
Diagnostic Role of 18F-PSMA-1007 PET/CT in Prostate Cancer Staging: A Systematic Review

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
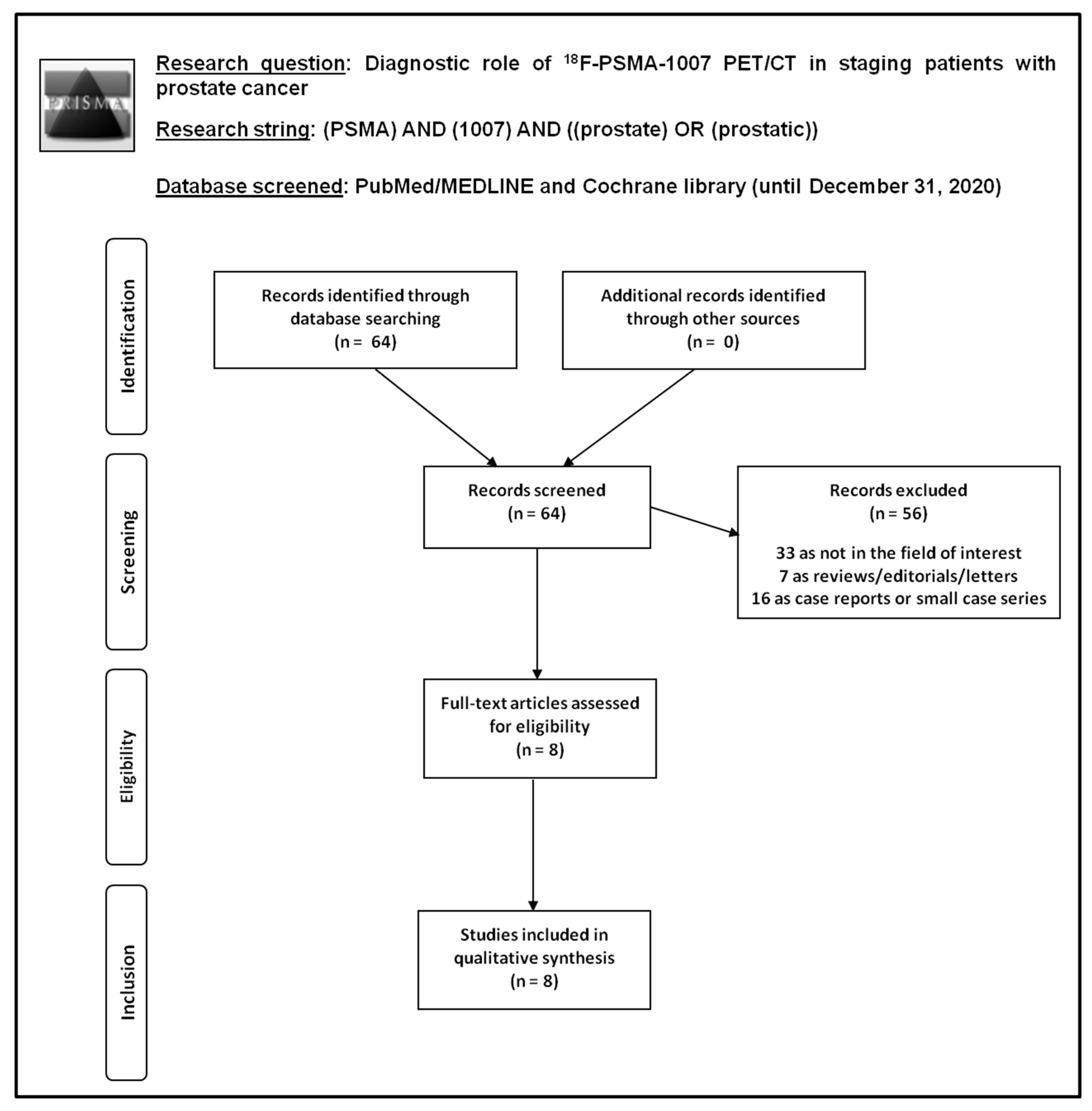
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
3. Results
3.1. Literature Search
3.2. Qualitative Analysis (Systematic Review)
3.2.1. Basic Study and Patient Characteristics
3.2.2. Technical Aspects
3.2.3. Quality Assessment
3.2.4. Main Findings
4. Discussion
4.1. Discussion of Main Findings
4.2. Limitations
4.3. Suggestions for Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hassanipour-Azgomi, S.; Mohammadian-Hafshejani, A.; Ghoncheh, M.; Towhidi, F.; Jamehshorani, S.; Salehiniya, H. Incidence and mortality of prostate cancer and their relationship with the Human Development Index worldwide. Prostate Int. 2016, 4, 118–124. [Google Scholar] [CrossRef] [Green Version]
- Schiavina, R.; Chessa, F.; Borghesi, M.; Gaudiano, C.; Bianchi, L.; Corcioni, B.; Castellucci, P.; Ceci, F.; Ceravolo, I.; Barchetti, G.; et al. State-of-the-art imaging techniques in the management of preoperative staging and re-staging of prostate cancer. Int. J. Urol. 2018, 26, 18–30. [Google Scholar] [CrossRef] [Green Version]
- Fanti, S.; Minozzi, S.; Antoch, G.; Banks, I.; Briganti, A.; Carrio, I.; Chiti, A.; Clarke, N.; Eiber, M.; De Bono, J.; et al. Consensus on molecular imaging and theranostics in prostate cancer. Lancet Oncol. 2018, 19, e696–e708. [Google Scholar] [CrossRef]
- Annunziata, S.; Pizzuto, D.A.; Treglia, G. Diagnostic Performance of PET Imaging Using Different Radiopharmaceuticals in Prostate Cancer According to Published Meta-Analyses. Cancers 2020, 12, 2153. [Google Scholar] [CrossRef]
- Okarvi, S.M. Recent developments of prostate-specific membrane antigen (PSMA)-specific radiopharmaceuticals for precise imaging and therapy of prostate cancer: An overview. Clin. Transl. Imaging 2019, 7, 189–208. [Google Scholar] [CrossRef]
