
Detection Accuracy and Latency of Colorectal Lesions with Computer-Aided Detection System Based on Low-Bias Evaluation

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. DL-Based Algorithm to Assist Lesion Detection and Localization
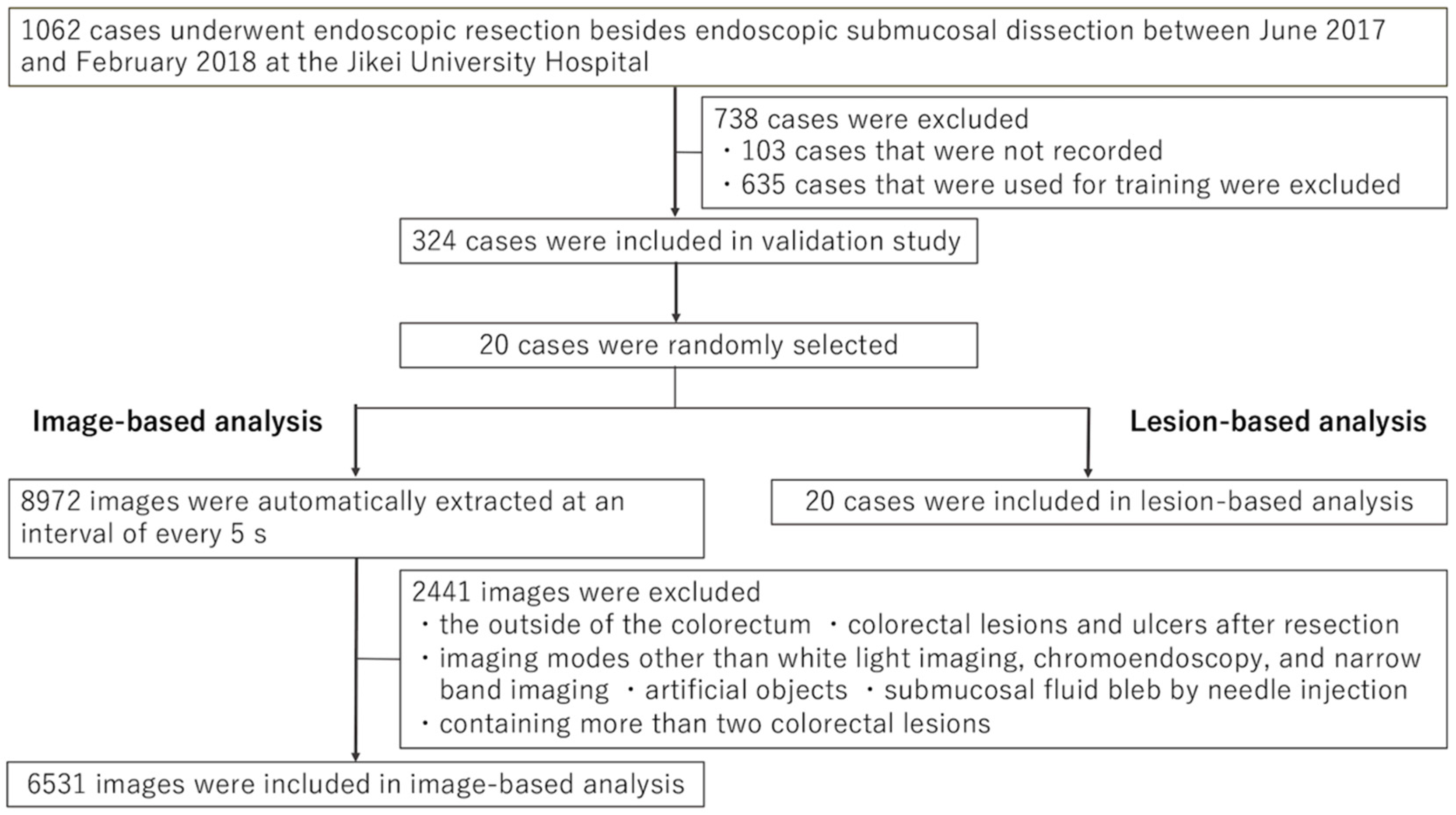
2.2. Objectives for Training and Validation
2.3. Image-Based Analysis to Calculate Diagnostic Performance Using Automatically Sampled Still Images
2.3.1. Receiver Operating Characteristic (ROC) Curve Drawing to Determine the Optimal Threshold
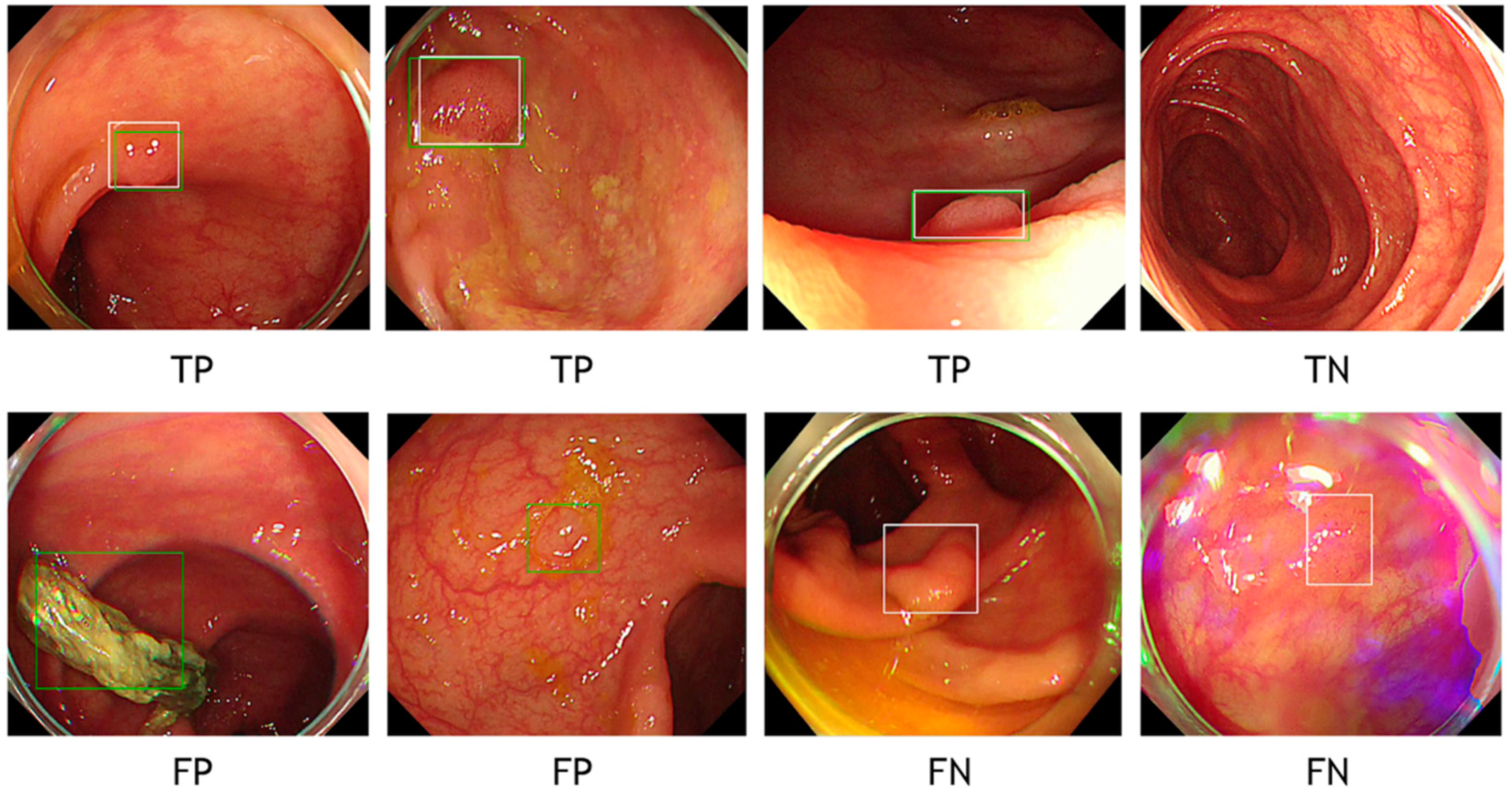
2.3.2. Definitions of True Positive, True Negative, False Positive, and False Negative
2.3.3. Localization Accuracy for Predicted Bounding Boxes Using Intersection over Union (IoU)
2.4. Lesion-Based Analysis by Reviewing Videos for Evaluating the Latency of CADe
2.5. Statistical Analysis
3. Results
3.1. Image-Based Analysis Using Automatically Sampled Still Images
3.2. Lesion-Based Analysis with Video Reviewing
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.Y.; Young, G.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef] [PubMed]
- Ladabaum, U.; Dominitz, J.A.; Kahi, C.; Schoen, R.E. Strategies for colorectal cancer screening. Gastroenterology 2020, 158, 418–432. [Google Scholar] [CrossRef]
- Kahi, C.J.; Pohl, H.; Myers, L.J.; Mobarek, D.; Robertson, D.J.; Imperiale, T.F. Colonoscopy and colorectal cancer mortality in the veterans affairs health care system: A case-control study. Ann. Intern. Med. 2018, 168, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Nishihara, R.; Wu, K.; Lochhead, P.; Morikawa, T.; Liao, X.; Qian, Z.R.; Inamura, K.; Kim, S.A.; Kuchiba, A.; Yamauchi, M.; et al. Long-term colorectal-cancer incidence and mortality after lower endoscopy. N. Engl. J. Med. 2013, 369, 1095–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zauber, A.; Winawer, S.; O’Brien, M.J.; Lansdorp-Vogelaar, I.; Van