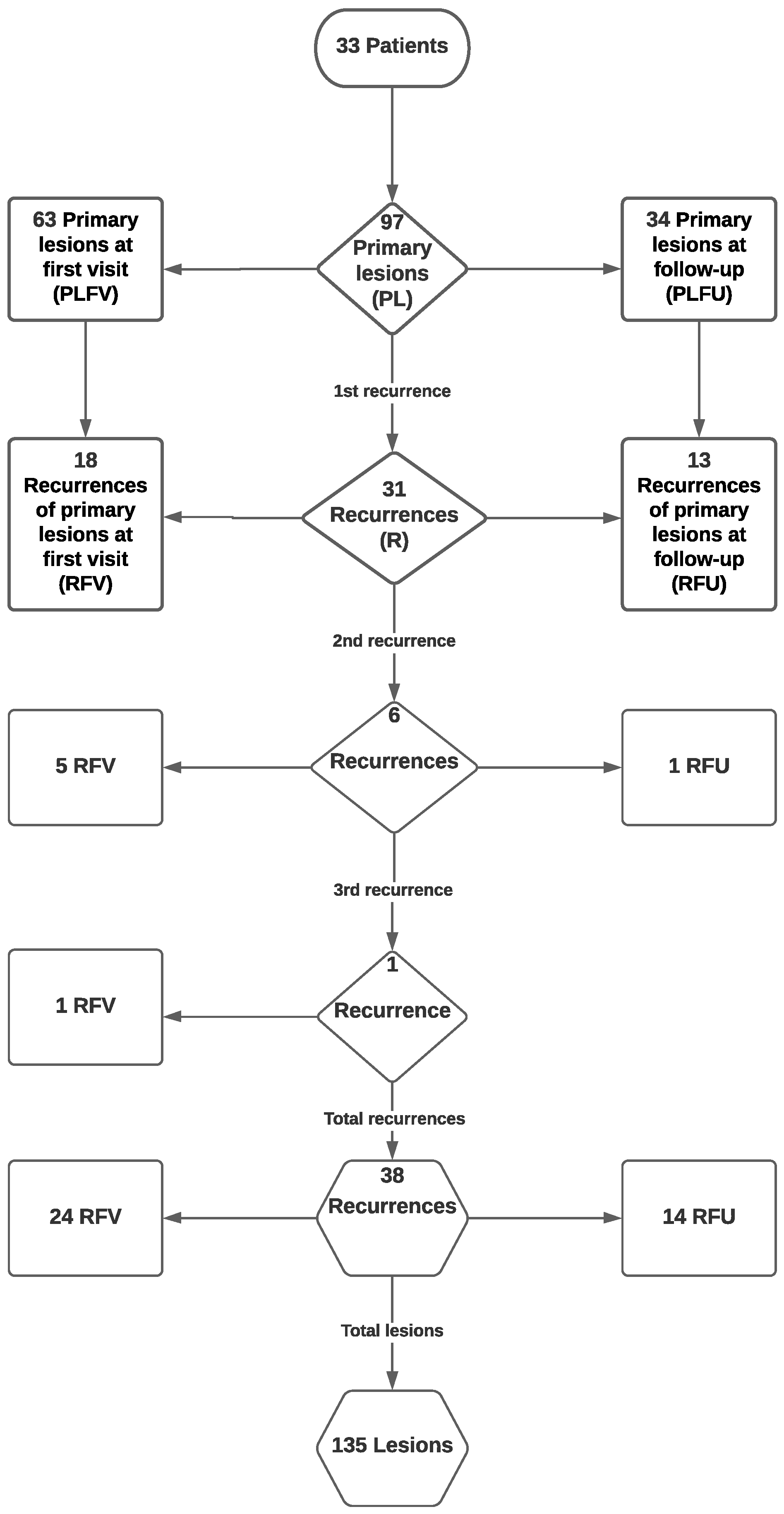
Noticeably, cancer development occurred in only one case and no patient developed OSCC in the same anatomic region as the initial OL; hence, statistical correlations of the various parameters with subsequent MT could not be carried out. This decreased number of MT in our study, despite adequate follow-up, could be attributed to the strict protocol used, involving very frequent recall appointments, meticulous oral examination by specialized clinicians, and prompt diagnostic and management intervention (including new biopsies, either excisional or incisional followed by laser ablation) for all new lesions detected. On the contrary, recurrence occurred in 18/63 PLs noticed at first visit; of these, four lesions recurred twice and one lesion recurred three times. In addition, during follow-up, 34 new primary OLs (defined as new lesions developing at different sites compared to the original primary OLs) were detected, out of which 13 recurred (once or, in one case, twice). Therefore, in the whole sample of 97 PLs, all of which were removed by surgical excision or laser ablation with adequate margin, a significant percentage (32% or approximately one in every three lesions) recurred once or more.
