
Assessment of Retinal Capillary Dropout after Transcatheter Aortic Valve Implantation by Optical Coherence Tomography Angiography

 , , ,
, , ,
Abstract
:1. Introduction
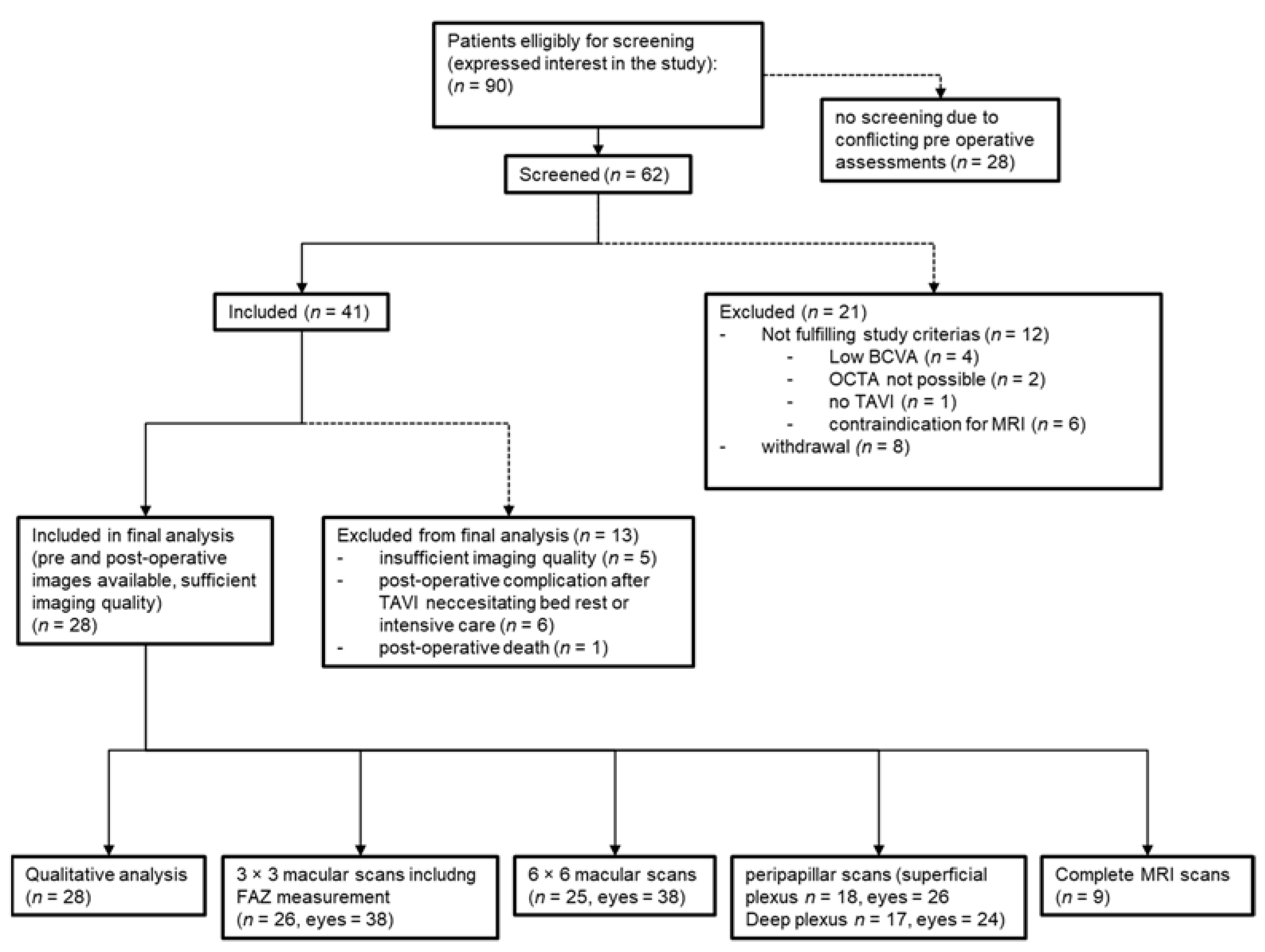
2. Materials and Methods
3. Results
3.1. Analysis of Demographics
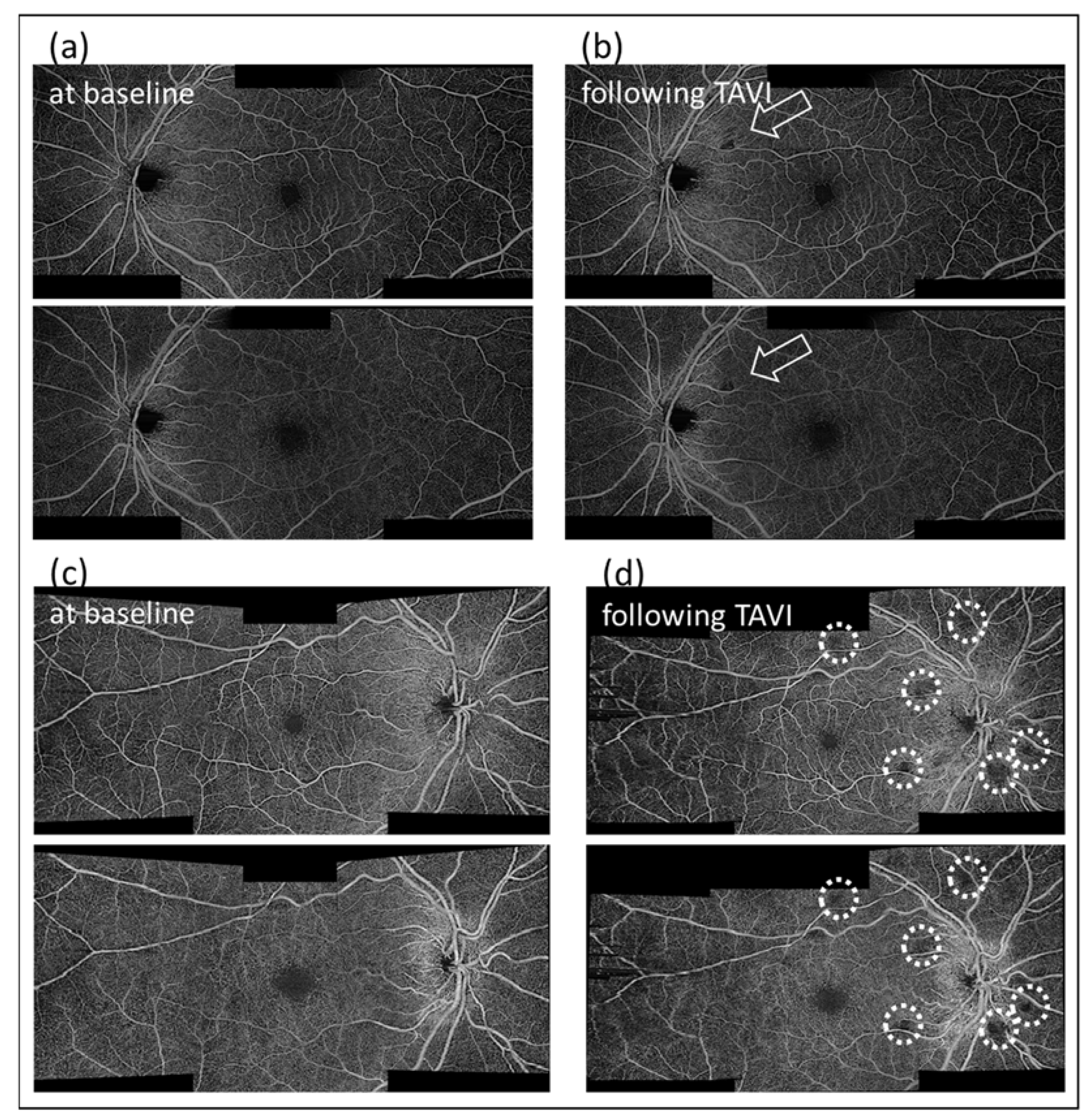
3.2. Qualitative Analysis
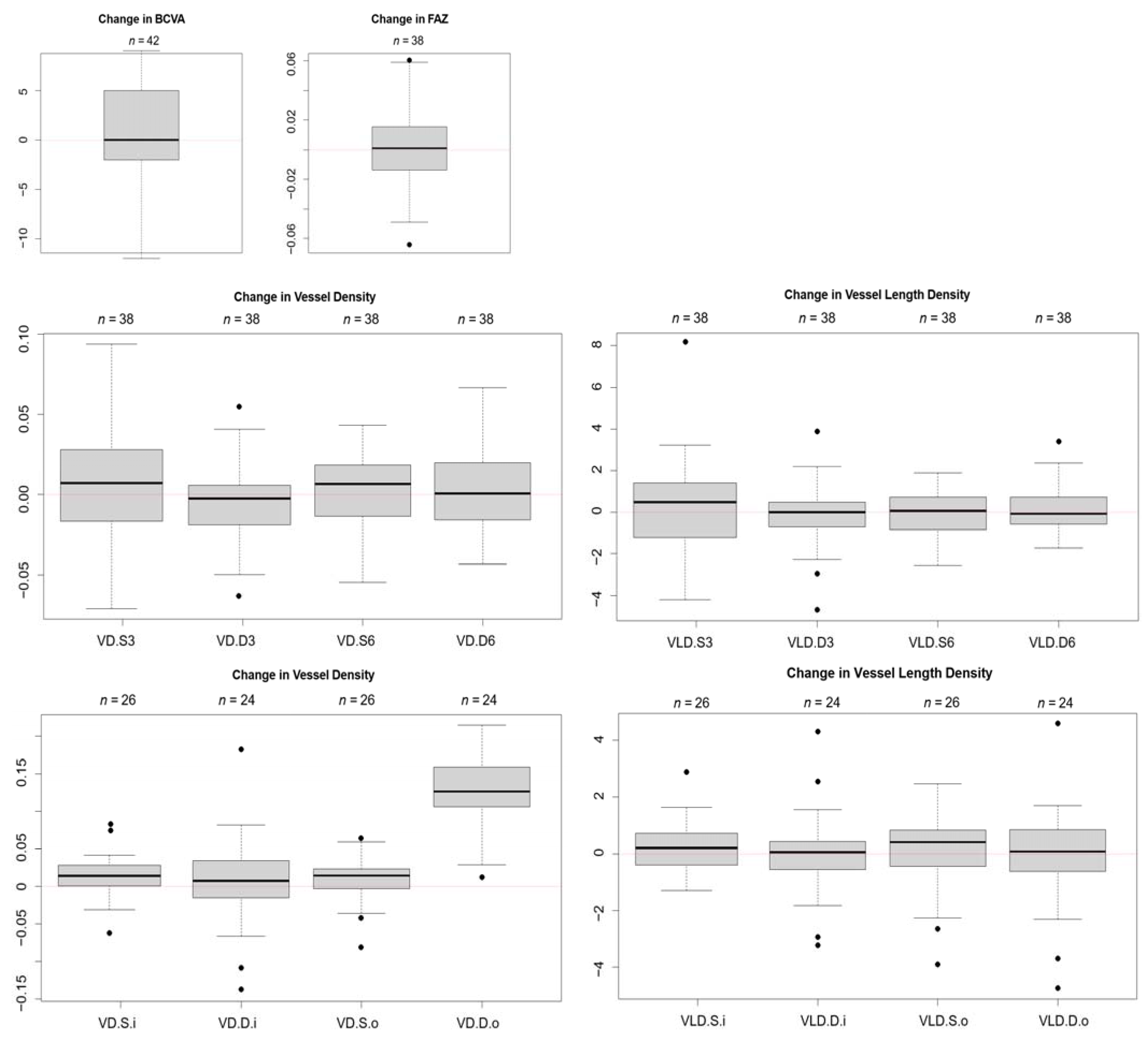
3.3. Quantitative Analysis
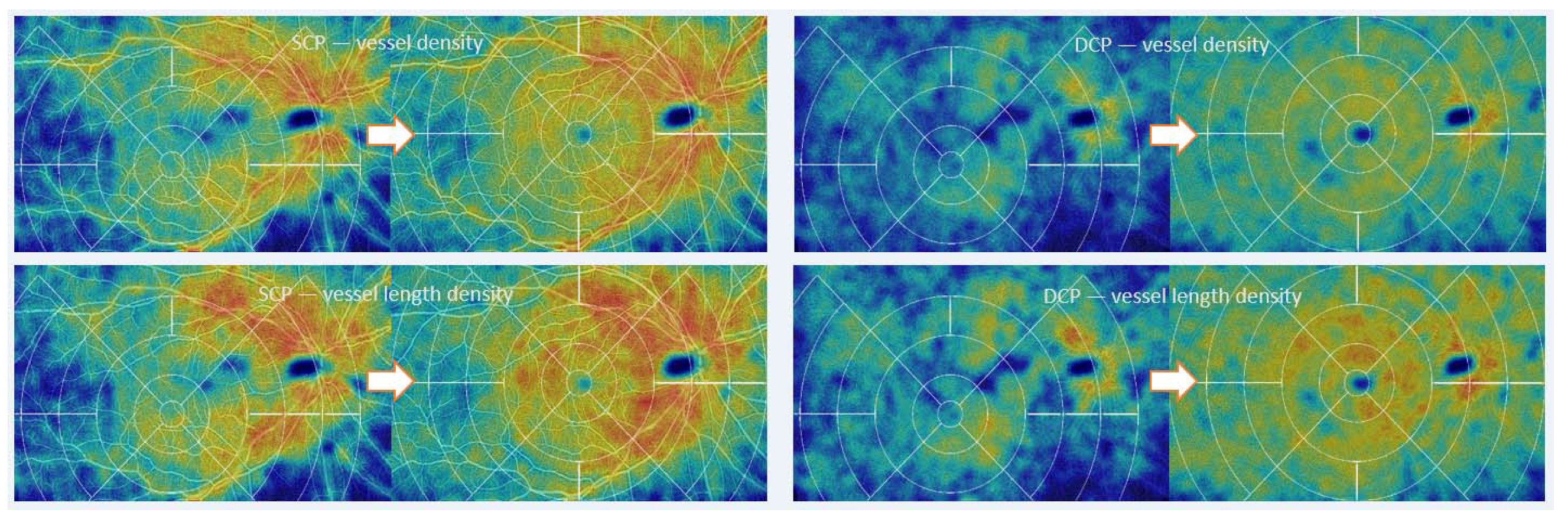
3.4. Heat Maps
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Mieghem, N.M.; Schipper, M.E.; Ladich, E.; Faqiri, E.; van der Boon, R.; Randjgari, A.; Schultz, C.; Moelker, A.; van Geuns, R.J.; Otsuka, F.; et al. Histopathology of embolic debris captured during transcatheter aortic valve replacement. Circulation 2013, 127, 2194–2201. [Google Scholar] [CrossRef]
- Kapadia, S.; Agarwal, S.; Miller, D.C.; Webb, J.G.; Mack, M.; Ellis, S.; Herrmann, H.C.; Pichard, A.D.; Tuzcu, E.M.; Svensson, L.G.; et al. Insights Into Timing, Risk Factors, and Outcomes of Stroke and Transient Ischemic Attack After Transcatheter Aortic Valve Replacement in the PARTNER Trial (Placement of Aortic Transcatheter Valves). Circ. Cardiovasc. Interv. 2016, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrmann, H.C.; Thourani, V.H.; Kodali, S.K.; Makkar, R.R.; Szeto, W.Y.; Anwaruddin, S.; Desai, N.; Lim, S.; Malaisrie, S.C.; Kereiakes, D.J.; et al. One-Year Clinical Outcomes With SAPIEN 3 Transcatheter Aortic Valve Replacement in High-Risk and Inoperable Patients With Severe Aortic Stenosis. Circulation 2016, 134, 130–140. [Google Scholar] [CrossRef]
