
Distinct Mechanical Properties of the Respiratory System Evaluated by Forced Oscillation Technique in Acute Exacerbation of COPD and Acute Decompensated Heart Failure

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population in Analysis
2.2. Study Design
2.3. Feasibility and Safety Procedures
2.4. Statistical Analysis
3. Results
3.1. Blood Gas Analysis, Blood Tests, Symptoms, and Physical Examination
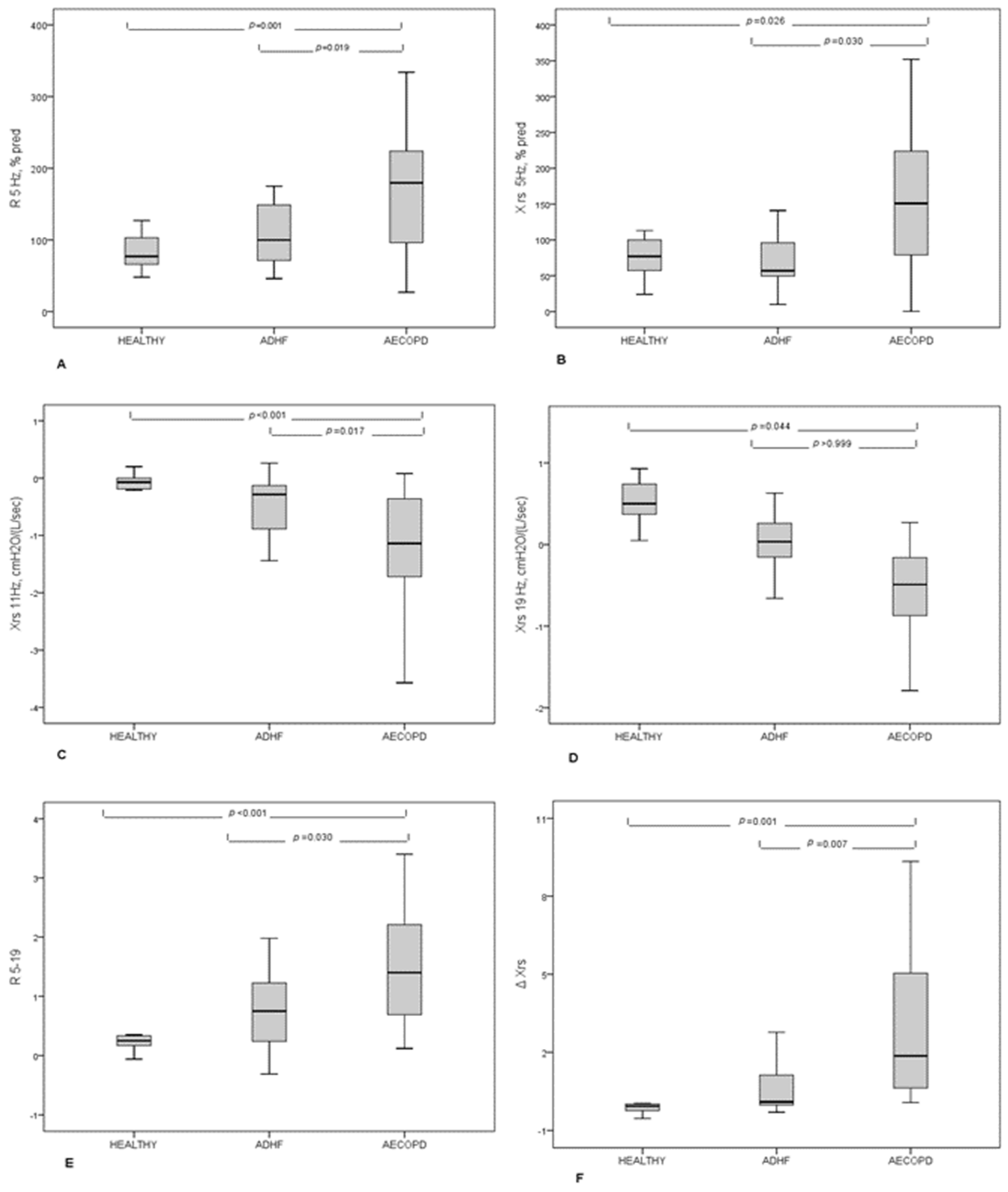
3.2. FOT Results
3.3. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, C.S.; Fitzgerald, J.M.; Schulzer, M.; Mak, E.; Ayas, N.T. Does This Dyspneic Patient in the Emergency Department Have Congestive Heart Failure? JAMA 2005, 294, 1944–1956. [Google Scholar] [CrossRef] [PubMed]
- Mantuani, D.; Frazee, B.W.; Fahimi, J.; Nagdev, A. Point-of-Care Multi-Organ Ultrasound Improves Diagnostic Accuracy in Adults Presenting to the Emergency Department with Acute Dyspnea. West. J. Emerg. Med. 2016, 17, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Yoshihisa, A.; Takiguchi, M.; Shimizu, T.; Nakamura, Y.; Yamauchi, H.; Iwaya, S.; Owada, T.; Miyata, M.; Abe, S.; Sato, T.; et al. Cardiovascular function and prognosis of patients with heart failure coexistent with chronic obstructive pulmonary disease. J. Cardiol. 2014, 64, 256–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macchia, A.; Moncalvo, J.J.R.; Kleinert, M.; Comignani, P.D.; Gimeno, G.; Arakaki, D.; Laffaye, N.; Fuselli, J.J.; Massolin, H.P.; Gambarte, J.; et al. Unrecognised ventricular dysfunction in COPD. Eur. Respir. J. 2011, 39, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Ishizu, T. Chronic obstructive pulmonary disease: Pathophysiological impact on heart failure in real clinical situation. J. Cardiol. 2014, 64, 250–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Jemtel, T.H.; Padeletti, M.; Jelic, S. Diagnostic and Therapeutic Challenges in Patients with Coexistent Chronic Obstructive Pulmonary Disease and Chronic Heart Failure. J. Am. Coll. Cardiol. 2007, 49, 171–180. [Google Scholar] [CrossRef] [Green Version]
- Witte, K.K.; Morice, A.; Clark, A.L.; Cleland, J.G. Airway resistance in chronic heart failure measured by impulse oscillometry. J. Card. Fail. 2002, 8, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Global Strategy for Diagnosis, Management, and Prevention of COPD–2017. Available online: https://goldcopd.org/wp-content/uploads/2017/02/wms-GOLD-2017-FINAL.pdf (accessed on 17 March 2021).
