
MR-Imaging and Histopathological Diagnostic Work-Up of Patients with Spontaneous Lobar Intracerebral Hemorrhage: Results of an Institutional Prospective Registry Study

 ,
,  , , ,
, , ,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
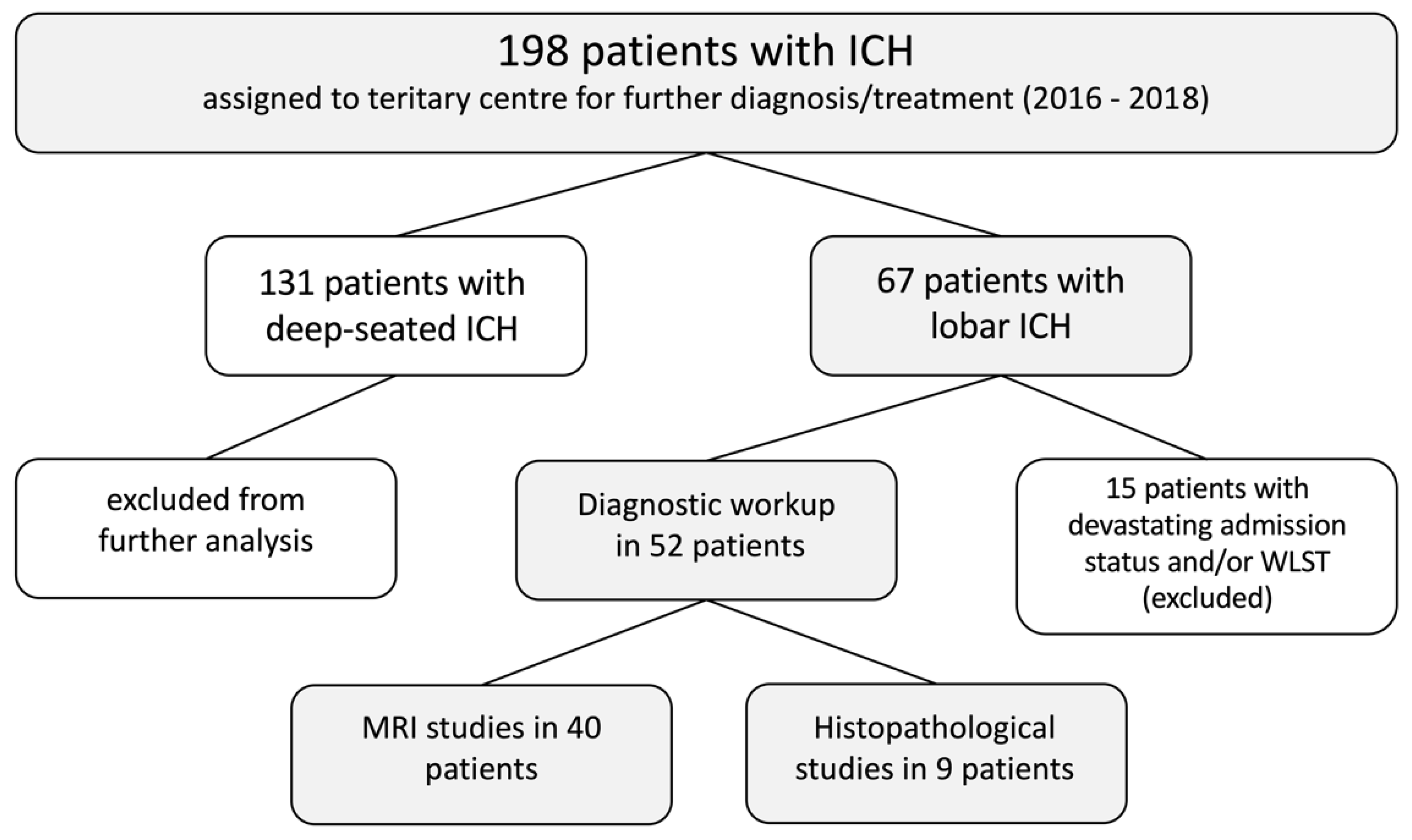
2.1. ICH Registry Study
2.2. Radiological Study
2.3. Treatment of ICH
2.4. Histopathological Study
2.5. Inclusion Criteria
3. Results
3.1. Treatment of ICH
3.2. Etiology of ICH
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Lawes, C.M.; Bennett, D.A.; Barker-Collo, S.L.; Parag, V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: A systematic review. Lancet Neurol. 2009, 8, 355–369. [Google Scholar] [CrossRef]
- Wasserman, J.K.; Yang, H.; Schlichter, L.C. Glial responses, neuron death and lesion resolution after intracerebral hemorrhage in young vs. aged rats. Eur. J. Neurosci. 2008, 28, 1316–1328. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.; Xiang, J.; Wu, P.; Su, J.; Ding, H.; Tang, Y.; Dong, Q. The role of aquaporin 4 in apoptosis after intracerebral hemorrhage. J. Neuroinflammation 2014, 11, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitchen, P.; Salman, M.M.; Halsey, A.M.; Clarke-Bland, C.; Macdonald, J.A.; Ishida, H.; Vogel, H.J.; Almutiri, S.; Logan, A.; Kreida, S.; et al. Targeting Aquaporin-4 Subcellular Localization to Treat Central Nervous System Edema. Cell 2020, 181, 784–799.e19. [Google Scholar] [CrossRef]
- Manoel, A.L.D.O. Surgery for spontaneous intracerebral hemorrhage. Crit. Care 2020, 24, 45. [Google Scholar] [CrossRef] [Green Version]
- Fahlström, A.; Redebrandt, H.N.; Zeberg, H.; Bartek, J.; Bartley, A.; Tobieson, L.; Erkki, M.; Hessington, A.; Troberg, E.; Mirza, S.; et al. A grading scale for surgically treated patients with spontaneous supratentorial intracerebral hemorrhage: The Surgical Swedish ICH Score. J. Neurosurg. 2020, 133, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Balasa, A.; Ghiga, D.; Andone, R.-S.; Zahan, A.E.; Florian, I.A.; Chinezu, R. Effects of Surgery on the 30-Day Survival Rate in Spontaneous Supratentorial Intracerebral Hemorrhage. Brain Sci. 2020, 11, 5. [Google Scholar] [CrossRef]
- Hadjiathanasiou, A.; Schuss, P.; Ilic, I.; Borger, V.; Vatter, H.; Güresir, E. Decompressive craniectomy for intracerebral haematoma: The influence of additional haematoma evacuation. Neurosurg. Rev. 2018, 41, 649–654. [Google Scholar] [CrossRef]
- Hessington, A.; Tsitsopoulos, P.P.; Fahlström, A.; Marklund, N. Favorable clinical outcome following surgical evacuation of deep-seated and lobar supratentorial intracerebral hemorrhage: A retrospective single-center analysis of 123 cases. Acta Neurochir. 2018, 160, 1737–1747. [Google Scholar] [CrossRef] [Green Version]
