
Comparison of Digital OPG and CBCT in Assessment of Risk Factors Associated with Inferior Nerve Injury during Mandibular Third Molar Surgery



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study and Sample Characteristics
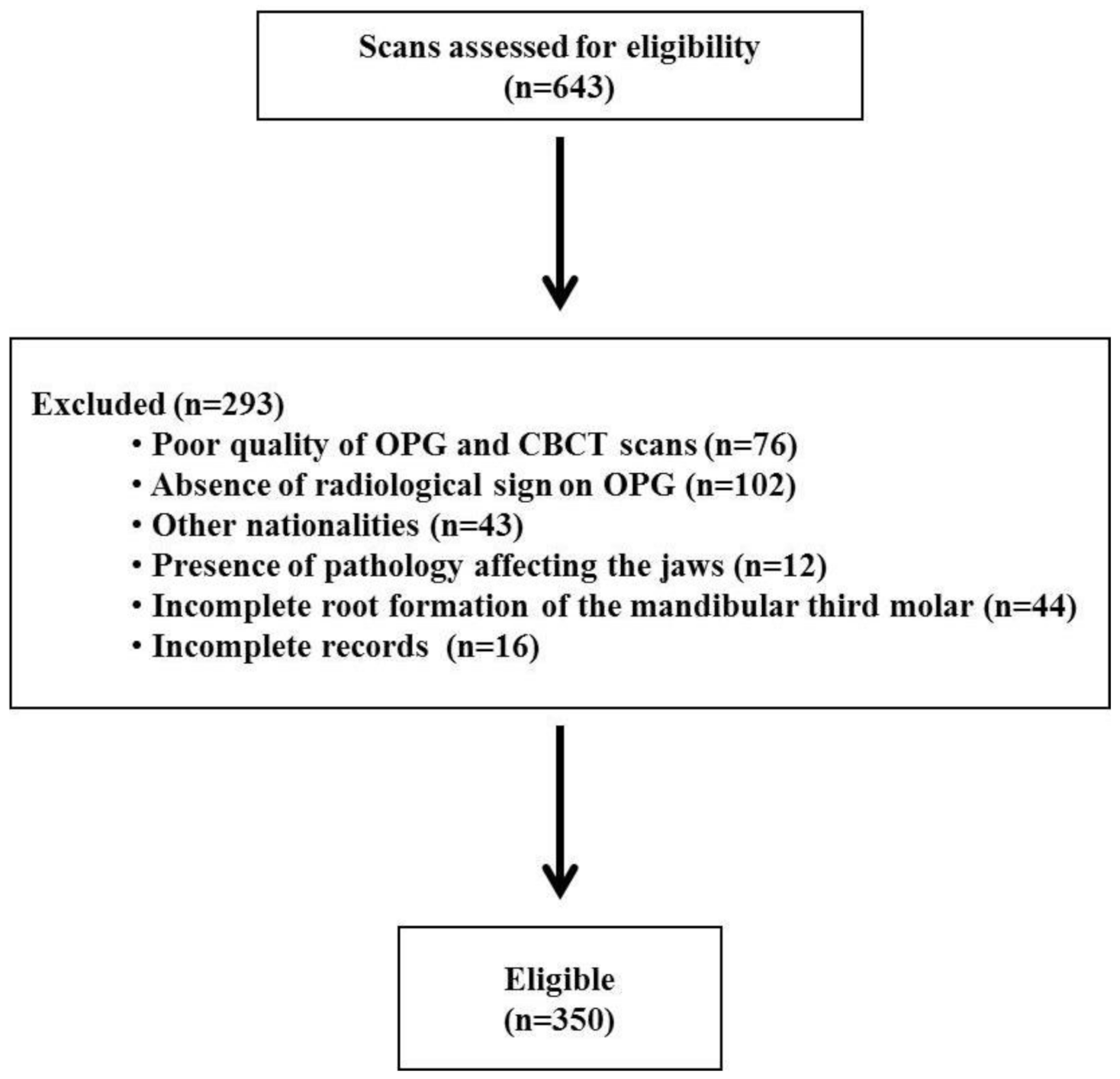
2.2. Sample Size
2.3. Inclusion and Exclusion Criteria
2.4. Evaluation of OPG Images
2.5. Analysis of CBCT Images
2.6. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mukherjee, S.; Vikraman, B.; Sankar, D.; Veerabahu, M.S. Evaluation of outcome following coronectomy for the management of mandibular third molars in close proximity to inferior alveolar nerve. J. Clin. Diagn. Res. 2016, 10, ZC57–ZC62. [Google Scholar] [CrossRef] [PubMed]
- Di Nardo, D.; Mazzucchi, G.; Lollobrigida, M.; Passariello, C.; Guarnieri, R.; Galli, M.; De Biase, A.; Testarelli, L. Immediate or delayed retrieval of the displaced third molar: A review. J. Clin. Exp. Dent. 2019, 11, e55–e61. [Google Scholar] [CrossRef]
- Tassoker, M. Diversion of the mandibular canal: Is it the best predictor of inferior alveolar nerve damage during mandibular third molar surgery on panoramic radiographs? Imaging Sci. Dent. 2019, 49, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yin, W.; Zhang, R.; Li, J.; Zheng, Y. Diagnostic value of panoramic radiography in predicting inferior alveolar nerve injury after mandibular third molar extraction: A meta-analysis. Aust. Dent. J. 2015, 60, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Pathak, S.; Mishra, N.; Rastogi, M.K.; Sharma, S. Significance of radiological variables studied on orthopantamogram to predict post-operative inferior alveolar nerve paresthesia after third molar extraction. J. Clin. Diagn. Res. 2014, 8, ZC62–ZC64. [Google Scholar] [CrossRef] [PubMed]
- Elkhateeb, S.M.; Awad, S.S. Accuracy of panoramic radiographic predictor signs in the assessment of proximity of impacted third molars with the mandibular canal. J. Taibah Univ. Med. Sci. 2018, 13, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Jo, Y.J.; Choi, J.S.; Kim, H.J.; Kim, J.; Moon, S.Y. Anatomical risk factors of inferior alveolar nerve injury association with surgical extraction of mandibular third molar in Korean population. Appl. Sci. 2021, 11, 816. [Google Scholar] [CrossRef]
- Ghai, S.; Choudhury, S. Role of panoramic imaging and cone beam ct for assessment of inferior alveolar nerve exposure and subsequent paresthesia following removal of impacted mandibular third molar. J. Maxillofac. Oral Surg. 2018, 17, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Sghaireen, M.G.; Srivastava, K.C.; Shrivastava, D.; Ganji, K.K.; Patil, S.R.; Abuonq, A.; Mousa, M.A.; Dar-Odeh, N.; Sghaireen, G.M.; Kamal, M.A.; et al. A CBCT based three-dimensional assessment of mandibular posterior region for evaluating the possibility of bypassing the inferior alveolar nerve while placing dental implants. Diagnostics 2020, 10, 406. [Google Scholar] [CrossRef]
- Neves, F.S.; Souza, T.C.; Almeida, S.M.; Haiter-Neto, F.; Freitas, D.Q.; Boscolo, F.N. Correlation of panoramic radiography and cone beam CT findings in the assessment of the relationship between impacted mandibular third molars and the mandibular canal. Dentomaxillofac. Radiol. 2012, 41, 553–557. [Google Scholar] [CrossRef] [Green Version]