- Frank, N.R. Influence of acute pulmonary vascular congestion on recoiling force of excised cats’ lung. J. Appl. Physiol. 1959, 14, 905–908. [Google Scholar] [CrossRef]
- Dubois, A.B.; Brody, A.W.; Lewis, D.H.; Burgess, B.F. Oscillation Mechanics of Lungs and Chest in Man. J. Appl. Physiol. 1956, 8, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Frank, N.R.; Radford, E.P.; Whittenberger, J.L. Static volume-pressure interrelations of the lungs and pulmonary blood vessels in excised cats’ lungs. J. Appl. Physiol. 1959, 14, 167–173. [Google Scholar] [CrossRef]
- Barnas, G.M.; Stamenovic, D.; Lutchen, K.R. Lung and chest wall impedances in the dog in normal range of breathing: Effects of pulmonary edema. J. Appl. Physiol. 1992, 73, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Peslin, R.; Da Silva, J.F.; Duvivier, C.; Chabot, F. Respiratory mechanics studied by forced oscillations during artificial ventilation. Eur. Respir. J. 1993, 6, 772–784. [Google Scholar]
- Cavalcanti, J.V.; Lopes, A.J.; Jansen, J.M.; Melo, P.L. Detection of changes in respiratory mechanics due to increasing degrees of airway obstruction in asthma by the forced oscillation technique. Respir. Med. 2006, 100, 2207–2219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaegashi, M.; Yalamanchili, V.A.; Kaza, V.; Weedon, J.; Heurich, A.E.; Akerman, M.J. The utility of the forced oscillation technique in assessing bronchodilator responsiveness in patients with asthma. Respir. Med. 2007, 101, 995–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dellacà, R.L.; Zannin, E.; Sancini, G.; Rivolta, I.; Leone, B.E.; Pedotti, A.; Miserocchi, G. Changes in the mechanical properties of the respiratory system during the development of interstitial lung edema. Respir. Res. 2008, 9, 51–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Celli, B.; MacNee, W.; Agusti, A.; Anzueto, A.; Berg, B.; Buist, A.; Calverley, P.; Chavannes, N.; Dillard, T.; Fahy, B.; et al. Standards for the diagnosis and treatment of patients with COPD: A summary of the ATS/ERS position paper. Eur. Respir. J. 2004, 23, 932–946. [Google Scholar] [CrossRef] [Green Version]
- Oostveen, E.; MacLeod, D.; Lorino, H.; Farre, R.; Hantos, Z.; Desager, K.; Marchal, F. The forced oscillation technique in clinical practice: Methodology, recommendations and future developments. Eur. Respir. J. 2003, 22, 1026–1041. [Google Scholar] [CrossRef]
