
Early Confirmation of Mycoplasma pneumoniae Infection by Two Short-Term Serologic IgM Examination

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Study Definitions
2.3. Study Design
2.4. Statistical Analysis
3. Results
3.1. Demographic, Clinical, and Laboratory Findings
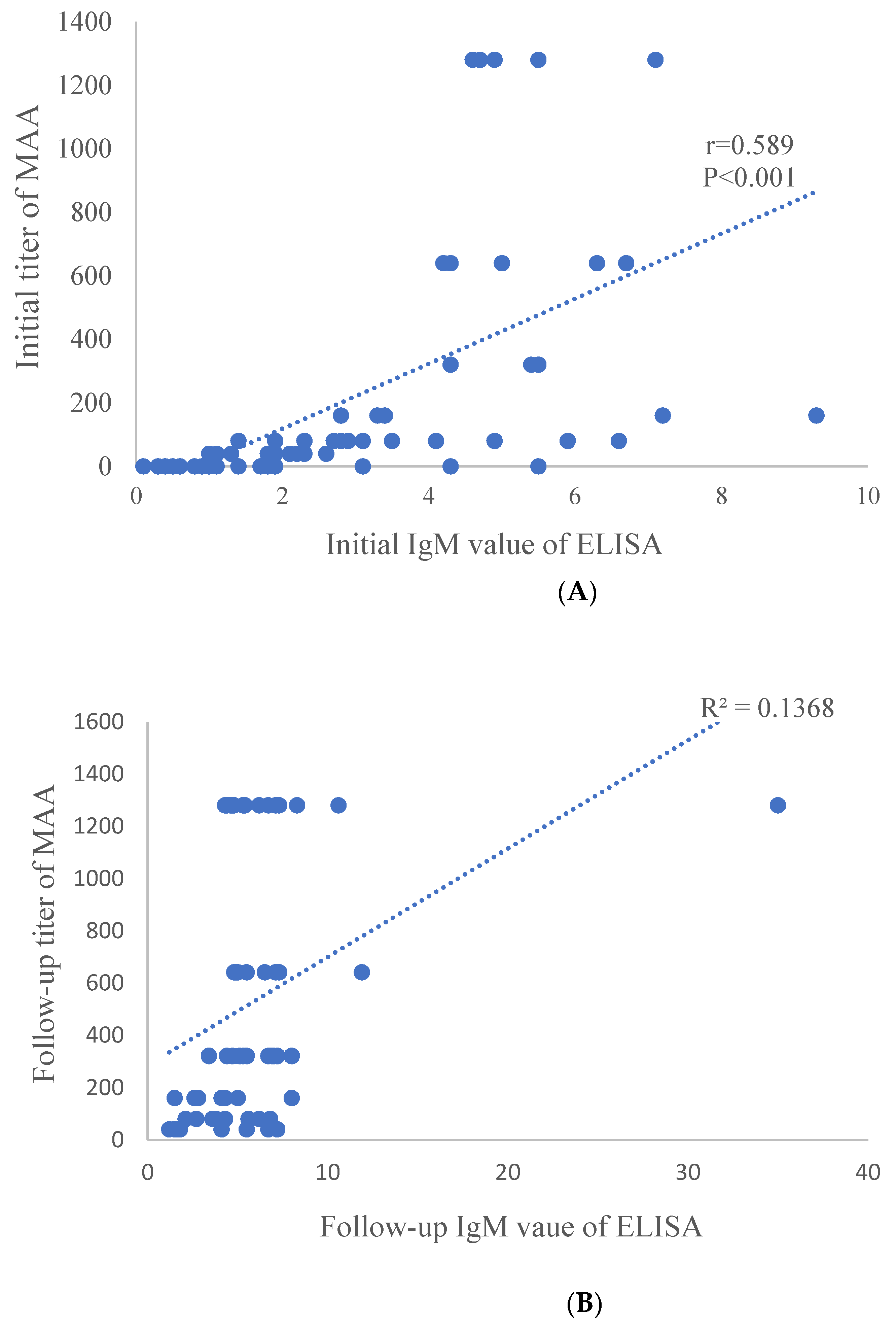
3.2. Comparison between MAA and ELISA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MP | Mycoplasma pneumoniae |
| MAA | microparticle agglutination assay |
| ELISA | enzyme-linked immunosorbent assays |
| PCR | polymerase chain reaction |
| IgM | immunoglobulin M |
References
- Lee, K.-Y. Pediatric respiratory infections by Mycoplasma pneumoniae. Expert Rev. Anti-Infect. Ther. 2008, 6, 509–521. [Google Scholar] [CrossRef]
- Eun, B.W.; Kim, N.H.; Choi, E.H.; Lee, H.J. Mycoplasma pneumoniae in Korean children: The epidemiology of pneumonia over an 18-year period. J. Infect. 2008, 56, 326–331. [Google Scholar] [CrossRef]
- Kim, E.-K.; Youn, Y.-S.; Rhim, J.-W.; Shin, M.-S.; Kang, J.-H.; Lee, K.-Y. Epidemiological comparison of threeMycoplasma pneumoniaepneumonia epidemics in a single hospital over 10 years. Korean J. Pediatr. 2015, 58, 172–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, S.Y.; Jwa, H.J.; Yang, E.A.; Kil, H.R.; Lee, J.H. Effects of Methylprednisolone Pulse Therapy on Refractory Mycoplasma pneumoniae Pneumonia in Children. Allergy Asthma Immunol. Res. 2014, 6, 22–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Zhou, Y.; Li, S.; Yang, D.; Wu, X.; Chen, Z. The Clinical Characteristics and Predictors of Refractory Mycoplasma pneumoniae Pneumonia in Children. PLoS ONE 2016, 11, e0156465. [Google Scholar] [CrossRef] [Green Version]
- Giulia, B.; Luisa, A.; Concetta, S.; Bruna, L.S.; Chiara, B.; Marcello, C. Procalcitonin and community-acquired pneumonia (CAP) in children. Clin. Chim. Acta 2015, 451, 215–218. [Google Scholar] [CrossRef] [Green Version]
- Agnello, L.; Bellia, C.; Di Gangi, M.; Sasso, B.L.; Calvaruso, L.; Bivona, G.; Scazzone, C.; Dones, P.; Ciaccio, M. Utility of serum procalcitonin and C-reactive protein in severity assessment of community-acquired pneumonia in children. Clin. Biochem. 2016, 49, 47–50. [Google Scholar] [CrossRef]
- Jeong, J.E.; Soh, J.E.; Kwak, J.H.; Jung, H.L.; Shim, J.W.; Kim, D.S.; Park, M.S.; Shim, J.Y. Increased procalcitonin level is a risk factor for prolonged fever in children with Mycoplasma pneumonia. Korean J. Pediatr. 2018, 61, 258–263. [Google Scholar] [CrossRef]
- Dorigo-Zetsma, J.W.; Zaat, S.A.J.; Dillen, P.M.E.W.-V.; Spanjaard, L.; Rijntjes, J.; Van Waveren, G.; Jensen, J.S.; Angulo, A.F.; Dankert, J. Comparison of PCR, Culture, and Serological Tests for Diagnosis of Mycoplasma pneumoniae Respiratory Tract Infection in Children. J. Clin. Microbiol. 1999, 37, 14–17. [Google Scholar] [CrossRef] [Green Version]