Holmstup et al. [
27] reported a 12.8% recurrence rate of OPMDs (12/94) following scalpel surgical removal, including 2/39 (5.1%) homogeneous OL, 8/46 (17.4%) non-homogeneous OL and 2/9 (22.2%) erythroplakias. Similar to these findings, we noted more frequent recurrences in non-homogeneous OLs (12/26, 46.2%) vs. homogeneous OLs (19/71, 26.8%), this difference approaching but not reaching statistical significance (
p = 0.087). However, although the overall frequency of recurrence was higher in our study, Holmstrup et al. reported a higher rate of MT (11/94, 11.7%), which, interestingly, occurred in 4 out of 12 recurring lesions in their series [
27].
In the study by Sundberg et al. [
12], out of 103 patients with surgically excised OLs, 43 (41.8%) developed recurrence, including 23/41 (56.1%) patients with non-homogeneous OLs and 20/62 (32.3%) patients with homogeneous OLs. These findings are in accord with our data, supporting the high incidence of recurrence in OL, despite adequate removal, and further substantiating an increased risk of recurrence for non-homogeneous lesions. Again, a relationship between recurrence and risk of MT was shown by Sundberg et al., as all four patients developing OSCC belonged to the group with recurring OL [
12].
Kuribayashi et al. [
19] reported a recurrence rate of 15.1% (8/53 surgically removed OL lesions). Similar to our study, only one of their patients developed OSCC (1.9%). However, in contrast with our findings, as well as those of Holmstrup et al. [
27] and Sundberg et al. [
12], homogeneous OLs showed a higher recurrence rate compared to non-homogeneous. The recurrence rate has also been associated with the treatment method used; for example, Ishii et al. [
28] showed that recurrences occurred in about 29% and 25% of OLs treated by laser surgery and surgical excision, respectively, while Monteiro et al. [
29] compared different surgical modalities (including scalpel excision vs. different types of laser) and did not find differences in the recurrence rate. In a recent systematic review [
30], the authors concluded that surgical laser excision may lower OL recurrence rate compared to conventional treatment, although it does not affect the risk of MT. Such discrepancies among the aforementioned studies may be due to sample bias and methodological differences, such as variations in study design, management and screening protocols. In addition, it should be noted that, independent of the surgical method used to completely remove a lesion within clinically or even microscopically healthy margins, there is always the possibility that molecular changes may persist in the surrounding tissues, possibly giving rise to recurrences; in this regard, recent publications have highlighted the existence of molecular changes in surgical margins of OL and have suggested that the use of non-invasive diagnostic adjuncts, such as autofluorescence, may enhance visualization of actual borders of the lesion, possibly facilitating complete excision in clear molecular margins [
15,
31,
32].
Besides homogeneity vs. non-homogeneity, other clinical characteristics of OL have also been reported to affect its biologic behavior. It is well established that increased size (>200 mm
2) and site of involvement (tongue and floor of mouth) show significant association with cancer development [
13]. Inconclusive data can be drawn from previous studies regarding the effect of these parameters in recurrence. Kuribayashi et al. [
19] reported a positive correlation between recurrence and involvement of the gingiva, while Chainani-Wu et al. [
33] demonstrated that early recurrence of OLs removed by CO
2 laser surgery was significantly associated only with poor accessibility of the lesion margins, such as gingival lesions with facial and palatal involvement or extensive lesions in posterior locations. On the other hand, other studies have failed to show an association between lesion location and recurrence [
12,
28]. Our results did not disclose significant associations of local recurrence with the site of OL, although lesions located in palatal mucosa appeared to recur more frequently (66.7%), compared to gingiva and alveolar mucosa (34.3%), ventral tongue/floor of mouth (33.3%), buccal mucosa (29.0%) and lateral/dorsal tongue (15.4%). Similarly, size did not significantly correlate with risk of recurrence, despite that fact that 40.7% of larger (≥2.0 cm) PLs recurred compared to 29.0% of smaller (<2.0 cm) PLs.
