
Role of the Appendicular Skeletal Muscle Index for Predicting the Recurrence-Free Survival of Head and Neck Cancer

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
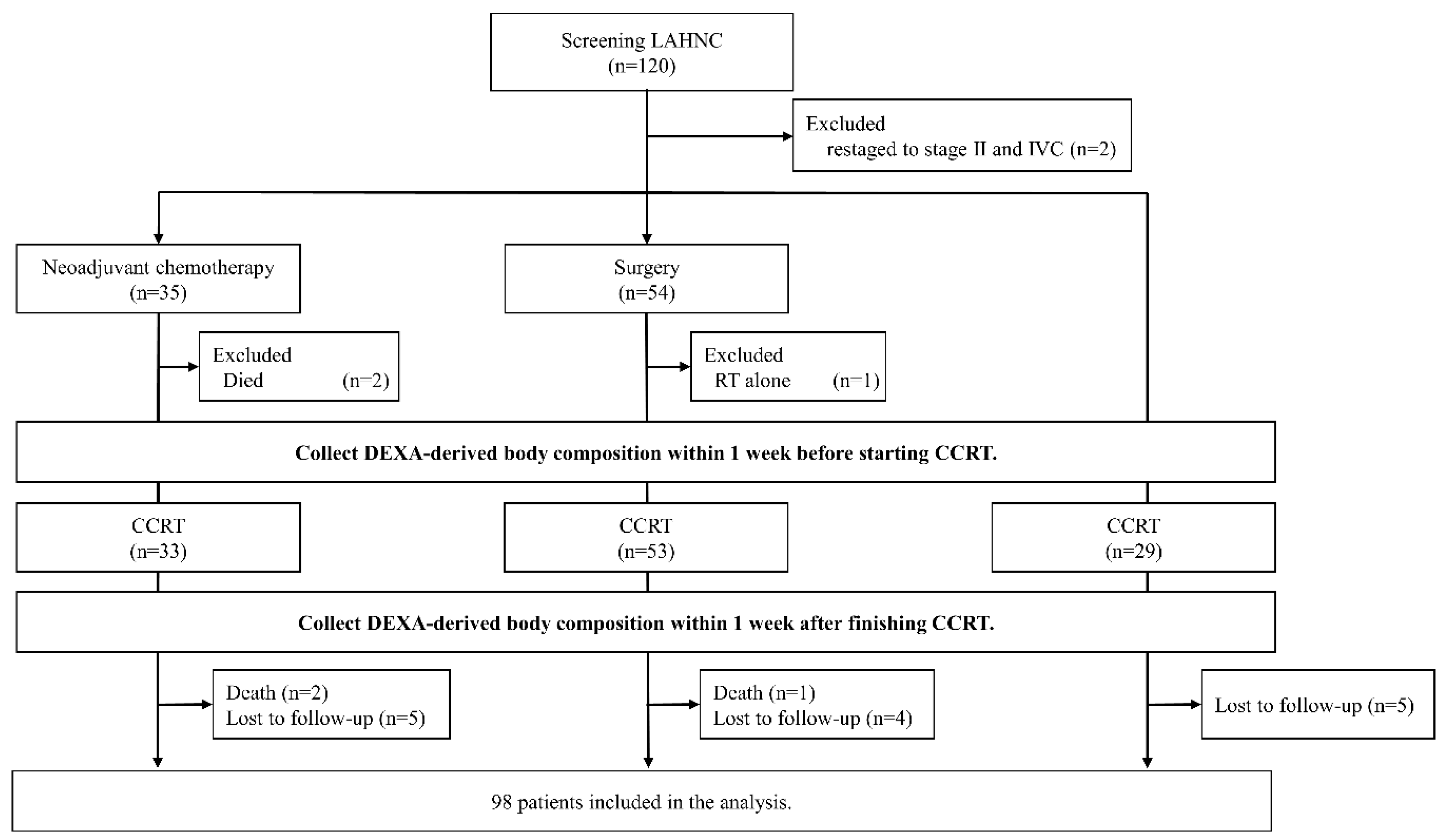
2.1. Enrollment
2.2. CCRT Schedule
2.3. Clinicopathological Data and Nutrition Assessment Methods
2.4. Body Composition Measurement
2.5. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fouladiun, M.; Körner, U.; Bosaeus, I.; Daneryd, P.; Hyltander, A.; Lundholm, K.G. Body composition and time course changes in regional distribution of fat and lean tissue in unselected cancer patients on palliative care—Correlations with food intake, metabolism, exercise capacity, and hormones. Cancer 2005, 103, 2189–2198. [Google Scholar] [CrossRef]
- Dechaphunkul, T.; Martin, L.; Alberda, C.; Olson, K.; Baracos, V.; Gramlich, L. Malnutrition assessment in patients with cancers of the head and neck: A call to action and consensus. Crit. Rev. Oncol. 2013, 88, 459–476. [Google Scholar] [CrossRef] [PubMed]
- Pring, E.T.; Malietzis, G.; Kennedy, R.H.; Athanasiou, T.; Jenkins, J.T. Cancer cachexia and myopenia—Update on management strategies and the direction of future research for optimizing body composition in cancer—A narrative review. Cancer Treat. Rev. 2018, 70, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Wendrich, A.W.; Swartz, J.E.; Bril, S.I.; Wegner, I.; De Graeff, A.; Smid, E.J.; De Bree, R.; Pothen, A.J. Low skeletal muscle mass is a predictive factor for chemotherapy dose-limiting toxicity in patients with locally advanced head and neck cancer. Oral Oncol. 2017, 71, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-P.; Joh, J.-Y.; Kim, S.; Hwang, H.-S.; Shin, I.-S. The application of different appendicular skeletal muscle cutoff points and research definitions associated with health-related quality of life in Korean older people: Data from KNHANES 2008–2011. BMC Geriatr. 2014, 14, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Pongchaiyakul, C.; Limpawattana, P.; Kotruchin, P.; Rajatanavin, R. Prevalence of sarcopenia and associated factors among Thai population. J. Bone Miner. Metab. 2013, 31, 346–350. [Google Scholar] [CrossRef]
- Limpawattana, P.; Teerakulpisut, D.; Wirasorn, K.; Sookprasert, A.; Khuntikeo, N.; Chindaprasirt, J. The impact of skeletal muscle mass on survival outcome in biliary tract cancer patients. PLoS ONE 2018, 13, e0204985. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.C.; Schmitz, K.H. Weight lifting and appendicular skeletal muscle mass among breast cancer survivors: A randomized controlled trial. Breast Cancer Res. Treat. 2015, 151, 385–392. [Google Scholar] [CrossRef] [Green Version]