- Dellaca, R.L.; Santus, P.; Aliverti, A.; Stevenson, N.; Centanni, S.; Macklem, P.T.; Pedotti, A.; Calverley, P.M.A. De-tection of expiratory flow limitation in COPD using the forced oscillation technique. Eur. Respir. J. 2004, 23, 232–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dellacà, R.L.; Duffy, N.; Pompilio, P.P.; Aliverti, A.; Koulouris, N.G.; Pedotti, A.; Calverley, P.M.A. Expiratory flow limitation detected by forced oscillation and negative expiratory pressure. Eur. Respir. J. 2006, 29, 363–374. [Google Scholar] [CrossRef] [Green Version]
- Collins, S.P.; Lindsell, C.J.; Peacock, W.F.; Eckert, D.C.; Askew, J.; Storrow, A.B. Clinical characteristics of emergency department heart failure patients initially diagnosed as non-heart failure. BMC Emerg. Med. 2006, 6, 11. [Google Scholar] [CrossRef] [Green Version]
- Pivetta, E.; Goffi, A.; Lupia, E.; Tizzani, M.; Porrino, G.; Ferreri, E.; Volpicelli, G.; Balzaretti, P.; Banderali, A.; Iacobucci, A.; et al. Lung Ultrasound-Implemented Diagnosis of Acute Decompensated Heart Failure in the ED. Chest 2015, 148, 202–210. [Google Scholar] [CrossRef] [Green Version]
- Frasure, S.E.; Matilsky, D.K.; Siadecki, S.D.; Platz, E.; Saul, T.; Lewiss, R.E. Impact of patient positioning on lung ultrasound findings in acute heart failure. Eur. Hear. J. Acute Cardiovasc. Care 2015, 4, 326–332. [Google Scholar] [CrossRef]
- Santus, P.; Centanni, S.; Verga, M.; Di Marco, F.; Matera, M.; Cazzola, M. Comparison of the acute effect of tiotropium versus a combination therapy with single inhaler budesonide/formoterol on the degree of resting pulmonary hyperinflation. Respir. Med. 2006, 100, 1277–1281. [Google Scholar] [CrossRef] [Green Version]
- Giner, J.; Plaza, V.; Rigau, J.; Solà, J.; Bolibar, I.; Sanchis, J. Spirometric Standards and Patient Characteristics: An Exploratory Study of Factors Affecting Fulfillment in Routine Clinical Practice. Respir. Care 2014, 59, 1832–1837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverman, R.A.; Flaster, E.; Enright, P.L.; Simonson, S.G. FEV 1 Performance among Patients with Acute Asthma. Chest 2007, 131, 164–171. [Google Scholar] [CrossRef]
- A Camargo, C.; Tsai, C.-L.; Clark, S.; A Kenney, P.; Radeos, M.S. Spirometric correlates of dyspnea improvement among emergency department patients with chronic obstructive pulmonary disease exacerbation. Respir. Care 2008, 53, 892–896. [Google Scholar] [PubMed]