- Brott, T.; Thalinger, K.; Hertzberg, V. Hypertension as a risk factor for spontaneous intracerebral hemorrhage. Stroke 1986, 17, 1078–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohtani, R.; Kazui, S.; Tomimoto, H.; Minematsu, K.; Naritomi, H. Clinical and Radiographic Features of Lobar Cerebral Hemorrhage: Hypertensive Versus Non-hypertensive Cases. Intern. Med. 2003, 42, 576–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuss, P.; Hadjiathanasiou, A.; Ilic, I.; Brandecker, S.; Güresir, Á.; Vatter, H.; Güresir, E. Risk of Rebleeding in Patients Suffering From Ruptured Brain Arteriovenous Malformations Undergoing Subacute Treatment: A Single-Center Series and Systematic Review of the Literature. World Neurosurg. 2020, 134, e610–e615. [Google Scholar] [CrossRef]
- Hilkens, N.A.; Van Asch, C.J.J.; Werring, D.J.; Wilson, D.E.; Rinkel, G.J.; Algra, A.; Velthuis, B.K.; Kort, G.A.P.D.; Witkamp, T.D.; Van Nieuwenhuizen, K.M.; et al. Predicting the presence of macrovascular causes in non-traumatic intracerebral haemorrhage: The DIAGRAM prediction score. J. Neurol. Neurosurg. Psychiatry 2018, 89, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.E.; Rosand, J.; Greenberg, S.M. Imaging of hemorrhagic stroke. Magn. Reson. Imaging Clin. N. Am. 2006, 14, 127–140. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Samarasekera, N.; Fonville, A.; Lerpiniere, C.; Farrall, A.J.; Wardlaw, J.M.; White, P.M.; Smith, C.; Salman, R.A.-S.; Addison, A.; Ahmad, K.; et al. Influence of Intracerebral Hemorrhage Location on Incidence, Characteristics, and Outcome. Stroke 2015, 46, 361–368. [Google Scholar] [CrossRef] [Green Version]
- Kothari, R.U.; Brott, T.; Broderick, J.P.; Barsan, W.G.; Sauerbeck, L.R.; Zuccarello, M.; Khoury, J. The ABCs of Measuring Intracerebral Hemorrhage Volumes. Stroke 1996, 27, 1304–1305. [Google Scholar] [CrossRef] [PubMed]
- Hemphill, J.C.; Greenberg, S.M.; Anderson, C.S.; Becker, K.; Bendok, B.R.; Cushman, M.; Fung, G.L.; Goldstein, J.N.; Macdonald, R.L.; Mitchell, P.H.; et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage. Stroke 2015, 46, 2032–2060. [Google Scholar] [CrossRef] [Green Version]
- Schuss, P.; Hadjiathanasiou, A.; Brandecker, S.; Güresir, Á.; Borger, V.; Wispel, C.; Vatter, H.; Güresir, E. Anticoagulation Therapy in Patients Suffering from Aneurysmal Subarachnoid Hemorrhage: Influence on Functional Outcome—a Single-Center Series and Multivariate Analysis. World Neurosurg. 2017, 99, 348–352. [Google Scholar] [CrossRef]
- Kirollos, R.W.; Tyagi, A.K.; Ross, S.A.; Van Hille, P.T.; Marks, P.V. Management of Spontaneous Cerebellar Hematomas: A Prospective Treatment Protocol. Neurosurgery 2001, 49, 1378–1387. [Google Scholar] [CrossRef] [Green Version]