- Kilgour, R.D.; Vigano, A.; Trutschnigg, B.; Hornby, L.; Lucar, E.; Bacon, S.L.; Morais, J.A. Cancer-related fatigue: The impact of skeletal muscle mass and strength in patients with advanced cancer. J. Cachex Sarcopenia Muscle 2010, 1, 177–185. [Google Scholar] [CrossRef] [Green Version]
- Jackson, W.; Alexander, N.; Schipper, M.; Fig, L.; Feng, F.; Jolly, S. Characterization of changes in total body composition for patients with head and neck cancer undergoing chemoradiotherapy using dual-energy x-ray absorptiometry. Head Neck 2013, 36, 1356–1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lønbro, S.; Dalgas, U.; Primdahl, H.; Johansen, J.; Nielsen, J.L.; Overgaard, J.; Overgaard, K. Lean body mass and muscle function in head and neck cancer patients and healthy individuals—Results from the DAHANCA 25 study. Acta Oncol. 2013, 52, 1543–1551. [Google Scholar] [CrossRef] [Green Version]
- Silver, H.J.; Dietrich, M.S.; Murphy, B.A. Changes in body mass, energy balance, physical function, and inflammatory state in patients with locally advanced head and neck cancer treated with concurrent chemoradiation after low-dose induction chemotherapy. Head Neck 2007, 29, 893–900. [Google Scholar] [CrossRef]
- Jager-Wittenaar, H.; Dijkstra, P.U.; Vissink, A.; Langendijk, J.A.; Van Der Laan, B.F.; Pruim, J.; Roodenburg, J.L.N. Changes in nutritional status and dietary intake during and after head and neck cancer treatment. Head Neck 2010, 33, 863–870. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.-C.; Lin, Y.-C.; Ng, S.-H.; Cheung, Y.-C.; Wang, C.-H.; Chen, F.-P.; Chang, H.-P.; Sung, C.-M.; Fan, C.-M.; Chen, S.-H.; et al. Effect of Chemotherapy on Dual-Energy X-ray Absorptiometry (DXA) Body Composition Precision Error in Head and Neck Cancer Patients. J. Clin. Densitom. 2019, 22, 437–443. [Google Scholar] [CrossRef]
- Wang, C.-H.; Wang, H.-M.; Pang, Y.-P.; Yeh, K.-Y. Early nutritional support in non-metastatic stage IV oral cavity cancer patients undergoing adjuvant concurrent chemoradiotherapy: Analysis of treatment tolerance and outcome in an area endemic for betel quid chewing. Support. Care Cancer 2011, 20, 1169–1174. [Google Scholar] [CrossRef]
