
Valid and Reliable Assessment of Upper Respiratory Tract Specimen Collection Skills during the COVID-19 Pandemic

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Developing the Theoretical and Practical Test
2.2. Participants
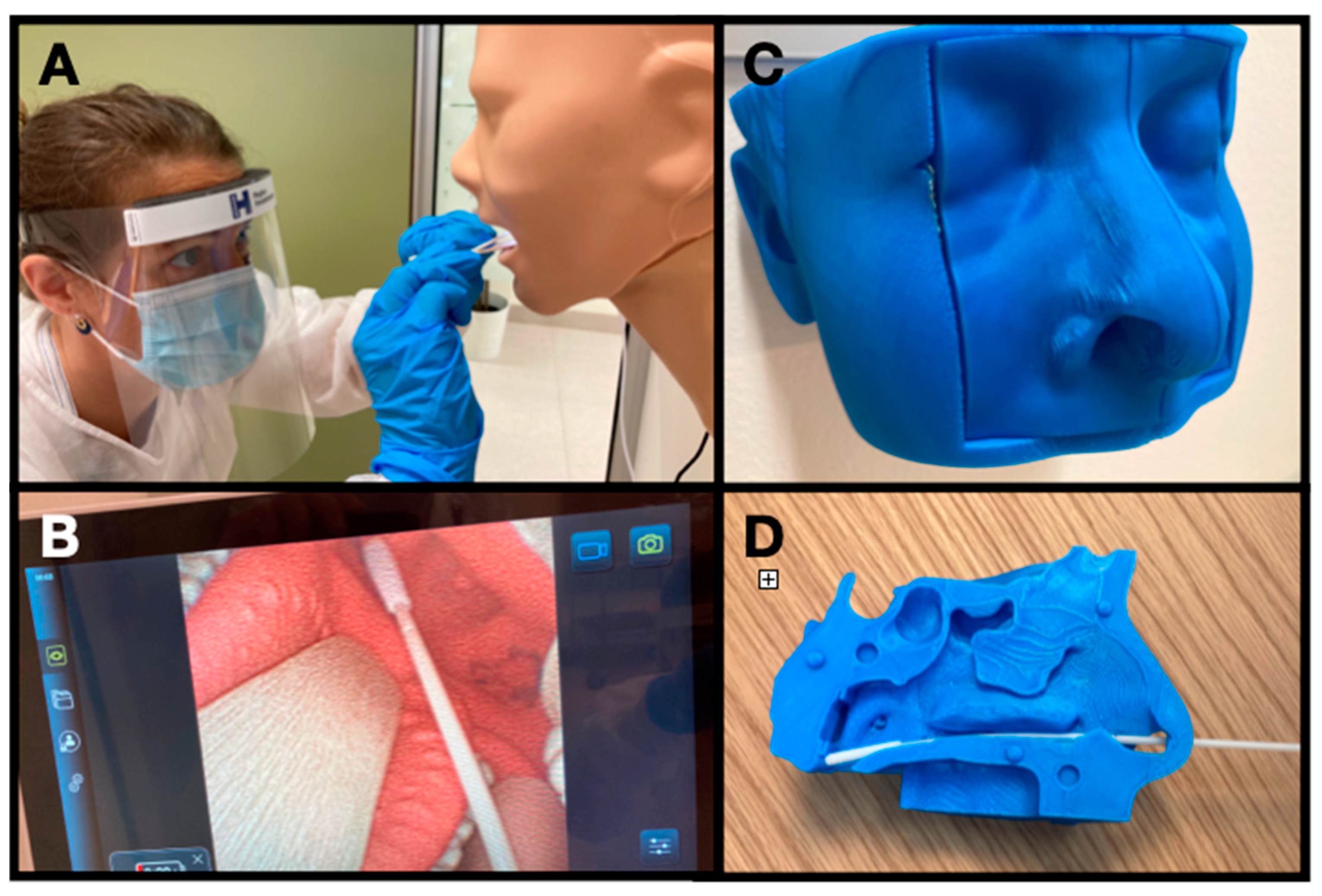
2.3. Test Setup
2.4. OPS and NPS Training of the Group of Novices
2.5. Competence Assessment
2.6. Statistics
3. Results
3.1. Content Evidence
3.2. Response Process
3.3. Internal Structure
3.4. Relations to Other Variables
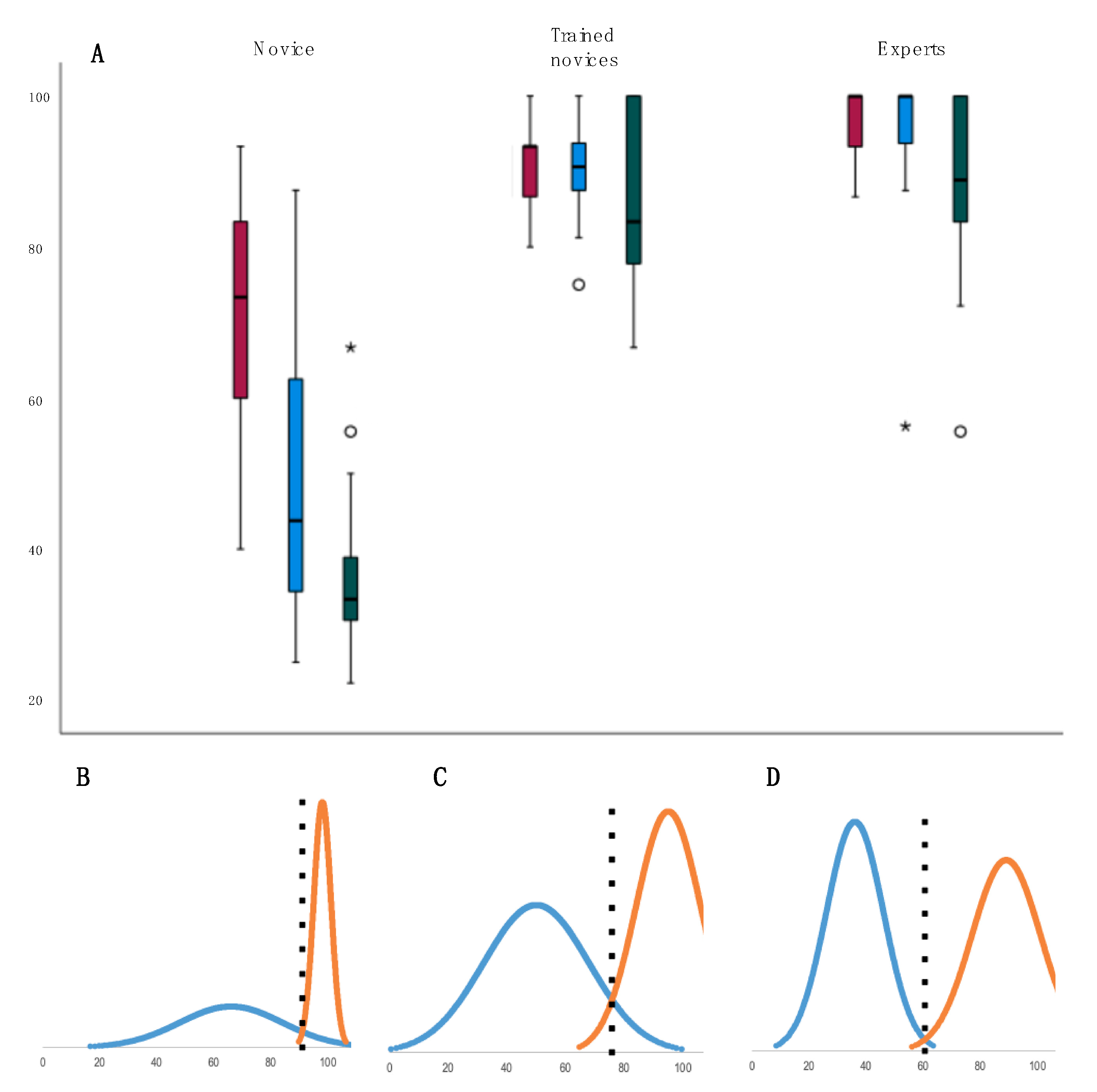
3.5. Test Consequences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
| Name _____________________________ | Correctly Performed | Not Correctly Performed | Not Relevant | |||
| 1 | The swab is performed with correct use of personal protective equipment. | ☐ | ☐ | ☐ | ||
| 2 | The swab is performed in compliance with proper infection prevention and control principles | ☐ | ☐ | ☐ | ||
| 3 | The swab is performed at a height where a good visualization of the oropharyngeal wall is ensured. | ☐ | ☐ | ☐ | ||
| 4 | The swab is held correctly between the thumb and the first and second finger. | ☐ | ☐ | ☐ | ||
| 5 | The patient is instructed in saying “ahhh” or to take a breath so the soft palate will rise. Tongue depressor is used if relevant to improve visualization. | ☐ | ☐ | ☐ | ||
| 6 | The swab is inserted and withdrawn without touching the tongue or cheeks. | ☐ | ☐ | ☐ | ||
| 7 | The swab collects sufficient material from the oropharyngeal wall and both tonsils with a rotating or painting movement. | ☐ | ☐ | ☐ | ||
| 8 | The swab is placed in the vial and managed in accordance with the local guidelines. | ☐ | ☐ | ☐ | ||
| Number correct | _____ | |||||
| General Assesement | bad | unacceptable | acceptable | good | excellent |
| Name __________________________ | Correctly Performed | Not Cerrectly Performed | Not Relevant | |||
| 1 | The swab is performed with correct use of personal protective equipment. | ☐ | ☐ | ☐ | ||
| 2 | The swab is performed in compliance with proper infection prevention and control principles | ☐ | ☐ | ☐ | ||
| 3 | The patient is instructed in leaning the head slightly back throughout the procedure. | ☐ | ☐ | ☐ | ||
| 4 | The tip of the swab enters the nasal cavity correctly (depending on how much the head is leaned back) | ☐ | ☐ | ☐ | ||