- Räty, R.; Rönkkö, E.; Kleemola, M. Sample type is crucial to the diagnosis of Mycoplasma pneumoniae pneumonia by PCR. J. Med. Microbiol. 2005, 54, 287–291. [Google Scholar] [CrossRef] [Green Version]
- Thurman, K.A.; Walter, N.D.; Schwartz, S.B.; Mitchell, S.L.; Dillon, M.T.; Baughman, A.L.; Deutscher, M.; Fulton, J.P.; Tongren, J.E.; Hicks, L.A.; et al. Comparison of Laboratory Diagnostic Procedures for Detection of Mycoplasma pneumoniaein Community Outbreaks. Clin. Infect. Dis. 2009, 48, 1244–1249. [Google Scholar] [CrossRef] [Green Version]
- Dorigo-Zetsma, J.W.; Wilbrink, B.; Van Der Nat, H.; Bartelds, A.I.M.; Heijnen, M.A.; Dankert, J. Results of Molecular Detection ofMycoplasma pneumoniaeamong Patients with Acute Respiratory Infection and in Their Household Contacts Reveals Children as Human Reservoirs. J. Infect. Dis. 2001, 183, 675–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spuesens, E.B.M.; Fraaij, P.L.A.; Visser, E.G.; Hoogenboezem, T.; Hop, W.C.J.; Van Adrichem, L.N.A.; Weber, F.; Moll, H.A.; Broekman, B.; Berger, M.Y.; et al. Carriage of Mycoplasma pneumoniae in the Upper Respiratory Tract of Symptomatic and Asymptomatic Children: An Observational Study. PLoS Med. 2013, 10, e1001444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, J.M.; Binnicker, M.J.; Campbell, S.; Carroll, K.C.; Chapin, K.C.; Gilligan, P.H.; Gonzalez, M.D.; Jerris, R.C.; Kehl, S.C.; Patel, R.; et al. A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiologya. Clin. Infect. Dis. 2018, 67, e1–e94. [Google Scholar] [CrossRef]
- Sauteur, P.M.M.; Unger, W.W.J.; Van Rossum, A.M.C.; Berger, C. The Art and Science of Diagnosing Mycoplasma pneumoniae Infection. Pediatr. Infect. Dis. J. 2018, 37, 1192–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, C.E.; Sillis, M.; Wreghitt, T.G. Evaluation of Serodia Myco II particle agglutination test for detecting Mycoplasma pneumoniae antibody: Comparison with mu-capture ELISA and indirect immunofluorescence. J. Clin. Pathol. 1990, 43, 163–165. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.-Y.; Lee, H.-S.; Hong, J.-H.; Lee, M.-H.; Lee, J.-S.; Burgner, D.; Lee, B.-C. Role of prednisolone treatment in severe Mycoplasma pneumoniae pneumonia in children. Pediatr. Pulmonol. 2006, 41, 263–268. [Google Scholar] [CrossRef]
- Youn, Y.-S.; Lee, K.-Y.; Hwang, J.-Y.; Rhim, J.-W.; Kang, J.-H.; Lee, J.-S.; Kim, J.-C. Difference of clinical features in childhood Mycoplasma pneumoniae pneumonia. BMC Pediatr. 2010, 10, 48. [Google Scholar] [CrossRef] [Green Version]