In addition to clinical features, diverse demographic and social characteristics of OL patients have been extensively investigated regarding their risk of cancer development. More precisely, females and non-smokers are considered to display a higher potential for MT [
13] and this socio-demographic profile has been suggested as a diagnostic criterion for proliferative verrucous leukoplakia (PVL), which is by definition a more aggressive entity [
34]. Additionally, increased age is a risk factor for OSCC occurrence in OL patients [
13]. The aforementioned literature on the risk of recurrence failed to disclose similar age-related associations [
12,
19,
33] with the exception of Kuribayashi et al. [
19], who reported a higher rate of recurrence in older patients (≥59 years). Further, neither gender nor smoking and drinking habits showed correlation with recurrence, similar to our findings.
It is widely acknowledged that oral epithelial dysplasia remains the most crucial predictor of OL progression, as most studies have shown that higher grades of dysplasia (such as moderately and severely dysplastic lesions, or high-grade lesions upon the binary grading system) carry an increased risk of cancer development compared to non-dysplastic or mildly dysplastic (or low grade) lesions [
6,
13,
14,
21,
35]. For example, Warnakulashuriya et al. [
36] have reported MT rates of 4.8%, 15.7% and 26.7% for mild, moderate and severe dysplasia, respectively, supporting that the severity of dysplasia bears significance as predictor for cancer development, while Kujan et al. [
35], using the binary system, demonstrated a much higher rate of MT for high-grade vs. low-grade lesions (80% vs. 15%). This has led to individualized management protocols based on the degree of dysplasia, with several authors supporting a lenient follow-up without excision for hyperplastic lesions or even certain mild dysplasias of low suspicion [
37]. Despite the unquestionable correlation between risk of MT and presence and degree of dysplasia, which, however, by itself cannot be considered as a reliable factor to predict the behavior of a given lesion, the association of dysplasia with increased likelihood of recurrences remains ambiguous. More precisely, previous studies did not display significant associations between dysplasia and OL recurrence [
12,
19,
28], similarly to our study, in which, however, dysplastic lesions recurred at a higher percentage compared to hyperplastic lesions (34.5% vs. 15.4%). These findings could strengthen the notion of a more interventional approach in the management of all OLs (i.e., complete removal and close follow-up) independently of the degree of dysplasia. Recent molecular findings seem to further support the behavioral similarities between dysplastic and non-dysplastic OLs, in that hyperkeratotic OLs with no dysplasia display similar molecular characteristics with dysplastic OLs [
38].
Further to sociodemographic, clinical and histopathologic features, we additionally investigated selected biomarkers that are deregulated during cancer. More specifically, we assessed the immunohistochemical expression of molecules that are involved in the signal transduction and activator of transcription 3 (STAT3) oncogenic signaling pathway by exerting proliferative and/or antiapoptotic effects [
20,
39]. In terms of oral carcinogenesis, these biomarkers have previously been investigated to a variable extent both in OSCC and OPMDs [
14]; however, their correlation with risk of OL recurrence remains unknown.
STAT3 has been characterized as an oncogenic molecule, which is activated by different upstream events, conveys messages to the nucleus and drives the transcription of molecules promoting cell proliferation (such as cyclin D1 and other regulators of the cell cycle) [
40] and inhibiting apoptosis (such as Bcl-xL and survivin) [
20,
41]. STAT3 aberrant expression has been associated with poor clinical outcome in OSCC [
42,
43,
44]. In addition, it has been demonstrated that dysplastic lesions are characterized by increased STAT3 expression levels [
43]. Nevertheless, in our study, tyrosine phosphorylated (activated) STAT3, despite its expression in the majority of OLs, did not show a correlation with degree of dysplasia nor was a predictor of recurrence.