- Zain-Alabdeen, E.H.; Alhazmi, R.A.; Alsaedi, R.N.; Alouf, A.A.; Alahmady, O.A. Preoperative cone beam computed tomography evaluation of mandibular second and third molars in relation to the inferior alveolar canal. Saudi J. Health Sci. 2020, 9, 243–247. [Google Scholar] [CrossRef]
- Kubota, S.; Imai, T.; Nakazawa, M.; Uzawa, N. Risk stratification against inferior alveolar nerve injury after lower third molar extraction by scoring on cone-beam computed tomography image. Odontology 2020, 108, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Liu, J.; Pei, J.; Liu, Y.; Pan, J. The risk factors that can increase possibility of mandibular canal wall damage in adult: A cone-beam computed tomography (CBCT) study in a Chinese population. Med. Sci. Monit. 2018, 24, 26–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, N.; van Wijk, A.; Berkhout, E.; Sanderink, G.; De Lange, J.; Wang, H.; van der Heijden, G.J. Predictive value of panoramic radiography for injury of inferior alveolar nerve after mandibular third molar surgery. J. Oral Maxillofac. Surg. 2017, 75, 663–679. [Google Scholar] [CrossRef]
- Rood, J.P.; Shehab, B.A. The radiological prediction of inferior alveolar nerve injury during third molar surgery. Br. J. Oral Maxillofac. Surg. 1990, 28, 20–25. [Google Scholar] [CrossRef]
- Palma-Carrio, C.; Garcia-Mira, B.; Larrazabal-Moron, C.; Penarrocha-Diago, M. Radiographic signs associated with inferior alveolar nerve damage following lower third molar extraction. Med. Oral Patol. Oral Cir. Bucal. 2010, 15, e886–e890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, P.S.; Shah, J.S.; Dudhia, B.B.; Butala, P.B.; Jani, Y.V.; Macwan, R.S. Comparison of panoramic radiograph and cone beam computed tomography findings for impacted mandibular third molar root and inferior alveolar nerve canal relation. Indian J. Dent. Res. 2020, 31, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Qassadi, T.M.; Shafei, A.A.; Alhazmi, A.A.; Odabi, N.I. Prevalence and pattern of third molar impaction among the Saudi Population in Jazan Region, Saudi Arabia. Saudi J. Oral Dent. Res. 2020, 5, 36–42. [Google Scholar] [CrossRef]
- Tantanapornkul, W.; Okouchi, K.; Fujiwara, Y.; Yamashiro, M.; Maruoka, Y.; Ohbayashi, N.; Kurabayashi, T. A comparative study of cone-beam computed tomography and conventional panoramic radiography in assessing the topographic relationship between the mandibular canal and impacted third molars. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Winter, G.B. Impacted Mandibular Third Molar. American Medical Book Company: St. Louis, MO, USA, 1926; pp. 241–279. [Google Scholar]
- Ghaeminia, H.; Meijer, G.J.; Soehardi, A.; Borstlap, W.A.; Mulder, J.; Berge, S.J. Position of the impacted third molar in relation to the mandibular canal. Diagnostic accuracy of cone beam computed tomography compared with panoramic radiography. Int. J. Oral Maxillofac. Surg. 2009, 38, 964–971. [Google Scholar] [CrossRef]