- Nuis, R.J.; Van Mieghem, N.M.; Schultz, C.J.; Moelker, A.; van der Boon, R.M.; van Geuns, R.J.; van der Lugt, A.; Serruys, P.W.; Rodés-Cabau, J.; van Domburg, R.T.; et al. Frequency and causes of stroke during or after transcatheter aortic valve implantation. Am. J. Cardiol. 2012, 109, 1637–1643. [Google Scholar] [CrossRef] [PubMed]
- Kahlert, P.; Knipp, S.C.; Schlamann, M.; Thielmann, M.; Al-Rashid, F.; Weber, M.; Johansson, U.; Wendt, D.; Jakob, H.G.; Forsting, M.; et al. Silent and apparent cerebral ischemia after percutaneous transfemoral aortic valve implantation: A diffusion-weighted magnetic resonance imaging study. Circulation 2010, 121, 870–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanem, A.; Müller, A.; Nähle, C.P.; Kocurek, J.; Werner, N.; Hammerstingl, C.; Schild, H.H.; Schwab, J.O.; Mellert, F.; Fimmers, R.; et al. Risk and fate of cerebral embolism after transfemoral aortic valve implantation: A prospective pilot study with diffusion-weighted magnetic resonance imaging. J. Am. Coll. Cardiol. 2010, 55, 1427–1432. [Google Scholar] [CrossRef] [Green Version]
- Pagnesi, M.; Martino, E.A.; Chiarito, M.; Mangieri, A.; Jabbour, R.J.; Van Mieghem, N.M.; Kodali, S.K.; Godino, C.; Landoni, G.; Colombo, A.; et al. Silent cerebral injury after transcatheter aortic valve implantation and the preventive role of embolic protection devices: A systematic review and meta-analysis. Int. J. Cardiol. 2016, 221, 97–106. [Google Scholar] [CrossRef]