- Schuss, P.; Marx, J.; Borger, V.; Brandecker, S.; Güresir, Á.; Hadjiathanasiou, A.; Hamed, M.; Schneider, M.; Surges, R.; Vatter, H.; et al. Cavernoma-related epilepsy in cavernous malformations located within the temporal lobe: Surgical management and seizure outcome. Neurosurg. Focus 2020, 48, E6. [Google Scholar] [CrossRef] [Green Version]
- Schneider, M.; Potthoff, A.-L.; Keil, V.C.; Güresir, Á.; Weller, J.; Borger, V.; Hamed, M.; Waha, A.; Vatter, H.; Güresir, E.; et al. Surgery for temporal glioblastoma: Lobectomy outranks oncosurgical-based gross-total resection. J. Neuro Oncol. 2019, 145, 143–150. [Google Scholar] [CrossRef]
- Hemphill, J.C.; Bonovich, D.C.; Besmertis, L.; Manley, G.T.; Johnston, S.C. The ICH Score. Stroke 2001, 32, 891–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thabet, A.; Kottapally, M.; Hemphill, J.C. Management of intracerebral hemorrhage. Handb. Clin. Neurol. 2017, 140, 177–194. [Google Scholar] [CrossRef]
- Zhu, H.; Wang, Z.; Yu, J.; Yang, X.; He, F.; Liu, Z.; Che, F.; Chen, X.; Ren, H.; Hong, M.; et al. Role and mechanisms of cytokines in the secondary brain injury after intracerebral hemorrhage. Prog. Neurobiol. 2019, 178, 101610. [Google Scholar] [CrossRef] [PubMed]
- Kaur, P.; Radotra, B.; Minz, R.W.; Gill, K.D. Impaired mitochondrial energy metabolism and neuronal apoptotic cell death after chronic dichlorvos (OP) exposure in rat brain. NeuroToxicology 2007, 28, 1208–1219. [Google Scholar] [CrossRef]
- Liu, T.; Zhou, J.; Cui, H.; Li, P.; Li, H.; Wang, Y.; Tang, T. Quantitative proteomic analysis of intracerebral hemorrhage in rats with a focus on brain energy metabolism. Brain Behav. 2018, 8, e01130. [Google Scholar] [CrossRef] [Green Version]
- Bordone, M.P.; Salman, M.M.; Titus, H.E.; Amini, E.; Andersen, J.V.; Chakraborti, B.; Diuba, A.V.; Dubouskaya, T.G.; Ehrke, E.; De Freitas, A.E.; et al. The energetic brain—A review from students to students. J. Neurochem. 2019, 151, 139–165. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Wu, T.; Xu, X.; Wang, J.; Wang, J. Iron Toxicity in Mice with Collagenase-Induced Intracerebral Hemorrhage. Br. J. Pharmacol. 2010, 31, 1243–1250. [Google Scholar] [CrossRef]
- Wang, J. Preclinical and clinical research on inflammation after intracerebral hemorrhage. Prog. Neurobiol. 2010, 92, 463–477. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, M.J.; Xavier, D.; Liu, L.; Zhang, H.; Chin, S.L.; Rao-Melacini, P.; Rangarajan, S.; Islam, S.; Pais, P.; McQueen, M.J.; et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): A case-control study. Lancet 2010, 376, 112–123. [Google Scholar] [CrossRef]