- Youn, Y.-S.; Lee, S.-C.; Rhim, J.-W.; Shin, M.-S.; Kang, J.-H.; Lee, K.-Y. Early Additional Immune-Modulators for Mycoplasma pneumoniae Pneumonia in Children: An Observation Study. Infect. Chemother. 2014, 46, 239–247. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-C.; Youn, Y.-S.; Rhim, J.-W.; Kang, J.-H.; Lee, K.-Y. Early Serologic Diagnosis of Mycoplasma pneumoniae Pneumonia. Med. 2016, 95, e3605. [Google Scholar] [CrossRef]
- Yang, E.-A.; Kang, H.-M.; Rhim, J.-W.; Kang, J.-H.; Lee, K.-Y. Early Corticosteroid Therapy for Mycoplasma pneumoniae Pneumonia Irrespective of Used Antibiotics in Children. J. Clin. Med. 2019, 8, 726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Chen, X.; Xu, A. Profile of Specific Antibodies to the SARS-Associated Coronavirus. N. Engl. J. Med. 2003, 349, 508–509. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, P.-R.; Huang, L.-M.; Chen, P.-J.; Kao, C.-L.; Yang, P.-C. Chronological evolution of IgM, IgA, IgG and neutralisation antibodies after infection with SARS-associated coronavirus. Clin. Microbiol. Infect. 2004, 10, 1062–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, K.H.; Cheng, V.C.C.; Woo, P.C.Y.; Lau, S.K.P.; Poon, L.L.M.; Guan, Y.; Seto, W.H.; Yuen, K.Y.; Peiris, J.S.M. Serological Responses in Patients with Severe Acute Respiratory Syndrome Coronavirus Infection and Cross-Reactivity with Human Coronaviruses 229E, OC43, and NL63. Clin. Diagn. Lab. Immunol. 2005, 12, 1317–1321. [Google Scholar] [CrossRef] [Green Version]
- Murchu, O.; Byrne, E.; Walsh, P.; Carty, K.A.; Connolly, P.G.; De Gascun, M.; Jordan, C.; Keoghan, K.; O’Brien, M.; O’Neill, K.K.; et al. Immune response following infection with SARS-CoV -2 and other coronaviruses: A rapid review. Rev. Med. Virol. 2020, 23, e2162. [Google Scholar] [CrossRef]
- Yu, J.; Yoo, Y.; Kim, D.K.; Kang, H.; Koh, Y.Y. Distributions of Antibody Titers to Mycoplasma pneumoniae in Korean Children in 2000–2003. J. Korean Med. Sci. 2005, 20, 542–547. [Google Scholar] [CrossRef] [Green Version]
- Beersma, M.F.C.; Dirven, K.; Van Dam, A.P.; Templeton, K.E.; Claas, E.C.J.; Goossens, H. Evaluation of 12 Commercial Tests and the Complement Fixation Test for Mycoplasma pneumoniae-Specific Immunoglobulin G (IgG) and IgM Antibodies, with PCR Used as the "Gold Standard". J. Clin. Microbiol. 2005, 43, 2277–2285. [Google Scholar] [CrossRef] [Green Version]
- Petitjean, J.; Vabret, A.; Gouarin, S.; Freymuth, F. Evaluation of Four Commercial Immunoglobulin G (IgG)- and IgM-Specific Enzyme Immunoassays for Diagnosis of Mycoplasma pneumoniae Infections. J. Clin. Microbiol. 2002, 40, 165–171. [Google Scholar] [CrossRef] [Green Version]
- Loens, K.; Ieven, M. Mycoplasma pneumoniae: Current Knowledge on Nucleic Acid Amplification Techniques and Serological Diagnostics. Front. Microbiol. 2016, 7, 448. [Google Scholar] [CrossRef]