- Sedaghatfar, M.; August, M.A.; Dodson, T.B. Panoramic radiographic findings as predictors of inferior alveolar nerve exposure following third molar extraction. J. Oral Maxillofac. Surg. 2005, 63, 3–7. [Google Scholar] [CrossRef]
- Gomes, A.C.; Vasconcelos, B.C.; Silva, E.D.; Ade, F.C., Jr.; Neto, I.C.P. Sensitivity and specificity of pantomography to predict inferior alveolar nerve damage during extraction of impacted lower third molars. J. Oral Maxillofac. Surg. 2008, 66, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Szalma, J.; Lempel, E.; Jeges, S.; Szabó, G.; Olasz, L. The prognostic value of panoramic radiography of inferior alveolar nerve damage after mandibular third molar removal: Retrospective study of 400 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Halli, R.; Gadre, P.; Gadre, K.S. Correlation of panoramic radiographs and spiral CT scan in the preoperative assessment of intimacy of the inferior alveolar canal to impacted mandibular third molars. J. Craniofac. Surg. 2011, 22, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Monaco, G.; Montevecchi, M.; Bonetti, G.A.; Gatto, M.R.; Checchi, L. Reliability of panoramic radiography in evaluating the topographic relationship between the mandibular canal and impacted third molars. J. Am. Dent. Assoc. 2004, 135, 312–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerjes, W.; El-Maaytah, M.; Swinson, B.; Upile, T.; Thompson, G.; Gittelmon, S.; Baldwin, D.; Hadi, H.; Vourvachis, M.; Abizadeh, N.; et al. Inferior alveolar nerve injury and surgical difficulty prediction in third molar surgery: The role of dental panoramic tomography. J. Clin. Dent. 2006, 17, 122–130. [Google Scholar] [PubMed]
- Hasani, A.; Ahmadi Moshtaghin, F.; Roohi, P.; Rakhshan, V. Diagnostic value of cone beam computed tomography and panoramic radiography in predicting mandibular nerve exposure during third molar surgery. Int. J. Oral Maxillofac. Surg. 2017, 46, 230–235. [Google Scholar] [CrossRef]
- Blaeser, B.F.; August, M.A.; Donoff, R.B.; Kaban, L.B.; Dodson, T.B. Panoramic radiographic risk factors for inferior alveolar nerve injury after third molar extraction. J. Oral Maxillofac. Surg. 2003, 61, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Pandey, R.; Ravindran, C.; Pandiyan, D.; Gupta, A.; Aggarwal, A.; Aryasri, S. Assessment of Roods and Shehab criteria if one or more radiological signs are present in orthopantomogram and position of the mandibular canal in relation to the third molar apices using cone beam computed tomography: A radiographic study. Tanta Dent. J. 2018, 15, 33–38. [Google Scholar] [CrossRef]
- Jhamb, A.; Dolas, R.S.; Pandilwar, P.K.; Mohanty, S. Comparative efficacy of spiral computed tomography and orthopantomography in preoperative detection of relation of inferior alveolar neurovascular bundle to the impacted mandibular third molar. J. Oral Maxillofac. Surg. 2009, 67, 58–66. [Google Scholar] [CrossRef]
- Szalma, J.; Lempel, E.; Jeges, S.; Olasz, L. Darkening of third molar roots: Panoramic radiographic associations with inferior alveolar nerve exposure. J. Oral Maxillofac. Surg. 2011, 69, 1544–1549. [Google Scholar] [CrossRef] [PubMed]