- Tse, H.N.; Tseng, C.Z.S.; Wong, K.Y.; Yee, K.S.; Ng, L.Y. Accuracy of forced oscillation technique to assess lung function in geriatric COPD population. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 1105–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ducharme, F.M.; Davis, G.M. Respiratory Resistance in the Emergency Department. Chest 1998, 113, 1566–1572. [Google Scholar] [CrossRef]
- Hawkins, N.M.; Virani, S.; Ceconi, C. Heart failure and chronic obstructive pulmonary disease: The challenges facing physicians and health services. Eur. Hear. J. 2013, 34, 2795–2807. [Google Scholar] [CrossRef] [Green Version]
- Brenner, S.; Güder, G.; Berliner, D.; Deubner, N.; Fröhlich, K.; Ertl, G.; Jany, B.; Angermann, C.E.; Störk, S. Airway obstruction in systolic heart failure–COPD or congestion? Int. J. Cardiol. 2013, 168, 1910–1916. [Google Scholar] [CrossRef] [PubMed]
- Young, H.M.; Guo, F.; Eddy, R.L.; Maksym, G.; Parraga, G. Oscillometry and pulmonary MRI measurements of ventilation heterogeneity in obstructive lung disease: Relationship to quality of life and disease control. J. Appl. Physiol. 2018, 125, 73–85. [Google Scholar] [CrossRef]
- Lutchen, K.R.; Gillis, H. Relationship between heterogeneous changes in airway morphometry and lung resistance and elastance. J. Appl. Physiol. 1997, 83, 1192–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Marco, F.; Terraneo, S.; Job, S.; Rinaldo, R.F.; Papa, G.F.S.; Roggi, M.A.; Santus, P.; Centanni, S. Cardiopulmonary exercise testing and second-line pulmonary function tests to detect obstructive pattern in symptomatic smokers with borderline spirometry. Respir. Med. 2017, 127, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| AECOPD (n = 25) | ADHF (n = 24) | HEALTHY (n = 11) | p * | P AECOPD vs. ADHF ** | |
|---|---|---|---|---|---|
| Age, median IQR, years | 70 (66–76) | 80 (67–83) | 70 (69–71) | 0.081 | |
| Male, n (%) | 20 (80) | 12 (50) | 7 (64) | 0.088 | |
| BMI, kg/m2 | 24.6 (22–28.3) | 28.0 (24.5–33.1) | 23.1 (22.8–26.6) | 0.017 | 0.049 |
| Smoking history | |||||
| Current, n (%) | 12 (57) | 1 (5) | 0 (0) | <0.001 | <0.001 |
| Ex, n (%) | 9 (43) | 9 (43) | 1 (9) | ||
| Never, n (%) | 0 (0) | 11 (52) | 0 (0) | ||
| Previous AHF, n (%) | 0 (0) | 9 (38) | 0 (0) | <0.001 | 0.001 |
| Valvular heart disease, n (%) | 2 (8) | 5 (21) | 0 (0) | 0.154 | 0.247 |
| OSAS, n (%) | 1 (4) | 2 (8) | 0 (0) | 0.811 | |
| Atrial fibrillation, n (%) | 3 (12) | 10 (42) | 1 (9) | 0.023 | 0.025 |
| Arterial hypertension, n (%) | 13 (52) | 16 (67) | 2 (18) | 0.029 | 0.387 |
| Ischemic heart disease, n (%) | 7 (28) | 10 (42) | 0 (0) | 0.040 | 0.377 |