- Wang, L.; Feng, Z.; Zhao, M.; Yang, S.; Yan, X.; Guo, W.; Shi, Z.; Li, G. A comparison study between GeXP-based multiplex-PCR and serology assay for Mycoplasma pneumoniae detection in children with community acquired pneumonia. BMC Infect. Dis. 2017, 17, 1–7. [Google Scholar] [CrossRef]
- Youn, Y.S.; Lee, K.Y.; Hwang, J.Y.; Yim, J.W.; Kang, J.H.; Lee, J.S. Comparison of Diagnostic Methods and the Changes of IgG Subclasses in Children with Mycoplasma pneumoniae pneumonia. Pediatr. Allergy Respir. Dis. 2009, 19, 137–145. [Google Scholar]
- Lee, K.-Y. A Common Immunopathogenesis Mechanism for Infectious Diseases: The Protein-Homeostasis-System Hypothesis. Infect. Chemother. 2015, 47, 12–26. [Google Scholar] [CrossRef]
- Lee, K.-Y.; Rhim, J.-W.; Kang, J.-H. Immunopathogenesis of COVID-19 and early immunomodulators. Clin. Exp. Pediatr. 2020, 63, 239–250. [Google Scholar] [CrossRef]
- Sauteur, P.M.M.; Krautter, S.; Ambroggio, L.; Seiler, M.; Paioni, P.; Relly, C.; Capaul, R.; Kellenberger, C.; Haas, T.; Gysin, C.; et al. Improved Diagnostics Help to Identify Clinical Features and Biomarkers That Predict Mycoplasma pneumoniae Community-acquired Pneumonia in Children. Clin. Infect. Dis. 2020, 71, 1645–1654. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Positive Rates, n (%) | ||
| Testing Method | At Presentation | At Discharge |
| MAA * | 38 (61) | 62 (100) |
| ELISA | 44 (71) | 62 (100) |
| PCR | 32 (52) | ND |
| Positive Results, n (%) | ||||
|---|---|---|---|---|
| MAA (n = 62) | ELISA (n = 62) | |||
| 1st Examination | 2nd Examination | |||
| Seroconversion | 24 (39) | IgM negative | 12 | All IgM positive, but 1 case decreased value |
| (negative→ ≥1:40) | IgM equivocal | 4 | ||
| IgM positive | 8 | |||
| Increased titer | 27 (44) | IgM equivocal | 2 | All IgM positive (26 cases increases and 1 case showed same value) |
| IgM positive | 25 | |||
| Both high titer of ≥1:640 | 11 (18) | IgM positive | 11 | 5 cases increase, 4 cases decrease, 2 cases same value |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, H.E.; Kang, H.M.; Yang, E.A.; Han, H.Y.; Han, S.B.; Rhim, J.W.; Lee, K.-Y. Early Confirmation of Mycoplasma pneumoniae Infection by Two Short-Term Serologic IgM Examination. Diagnostics 2021, 11, 353. https://doi.org/10.3390/diagnostics11020353
Jeon HE, Kang HM, Yang EA, Han HY, Han SB, Rhim JW, Lee K-Y. Early Confirmation of Mycoplasma pneumoniae Infection by Two Short-Term Serologic IgM Examination. Diagnostics. 2021; 11(2):353. https://doi.org/10.3390/diagnostics11020353
Chicago/Turabian StyleJeon, Ha Eun, Hyun Mi Kang, Eun Ae Yang, Hye Young Han, Seung Beom Han, Jung Woo Rhim, and Kyung-Yil Lee. 2021. "Early Confirmation of Mycoplasma pneumoniae Infection by Two Short-Term Serologic IgM Examination" Diagnostics 11, no. 2: 353. https://doi.org/10.3390/diagnostics11020353