| 5 | The swab is inserted in the midline following the floor of the nose (pointing downwards toward the ear). | ☐ | ☐ | ☐ | ||
| 6 | The swab is inserted until resistance is met by the posterior oropharyngeal wall (8-11 cm) | ☐ | ☐ | ☐ | ||
| 7 | The swab is left in place for a second and rotate it three times. | ☐ | ☐ | ☐ | ||
| 8 | The swab is withdrawn slowly while being rotated. | ☐ | ☐ | ☐ | ||
| 9 | The swab is placed in the vial and managed in accordance with the local guidelines. | ☐ | ☐ | ☐ | ||
| Number correct | _____ | |||||
| General Assesement | bad | unacceptable | acceptable | good | excellent |
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Mercer, T.R.; Salit, M. Testing at scale during the COVID-19 pandemic. Nat. Rev. Genet. 2021, 22, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Diagnostic Testing for SARS-CoV-2–Interim Guidance. World Health Organization: Geneva, Switzerland. WHO. Available online: https://apps.who.int/iris/handle/10665/334254?locale-attribute=en (accessed on 25 October 2021).
- Prevention CfDCa. Availabe online: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed on 25 August 2021).
- Higgins, T.S.; Wu, A.W.; Ting, J.Y. SARS-CoV-2 Nasopharyngeal Swab Testing-False-Negative Results From a Pervasive Anatomical Misconception. JAMA Otolaryngol-Head Neck Surg. 2020, 146, 993–994. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Montori, V.M.; Sampathkumar, P. COVID-19 Testing: The Threat of False-Negative Results. Mayo Clin. Proc. 2020, 95, 1127–1129. [Google Scholar] [CrossRef]
- Downing, S.M.; Yudkowsky, R. Assessment in Health Professions Education; Routledge: Oxfordshire, UK, 2009; 336p. [Google Scholar]
- Zedtwitz-Liebenstein, K. Correctly performed nasal swabs. Infection 2021, 49, 763–764. [Google Scholar] [CrossRef] [PubMed]
- Callesen, R.E.; Kiel, C.M.; Hovgaard, L.H.; Jakobsen, K.K.; Papesch, M.; von Buchwald, C.; Todsen, T. Optimal Insertion Depth for Nasal Mid-Turbinate and Nasopharyngeal Swabs. Diagnostics 2021, 11, 1257. [Google Scholar] [CrossRef]
- Pondaven-Letourmy, S.; Alvin, F.; Boumghit, Y.; Simon, F. How to perform a nasopharyngeal swab in adults and children in the COVID-19 era. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2020, 137, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Petruzzi, G.; De Virgilio, A.; Pichi, B.; Mazzola, F.; Zocchi, J.; Mercante, G.; Spriano, G.; Pellini, R. COVID-19: Nasal and oropharyngeal swab. Head Neck 2020, 42, 1303–1304. [Google Scholar] [CrossRef] [PubMed]