| Cancer, n (%) | 2 (8) | 2 (8) | 0 (0) | 0.617 | >0.999 |
| AECOPD (n = 25) | ADHF (n = 24) | p | |
|---|---|---|---|
| Dyspnea | <0.001 | ||
| new onset, n (%) | 2 (8) | 14 (58) | |
| worsening from usual, n (%) | 23 (92) | 10 (42) | |
| Orthopnea, n (%) | 2 (8) | 12 (50) | 0.001 |
| Cough, n (%) | 19 (76) | 6 (25) | 0.001 |
| Increased sputum volume, n (%) | 15 (60) | 3 (12) | 0.001 |
| Increased sputum purulence, n (%) | 6 (24) | 0 (0) | 0.022 |
| Hemoptysis, n (%) | 1 (4) | 0 (0) | >0.999 |
| Thoracic pain, n (%) | 3 (12) | 2 (8) | >0.999 |
| Fever, n (%) | 7 (28) | 3 (13) | 0.289 |
| Oliguria, n (%) | 0 (0) | 4 (17) | 0.109 |
| Chest examination | |||
| Normal, n (%) | 1 (5) | 7 (32) | >0.001 |
| Globally reduced, n (%) | 18 (90) | 5 (23) | |
| Focally reduced, n (%) | 1 (5) | 10 (46) | |
| Rhonchi, n (%) | 15 (68) | 0 (0) | <0.001 |
| Crackles, n (%) | 1 (5) | 15 (75) | |
| Rhonchi and crackles | 1 (4) | 2 (8) | |
| Normal heart sound, n (%) | 17 (85) | 9 (41) | 0.005 |
| Arrhythmia, n (%) | 1 (5) | 7 (32) | 0.047 |
| Lower limbs swelling, n (%) | 1 (5) | 13 (50) | <0.001 |
| Jugular turgescence, n (%) | 0 (0) | 2 (9) | 0.305 |
| RR, breath/min | 16 (15–19) | 17 (15–20) | 0.782 |
| HR, beats/min | 80 (74–92) | 79 (71–93) | 0.723 |
| Systolic arterial pressure, mmHg | 140 (120–150) | 140 (122–155) | 0.668 |
| Diastolic arterial pressure, mmHg | 80 (70–85) | 80 (65–90) | 0.957 |
| Body temperature, °C | 36.0 (36.0–36.4) | 36.0 (36.0–36.0) | 0.408 |
| Oxygen therapy, l/min | 3 (1–4) | 3 (1–3) | 0.605 |
| AECOPD (n = 25) | ADHF (n = 24) | p | |
|---|---|---|---|
| WBC, cells/L | 10,200 (8500–12,500) | 8800 (8200–11,200) | 0.299 |
| Platelets,·cells/L | 203,000 (173,000–285,000) | 256,000 (175,000–309,000) | 0.664 |
| Hemoglobin, g/dL | 13.1 (12.0–13.7) | 11.0 (10.0–13.7) | 0.018 |
| Hematocrit, % | 38.7 (34.4–42.6) | 34.65 (31.3–40.8) | 0.045 |
| Creatinine, mg/dL | 0.9 (0.62–0.9) | 1.25 (0.8–1.7) | 0.003 |
| Azotemia, mg/dL | 19 (14–22) | 31 (23–39) | 0.001 |
| Sodium, mEq/L | 139 (137–142) | 141 (137–143) | 0.312 |
| Potassium, mEq/L | 4.2 (3.9–4.5) | 4.2 (3.9–4.9) | 0.609 |
| NTproBNP, pg/mL | 435 (179–800) | 3965 (1093–5965) | <0.001 |
| AST, U/L | 20 (17–26) | 31 (21–36) | 0.016 |
| pH * | 7.41 (7.38–7.43) | 7.40 (7.31–7.42) | 0.349 |
| PaO2, mmHg | 56 (49–59) | 55 (49–59) | 0.817 |
| PaCO2, mmHg | 43 (36–48) | 38 (34–39) | 0.076 |
| HCO3, mmol/L | 25.4 (24–27) | 21.8 (19.7–23.1) | 0.014 |
