
Contrast-Enhanced Ultrasound for Precise Sentinel Lymph Node Biopsy in Women with Early Breast Cancer: A Preliminary Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Instrument and Contrast Agent
2.3. Contrast-Enhanced Ultrasound
2.4. Conventional Ultrasound
2.5. SLNB Process
2.6. Statistics
3. Results
3.1. Patients Demographic Characteristics
3.2. Identification of SLN by CEUS or Blue Stain
3.3. Lymphatic Drainage Patterns to SLNs
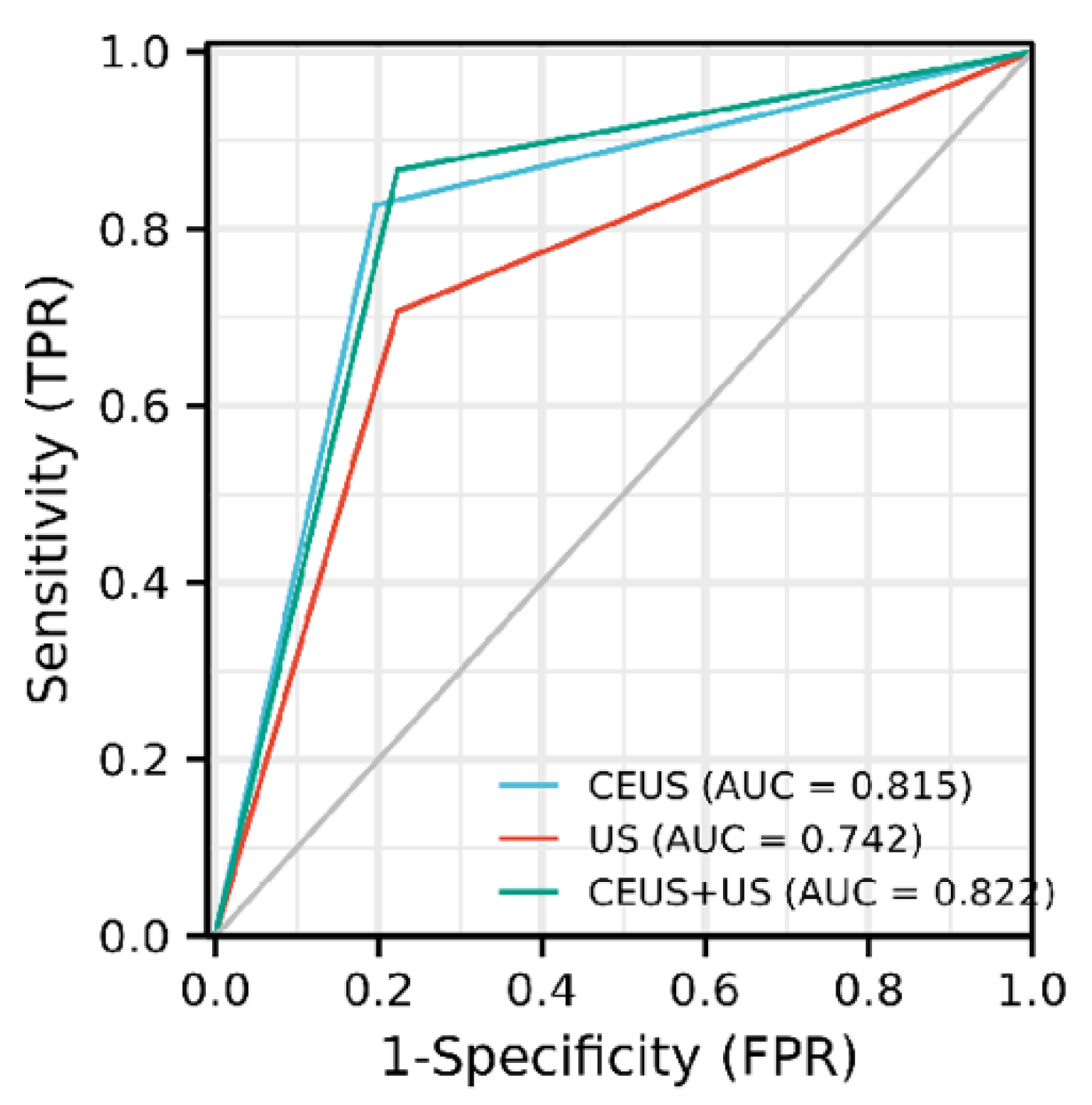
3.4. Diagnostic Performance of CEUS, US, and CEUS + US for SLN Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Burstein, H.J.; Winer, E.P.; Gnant, M.; Dubsky, P.; Loibl, S.; Colleoni, M.; Regan, M.M.; Piccart-Gebhart, M.; Senn, H.-J. De-escalating and escalating treatments for early-stage breast cancer: The St. Gallen International Expert Consensus Conference on the Primary Therapy of Early Breast Cancer 2017. Ann. Oncol. 2017, 28, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Kuijer, A.; Dominici, L.S.; Rosenberg, S.M.; Hu, J.; Gelber, S.; Di Lascio, S.; Wong, J.S.; Ruddy, K.J.; Tamimi, R.M.; Schapira, L. Arm Morbidity After Local Therapy for Young Breast Cancer Patients. Ann. Surg. Oncol. 2021, 28, 6071–6082. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, S.Q.; Zhang, G.J.; Jansen, L.; de Vries, J.; Schröder, C.P.; de Vries, E.G.; van Dam, G.M. Evolution in sentinel lymph node biopsy in breast cancer. Crit. Rev. Oncol. Hematol. 2018, 123, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Niebling, M.G.; Pleijhuis, R.G.; Bastiaannet, E.; Brouwers, A.H.; Van Dam, G.M.; Hoekstra, H.J. A systematic review and meta-analyses of sentinel lymph node identification in breast cancer and melanoma, a plea for tracer mapping. Eur. J. Surg. Oncol. 2016, 42, 466–473. [Google Scholar] [CrossRef]
- Wang, Z.; Cui, Y.; Zheng, M.; Ge, H.; Huang, Y.; Peng, J.; Xie, H.; Wang, S. Comparison of indocyanine green fluorescence and methylene blue dye in the detection of sentinel lymph nodes in breast cancer. Gland Surg. 2020, 9, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- Mansel, R.E.; Fallowfield, L.; Kissin, M.; Goyal, A.; Newcombe, R.G.; Dixon, J.M.; Yiangou, C.; Horgan, K.; Bundred, N.; Monypenny, I. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: The ALMANAC Trial. J. Natl. Cancer Inst. 2006, 98, 599–609. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; He, Y.; Wang, J.; Huo, L.; Fan, Z.; Li, J.; Xie, Y.; Wang, T.; Ouyang, T. Feasibility of using negative ultrasonography results of axillary lymph nodes to predict sentinel lymph node metastasis in breast cancer patients. Cancer Med. 2018, 7, 3066–3072. [Google Scholar] [CrossRef]
