
Quantification of the Therapist’s Gentle Pull for Pinch Strength Testing Based on FMA and MMT: An Experimental Study with Healthy Subjects

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Quantification of Gentle Pull
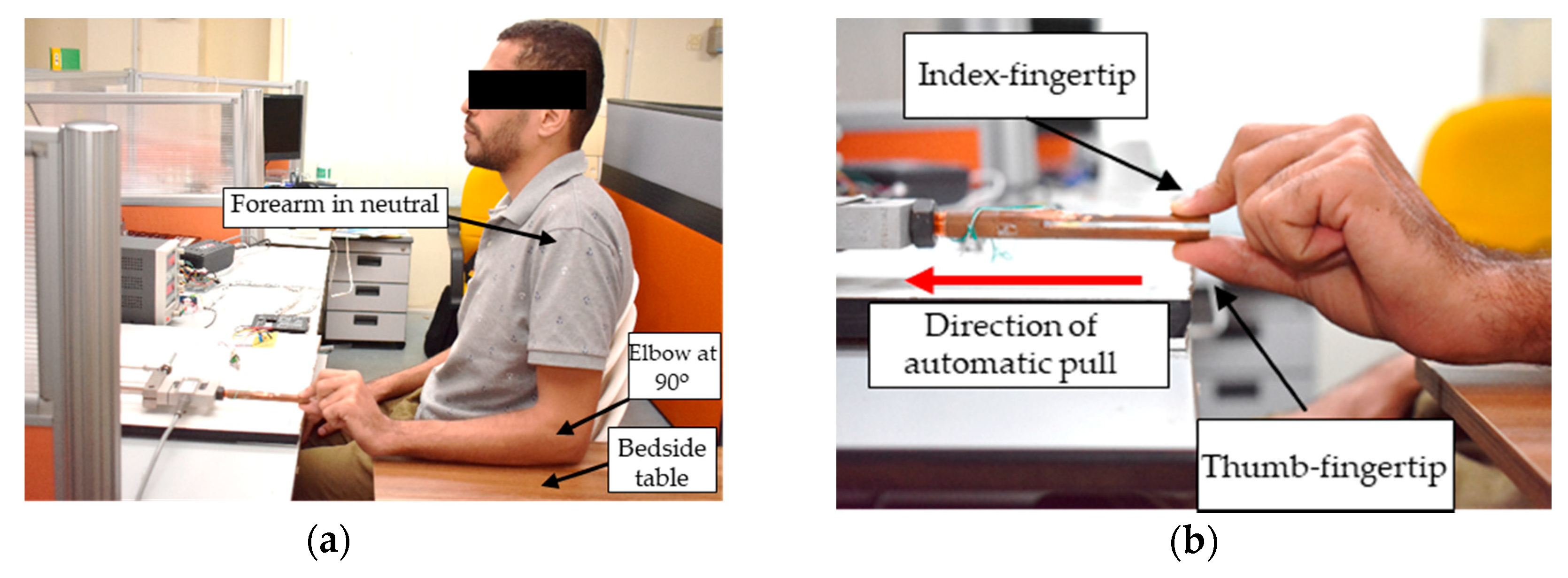
2.2. Exeprimental Protocol for Healthy Subjects
3. Results
3.1. Quantitative Value of Gentle Pull
3.2. Pulling Forces of Normal Subjects at Slip-Away
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kim, J.-Y.; Cha, Y.-R.; Lee, S.-H.; Jung, B.-K. Development and Evaluation of Tip Pinch Strength Measurement on a Paretic Hand Rehabilitation Device. KSII Trans. Internet Inf. Syst. 2017, 11, 1201–1216. [Google Scholar]
- Eroğlu, M.; Karapolat, H.; Atamaz, F.; Tanıgör, G.; Kirazlı, Y. Occupational therapy assessment and treatment approach in patients with subacute and chronic stroke: A single-blind, prospective, randomized clinical trial. Turk. J. Phys. Med. Rehabil. 2020, 66, 316. [Google Scholar] [PubMed]
- Fugl-Meyer, A.R. Post-stroke hemiplegia assessment of physical properties. Scand. J. Rehabil. Med. Suppl. 1980, 7, 85–93. [Google Scholar] [PubMed]
- See, J.; Dodakian, L.; Chou, C.; Chan, V.; McKenzie, A.; Reinkensmeyer, D.J.; Cramer, S.C. A standardized approach to the Fugl-Meyer assessment and its implications for clinical trials. Neurorehabil. Neural Repair 2013, 27, 732–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woytowicz, E.J.; Rietschel, J.C.; Goodman, R.N.; Conroy, S.S.; Sorkin, J.D.; Whitall, J.; Waller, S.M. Determining levels of upper extremity movement impairment by applying a cluster analysis to the Fugl-Meyer assessment of the upper extremity in chronic stroke. Arch. Phys. Med. Rehabil. 2017, 98, 456–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krakauer, J.W.; Carmichael, S.T. Broken Movement: The Neurobiology of Motor Recovery after Stroke; MIT Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Simbaña, E.D.O.; Baeza, P.S.-H.; Jardón Huete, A.; Balaguer, C. Review of Automated Systems for Upper Limbs Functional Assessment in Neurorehabilitation. IEEE Access 2019, 7, 32352–32367. [Google Scholar] [CrossRef]
- Deakin, A.; Hill, H.; Pomeroy, V.M. Rough guide to the Fugl-Meyer Assessment: Upper limb section. Physiotherapy 2003, 89, 751–763. [Google Scholar] [CrossRef]
- Kendall, F.P.; McCreary, E.K.; Provance, P.G.; Rodgers, M.; Romani, W.A. Muscles: Testing and Function with Posture and Pain; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; pp. 212–213. [Google Scholar]
- Baschung Pfister, P.; de Bruin, E.D.; Sterkele, I.; Maurer, B.; de Bie, R.A.; Knols, R.H. Manual muscle testing and hand-held dynamometry in people with inflammatory myopathy: An intra-and interrater reliability and validity study. PLoS ONE 2018, 13, e0194531. [Google Scholar] [CrossRef]
- Lewinson, R.T.; Ganesh, A.; Yeung, M.M. The Biomechanics of Manual Muscle Testing in the Neuromuscular Exam. Can. J. Neurol. Sci. 2018, 45, 518–521. [Google Scholar] [CrossRef] [Green Version]