- Bell, G.W. Use of dental panoramic tomographs to predict the relation between mandibular third molar teeth and the inferior alveolar nerve. Radiological and surgical findings, and clinical outcome. Br. J. Oral Maxillofac. Surg. 2004, 42, 21–27. [Google Scholar] [CrossRef]
- Nakamori, K.; Fujiwara, K.; Miyazaki, A.; Tomihara, K.; Tsuji, M.; Nakai, M.; Michifuri, Y.; Suzuki, R.; Komai, K.; Shimanishi, M.; et al. Clinical assessment of the relationship between the third molar and the inferior alveolar canal using panoramic images and computed tomography. J. Oral Maxillofac. Surg. 2008, 66, 2308–2313. [Google Scholar] [CrossRef]
- Fauzi, A.A.; Nazimi, A.J.; Rashdi, M.F.; Fouzi, N.; Kamarudin, N.A.; Ramli, R. Interruption regions in the white line: A novel panoramic finding in the risk assessment of mandibular canal exposure by third molar. J. Clin. Diagn. Res. 2019, 13, ZC01–ZC07. [Google Scholar] [CrossRef]
- Ueda, M.; Nakamori, K.; Shiratori, K.; Igarashi, T.; Sasaki, T.; Anbo, N.; Kaneko, T.; Suzuki, N.; Dehari, H.; Sonoda, T.; et al. Clinical significance of computed tomographic assessment and anatomic features of the inferior alveolar canal as risk factors for injury of the inferior alveolar nerve at third molar surgery. J. Oral Maxillofac. Surg. 2012, 70, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Susarla, S.M.; Sidhu, H.K.; Avery, L.L.; Dodson, T.B. Does computed tomographic assessment of inferior alveolar canal cortical integrity predict nerve exposure during third molar surgery? J. Oral Maxillofac. Surg. 2010, 68, 1296–1303. [Google Scholar] [CrossRef]
- Nakamori, K.; Tomihara, K.; Noguchi, M. Clinical significance of computed tomography assessment for third molar surgery. World. J. Radiol. 2014, 6, 417–423. [Google Scholar] [CrossRef]
- Park, W.; Choi, J.W.; Kim, J.Y.; Kim, B.C.; Kim, H.J.; Lee, S.H. Cortical integrity of the inferior alveolar canal as a predictor of paresthesia after third-molar extraction. J. Am. Dent. Assoc. 2010, 141, 271–278. [Google Scholar] [CrossRef]
- Nakayama, K.; Nonoyama, M.; Takaki, Y.; Kagawa, T.; Yuasa, K.; Izumi, K.; Ozeki, S.; Ikebe, T. Assessment of the relationship between impacted mandibular third molars and inferior alveolar nerve with dental 3-dimensional computed tomography. J. Oral Maxillofac. Surg. 2009, 67, 2587–2591. [Google Scholar] [CrossRef]
- Waseem, N.; Asim, M.A.; Maqsood, A.; Ghafoor, M.W.; Mirza, N.; Khalid, M.O. Evaluation of patterns of impacted third molars and their association with vital structures by radiographic examination. Pak. Armed Forces Med. J. 2021, 71, 255–260. [Google Scholar] [CrossRef]
- Kursun, S.; Hakan, K.M.; Bengi, O.; Nihat, A. Use of cone beam computed tomography to determine the accuracy of panoramic radiological markers: A pilot study. J. Dent. Sci. 2015, 10, 167–171. [Google Scholar] [CrossRef] [Green Version]
- Dalili, Z.; Mahjoub, P.; Sigaroudi, A.K. Comparison between cone beam computed tomography and panoramic radiography in the assessment of the relationship between the mandibular canal and impacted class C mandibular third molars. Dent. Res. J. (Isfahan) 2011, 8, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Saha, N.; Kedarnath, N.S.; Singh, M. Orthopantomography and cone-beam computed tomography for the relation of inferior alveolar nerve to the impacted mandibular third molars. Ann. Maxillofac. Surg. 2019, 9, 4–9. [Google Scholar] [CrossRef]