- Honda, K.; Ishiyama, K.; Suzuki, S.; Kawasaki, Y.; Saito, H.; Horii, A. Sentinel Lymph Node Biopsy Using Preoperative Computed Tomographic Lymphography and Intraoperative Indocyanine Green Fluorescence Imaging in Patients with Localized Tongue Cancer. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 735–740. [Google Scholar] [CrossRef]
- Wen, S.; Liang, Y.; Kong, X.; Liu, B.; Ma, T.; Zhou, Y.; Jiang, L.; Li, X.; Yang, Q. Application of preoperative computed tomographic lymphography for precise sentinel lymph node biopsy in breast cancer patients. BMC Surg. 2021, 21, 187. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, X.; He, J.; Gou, B.; Luo, Y.; Deng, S.; Wen, H.; Zhou, L. Percutaneous contrast-enhanced ultrasound for localization and diagnosis of sentinel lymph node in early breast cancer. Sci. Rep. 2019, 9, 13545. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Averkiou, M.; Nielsen, M.B.; Barr, R.G.; Burns, P.N.; Calliada, F.; Cantisani, V.; Choi, B.; Chammas, M.C.; Clevert, D.-A. How to perform Contrast-Enhanced Ultrasound (CEUS). Ultrasound Int. Open 2018, 4, E2–E15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Z.; Cheng, X.; Li, J.; Jiang, J.; Jiang, Z.; Li, H.; Li, T.; Zhang, Z.; Tan, B.; Lu, M. Preliminary study of real-time three-dimensional contrast-enhanced ultrasound of sentinel lymph nodes in breast cancer. Eur. Radiol. 2020, 30, 1426–1435. [Google Scholar] [CrossRef]
- Sharma, N.; Cox, K. Axillary Nodal Staging with Contrast-Enhanced Ultrasound. Curr. Breast Cancer Rep. 2017, 9, 259–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coronado-Gutiérrez, D.; Santamaría, G.; Ganau, S.; Bargalló, X.; Orlando, S.; Oliva-Brañas, M.E.; Perez-Moreno, A.; Burgos-Artizzu, X.P. Quantitative Ultrasound Image Analysis of Axillary Lymph Nodes to Diagnose Metastatic Involvement in Breast Cancer. Ultrasound Med. Biol. 2019, 45, 2932–2941. [Google Scholar] [CrossRef]
- Wallis, M.G.; Kilburn-Toppin, F.; Taylor-Phillips, S. Does preoperative axillary staging lead to overtreatment of women with screen-detected breast cancer? Clin. Radiol. 2018, 73, 467–472. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Li, Y.; Mao, F.; Zhang, J.; Zhu, Q.; Shen, S.; Lin, Y.; Zhang, X.; Liu, H.; Xiao, M. Preliminary study of contrast-enhanced ultrasound in combination with blue dye vs. indocyanine green fluorescence, in combination with blue dye for sentinel lymph node biopsy in breast cancer. BMC Cancer 2019, 19, 939. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Zhou, W.; Li, C.; Gong, H.; Li, C.; Yang, N.; Zha, X.; Chen, L.; Xia, T.; Liu, X. Variation of sentinel lymphatic channels (SLCs) and sentinel lymph nodes (SLNs) assessed by contrast-enhanced ultrasound (CEUS) in breast cancer patients. World J. Surg. Oncol. 2017, 15, 127. [Google Scholar] [CrossRef]