- Otten, P.; Kim, J.; Son, S.H. A framework to automate assessment of upper-limb motor function impairment: A feasibility study. Sensors 2015, 15, 20097–20114. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Lee, Y.-S.; Kim, J. Automated evaluation of upper-limb motor function impairment using Fugl-Meyer assessment. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Sadun, A.S.; Jalani, J.; Sukor, J.A. Force Sensing Resistor (FSR): A brief overview and the low-cost sensor for active compliance control. In Proceedings of the First International Workshop on Pattern Recognition, Tokyo, Japan, 11 July 2016; p. 1001112. [Google Scholar]
- Rao, S.; Rao, R. Experimental investigation on the suitability of flexible pressure sensor for wrist pulse measurement. Health Technol. 2019, 9, 143–151. [Google Scholar] [CrossRef]
- Hamilton, M.; Behdinan, K.; Andrysek, J. Evaluating the Effects of Load Area and Sensor Configuration on the Performance of Pressure Sensors at Simulated Body-Device Interfaces. IEEE Sens. J. 2020, 20, 5187–5194. [Google Scholar] [CrossRef]
- Alsayed, A.; Kamil, R.; Ramli, H.; As’Arry, A. An Automated Data Acquisition System for Pinch Grip Assessment Based on Fugl Meyer Protocol: A Feasibility Study. Appl. Sci. 2020, 10, 3436. [Google Scholar] [CrossRef]
- Alsayed, A.; Kamil, R.; Ramli, H.R.; As’Arry, A. Design and Calibration of Pinch Force Measurement Using Strain Gauge for Post-Stroke Patients. Int. J. Integr. Eng. 2019, 11, 40–50. [Google Scholar] [CrossRef]
- Page, S.J.; Levine, P.; Hade, E. Psychometric properties and administration of the wrist/hand subscales of the Fugl-Meyer Assessment in minimally impaired upper extremity hemiparesis in stroke. Arch. Phys. Med. Rehabil. 2012, 93, 2373–2376. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, K.J.; Tilson, J.K.; Cen, S.Y.; Rose, D.K.; Hershberg, J.; Correa, A.; Gallichio, J.; McLeod, M.; Moore, C.; Wu, S.S.; et al. Fugl-Meyer assessment of sensorimotor function after stroke: Standardized training procedure for clinical practice and clinical trials. Stroke 2011, 42, 427–432. [Google Scholar] [CrossRef] [Green Version]
- Iijima, A.; Shimizu, K.; Kobashi, H.; Saito, A.; Kamiya, K. Repeatability, reproducibility, and comparability of subjective and objective measurements of intraocular forward scattering in healthy subjects. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [Green Version]
- Scheel, C.; Mecham, J.; Zuccarello, V.; Mattes, R. An evaluation of the inter-rater and intra-rater reliability of OccuPro’s functional capacity evaluation. Work 2018, 60, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, W.H.; Cuthbert, S.C. Common errors and clinical guidelines for manual muscle testing: ” the arm test” and other inaccurate procedures. Chiropr. Osteopat. 2008, 16, 16. [Google Scholar] [CrossRef] [Green Version]
- Krause, D.A.; Neuger, M.D.; Lambert, K.A.; Johnson, A.E.; DeVinny, H.A.; Hollman, J.H. Effects of examiner strength on reliability of hip-strength testing using a handheld dynamometer. J. Sport Rehabil. 2014, 23, 56–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derler, S.; Gerhardt, L.-C.; Lenz, A.; Bertaux, E.; Hadad, M. Friction of human skin against smooth and rough glass as a function of the contact pressure. Tribol. Int. 2009, 42, 1565–1574. [Google Scholar] [CrossRef]