- Petzold, A.; Islam, N.; Hu, H.H.; Plant, G.T. Embolic and nonembolic transient monocular visual field loss: A clinicopathologic review. Surv. Ophthalmol. 2013, 58, 42–62. [Google Scholar] [CrossRef]
- Rimpiläinen, R.; Hautala, N.; Koskenkari, J.; Rimpiläinen, J.; Ohtonen, P.; Mustonen, P.; Surcel, H.M.; Savolainen, E.R.; Mosorin, M.; Ala-Kokko, T.; et al. Comparison of the use of minimized cardiopulmonary bypass with conventional techniques on the incidence of retinal microemboli during aortic valve replacement surgery. Perfusion 2011, 26, 479–486. [Google Scholar] [CrossRef]
- Cugati, S.; Wang, J.J.; Rochtchina, E.; Mitchell, P. Ten-year incidence of retinal emboli in an older population. Stroke 2006, 37, 908–910. [Google Scholar] [CrossRef] [Green Version]
- Rim, T.H.; Han, J.; Choi, Y.S.; Hwang, S.S.; Lee, C.S.; Lee, S.C.; Kim, S.S. Retinal Artery Occlusion and the Risk of Stroke Development: Twelve-Year Nationwide Cohort Study. Stroke 2016, 47, 376–382. [Google Scholar] [CrossRef]
- Zhang, A.; Zhang, Q.; Chen, C.L.; Wang, R.K. Methods and algorithms for optical coherence tomography-based angiography: A review and comparison. J. Biomed. Opt. 2015, 20, 100901. [Google Scholar] [CrossRef] [Green Version]
- Potsaid, B.; Baumann, B.; Huang, D.; Barry, S.; Cable, A.E.; Schuman, J.S.; Duker, J.S.; Fujimoto, J.G. Ultrahigh speed 1050 nm swept source/Fourier domain OCT retinal and anterior segment imaging at 100,000 to 400,000 axial scans per second. Opt. Express 2010, 18, 20029–20048. [Google Scholar] [CrossRef] [Green Version]