- Luo, J.; Feng, L.; Zhou, Q.; Chen, Q.; Liu, J.; Wu, C.; Luo, J.; Chen, J.; Wu, H.; Deng, W. The value of contrast-enhanced ultrasound in determining the location of sentinel lymph nodes in breast cancer. Cancer Imaging 2021, 21, 28. [Google Scholar] [CrossRef]
- Giuliano, A.E.; Hunt, K.K.; Ballman, K.V.; Beitsch, P.D.; Whitworth, P.W.; Blumencranz, P.W.; Leitch, A.M.; Saha, S.; McCall, L.M.; Morrow, M. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: A randomized clinical trial. Jama 2011, 305, 569–575. [Google Scholar] [CrossRef] [Green Version]
- Xie, F.; Zhang, D.; Cheng, L.; Yu, L.; Yang, L.; Tong, F.; Liu, H.; Wang, S.; Wang, S. Intradermal microbubbles and contrast-enhanced ultrasound (CEUS) is a feasible approach for sentinel lymph node identification in early-stage breast cancer. World J. Surg. Oncol. 2015, 13, 319. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhang, J.; Zhu, Q.L.; Jiang, Y.X.; Sun, Q.; Zhou, Y.D.; Wang, M.Q.; Meng, Z.L.; Mao, X.X. The value of contrast-enhanced ultrasound for sentinel lymph node identification and characterisation in pre-operative breast cancer patients: A prospective study. Eur. Radiol. 2018, 28, 1654–1661. [Google Scholar] [CrossRef] [PubMed]
- Cui, Q.; Dai, L.; Li, J.; Xue, J. Accuracy of CEUS-guided sentinel lymph node biopsy in early-stage breast cancer: A study review and meta-analysis. World J. Surg. Oncol. 2020, 18, 112. [Google Scholar] [CrossRef] [PubMed]
- McMasters, K.M.; Wong, S.L.; Chao, C.; Woo, C.; Tuttle, T.M.; Noyes, R.D.; Carlson, D.J.; Laidley, A.L.; McGlothin, T.Q.; Ley, P.B. Defining the optimal surgeon experience for breast cancer sentinel lymph node biopsy: A model for implementation of new surgical techniques. Ann. Surg. 2001, 234, 292. [Google Scholar] [CrossRef] [PubMed]
- Goel, V.; Raju, K.; Dasu, S.; Nusrath, S. Awareness of Lymphatic Anatomy to Decrease False Negative Sentinel Lymph Node Rate in Breast Cancer. Indian J. Surg. Oncol. 2019, 10, 673–675. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Suga, K.; Maeda, K.; Maeda, N.; Yoshimura, K.; Oka, M. Breast sentinel lymph node navigation with three-dimensional computed tomography-lymphography: A 12-year study. Breast Cancer 2016, 23, 456–462. [Google Scholar] [CrossRef]
- Shimazu, K.; Miyake, T.; Tanei, T.; Naoi, Y.; Shimoda, M.; Kagara, N.; Kim, S.J.; Noguchi, S. Real-Time Visualization of Lymphatic Flow to Sentinel Lymph Nodes by Contrast-Enhanced Ultrasonography with Sonazoid in Patients with Breast Cancer. Ultrasound Med. Biol. 2019, 45, 2634–2640. [Google Scholar] [CrossRef]