- Bigagnoli, S.; Greco, C.; Costantinides, F.; Porrelli, D.; Bevilacqua, L.; Maglione, M. CBCT radiological features as predictors of nerve injuries in third molar extractions: Multicenter prospective study on a northeastern Italian population. Dent. J. 2021, 9, 23. [Google Scholar] [CrossRef]
- Maegawa, H.; Sano, K.; Kitagawa, Y.; Ogasawara, T.; Miyauchi, K.; Sekine, J.; Inokuchi, T. Pre-operative assessment of the relationship between the mandibular third molar and the mandibular canal by axial computed tomography with coronal and sagittal reconstruction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 639–646. [Google Scholar] [CrossRef]
- Wang, W.Q.; Chen, M.Y.; Huang, H.L.; Fuh, L.J.; Tsai, M.T.; Hsu, J.T. New quantitative classification of the anatomical relationship between impacted third molars and the inferior alveolar nerve. BMC Med. Imaging 2015, 15, 59. [Google Scholar] [CrossRef] [Green Version]
- Yabroudi, F.; Pedersen, S.S. Cone beam tomography (CBCT) as a diagnostic tool to assess the relationship between the inferior alveolar nerve and roots of mandibular wisdom teeth. Smile Dent. J. 2012, 7, 12–16. [Google Scholar]
- Pippi, R.; Santoro, M. A multivariate statistical analysis on variables affecting inferior alveolar nerve damage during third molar surgery. Br. Dent. J. 2015, 219, E3. [Google Scholar] [CrossRef]
- Salam, S.; Rehman, A.Z.U.; Alam, S.; Jamil, Y.; Irshad, M. Relative position of mandibular third molar and inferior alveolar nerve using cone beam computed tomography. Isra Med. J. 2020, 12, 208–210. [Google Scholar]
- Nemsia, H.; Tellili, N.; Bouanene, I.; Tlili, M.; Khenfir, F.; Khalfi, M.S.; ben Amor, F. Classification of impacted mandibular third molars using cone beam computed tomography based on neurological risks: NRC. Med. Buccale Chir. Buccale 2017, 23, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Xu, G.Z.; Yang, C.; Fan, X.D.; Yu, C.Q.; Cai, X.Y.; Wang, Y.; He, D. Anatomic relationship between impacted third mandibular molar and the mandibular canal as the risk factor of inferior alveolar nerve injury. Br. J. Oral Maxillofac. Surg. 2013, 51, e215–e219. [Google Scholar] [CrossRef]
- Quek, S.L.; Tay, C.K.; Tay, K.H.; Toh, S.L.; Lim, K.C. Pattern of third molar impaction in a Singapore Chinese population: A retrospective radiographic survey. Int. J. Oral Maxillofac. Surg. 2003, 32, 548–552. [Google Scholar] [CrossRef]
- Cheung, L.K.; Leung, Y.Y.; Chow, L.K.; Wong, M.C.; Chan, E.K.; Fok, Y.H. Incidence of neurosensory deficits and recovery after lower third molar surgery: A prospective clinical study of 4338 cases. Int. J. Oral Maxillofac. Surg. 2010, 39, 320–326. [Google Scholar] [CrossRef] [Green Version]
- Bozzatello, J. Relationship between craniofacial architecture and retained lower third molar. Its’ symptomatology. Rev. Fac. Cienc. Med. (Cordoba Argent.) 2006, 63, 38–42. [Google Scholar]