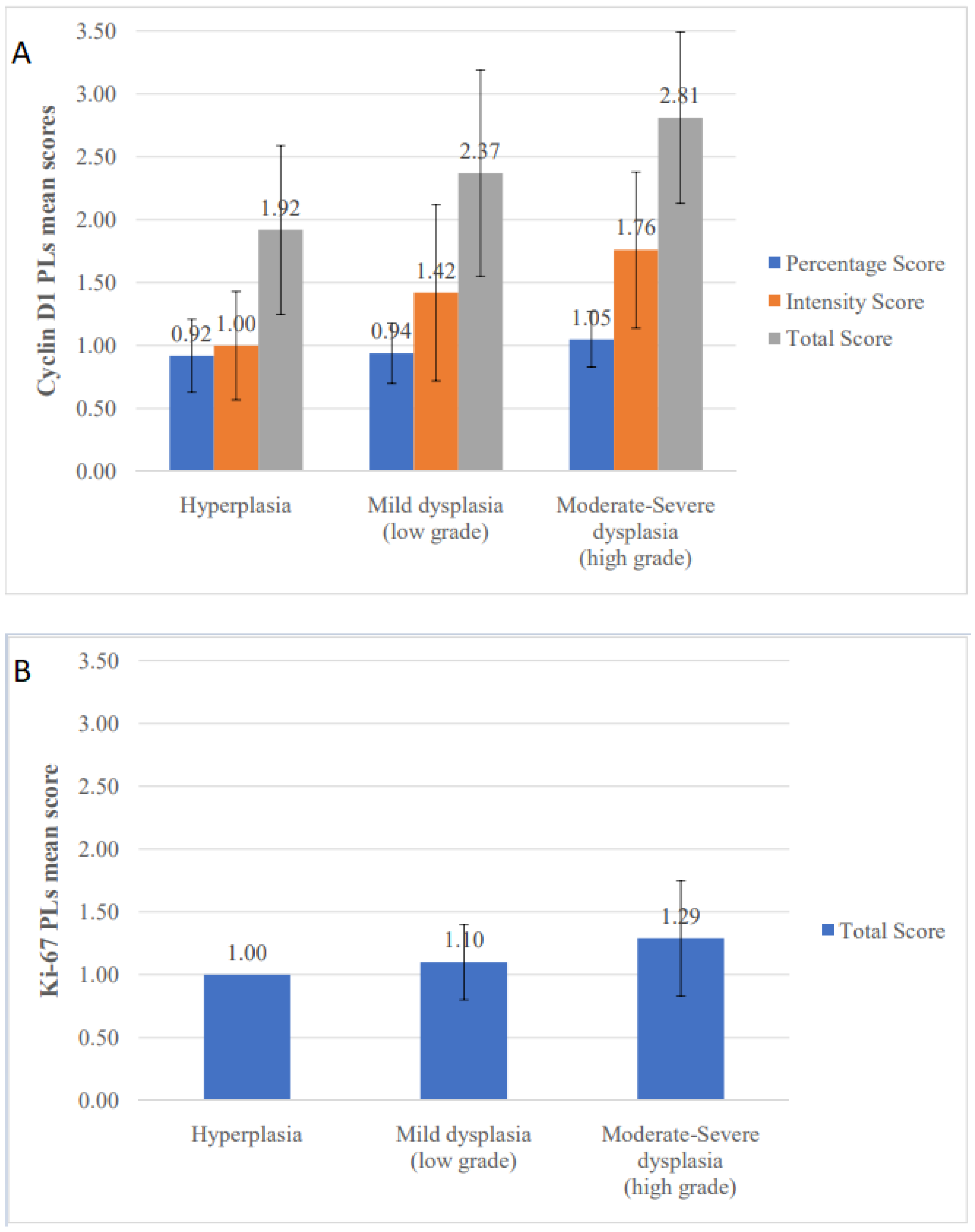
Among STAT3 downstream molecules, cyclin D1 has also been implicated in the biologic behavior of OSCC [
45]. Concerning oral premalignancy, an association of cyclin D1 expression with progression of the epithelium to a more dysplastic stage has been reported [
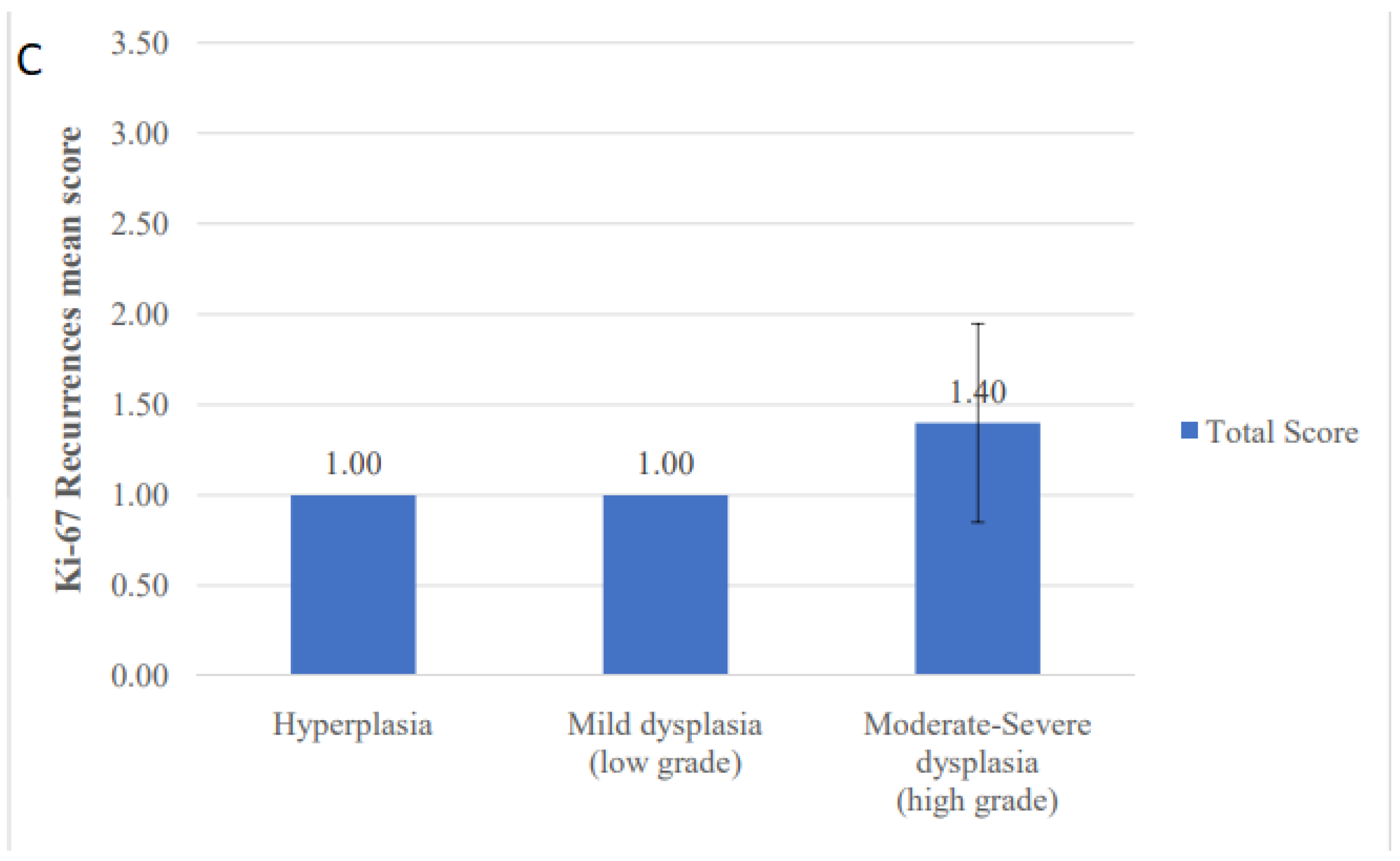
46]; however, the potential prognostic value of cyclin D1 in terms of OL recurrence and/or MT is uncertain. In our study, a correlation between cyclin D1 expression and degree of dysplasia was noticed; however, no association with recurrent behavior was seen. Similarly, Ki-67 index, a major indicator of the cell proliferative activity, was found to be positively associated with the degree of dysplasia, in accord with previous publications [
47]. Nonetheless, we did not find any correlation between Ki-67 levels and risk of recurrence, despite the fact that this molecule has been previously associated with progression of OL lesions [
48,
49,
50].
In addition to cell proliferation, the STAT3 signaling pathway also regulates the expression of downstream molecules that exert antiapoptotic activity. Specifically, Bcl-xL is induced by oncogenic STAT3 signaling and displays elevated expression in various types of cancer, including head and neck SCC [