- Ceci, F.; Fanti, S. PSMA-PET/CT imaging in prostate cancer: Why and when. Clin. Transl. Imaging 2019, 7, 377–379. [Google Scholar] [CrossRef] [Green Version]
- Ceci, F.; Castellucci, P.; Fanti, S. Current application and future perspectives of PSMA PET imaging in prostate cancer. Q. J. Nucl. Med. Mol. Imaging 2019, 63, 7–18. [Google Scholar] [CrossRef]
- Von Eyben, F.E.; Baumann, G.S.; Baum, R.P. PSMA diagnostics and treatments of prostate cancer become mature. Clin. Transl. Imaging 2018, 6, 145–148. [Google Scholar] [CrossRef] [Green Version]
- Treglia, G.; Mestre, R.P.; Ferrari, M.; Bosetti, D.G.; Pascale, M.; Oikonomou, E.; De Dosso, S.; Jermini, F.; O Prior, J.; Roggero, E.; et al. Radiolabelled choline versus PSMA PET/CT in prostate cancer restaging: A meta-analysis. Am. J. Nucl. Med. Mol. Imaging 2019, 9, 127–139. [Google Scholar] [PubMed]
- Mestre, R.P.; Treglia, G.; Ferrari, M.; Pascale, M.; Mazzara, C.; Azinwi, N.C.; Llado’, A.; Stathis, A.; Giovanella, L.; Roggero, E. Correlation between PSA kinetics and PSMA-PET in prostate cancer restaging: A meta-analysis. Eur. J. Clin. Investig. 2018, 49, e13063. [Google Scholar] [CrossRef]
- Sengupta, S.; Krishnan, M.A.; Chattopadhyay, S.; Chelvam, V. Comparison of prostate-specific membrane antigen ligands in clinical translation research for diagnosis of prostate cancer. Cancer Rep. 2019, 2, e1169. [Google Scholar] [CrossRef]
- Eiber, M.; Fendler, W.P.; Rowe, S.P.; Calais, J.; Hofman, M.S.; Maurer, T.; Schwarzenboeck, S.M.; Kratowchil, C.; Herrmann, K.; Giesel, F.L. Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy. J. Nucl. Med. 2017, 58, 67S–76S. [Google Scholar] [CrossRef] [Green Version]
- Gourni, E.; Henriksen, G. Metal-Based PSMA Radioligands. Molecules 2017, 22, 523. [Google Scholar] [CrossRef] [Green Version]
- Czarniecki, M.; Mena, E.; Lindenberg, L.; Cacko, M.; Harmon, S.; Radtke, J.P.; Giesel, F.; Turkbey, B.; Choyke, P.L. Keeping up with the prostate-specific membrane antigens (PSMAs): An introduction to a new class of positron emission tomography (PET) imaging agents. Transl. Androl. Urol. 2018, 7, 831–843. [Google Scholar] [CrossRef]