- Nielsen Moody, A.; Bull, J.; Culpan, A.M.; Munyombwe, T.; Sharma, N.; Whitaker, M.; Wolstenhulme, S. Preoperative sentinel lymph node identification, biopsy and localisation using contrast enhanced ultrasound (CEUS) in patients with breast cancer: A systematic review and meta-analysis. Clin. Radiol. 2017, 72, 959–971. [Google Scholar] [CrossRef]
- Li, J.; Lu, M.; Cheng, X.; Hu, Z.; Li, H.; Wang, H.; Jiang, J.; Li, T.; Zhang, Z.; Zhao, C. How Pre-operative Sentinel Lymph Node Contrast-Enhanced Ultrasound Helps Intra-operative Sentinel Lymph Node Biopsy in Breast Cancer: Initial Experience. Ultrasound Med. Biol. 2019, 45, 1865–1873. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Patients |
|---|---|
| Patient age (years) | 28~76 |
| Mean age (years) | 51.88 ± 10.61 |
| Menopause status | |
| Premenopausal | 103 |
| Post-menopause | 98 |
| Breast lesions location | |
| Central quadrant | 9 |
| Upper outer quadrant | 84 |
| Upper inner quadrant | 37 |
| Lower outer quadrant | 53 |
| Lower inner quadrant | 18 |
| Tumor size (cm) | 0.52~4.94 |
| Average tumor size (cm) | 2.35 ± 1.10 |
| History | |
| Invasive ductal carcinoma | 141 |
| Invasive lobular carcinoma | 45 |
| Other | 15 |
| Molecular subtypes | |
| Luminal A | 69 |
| Luminal B | 86 |
| HER-2 positive | 33 |
| Triple-negative | 13 |
| No. of SLNs Per Patients | The Number and Percentage of Patients | p |
|---|---|---|
| CEUS(%) | ||
| 1 | 146 (78.07%) | <0.001 |
| 2 | 35 (18.72%) | |
| 3 | 6 (3.21%) | |
| 4 | 0 (0.00%) | |
| 5 | 0 (0.00%) | |
| Total | 187 (100%) |
| Methods | Sen | Spe | PPV | NPV | AUC (95% CI) |
|---|---|---|---|---|---|
| US *,# | 70.67% (53/75) | 77.68% (87/112) | 67.95% (53/78) | 79.82% (87/109) | 0.742 (0.677–0.806) |
| CEUS & | 82.67% (62/75) | 80.36% (90/112) | 73.81% (62/84) | 87.38% (90/103) | 0.815 (0.758–0.872) |
| US + CEUS | 86.67% (65/75) | 77.68% (87/112) | 72.22% (65/90) | 89.69% (87/97) | 0.822 (0.767–0.876) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, Y.; Fan, X.; Yang, D.; Dong, T.; Jia, Y.; Nie, F. Contrast-Enhanced Ultrasound for Precise Sentinel Lymph Node Biopsy in Women with Early Breast Cancer: A Preliminary Study. Diagnostics 2021, 11, 2104. https://doi.org/10.3390/diagnostics11112104
Zhu Y, Fan X, Yang D, Dong T, Jia Y, Nie F. Contrast-Enhanced Ultrasound for Precise Sentinel Lymph Node Biopsy in Women with Early Breast Cancer: A Preliminary Study. Diagnostics. 2021; 11(11):2104. https://doi.org/10.3390/diagnostics11112104
Chicago/Turabian StyleZhu, Yangyang, Xiao Fan, Dan Yang, Tiantian Dong, Yingying Jia, and Fang Nie. 2021. "Contrast-Enhanced Ultrasound for Precise Sentinel Lymph Node Biopsy in Women with Early Breast Cancer: A Preliminary Study" Diagnostics 11, no. 11: 2104. https://doi.org/10.3390/diagnostics11112104