- Deshpande, P.; VGuledgud, M.; Patil, K. Proximity of impacted mandibular third molars to the inferior alveolar canal and its radiographic predictors: A panoramic radiographic study. J. Maxillofac. Oral Surg. 2013, 12, 145–151. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, E.; Grubor, D.; Chandu, A. Risk factors for permanent injury of inferior alveolar and lingual nerves during third molar surgery. J. Oral Maxillofac. Surg. 2014, 72, 2394–2401. [Google Scholar] [CrossRef]
- Bataineh, A.B.; Albashaireh, Z.S.; Hazza’a, A.M. The surgical removal of mandibular third molars: A study in decision making. Quintessence Int. 2002, 33, 613–617. [Google Scholar] [PubMed]
- Almendros-Marques, N.; Berini-Aytes, L.; Gay-Escoda, C. Influence of lower third molar position on the incidence of preoperative complications. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 725–732. [Google Scholar] [CrossRef]
- Selvi, F.; Dodson, T.B.; Nattestad, A.; Robertson, K.; Tolstunov, L. Factors that are associated with injury to the inferior alveolar nerve in high-risk patients after removal of third molars. Br. J. Oral Maxillofac. Surg. 2013, 51, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, Y.T.; Kayıpmaz, S.; Senel, F.C.; Atasoy, K.T.; Gumrukcu, Z. Does additional cone beam computed tomography decrease the risk of inferior alveolar nerve injury in high-risk cases undergoing third molar surgery? Does CBCT decrease the risk of IAN injury? Int. J. Oral Maxillofac. Surg. 2017, 46, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Ri, S.; Shigeta, T.; Akashi, M.; Imai, Y.; Kakei, Y.; Shibuya, Y.; Komori, T. Risk factors associated with inferior alveolar nerve injury after extraction of the mandibular third molar—A comparative study of pre-operative images by panoramic radiography and computed tomography. Int. J. Oral Maxillofac. Surg. 2013, 42, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Shiratori, K.; Nakamori, K.; Ueda, M.; Sonoda, T.; Dehari, H. Assessment of the shape of the inferior alveolar canal as a marker for increased risk of injury to the inferior alveolar nerve at third molar surgery: A prospective study. J. Oral Maxillofac. Surg. 2013, 71, 2012–2019. [Google Scholar] [CrossRef] [PubMed]
- Tay, A.B.; Go, W.S. Effect of exposed inferior alveolar neurovascular bundle during surgical removal of impacted lower third molars. J. Oral Maxillofac. Surg. 2004, 62, 592–600. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Presence of Cortication n (%) | Absence of Cortication n (%) | Total Number of Cases n (%) | p Value | |
|---|---|---|---|---|---|
| Age | ≤30 years | 42 (31.8) | 90 (68.2) | 132 (37.7) | 0.503 |
| >30 years | 62 (28.4) | 156 (71.6) | 218 (62.3) | ||
| Sex | Male | 65 (31.4) | 142 (68.6) | 207 (59.1) | 0.553 |
| Female | 39 (27.3) | 104 (72.7) | 143 (40.9) | ||
| Site of mandibular third molar | Left | 57 (32%) | 121 (68%) | 178 (50.9) | 0.429 |
| Right | 47 (27.3%) | 125 (72.7%) | 172 (49.1) | ||
| Winter’s classification for angulation of impacted mandibular third molar | Mesio-angular | 51 (26.6) | 141 (73.4) | 192 (54.9) | 0.141 |
| Disto-angular | 3 (17.6) | 14 (82.4) | 17 (4.9) | ||
| Horizontal | 19 (32.2) | 40 (67.8) | 59 (16.8) | ||
| Vertical | 31 (37.8) | 51 (62.2) | 82 (23.4) | ||