- Zippel, C.; Ronski, S.C.; Bohnet-Joschko, S.; Giesel, F.L.; Kopka, K. Current Status of PSMA-Radiotracers for Prostate Cancer: Data Analysis of Prospective Trials Listed on ClinicalTrials.gov. Pharmaceuticals 2020, 13, 12. [Google Scholar] [CrossRef] [Green Version]
- Pastorino, S.; Riondato, M.; Uccelli, L.; Giovacchini, G.; Giovannini, E.; Duce, V.; Ciarmiello, A. Toward the Discovery and Development of PSMA Targeted Inhibitors for Nuclear Medicine Applications. Curr. Radiopharm. 2020, 13, 63–79. [Google Scholar] [CrossRef]
- Wester, H.-J.; Schottelius, M. PSMA-Targeted Radiopharmaceuticals for Imaging and Therapy. Semin. Nucl. Med. 2019, 49, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Foley, R.; Redman, S.; Graham, R.; Loughborough, W.; Little, D. Fluorine-18 labelled prostate-specific membrane antigen (PSMA)-1007 positron-emission tomography–computed tomography: Normal patterns, pearls, and pitfalls. Clin. Radiol. 2020, 75, 903–913. [Google Scholar] [CrossRef]
- Cardinale, J.; Schäfer, M.; Benešová, M.; Bauder-Wüst, U.; Leotta, K.; Eder, M.; Neels, O.C.; Haberkorn, U.; Giesel, F.L.; Kopka, K. Preclinical Evaluation of 18 F-PSMA-1007, a New Prostate-Specific Membrane Antigen Ligand for Prostate Cancer Imaging. J. Nucl. Med. 2016, 58, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Treglia, G.; Annunziata, S.; Pizzuto, D.A.; Giovanella, L.; Prior, J.O.; Ceriani, L. Detection Rate of 18F-Labeled PSMA PET/CT in Biochemical Recurrent Prostate Cancer: A Systematic Review and a Meta-Analysis. Cancers 2019, 11, 710. [Google Scholar] [CrossRef] [Green Version]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; the PRISMA-DTA Group. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, R.; Treglia, G. Systematic reviews and meta-analyses of diagnostic studies: A practical guideline. Clin. Transl. Imaging 2017, 5, 83–87. [Google Scholar] [CrossRef]
- Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 31 December 2020).