- Adams, M.J.; Johnson, S.A.; Lefèvre, P.; Lévesque, V.; Hayward, V.; André, T.; Thonnard, J.-L. Finger pad friction and its role in grip and touch. J. R. Soc. Interface 2013, 10, 20120467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberge, J.-P.; Ruotolo, W.; Duchaine, V.; Cutkosky, M. Improving industrial grippers with adhesion-controlled friction. IEEE Robot. Autom. Lett. 2018, 3, 1041–1048. [Google Scholar] [CrossRef]
- Miall, R.C.; Rosenthal, O.; Ørstavik, K.; Cole, J.D.; Sarlegna, F.R. Loss of haptic feedback impairs control of hand posture. Exp. Brain Res. 2019, 237, 2167–2184. [Google Scholar] [CrossRef] [Green Version]
- Puh, U. Age-related and sex-related differences in hand and pinch grip strength in adults. Int. J. Rehabil. Res. 2010, 33, 4–11. [Google Scholar] [CrossRef]
- Maleki-Ghahfarokhi, A.; Dianat, I.; Feizi, H.; Asghari-Jafarabadi, M. Influences of gender, hand dominance, and anthropometric characteristics on different types of pinch strength: A partial least squares (PLS) approach. Appl. Ergon. 2019, 79, 9–16. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial | Therapist 1 | Therapist 2 | Therapist 3 | |
|---|---|---|---|---|
| 1 | 4.32 | 6.61 | 7.73 | |
| 2 | 5.46 | 6.54 | 5.74 | |
| 3 | 5.95 | 8.31 | 6.46 | |
| Mean | 5.24 | 7.15 | 6.64 | 6.34 |
| Variable | Trial 1 | Trial 2 | Title 3 | Mean |
|---|---|---|---|---|
| Pinch force (N) | 16.3 | 19.21 | 18.43 | 17.98 |
| Pulling force (N) | 10.27 | 10.94 | 11.98 | 11.06 |
| Pinch-pulling Pearson’s (r) | 0.977 | 0.846 | 0.950 | 0.924 |
| Variable | Cronbach’s Alpha | Pearson’s (r) | ||
|---|---|---|---|---|
| R | L | R | L | |
| Pinch force | 0.918 ± 0.05 | 0.907 ± 0.05 | 0.917 ± 0.03 | 0.893 ± 0.05 |
| Pulling force | 0.899 ± 0.05 | 0.908 ± 0.04 | ||
| Variable | Mean | Standard Deviation | Range | |
|---|---|---|---|---|
| Pinch force (N) | Right hand | 19.92 | 3.48 | 12.35–28.34 |
| Left hand | 17.68 | 3.09 | 11.15–25.12 | |
| Pulling force (N) | Right hand | 14.84 | 3.57 | 8.11–25.25 |
| Left hand | 13 | 2.72 | 7.69–20.93 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsayed, A.; Kamil, R.; Rowe, V.; Salim, M.S.F.; Ramli, H.R.; As’arry, A. Quantification of the Therapist’s Gentle Pull for Pinch Strength Testing Based on FMA and MMT: An Experimental Study with Healthy Subjects. Diagnostics 2021, 11, 225. https://doi.org/10.3390/diagnostics11020225
Alsayed A, Kamil R, Rowe V, Salim MSF, Ramli HR, As’arry A. Quantification of the Therapist’s Gentle Pull for Pinch Strength Testing Based on FMA and MMT: An Experimental Study with Healthy Subjects. Diagnostics. 2021; 11(2):225. https://doi.org/10.3390/diagnostics11020225
Chicago/Turabian StyleAlsayed, Abdallah, Raja Kamil, Veronica Rowe, Mazatulfazura S. F. Salim, Hafiz R. Ramli, and Azizan As’arry. 2021. "Quantification of the Therapist’s Gentle Pull for Pinch Strength Testing Based on FMA and MMT: An Experimental Study with Healthy Subjects" Diagnostics 11, no. 2: 225. https://doi.org/10.3390/diagnostics11020225