Ballegooijen, M.; Hankey, G.; Shi, W.; Bond, J.; Schapiro, J.; Panish, J.; et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N. Engl. J. Med. 2012, 366, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Chang-Claude, J.; Seiler, C.M.; Rickert, A.; Hoffmeister, M. Protection from colorectal cancer after colonoscopy: A population-based, case-control study. Ann. Intern. Med. 2011, 154, 22–30. [Google Scholar] [CrossRef]
- Robertson, D.J.; Lieberman, D.A.; Winawer, S.J.; Ahnen, D.J.; Baron, J.A.; Schatzkin, A.; Cross, A.J.; Zauber, A.G.; Church, T.R.; Lance, P.; et al. Colorectal cancers soon after colonoscopy: A pooled multicohort analysis. Gut 2014, 63, 949–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaminski, M.; Wieszczy, P.; Rupinski, M.; Wojciechowska, U.; Didkowska, J.; Kraszewska, E.; Kobiela, J.; Franczyk, R.; Rupinska, M.; Kocot, B.; et al. Increased rate of adenoma detection associates with reduced risk of colorectal cancer and death. Gastroenterology 2017, 153, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Corley, D.A.; Jensen, C.D.; Marks, A.; Zhao, W.K.; Lee, J.K.; Doubeni, C.; Zauber, A.G.; De Boer, J.; Fireman, B.H.; Schottinger, J.E.; et al. Adenoma detection rate and risk of colorectal cancer and death. N. Engl. J. Med. 2014, 370, 1298–1306. [Google Scholar] [CrossRef] [Green Version]
- Kaminski, M.; Regula, J.; Kraszewska, E.; Polkowski, M.; Wojciechowska, U.; Didkowska, J.; Zwierko, M.; Rupinski, M.; Nowacki, M.P.; Butruk, E. Quality indicators for colonoscopy and the risk of interval cancer. N. Engl. J. Med. 2010, 362, 1795–1803. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, N.S.; Ket, S.; Bassett, P.; Aponte, D.; De Aguiar, S.; Gupta, N.; Horimatsu, T.; Ikematsu, H.; Inoue, T.; Kaltenbach, T.; et al. Narrow-band imaging for detection of neoplasia at colonoscopy: A meta-analysis of data from individual patients in randomized controlled trials. Gastroenterology 2019, 157, 462–471. [Google Scholar] [CrossRef]