- Anttinen, M.; Ettala, O.; Malaspina, S.; Jambor, I.; Sandell, M.; Kajander, S.; Rinta-Kiikka, I.; Schildt, J.; Saukko, E.; Rautio, P.; et al. A Prospective Comparison of 18F-prostate-specific Membrane Antigen-1007 Positron Emission Tomography Computed Tomography, Whole-body 1.5 T Magnetic Resonance Imaging with Diffusion-weighted Imaging, and Single-photon Emission Computed Tomography/Computed Tomography with Traditional Imaging in Primary Distant Metastasis Staging of Prostate Cancer (PROSTAGE). Eur. Urol. Oncol. 2020. [Google Scholar] [CrossRef]
- Giesel, F.L.; Hadaschik, B.; Cardinale, J.; Radtke, J.; Vinsensia, M.; Lehnert, W.; Kesch, C.; Tolstov, Y.; Singer, S.; Grabe, N.; et al. F-18 labelled PSMA-1007: Biodistribution, radiation dosimetry and histopathological validation of tumor lesions in prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 678–688. [Google Scholar] [CrossRef] [Green Version]
- Giesel, F.L.; Will, L.; Lawal, I.; Lengana, T.; Kratochwil, C.; Vorster, M.; Neels, O.; Reyneke, F.; Haberkorn, U.; Kopka, K.; et al. Intraindividual Comparison of 18F-PSMA-1007 and 18F-DCFPyL PET/CT in the Prospective Evaluation of Patients with Newly Diagnosed Prostate Carcinoma: A Pilot Study. J. Nucl. Med. 2018, 59, 1076–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, J.-J.; Liu, B.-L.; Wang, Z.-Q.; Tang, K.; Ji, X.-W.; Yin, W.-W.; Lin, J.; Zheng, X.-W. The value of 18F-PSMA-1007 PET/CT in identifying non-metastatic high-risk prostate cancer. EJNMMI Res. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Kesch, C.; Vinsensia, M.; Radtke, J.P.; Schlemmer, H.P.; Heller, M.; Ellert, E.; Holland-Letz, T.; Duensing, S.; Grabe, N.; Afshar-Oromieh, A.; et al. Intraindividual Comparison of 18F-PSMA-1007 PET/CT, Multiparametric MRI, and Radical Prostatectomy Specimens in Patients with Primary Prostate Cancer: A Retrospective, Proof-of-Concept Study. J. Nucl. Med. 2017, 58, 1805–1810. [Google Scholar] [CrossRef] [Green Version]
- Kuten, J.; Fahoum, I.; Savin, Z.; Shamni, O.; Gitstein, G.; Hershkovitz, D.; Mabjeesh, N.J.; Yossepowitch, O.; Mishani, E.; Even-Sapir, E. Head-to-Head Comparison of 68Ga-PSMA-11 with 18F-PSMA-1007 PET/CT in Staging Prostate Cancer Using Histopathology and Immunohistochemical Analysis as a Reference Standard. J. Nucl. Med. 2019, 61, 527–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Privé, B.M.; Israël, B.; Schilham, M.G.M.; Muselaers, C.H.J.; Zámecnik, P.; Mulders, P.F.A.; Witjes, J.A.; Sedelaar, M.; Mehra, N.; Verzijlbergen, F.; et al. Evaluating F-18-PSMA-1007-PET in primary prostate cancer and comparing it to multi-parametric MRI and histopathology. Prostate Cancer Prostatic Dis. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sprute, K.; Kramer, V.; Koerber, S.A.; Meneses, M.; Fernandez, R.; Soza-Ried, C.; Eiber, M.; Weber, W.A.; Rauscher, I.; Rahbar, K.; et al. Diagnostic Accuracy of 18F-PSMA-1007 PET/CT Imaging for Lymph Node Staging of Prostate Carcinoma in Primary and Biochemical Recurrence. J. Nucl. Med. 2021, 62, 208–213. [Google Scholar] [CrossRef]
- Treglia, G.; Sadeghi, R. Meta-analyses and systematic reviews on PET and PET/CT in oncology: The state of the art. Clin. Transl. Imaging 2013, 1, 73–75. [Google Scholar] [CrossRef] [Green Version]