51,
52]. Further, overexpression of Bcl-xL in OSCCs is related to advanced tumor stages, locoregional lymph node metastasis, and degree of differentiation [
53,
54]. However, there is very limited available information on the expression of Bcl-xL in oral premalignancy; Schoelch et al. [
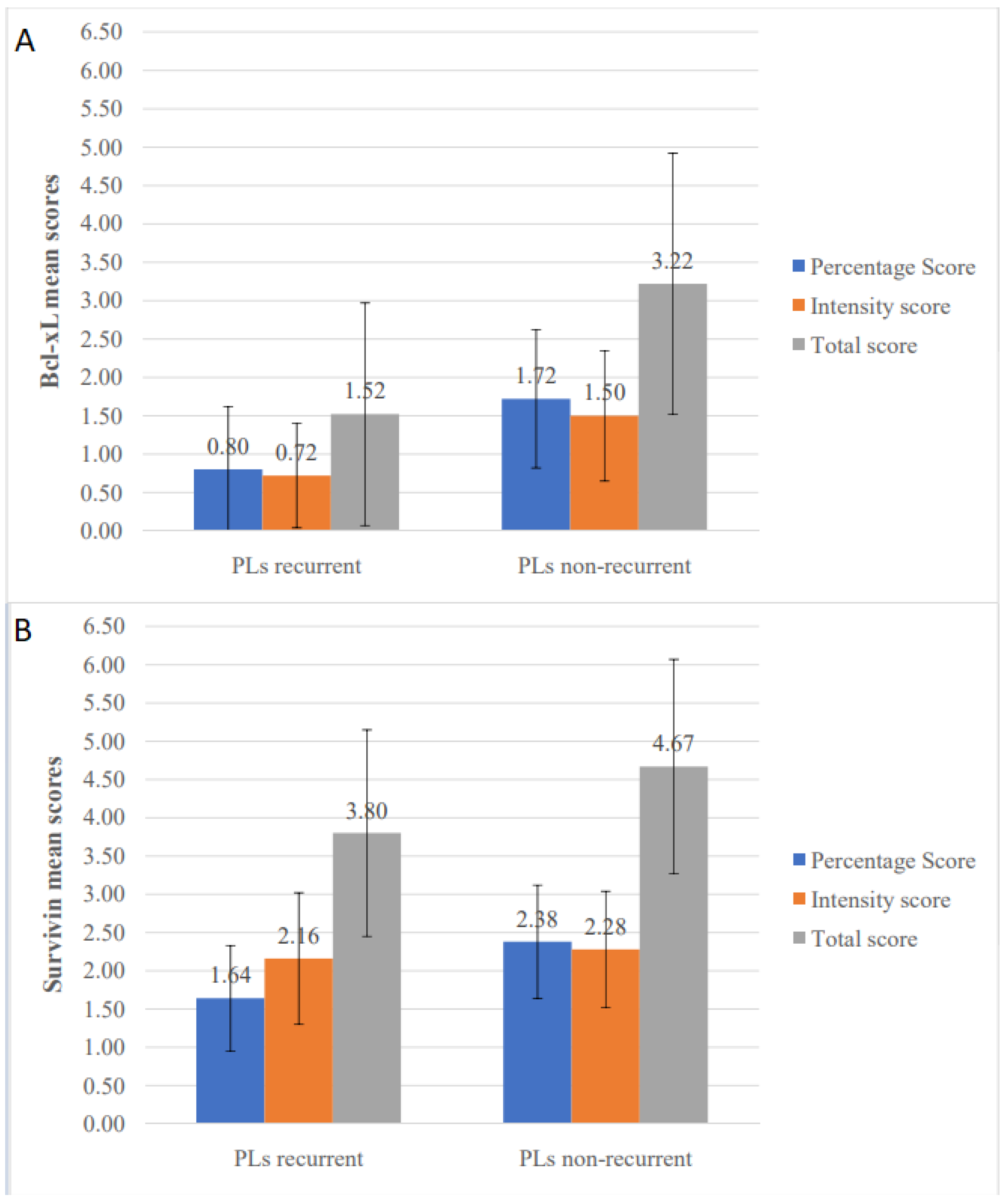
55] reported that Bcl-X (including both splice variants Bcl-xL and Bcl-xS) demonstrated immunohistochemical positivity in 70% of hyperkeratotic and mildly dysplastic lesions and 85.7% of moderate/severe dysplasias and carcinomas in situ, concluding that this molecule is expressed early in the process of oral carcinogenesis. In our study, Bcl-xL was expressed in the majority of both primary and recurrent lesions (82.4% and 94.7%, respectively), not being associated with the presence and degree of dysplasia. Interestingly, comparison between non-recurrent and recurrent PLs revealed lower Bcl-xL expression levels in the latter group; indeed, lower Bcl-xL percentage, intensity and total IHC scores were identified as significant risk factors for OL recurrence in univariate analysis, the percentage score also remaining significant in multivariate analysis.
Survivin, another downstream molecule of the STAT3 signaling pathway and a well-known inhibitor of apoptosis, has been shown to be expressed in oral premalignancy [
56] displaying positive correlations with dysplastic phenotype [
57] and progression to malignancy [
58]. However, no study to this date has investigated the relationship between the expression of this marker and the risk of OL recurrence. Our findings did not support an association between survivin IHC expression and degree of dysplasia. However, surprisingly, its expression correlated inversely with the risk of local recurrence with decreased levels of survivin in recurrent cases; in univariate (but not multivariate) analysis, survivin percentage score emerged as a significant risk factor for recurrence. These data highlight the complexity of oral carcinogenesis and suggest the possibility that various molecules may be involved in different and sometimes unexpected ways in diverse aspects of progression, i.e., recurrence vs. MT. Nonetheless, validation and clarification of these findings and the potential role of specific molecules as predictors of recurrence necessitate larger studies investigating these immunomarkers in recurrent vs. non-recurrent OLs.