- Tziatzios, G.; Gkolfakis, P.; Lazaridis, L.D.; Facciorusso, A.; Antonelli, G.; Hassan, C.; Repici, A.; Sharma, P.; Rex, D.K.; Triantafyllou, K. High-definition colonoscopy for improving adenoma detection: A systematic review and meta-analysis of randomized controlled studies. Gastrointest. Endosc. 2020, 91, 1027–1036.e9. [Google Scholar] [CrossRef]
- Subramanian, V.; Mannath, J.; Hawkey, C.J.; Ragunath, K. High definition colonoscopy vs. standard video endoscopy for the detection of colonic polyps: A meta-analysis. Endoscopy 2011, 43, 499–505. [Google Scholar] [CrossRef]
- Wang, X.; Yang, W.; Weinreb, J.; Han, J.; Li, Q.; Kong, X.; Yan, Y.; Ke, Z.; Luo, B.; Liu, T.; et al. Searching for prostate cancer by fully automated magnetic resonance imaging classification: Deep learning versus non-deep learning. Sci. Rep. 2017, 7, 15415. [Google Scholar] [CrossRef] [Green Version]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef] [PubMed]
- Misawa, M.; Kudo, S.-E.; Mori, Y.; Cho, T.; Kataoka, S.; Yamauchi, A.; Ogawa, Y.; Maeda, Y.; Takeda, K.; Ichimasa, K.; et al. Artificial Intelligence-Assisted Polyp Detection for Colonoscopy: Initial Experience. Gastroenterology 2018, 154, 2027–2029.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urban, G.; Tripathi, P.; Alkayali, T.; Mittal, M.; Jalali, F.; Karnes, W.; Baldi, P. Deep Learning Localizes and Identifies Polyps in Real Time with 96% Accuracy in Screening Colonoscopy. Gastroenterology 2018, 155, 1069–1078.e8. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Xiao, X.; Brown, J.R.G.; Berzin, T.M.; Tu, M.; Xiong, F.; Hu, X.; Liu, P.; Song, Y.; Zhang, D.; et al. Development and validation of a deep-learning algorithm for the detection of polyps during colonoscopy. Nat. Biomed. Eng. 2018, 2, 741–748. [Google Scholar] [CrossRef]