- Rahbar, K.; Afshar-Oromieh, A.; Seifert, R.; Wagner, S.; Schäfers, M.; Bögemann, M.; Weckesser, M. Do fasting or high caloric drinks affect the physiological uptake of fluorine-18 prostate-specific membrane antigen-1007 in liver and bowel? World J. Nucl. Med. 2020, 19, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Crespo, A. Comparison of Gallium-68 and Fluorine-18 imaging characteristics in positron emission tomography. Appl. Radiat. Isot. 2013, 76, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Bunka, M.; Müller, C.; Vermeulen, C.; Haller, S.; Türler, A.; Schibli, R.; van der Meulen, N.P. Imaging quality of 44Sc in comparison with five other PET radionuclides using Derenzo phantoms and preclinical PET. Appl. Radiat. Isot. 2016, 110, 129–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mottet, N.; Bergh, R.C.V.D.; Briers, E.; Broeck, T.V.D.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer—2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Year | Country | Study Design | Type Of Patients Evaluated | PCa Patients Performing 18F-PSMA-1007 PET/CT | Mean/Median Age (Years) | Gleason Score (Percentage) | Median PSA Values Before PET/CT (ng/ml) (Range) |
|---|---|---|---|---|---|---|---|---|
| Anttinen et al. [24] | 2020 | Finland | Prospective single-center | Patients with high-risk PCa at staging | 80 | Mean: 70 ± 7 | GS 6: 3 (4%) GS 7: 30 (37%) GS 8: 13 (16%) GS 9–10: 34 (43%) | 12 (3–2000) |
| Giesel et al. [25] | 2017 | Germany | Retrospective single-center | Patients with high-risk PCa at staging | 10 | Median: 65 (55–77) | GS 7: 3 (30%) GS 8: 2 (20%) GS 9: 5 (50%) | 14 (5.8–87.3) |
| Giesel et al. [26] | 2018 | Germany and South Africa | Prospective bicentric | Patients with PCa at staging | 12 | Median: 66 (54–82) | GS 6: 1 (8%) GS 7: 5 (42%) GS 8: 4 (33%) GS 9: 2 (17%) | 85 (10–279.8) |
| Hong et al. [27] | 2020 | China | Retrospective single-center | Patients with non-metastatic intermediate- or high-risk PCa at staging | 101 | Median: 69 (43–87) | GS 6: 4 (4%) GS 7: 67 (66%) GS 8: 9 (9%) GS 9: 21 (21%) | 11.1 (0.97–178.2) |
| Kesch et al. [28] | 2017 | Germany | Retrospective single-center | Patients with high-risk PCa at local staging | 10 | Median: 67 (55–77) | GS 7: 3 (30%) GS 9: 7 (70%) | 13.1 (5.8–40) |
| Kuten et al. [29] | 2020 | Israel | Prospective single-center | Patients with intermediate- or high-risk PCa at staging | 16 | Median: 68 (56–74) | GS 6: 2 (12%) GS 7: 11 (69%) GS 8: 3 (19%) | 6.35 (3.5–14.44) |
| Privé et al. [30] | 2020 | Netherlands | Retrospective single-center | Patients with intermediate- or high-risk PCa at staging | 53 | Median: 67 | GS 6: 5 (9%) GS 7: 19 (36%) GS 8: 12 (23%) GS 9–10: 17 (32%) | 12 |
| Sprute et al. [31] | 2020 | Germany, Chile, Japan | Retrospective multicenter | Patients with PCa at staging | 87 | Median: 69 (48–78) | GS 6: 3% GS 7: 60% GS 8: 7% GS 9: 30% | 11.7 (0.1–120) |
| Authors | Hybrid Imaging Modality | Fasting/Hydration before Radiotracer Injection | Mean Radiotracer Injected Activity (MBq) (Range) | Time Interval between Radiotracer Injection and Image Acquisition (Minutes) | PET/CT Scan Extension | Image Analysis | Other Imaging Performed for Comparison |
|---|---|---|---|---|---|---|---|
| Anttinen et al. [24] | PET/CT with low-dose CT | NR/NR | 263 ± 27 (205–355) | 60 | From vertex to mid-thigh | visual and semi-quantitative (SUVmax) | Planar scintigraphy and SPECT/CT with 99mTc-diphosphonates, CT, WBMRI with DWI |
| Giesel et al. [25] | PET/CT with low-dose CT | NR/NR | 275 (111–356) | 60 + 180 | NR | visual and semi-quantitative (SUVmax) | – |
| Giesel et al. [26] | PET/CT with low-dose CT | 4 h/NR | 240–260 | 120 | From vertex to thighs | visual and semi-quantitative (SUVmax) | 18F-DCFPyL PET/CT |
| Hong et al. [27] | PET/CT with low-dose CT | NR/NR | 4 MBq/kg; 291 (185–366) | 120 | From skull base to mid-thigh | visual and semi-quantitative (SUVmax) | – |