- Marty, F.M.; Chen, K.; Verrill, K.A. How to Obtain a Nasopharyngeal Swab Specimen. N. Engl. J. Med. 2020, 382, e76. [Google Scholar] [CrossRef]
- Kaufman, A.C.; Brewster, R.; Rajasekaran, K. How to Perform a Nasopharyngeal Swab-An Otolaryngology Perspective. Am. J. Med. 2020, 133, 1280–1282. [Google Scholar] [CrossRef] [PubMed]
- Fazio, E.; Abousiam, M.; Caselli, A.; Accorona, R.; Nebiaj, A.; Ermoli, I.; Erckert, B.; Calabrese, L.; Gazzini, L. Proper Procedures for Performing Nasopharyngeal and Oropharyngeal Swabs for COVID-19. ATS Sch. 2020, 1, 495–497. [Google Scholar] [CrossRef]
- Di Maio, P.; Iocca, O.; Cavallero, A.; Giudice, M. Performing the nasopharyngeal and oropharyngeal swab for 2019-novel coronavirus (SARS-CoV-2) safely: How to dress, undress, and technical notes. Head Neck 2020, 42, 1548–1551. [Google Scholar] [CrossRef] [PubMed]
- Todsen, T. Collecting of upper respiratory specimens for COVID-19 Testing. Ugeskr Laeger 2021, 183, V03210265. [Google Scholar]
- Sananes, N.; Lodi, M.; Koch, A.; Lecointre, L.; Sananes, A.; Lefebvre, N.; Debry, C. 3D-printed simulator for nasopharyngeal swab collection for COVID-19. Eur. Arch. Oto-Rhino-Laryngol. 2020, 278, 2649–2651. [Google Scholar] [CrossRef]
- Collecting of upper respiratory specimens for COVID-19 Testing. Availabe online: www.urt-sample.com (accessed on 25 October 2021).
- Jorgensen, M.; Konge, L.; Subhi, Y. Contrasting groups’ standard setting for consequences analysis in validity studies: Reporting considerations. Adv. Simul. 2018, 3, 5. [Google Scholar] [CrossRef] [PubMed]
- Hodges, B.; Regehr, G.; McNaughton, N.; Tiberius, R.; Hanson, M. OSCE checklists do not capture increasing levels of expertise. Acad. Med. 1999, 74, 1129–1134. [Google Scholar] [CrossRef]
- Abud, B.T.; Hajnas, N.M.; Redleaf, M.; Kerolus, J.L.; Lee, V. Assessing the Impact of a Training Initiative for Nasopharyngeal and Oropharyngeal Swabbing for COVID-19 Testing. OTO Open 2020, 4, 2473974X20953094. [Google Scholar] [CrossRef] [PubMed]