- Jackson, C.; Sudlow, C.L.M. Is hypertension a more frequent risk factor for deep than for lobar supratentorial intracerebral haemorrhage? J. Neurol. Neurosurg. Psychiatry 2006, 77, 1244–1252. [Google Scholar] [CrossRef] [Green Version]
- Lovelock, C.E.; Molyneux, A.J.; Rothwell, P.M. Change in incidence and aetiology of intracerebral haemorrhage in Oxfordshire, UK, between 1981 and 2006: A population-based study. Lancet Neurol. 2007, 6, 487–493. [Google Scholar] [CrossRef]
- Wakai, S.; Kumakura, N.; Nagai, M. Lobar intracerebral hemorrhage. J. Neurosurg. 1992, 76, 231–238. [Google Scholar] [CrossRef]
- Qureshi, A.I.; Tuhrim, S.; Broderick, J.P.; Batjer, H.H.; Hondo, H.; Hanley, D.F. Spontaneous Intracerebral Hemorrhage. N. Engl. J. Med. 2001, 344, 1450–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knudsen, K.A.; Rosand, J.; Karluk, D.; Greenberg, S.M. Clinical diagnosis of cerebral amyloid angiopathy: Validation of the Boston Criteria. Neurology 2001, 56, 537–539. [Google Scholar] [CrossRef]
- Linn, J.; Halpin, A.; Demaerel, P.; Ruhland, J.; Giese, A.D.; Dichgans, M.; Van Buchem, M.A.; Bruckmann, H.; Greenberg, S.M. Prevalence of superficial siderosis in patients with cerebral amyloid angiopathy. Neurology 2010, 74, 1346–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meretoja, A.; Strbian, D.; Putaala, J.; Curtze, S.; Haapaniemi, E.; Mustanoja, S.; Sairanen, T.; Satopää, J.; Silvennoinen, H.; Niemelä, M.; et al. SMASH-U. Stroke 2012, 43, 2592–2597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen-Kondering, U.R.; Weiler, C.; Langguth, P.; Larsen, N.; Flüh, C.; Kuhlenbäumer, G.; Jansen, O.; Margraf, N.G. Clinical and radiological differences between patients with probable cerebral amyloid angiopathy and mixed cerebral microbleeds. J. Neurol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Domingues, R.; Rossi, C.; Cordonnier, C. Diagnostic Evaluation for Nontraumatic Intracerebral Hemorrhage. Neurol. Clin. 2015, 33, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Van Asch, C.J.; Velthuis, B.K.; Rinkel, G.J.; Algra, A.; Kort, G.A.P.D.; Witkamp, T.D.; De Ridder, J.C.; Van Nieuwenhuizen, K.M.; De Leeuw, F.-E.; Schonewille, W.J.; et al. Diagnostic yield and accuracy of CT angiography, MR angiography, and digital subtraction angiography for detection of macrovascular causes of intracerebral haemorrhage: Prospective, multicentre cohort study. BMJ 2015, 351, h5762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hostettler, I.C.; Seiffge, D.J.; Werring, D.J. Intracerebral hemorrhage: An update on diagnosis and treatment. Expert Rev. Neurother. 2019, 19, 679–694. [Google Scholar] [CrossRef] [PubMed]