- Bøje, C.R.; Dalton, S.O.; Primdahl, H.; Kristensen, C.A.; Andersen, E.; Johansen, J.; Andersen, L.J.; Overgaard, J. Evaluation of comorbidity in 9388 head and neck cancer patients: A national cohort study from the DAHANCA database. Radiother. Oncol. 2014, 110, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Capra, S.; Ferguson, M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur. J. Clin. Nutr. 2002, 56, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Hangartner, T.N.; Warner, S.; Braillon, P.; Jankowski, L.; Shepherd, J. The Official Positions of the International Society for Clinical Densitometry: Acquisition of Dual-Energy X-Ray Absorptiometry Body Composition and Considerations Regarding Analysis and Repeatability of Measures. J. Clin. Densitom. 2013, 16, 520–536. [Google Scholar] [CrossRef]
- Nishigori, T.; Okabe, H.; Tanaka, E.; Tsunoda, S.; Hisamori, S.; Sakai, Y. Sarcopenia as a predictor of pulmonary complications after esophagectomy for thoracic esophageal cancer. J. Surg. Oncol. 2016, 113, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Kubrak, C.; Olson, K.; Jha, N.; Scrimger, R.; Parliament, M.; McCargar, L.J.; Koski, S.; Baracos, V.E. Clinical determinants of weight loss in patients receiving radiation and chemoirradiation for head and neck cancer: A prospective longitudinal view. Head Neck 2013, 35, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Romanello, V.; Scalabrin, M.; Albiero, M.; Blaauw, B.; Scorrano, L.; Sandri, M. Inhibition of the Fission Machinery Mitigates OPA1 Impairment in Adult Skeletal Muscles. Cells 2019, 8, 597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Y.; Kim, J.W.; Keum, K.C.; Lee, C.G.; Jeung, H.C.; Lee, I.J. Prognostic Significance of Sarcopenia With Inflammation in Patients With Head and Neck Cancer Who Underwent Definitive Chemoradiotherapy. Front. Oncol. 2018, 8, 457. [Google Scholar] [CrossRef] [Green Version]
- Ganju, R.G.; Morse, R.; Hoover, A.; TenNapel, M.; Lominska, C. The impact of sarcopenia on tolerance of radiation and outcome in patients with head and neck cancer receiving chemoradiation. Radiother. Oncol. 2019, 137, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Jung, A.R.; Roh, J.-L.; Kim, J.S.; Kim, S.-B.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Prognostic value of body composition on recurrence and survival of advanced-stage head and neck cancer. Eur. J. Cancer 2019, 116, 98–106. [Google Scholar] [CrossRef]
- Pai, P.C.; Chuang, C.C.; Chuang, W.C.; Tsang, N.-M.; Tseng, C.K.; Chen, K.H.; Yen, T.C.; Lin, C.Y.; Chang, K.P.; Lei, K.F. Pretreatment subcutaneous adipose tissue predicts the outcomes of patients with head and neck cancer receiving definitive radiation and chemoradiation in Taiwan. Cancer Med. 2018, 7, 1630–1641. [Google Scholar] [CrossRef] [PubMed]