- Mathews, S.S.; Varghese, L.; Trupthi, M.C.; Naomi, N.; Varghese, A.M. Covid 19 Pandemic-Training of Healthcare Workers in Obtaining a Nasopharyngeal Swab: Our Experience. Indian J. Otolaryngol. Head Neck Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Roychowdhury, P.; Ito, C.J. Role of the otolaryngologist in nasopharyngeal swab training: A case report and review of the literature. Otolaryngol. Case Rep. 2021, 20, 100316. [Google Scholar] [CrossRef]
- Todsen, T.; Kirkby, N.; Benfield, T. Is oropharyngeal sampling a reliable test to detect SARS-CoV-2? Lancet Infect. Dis. 2021, 21, 1348. [Google Scholar] [CrossRef]
- Tsang, N.N.Y.; So, H.C.; Ng, K.Y.; Cowling, B.J.; Leung, G.M.; Ip, D.K.M. Diagnostic performance of different sampling approaches for SARS-CoV-2 RT-PCR testing: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 1233–1245. [Google Scholar] [CrossRef]
- Todsen, T.; Henriksen, M.V.; Kromann, C.B.; Konge, L.; Eldrup, J.; Ringsted, C. Short- and long-term transfer of urethral catheterization skills from simulation training to performance on patients. BMC Med. Educ. 2013, 13, 29. [Google Scholar] [CrossRef] [Green Version]
- Melchiors, J.; Todsen, T.; Nilsson, P.; Wennervaldt, K.; Charabi, B.; Bottger, M.; Konge, L.; von Buchwald, C. Preparing for emergency: A valid, reliable assessment tool for emergency cricothyroidotomy skills. Otolaryngol. Head Neck Surg. 2015, 152, 260–265. [Google Scholar] [CrossRef]
- UHL WIPaC. Core Competencies for Infection Prevention and Control Professionals; World Health Organization: Geneva, Switzerland, 2020; p. 69. [Google Scholar]
- Jakobsen, K.K.; Jensen, J.S.; Todsen, T.; Tolsgaard, M.G.; Kirkby, N.; Lippert, F.; Vangsted, A.M.; Martel, C.J.; Klokker, M.; von Buchwald, C. Accuracy and cost description of rapid antigen test compared with reverse transcriptase-polymerase chain reaction for SARS-CoV-2 detection. Dan. Med. J. 2021, 68, A03210217. [Google Scholar] [PubMed]
- Mark, M.E.; LoSavio, P.; Husain, I.; Papagiannopoulos, P.; Batra, P.S.; Tajudeen, B.A. Effect of Implementing Simulation Education on Health Care Worker Comfort With Nasopharyngeal Swabbing for COVID-19. Otolaryngol. Head Neck Surg. 2020, 163, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Hiebert, N.M.; Chen, B.A.; Sowerby, L.J. Variability in instructions for performance of nasopharyngeal swabs across Canada in the era of COVID-19-what type of swab is actually being performed? J. Otolaryngol. Head Neck Surg. 2021, 50, 5. [Google Scholar] [CrossRef]