- Braaf, B.; Vermeer, K.A.; Sicam, V.A.; van Zeeburg, E.; van Meurs, J.C.; de Boer, J.F. Phase-stabilized optical frequency domain imaging at 1-µm for the measurement of blood flow in the human choroid. Opt. Express 2011, 19, 20886–20903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariampillai, A.; Standish, B.A.; Moriyama, E.H.; Khurana, M.; Munce, N.R.; Leung, M.K.; Jiang, J.; Cable, A.; Wilson, B.C.; Vitkin, I.A.; et al. Speckle variance detection of microvasculature using swept-source optical coherence tomography. Opt. Lett. 2008, 33, 1530–1532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hänsli, C.; Sugiura, Y.; Freund, K.B.; Zweifel, S. Correlation of Outer Retinal Tubulations and Choriocapillaris Flow Signal Deficits surrounding Geographic Atrophy. RETINA 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Rousseeuw, P.J.; Verboven, S. Robust estimation in very small samples. Comput. Stat. Data Anal. 2002, 40, 741–758. [Google Scholar] [CrossRef]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical coherence tomography angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef]
- Lei, J.; Durbin, M.K.; Shi, Y.; Uji, A.; Balasubramanian, S.; Baghdasaryan, E.; Al-Sheikh, M.; Sadda, S.R. Repeatability and Reproducibility of Superficial Macular Retinal Vessel Density Measurements Using Optical Coherence Tomography Angiography En Face Images. JAMA Ophthalmol. 2017, 135, 1092–1098. [Google Scholar] [CrossRef]