| AECOPD (n = 25) | ADHF (n = 24) | HEALTHY (n = 11) | p * | p AECOPD vs. AHF ** | |
|---|---|---|---|---|---|
| Rrs 5 Hz † | 4.44 (2.9–5.47) | 3.32 (2.25–4.76) | 2.12 (1.51–2.39) | 0.002 | 0.237 |
| Rrs 5 Hz, % | 179 (94–224) | 100 (67–149) | 77 (63–104) | 0.001 | 0.019 |
| Xrs 5 Hz † | −1.8 (−2.6–−0.92) | −0.98 (−1.47–−0.53) | −0.77 (−0.97–−0.69) | 0.026 | 0.126 |
| Xrs 5 Hz, % | 151 (74–231) | 57 (49.2–99) | 77 (39–102) | 0.005 | 0.005 |
| Rrs 11 Hz † | 3.36 (2.55–4.12) | 3.35 (2.04–4.44) | 1.99 (1.49–2.42) | 0.010 | >0.999 |
| Rrs 11 Hz, % | 141 (93–172) | 107 (69–128) | 75 (60–104) | 0.008 | 0.134 |
| Xrs 11 Hz † | −1.14 (1.73–−0.34) | −0.28 (−0.89–−0.11) | −0.07 (−0.21–0.01) | <0.001 | 0.017 |
| Xrs 11 Hz, % | 218 (−432–1195) | 104 (−33–260) | 23 (−97–76) | 0.227 | |
| Rrs 19 Hz † | 2.76 (2.10–3.31) | 2.94 (1.90–3.73) | 1.99 (1.19–2.21) | 0.044 | >0.999 |
| Rrs 19 Hz, % | 104 (77–132) | 88 (62–117) | 80 (47–91) | 0.032 | 0.424 |
| Xrs 19 Hz † | −0.49 (−0.87–−0.13) | 0.03 (−0.17–0.26) | 0.50 (0.33–0.78) | <0.001 | 0.005 |
| Rrs5–19 | 1.49 (1.03–2.16) | 0.44 (0.22–0.76) | 0.25 (0.16–0.35) | <0.001 | 0.030 |
| ΔXrs5 † | 1.86 (0.43–5.14) | 0.09 (−0.04–1.16) | −0.70 (−0.26–0.04) | <0.001 | 0.007 |
| Flow limitation, % | 10 (0–100) | 0 (0–12) | 0 | <0.001 | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terraneo, S.; Rinaldo, R.F.; Sferrazza Papa, G.F.; Ribolla, F.; Gulotta, C.; Maugeri, L.; Gatti, E.; Centanni, S.; Di Marco, F. Distinct Mechanical Properties of the Respiratory System Evaluated by Forced Oscillation Technique in Acute Exacerbation of COPD and Acute Decompensated Heart Failure. Diagnostics 2021, 11, 554. https://doi.org/10.3390/diagnostics11030554
Terraneo S, Rinaldo RF, Sferrazza Papa GF, Ribolla F, Gulotta C, Maugeri L, Gatti E, Centanni S, Di Marco F. Distinct Mechanical Properties of the Respiratory System Evaluated by Forced Oscillation Technique in Acute Exacerbation of COPD and Acute Decompensated Heart Failure. Diagnostics. 2021; 11(3):554. https://doi.org/10.3390/diagnostics11030554
Chicago/Turabian StyleTerraneo, Silvia, Rocco Francesco Rinaldo, Giuseppe Francesco Sferrazza Papa, Fulvia Ribolla, Carlo Gulotta, Laura Maugeri, Emiliano Gatti, Stefano Centanni, and Fabiano Di Marco. 2021. "Distinct Mechanical Properties of the Respiratory System Evaluated by Forced Oscillation Technique in Acute Exacerbation of COPD and Acute Decompensated Heart Failure" Diagnostics 11, no. 3: 554. https://doi.org/10.3390/diagnostics11030554