- Steiner, T.; Petersson, J.; Salman, R.A.-S.; Christensen, H.; Cordonnier, C.; Csiba, L.; Harnof, S.; Krieger, D.; Mendelow, D.; Molina, C.; et al. European research priorities for intracerebral haemorrhage. Cerebrovasc. Dis. 2011, 32, 409–419. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patients with Lobar ICH (n = 52) | |
|---|---|
| Mean age (±SD; yrs) | 61 ± 15 |
| Female sex | 28 (54%) |
| Anticoagulation medication prior ictus | 5 (10%) |
| NOAC medication prior ictus | 2 (4%) |
| Antiplatelet medication prior ictus | 9 (17%) |
| Comorbidities | |
| Hypertension | 22 (42%) |
| Coronary artery disease | 6 (11%) |
| Diabetes mellitus | 7 (13%) |
| Treatment of ICH | |
| Best medical treatment w/o any surgical therapy | 30 (58%) |
| Surgical treatment | 22 (42%) |
| EVD w/o further surgical procedures | 1 (2%) |
| Stereotactic aspiration | 3 (6%) |
| Craniotomy with ICH evacuation | 2 (4%) |
| DC w/o ICH evacuation | 10 (19%) |
| DC with ICH evacuation | 6 (11%) |
| Patients with Lobar ICH (n = 52) | |
|---|---|
| Macrovascular disease-related ICH | 14 (27%) |
| Ruptured intracranial aneurysm | 7 (13%) |
| Ruptured BAVM | 2 (4%) |
| Ruptured DAVF | 2 (4%) |
| Acute sinus venous thrombosis | 2 (4%) |
| Cerebral cavernous malformation | 1 (2%) |
| CAA-related ICH | 11 (21%) |
| Tumor-related ICH | 5 (10%) |
| Glioblastoma | 2 (4%) |
| Oligodendroglioma | 1 (2%) |
| Intracranial metastasis | 2 (4%) |
| Infectious embolic disease-related ICH | 6 (11%) |
| Unknown cause | 4 (8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schuss, P.; Bode, C.; Borger, V.; Coch, C.; Güresir, Á.; Hadjiathanasiou, A.; Hamed, M.; Kuchelmeister, K.; Lehmann, F.; Müller, M.; et al. MR-Imaging and Histopathological Diagnostic Work-Up of Patients with Spontaneous Lobar Intracerebral Hemorrhage: Results of an Institutional Prospective Registry Study. Diagnostics 2021, 11, 368. https://doi.org/10.3390/diagnostics11020368
Schuss P, Bode C, Borger V, Coch C, Güresir Á, Hadjiathanasiou A, Hamed M, Kuchelmeister K, Lehmann F, Müller M, et al. MR-Imaging and Histopathological Diagnostic Work-Up of Patients with Spontaneous Lobar Intracerebral Hemorrhage: Results of an Institutional Prospective Registry Study. Diagnostics. 2021; 11(2):368. https://doi.org/10.3390/diagnostics11020368
Chicago/Turabian StyleSchuss, Patrick, Christian Bode, Valeri Borger, Christoph Coch, Ági Güresir, Alexis Hadjiathanasiou, Motaz Hamed, Klaus Kuchelmeister, Felix Lehmann, Marcus Müller, and et al. 2021. "MR-Imaging and Histopathological Diagnostic Work-Up of Patients with Spontaneous Lobar Intracerebral Hemorrhage: Results of an Institutional Prospective Registry Study" Diagnostics 11, no. 2: 368. https://doi.org/10.3390/diagnostics11020368