- Yamada, M.; Saito, Y.; Imaoka, H.; Saiko, M.; Yamada, S.; Kondo, H.; Takamaru, H.; Sakamoto, T.; Sese, J.; Kuchiba, A.; et al. Development of a real-time endoscopic image diagnosis support system using deep learning technology in colonoscopy. Sci. Rep. 2019, 9, 14465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinsard, D.G.; Mori, Y.; Misawa, M.; Kudo, S.-E.; Rastogi, A.; Bagci, U.; Rex, D.K.; Wallace, M.B. Quality assurance of computer-aided detection and diagnosis in colonoscopy. Gastrointest. Endosc. 2019, 90, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Lui, T.K.L.; Guo, C.G.; Leung, W.K. Accuracy of artificial intelligence on histology prediction and detection of colorectal polyps: A systematic review and meta-analysis. Gastrointest. Endosc. 2020, 92, 11–22.e6. [Google Scholar] [CrossRef]
- Wang, P.; Berzin, T.M.; Brown, J.R.G.; Bharadwaj, S.; Becq, A.; Xiao, X.; Liu, P.; Li, L.; Song, Y.; Zhang, D.; et al. Real-time automatic detection system increases colonoscopic polyp and adenoma detection rates: A prospective randomised controlled study. Gut 2019, 68, 1813–1819. [Google Scholar] [CrossRef] [Green Version]
- Kamba, S.; Tamai, N.; Saitoh, I.; Matsui, H.; Horiuchi, H.; Kobayashi, M.; Sakamoto, T.; Ego, M.; Fukuda, A.; Tonouchi, A. Reducing adenoma miss rate of colonoscopy assisted by artificial intelligence: A multicenter randomized controlled trial. J. Gastroenterol. 2021, 56, 746–757. [Google Scholar] [CrossRef]
- Hassan, C.; Spadaccini, M.; Iannone, A.; Maselli, R.; Jovani, M.; Chandrasekar, V.T.; Antonelli, G.; Yu, H.; Areia, M.; Dinis-Ribeiro, M.; et al. Performance of artificial intelligence in colonoscopy for adenoma and polyp detection: A systematic review and meta-analysis. Gastrointest. Endosc. 2021, 93, 77–85.e6. [Google Scholar] [CrossRef] [PubMed]
- Ashat, M.; Klair, J.S.; Singh, D.; Murali, A.R.; Krishnamoorthi, R. Impact of real-time use of artificial intelligence in improving adenoma detection during colonoscopy: A systematic review and meta-analysis. Endosc. Int. Open. 2021, 9, E513–E521. [Google Scholar] [PubMed]