- Mitsiopoulos, N.; Baumgartner, R.N.; Heymsfield, S.B.; Lyons, W.; Gallagher, D.; Ross, R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J. Appl. Physiol. 1998, 85, 115–122. [Google Scholar] [CrossRef]
- Mourtzakis, M.; Prado, C.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef]
- Parsons, H.A.; Baracos, V.E.; Dhillon, N.; Hong, D.S.; Kurzrock, R. Body Composition, Symptoms, and Survival in Advanced Cancer Patients Referred to a Phase I Service. PLoS ONE 2012, 7, e29330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orell-Kotikangas, H.; Österlund, P.; Mäkitie, O.; Saarilahti, K.; Ravasco, P.; Schwab, U.; Mäkitie, A.A. Cachexia at diagnosis is associated with poor survival in head and neck cancer patients. Acta Oto-Laryngol. 2017, 137, 778–785. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total |
|---|---|
| Numbers (%) or Mean SD | |
| Included number of patients | 98 (100) |
| Age (years) | 53.4 8.3 |
| Sex (female:male) | 3 (3.1):95 (96.9) |
| Smoking (no:yes) | 6 (6.1):92 (93.9) |
| Alcohol consumption (no:yes) | 22 (22.4):76 (77.6) |
| Betel nut consumption (no:yes) | 34 (34.7):64 (65.3) |
| CCI (0:1:2:≥3) | 19 (19.4):27 (27.6):19 (19.4):33 (33.6) |
| Location | |
| Oral cavity | 50 (51.0) |
| Oropharynx | 22 (22.4) |
| Hypopharynx | 18 (18.4) |
| Larynx | 7 (7.1) |
| Unknown primary tumor | 1 (1.0) |
| Tumor status (T0:T1:T2:T3:T4) | 1 (1.0):4 (4.1):20 (20.4):10 (10.2):63 (64.3) |
| Lymph node status (N0:N1:N2:N3) | 17 (17.3):18 (18.4):57 (58.2):6 (6.1) |
| Tumor stage, AJCC 7th edition (III:IVA:IVB) | 9 (9.2):71 (72.4):18 (18.4) |
| Treatment modalities | |
| CCRT | 23 (23.5) |
| Surgery + CCRT | 49 (50.0) |
| Neoadjuvant chemotherapy + CCRT | 26 (26.5) |
| Cisplatin dose (mg/m2) | 221 57 |
| RT dose (Gy) | 67.1 4.9 |
| PG-SGA (well [0–3]:moderate [4–8):severe [≥9]) | 74 (75.5):23 (23.5):1 (1.0) |
| BMI (kg/m2) | 22.9 4.3 |
| Initial BWL (<10%:≥10%) | 73 (73.5):26 (26.5) |
| 2-year RFSR | 57.1% |
| Variables | Total | |||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| HR (95% CI) | p | HR (95% CI) | p | |
| Age (<60 y vs.≥60 y) | 1.644 (0.659–4.100) | 0.287 | ||
| Sex (female vs. male) | 1.519 (0.133–17.327) | 0.737 | ||
| Smoking (no vs. yes) | 1.538 (0.268–8.824) | 0.629 | ||
| Alcohol consumption (no vs. yes) | 2.400 (0.848–6.795) | 0.099 | ||
| Betel nut consumption (no vs. yes) | 1.964 (0.823–4.687) | 0.128 | ||
| CCI (<3 vs.≥3) | 2.050 (0.876–4.798) | 0.098 | ||