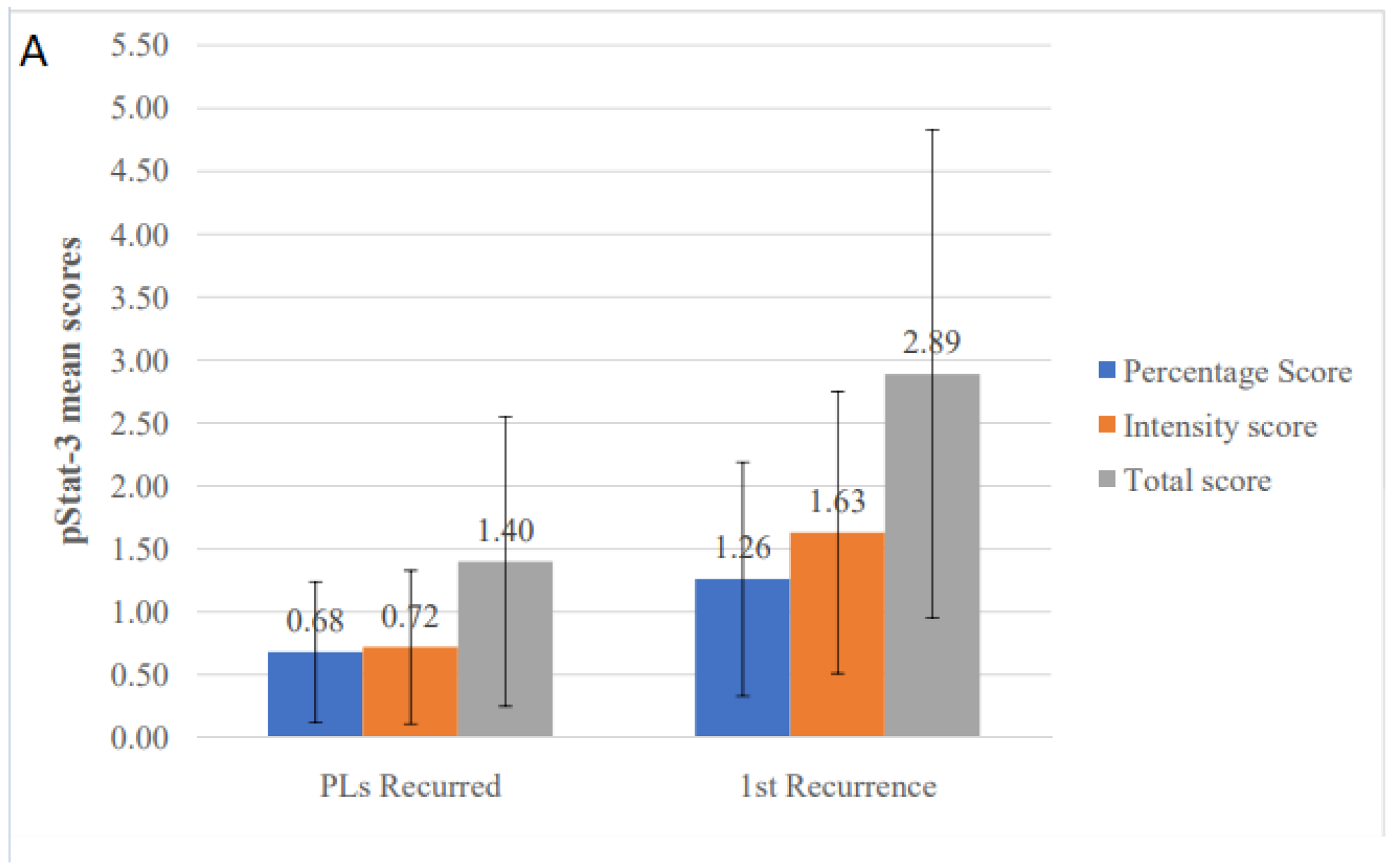
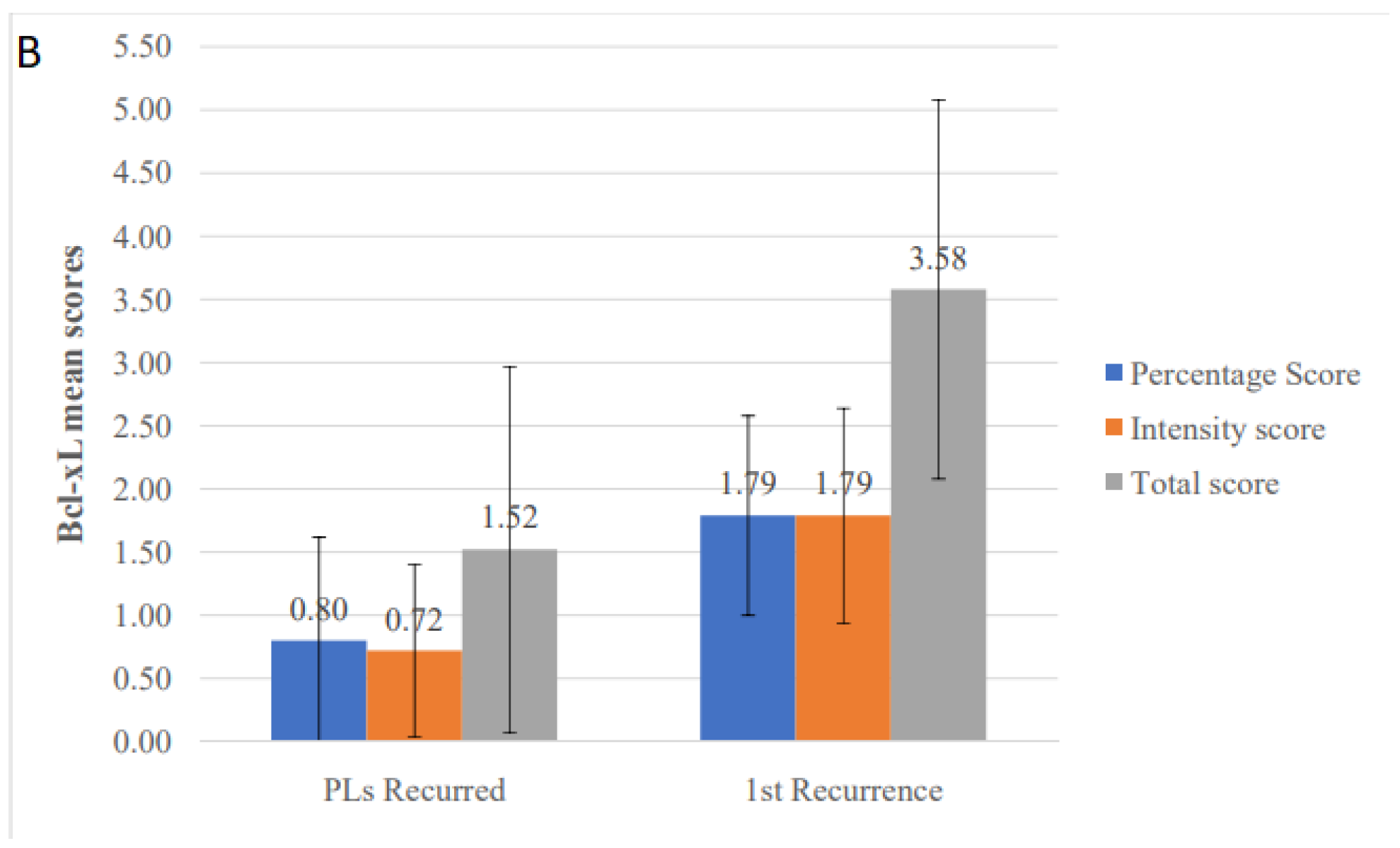
Another investigation carried out in our study was the comparison between PLs and their corresponding recurrences. Understanding how the clinical, histopathologic, and IHC features of OL lesions evolve through time and differ between first occurrence and recurrence is important. First of all, characterization of the biologic behavior of OPMDs as a function of time may give insight into the mechanisms of persistence and recurrence, possibly providing useful clues for the proper management of these lesions. Interestingly, we noticed a significantly milder clinicopathologic phenotype in the recurrent lesions, which tended to be significantly smaller and more homogeneous, also including a higher percentage of hyperplastic (non-dysplastic) cases. This should not be interpreted as an indication of a better biologic behavior in recurrences compared to PLs, but probably implies that proper follow-up could result into early detection of these lesions before they acquire aggressive phenotypic and molecular characteristics, thus highlighting the necessity of close monitoring of these patients. On the other hand, it is noteworthy that recurrences showed significantly higher expression levels of pSTAT3 and Bcl-xL (and a tendency also for higher expression of cyclin D1 and survivin) suggesting that, despite the lack of clinicopathologic features of aggressiveness, it is likely that recurrences may be characterized by an increased level of molecular aberrations, potentially linked to their risk of further progression.


 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}