| Kesch et al. [28] | PET/CT with low-dose CT | NR/NR | NR | 60 + 180 | NR | visual and semi-quantitative (SUVmax) | multi-parametric MRI |
| Kuten et al. [29] | PET/CT with low-dose CT | NR/yes | 4 MBq/kg | 60 | From vertex to mid-thigh | visual and semi-quantitative (SUVmax) | 68Ga-PSMA-11 PET/CT |
| Privé et al. [30] | PET/CT with contrast enhanced CT | NR/yes | ~250 | 90 ± 10 | NR | visual and semi-quantitative (SUVmax) | multi-parametric MRI |
| Sprute et al. [31] | PET/CT with low-dose CT | NR/NR | 270 | 90 (47–169) | NR | visual and semi-quantitative (SUVmax) | – |
| Authors | Reference Standard | Patient-Based Analysis | Lesion-Based Analysis | Change of Management by Using PET/CT | Study Quality * | Study Summary | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sensitivity | Specificity | Accuracy | Sensitivity | Specificity | Accuracy | |||||
| Anttinen et al. [24] *** | The reference standard diagnosis was defined using all available information accrued during at least 12 months of clinical follow-up | 86–95% | 76–90% | 80–89% | 72–86% | NR | NR | 14/79 (18%) | fair | 18F-PSMA-1007 PET/CT has superior sensitivity and the highest inter-reader agreement compared with standard and advanced imaging modalities for PCa staging. |
| Giesel et al. [25] | NR | 100% | 100% | 100% | 95% | 100% | NR | NR | fair | 18F-PSMA-1007 PET/CT has high sensitivity in detecting PCa lesions. |
| Giesel et al. [26] | NR | 100% | NR | NR | NR | NR | NR | NR | fair | Excellent imaging quality and concordance are achieved with both 18F-DCFPyL and 18F-PSMA-1007. |
| Hong et al. [27] *** | Histology | NR | NR | NR | NR | NR | NR | NR | fair | There is a significant positive correlation between PSA level/GS and SUVmax at 18F-PSMA-1007 PET/CT. |
| Kesch et al. [28] | Histology and mpMRI | 100% | NR | NR | 93% | 92% | 93% | NR | fair | Comparison with histopathology demonstrates that 18F-PSMA-1007 PET/CT is promising for accurate local staging of PCa. |
| Kuten et al. [29] | Histology | 100% | NR | NR | 100% | 91% | 95% | NR | fair | Both 18F-PSMA-1007 and 68Ga-PSMA-11 PET/CT may identify all dominant prostatic lesions in patients with PCa at staging. 18F-PSMA-1007 may detect additional lesions of limited clinical relevance. |
| Privé et al. [30] *** | Histology and mpMRI | 98% | NR | NR | NR | NR | NR | NR | fair | Dual imaging with mpMRI and 18F-PSMA-1007 PET/CT may improve staging of primary PCa. Higher PCa aggressiveness was associated with higher SUVmax at 18F-PSMA-1007 PET/CT. |
| Sprute et al. [31] *** | Histology | 74% ** | 99% ** | NR | 71% ** | 99.5% ** | NR | NR | fair | 18F-PSMA-1007 PET/CT reliably detects PCa lymph nodal metastases with very high specificity. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Awenat, S.; Piccardo, A.; Carvoeiras, P.; Signore, G.; Giovanella, L.; Prior, J.O.; Treglia, G. Diagnostic Role of 18F-PSMA-1007 PET/CT in Prostate Cancer Staging: A Systematic Review. Diagnostics 2021, 11, 552. https://doi.org/10.3390/diagnostics11030552
Awenat S, Piccardo A, Carvoeiras P, Signore G, Giovanella L, Prior JO, Treglia G. Diagnostic Role of 18F-PSMA-1007 PET/CT in Prostate Cancer Staging: A Systematic Review. Diagnostics. 2021; 11(3):552. https://doi.org/10.3390/diagnostics11030552
Chicago/Turabian StyleAwenat, Salam, Arnoldo Piccardo, Patricia Carvoeiras, Giovanni Signore, Luca Giovanella, John O. Prior, and Giorgio Treglia. 2021. "Diagnostic Role of 18F-PSMA-1007 PET/CT in Prostate Cancer Staging: A Systematic Review" Diagnostics 11, no. 3: 552. https://doi.org/10.3390/diagnostics11030552