| Location (OC vs. NOC) | 0.387 (0.170–0.884) | 0.024 | 0.418 (0.173–1.011) | 0.055 |
| Tumor status (T0–T2 vs. T3–T4) | 2.368 (0.883–6.351) | 0.087 | ||
| Lymph node status (N0–N1 vs. N2–N3) | 2.114 (0.887–5.034) | 0.091 | ||
| Tumor stage (III vs. IV) | 2.857 (0.562–14.525) | 0.206 | ||
| Treatment modalities | ||||
| CCRT | 1 | |||
| Surgery + CCRT | 0.688 (0.217–2.183) | 0.526 | ||
| Neoadjuvant chemotherapy + CCRT | 1.150 (0.424–3.117) | 0.784 | ||
| Cisplatin dose (<200 vs.≥200 mg/m2) | 0.681 (0.244–1.902) | 0.463 | ||
| RT dose (<68 vs.≥68 Gy) | 0.769 (0.345–1.716) | 0.521 | ||
| PG-SGA (well vs. moderate/severe) | 2.200 (0.882–5.489) | 0.091 | ||
| Initial BWL (<10% vs.≥10%) | 2.831 (1.123–7.138) | 0.027 | ||
| Baseline body composition | ||||
| BMI (<18.5 vs.≥18.5 kg/m2) | 0.245 (0.079–0.764) | 0.015 | 1.412 (0.237–8.418) | 0.705 |
| TLMI (<14.4 vs.≥14.4 kg/m2) * | 0.271 (0.102–0.717) | 0.009 | ||
| TFMI (<5.1 vs.≥5.1 kg/m2) * | 0.391 (0.171–0.895) | 0.026 | 0.519 (0.187–1.443) | 0.209 |
| ASMI (<6.1 vs.≥6.1 kg/m2) * | 0.211 (0.083–0.537) | 0.001 | 0.235 (0.062–0.885) | 0.030 |
| Overall | Pre-CCRT (n = 98) | Post-CCRT (n = 98) | Percent Change (95% CI) | p Value |
|---|---|---|---|---|
| BW, kg | 63.3 12.3 | 59.8 10.5 | 4.9 (6.5,3.3) | <0.001 |
| BMI, kg/m2 | 22.9 4.3 | 21.6 3.7 | 4.8 (6.4,3.2) | <0.001 |
| TLM, kg | 44.0 6.1 | 41.6 5.5 | 5.2 (6.4,4.0) | <0.001 |
| TFM, kg | 16.3 7.8 | 15.1 7.0 | 5.3 (9.2,1.5) | <0.001 |
| TLMI, kg/m2 | 15.9 2.0 | 15.0 1.8 | 5.1 (6.4,3.9) | <0.001 |
| TFMI, kg/m2 | 5.9 2.9 | 5.5 2.5 | 4.8 (9.1,0.6) | <0.001 |
| ASMI, kg/m2 | 6.8 1.2 | 6.3 1.1 | 7.7 (9.4,6.1) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, K.-Y.; Ling, H.H.; Ng, S.-H.; Wang, C.-H.; Chang, P.-H.; Chou, W.-C.; Chen, F.-P.; Lin, Y.-C. Role of the Appendicular Skeletal Muscle Index for Predicting the Recurrence-Free Survival of Head and Neck Cancer. Diagnostics 2021, 11, 309. https://doi.org/10.3390/diagnostics11020309
Yeh K-Y, Ling HH, Ng S-H, Wang C-H, Chang P-H, Chou W-C, Chen F-P, Lin Y-C. Role of the Appendicular Skeletal Muscle Index for Predicting the Recurrence-Free Survival of Head and Neck Cancer. Diagnostics. 2021; 11(2):309. https://doi.org/10.3390/diagnostics11020309
Chicago/Turabian StyleYeh, Kun-Yun, Hang Huong Ling, Shu-Hang Ng, Cheng-Hsu Wang, Pei-Hung Chang, Wen-Chi Chou, Fang-Ping Chen, and Yu-Ching Lin. 2021. "Role of the Appendicular Skeletal Muscle Index for Predicting the Recurrence-Free Survival of Head and Neck Cancer" Diagnostics 11, no. 2: 309. https://doi.org/10.3390/diagnostics11020309