| Position of IAC in relation to the mandibular third molar | Buccal side | 85 (50.6) | 83 (49.4) | 168 (48.0) | 0.003 |
| Lingual side | 8 (7.6) | 97 (92.4) | 105 (30.0) | ||
| Inferior | 11 (16.9) | 54 (83.1) | 65 (18.6) | ||
| Inter-radicular | 00 (0.0) | 12 (100) | 12 (3.4) | ||
| Signs on Panoramic Images | Presence of Cortication n (%) | Absence of Cortication n (%) | Total Number of Cases n (%) | p Value |
|---|---|---|---|---|
| Interruption of white line | 63 (35.2) | 116 (64.8) | 179 (51.1) | 0.047 |
| Darkening of roots | 21 (30.4) | 48 (69.6) | 69 (19.7) | |
| Diversion of mandibular canal | 3 (10.7) | 25 (89.3) | 28 (8.0) | |
| Narrowing of mandibular canal | 17 (29.8) | 40 (70.2) | 57 (16.3) | |
| DR + DMC | 0 (0.0) | 3(100) | 3 (0.9) | |
| DR + NMC | 0 (0.0) | 1(100) | 1 (0.3) | |
| DR + IWL | 0 (0.0) | 8(100) | 8 (2.3) | |
| DMC + NMC | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| DMC + IWL | 0 (0.0) | 1(100) | 1 (0.3) | |
| NMC + IWL | 0 (0.0) | 4(100) | 4 (1.1) | |
| Total | 104 (29.7) | 246 (70.3) | 350 (100) |
| Variables | B | S.E. | Wald | df | Sig. | Exp (B) | 95% C.I. for EXP(B) | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Interruption of white line | 5.298 | 8 | 0.725 | |||||
| Darkening of roots | −18.515 | 19,898.166 | 0.000 | 1 | 0.999 | 0.000 | 0.000 | |
| Diversion of mandibular canal | −19.044 | 19,898.166 | 0.000 | 1 | 0.999 | 0.000 | 0.000 | |
| Narrowing of mandibular canal | −17.836 | 19,898.166 | 0.000 | 1 | 0.999 | 0.000 | 0.000 | |
| DR + DMC | −19.787 | 19,898.166 | 0.000 | 1 | 0.999 | 0.000 | 0.000 | |
| DR + NMC | 0.545 | 30,568.425 | 0.000 | 1 | 1.000 | 1.725 | 0.000 | |
| DR + IWL | 0.545 | 44,848.767 | 0.000 | 1 | 1.000 | 1.725 | 0.000 | |
| DMC + IWL | −0.242 | 24,451.408 | 0.000 | 1 | 1.000 | 0.785 | 0.000 | |
| NMC + IWL | −0.242 | 44,848.767 | 0.000 | 1 | 1.000 | 0.785 | 0.000 | |
| Position of IAC | 3.787 | 5.682 | 2.334 | 1 | 0.0248 | 2.197 | 0.578 | 8.356 |
| Constant | 18.296 | 19,898.166 | 0.000 | 1 | 0.999 | 88,284,625.327 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Issrani, R.; Prabhu, N.; Sghaireen, M.; Alshubrmi, H.R.; Alanazi, A.M.; Alkhalaf, Z.A.; Alnusayri, M.O.; Aljohani, F.M.; Khan, Z.A. Comparison of Digital OPG and CBCT in Assessment of Risk Factors Associated with Inferior Nerve Injury during Mandibular Third Molar Surgery. Diagnostics 2021, 11, 2282. https://doi.org/10.3390/diagnostics11122282
Issrani R, Prabhu N, Sghaireen M, Alshubrmi HR, Alanazi AM, Alkhalaf ZA, Alnusayri MO, Aljohani FM, Khan ZA. Comparison of Digital OPG and CBCT in Assessment of Risk Factors Associated with Inferior Nerve Injury during Mandibular Third Molar Surgery. Diagnostics. 2021; 11(12):2282. https://doi.org/10.3390/diagnostics11122282
Chicago/Turabian StyleIssrani, Rakhi, Namdeo Prabhu, Mohammed Sghaireen, Hasna Rasheed Alshubrmi, Amal Mohamed Alanazi, Zainab Ali Alkhalaf, Mohammed Odhayd Alnusayri, Fahad Muqbil Aljohani, and Zafar A. Khan. 2021. "Comparison of Digital OPG and CBCT in Assessment of Risk Factors Associated with Inferior Nerve Injury during Mandibular Third Molar Surgery" Diagnostics 11, no. 12: 2282. https://doi.org/10.3390/diagnostics11122282