- Fusi-Rubiano, W.J.; Yang, Y.C.; Smallwood, A.F.; Chavan, R.C.; Khogali, S.; Narendran, N.; Cotton, J.M. Retinal embolic events: Frequency and impact following transcatheter aortic valve implantation (TAVI) for aortic stenosis. BMJ Open Ophthalmol. 2017, 1, e000033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, Z.; Lin, J.; Gao, C.; Xin, C.; Zhang, Q.; Chen, C.L.; Roisman, L.; Gregori, G.; Rosenfeld, P.J.; Wang, R.K. Quantitative assessment of the retinal microvasculature using optical coherence tomography angiography. J. Biomed. Opt. 2016, 21, 66008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, X.; Shen, Y.M.; Jiang, M.N.; Lou, X.F.; Shen, Y. Ocular Blood Flow Autoregulation Mechanisms and Methods. J. Ophthalmol. 2015, 2015, 864871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnould, L.; Guenancia, C.; Gabrielle, P.H.; Pitois, S.; Baudin, F.; Pommier, T.; Zeller, M.; Bron, A.M.; Creuzot-Garcher, C.; Cottin, Y. Influence of cardiac hemodynamic variables on retinal vessel density measurement on optical coherence tomography angiography in patients with myocardial infarction. J. Fr. Ophtalmol. 2020, 43, 216–221. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | |
|---|---|
| Male gender | 23 (82.1%) |
| Arterial hypertension | 24 (85.7%) |
| Arterial fibrilation | 2 (7.1%) |
| Diabetes | 7 (25%) |
| History of strokes | 2 (7.1%) |
| Ophthalmic baseline characteristics | |