- Todsen, T.; Tolsgaard, M.; Folke, F.; Jakobsen, K.K.; Ersboll, A.K.; Benfield, T.; von Buchwald, C.; Kirkby, N. SARS-CoV-2 in saliva, oropharyngeal and nasopharyngeal specimens. Dan. Med. J. 2021, 68, A01210087. [Google Scholar]
- Bundgaard, J.S.; Raaschou-Pedersen, D.T.; Todsen, T.; Ringgaard, A.; Torp-Pedersen, C.; Von Buchwald, C.; Iversen, K.; Bundgaard, H. Danish citizens’ preferences for at-home oropharyngeal/nasal SARS-CoV-2 specimen collection. Int. J. Infect. Dis. 2021, 109, 195–198. [Google Scholar] [CrossRef]
- Therchilsen, J.H.; von Buchwald, C.; Koch, A.; Dam Nielsen, S.; Rasmussen, D.B.; Thudium, R.F.; Kirkby, N.S.; Raaschou-Pedersen, D.E.T.; Bundgaard, J.S.; Iversen, K.; et al. Self-Collected versus Healthcare Worker-Collected Swabs in the Diagnosis of Severe Acute Respiratory Syndrome Coronavirus 2. Diagnostics 2020, 10, 678. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Novice Group (n = 24) | Group of Trained Novices (n = 24) | Expert Group (n = 16) | Pass-Fail Score | |
|---|---|---|---|---|
| MCQ score%, mean (SD) | 66 (18) | 93 (8) | 98 (3) | 91 |
| OPS-checklist, Mean (SD) | 50 (18) | 91 (6.9) | 95 (11) | 76 |
| NPS-checklist, Mean (SD) | 36 (10) | 86 (11) | 89 (12) | 61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Todsen, T.; Bohr, A.; Hovgaard, L.H.; Eið, R.C.; Benfield, T.; Svendsen, M.B.S.; Kirkby, N.; Konge, L.; von Buchwald, C.; Melchiors, J.; et al. Valid and Reliable Assessment of Upper Respiratory Tract Specimen Collection Skills during the COVID-19 Pandemic. Diagnostics 2021, 11, 1987. https://doi.org/10.3390/diagnostics11111987
Todsen T, Bohr A, Hovgaard LH, Eið RC, Benfield T, Svendsen MBS, Kirkby N, Konge L, von Buchwald C, Melchiors J, et al. Valid and Reliable Assessment of Upper Respiratory Tract Specimen Collection Skills during the COVID-19 Pandemic. Diagnostics. 2021; 11(11):1987. https://doi.org/10.3390/diagnostics11111987
Chicago/Turabian StyleTodsen, Tobias, Anne Bohr, Lisette Hvid Hovgaard, Rebekka Consuelo Eið, Thomas Benfield, Morten B. S. Svendsen, Nikolai Kirkby, Lars Konge, Christian von Buchwald, Jacob Melchiors, and et al. 2021. "Valid and Reliable Assessment of Upper Respiratory Tract Specimen Collection Skills during the COVID-19 Pandemic" Diagnostics 11, no. 11: 1987. https://doi.org/10.3390/diagnostics11111987