| Cataract (Mild And Moderate) | 12 (42.9%) |
| Age-Related Macular Degeneration | 5 (17.9%) |
| Pseudophakic | 8 (28.6%) |
| Glaucoma | 2 (7.1%) |
| Diabetic Retinopathy | 2 (7.1%) |
| Procedure related baseline characteristics | |
| Type of aortic stenosis | |
| 15 (53.6%) |
| 8 (28.6%) |
| 3 (10.7%) |
| 2 (7.1%) |
| Valve in valve operation | 2 (7.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gunzinger, J.M.; Ibrahimi, B.; Baur, J.; Wiest, M.R.J.; Piccirelli, M.; Pangalu, A.; Straumann, D.; Nietlispach, F.; Moarof, I.; Zweifel, S.A. Assessment of Retinal Capillary Dropout after Transcatheter Aortic Valve Implantation by Optical Coherence Tomography Angiography. Diagnostics 2021, 11, 2399. https://doi.org/10.3390/diagnostics11122399
Gunzinger JM, Ibrahimi B, Baur J, Wiest MRJ, Piccirelli M, Pangalu A, Straumann D, Nietlispach F, Moarof I, Zweifel SA. Assessment of Retinal Capillary Dropout after Transcatheter Aortic Valve Implantation by Optical Coherence Tomography Angiography. Diagnostics. 2021; 11(12):2399. https://doi.org/10.3390/diagnostics11122399
Chicago/Turabian StyleGunzinger, Jeanne Martine, Burbuqe Ibrahimi, Joel Baur, Maximilian Robert Justus Wiest, Marco Piccirelli, Athina Pangalu, Dominik Straumann, Fabian Nietlispach, Igal Moarof, and Sandrine Anne Zweifel. 2021. "Assessment of Retinal Capillary Dropout after Transcatheter Aortic Valve Implantation by Optical Coherence Tomography Angiography" Diagnostics 11, no. 12: 2399. https://doi.org/10.3390/diagnostics11122399