- Sumiyama, K.; Futakuchi, T.; Kamba, S.; Matsui, H.; Tamai, N. Artificial intelligence in endoscopy: Present and future perspectives. Dig. Endosc. 2021, 33, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. ImageNet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- Ioffe, S.; Szegedy, C. Batch normalization: Accelerating deep network training by reducing internal covariate shift. arXiv 2015, arXiv:1502.03167. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Maas, A.L.; Hannun, A.Y.; Ng, A.Y. Rectifier nonlinearities improve neural network acoustic models. Proc. ICML 2013, 30, 3. [Google Scholar]
- Perkins, N.J.; Schisterman, E.F. The inconsistency of “optimal” cutpoints obtained using two criteria based on the receiver operating characteristic curve. Am. J. Epidemiol. 2006, 163, 670–675. [Google Scholar] [CrossRef] [Green Version]
- Pepe, M.S. The Statistical Evaluation of Medical Tests for Classification and Prediction; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Hassan, C.; Wallace, M.B.; Sharma, P.; Maselli, R.; Craviotto, V.; Spadaccini, M.; Repici, A. New artificial intelligence system: First validation study versus experienced endoscopists for colorectal polyp detection. Gut 2020, 69, 799–800. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Imaging Mode (No. of Lesions/No. of Images (Prevalence (%)) | Youden Index | Probability Threshold | Sensitivity (95% CI)(%) | Specificity (95% CI)(%) | PPV (95% CI)(%) | NPV (95% CI)(%) | Accuracy (95% CI)(%) | IoU ≥ 0.5 (TP)(%) |
|---|---|---|---|---|---|---|---|---|
| Overall (662/6531 (10.1%)) | 0.897 | 0.27 | 94.6 (92.6–96.2) | 95.2 (94.6–95.7) | 68.8 (65.7–71.8) | 99.4 (99.1-99.6) | 95.1 (94.5–95.6) | 97.3 (609/626) |
| WLI (334/5527 (6.0%)) | 0.9 | 0.22 | 95.5 (92.7–97.5) | 94.5 (93.8–95.1) | 52.6 (48.5–56.6) | 99.7 (99.5–99.8) | 94.5 (93.9–95.1) | 96.9 (309/319) |
| 0.899 | 0.27 | 94.6 (91.6–96.8) | 95.3 (94.7–95.8) | 56.3 (52.1–60.5) | 99.6 (99.4–99.8) | 95.2 (94.6–95.8) | 97.2 (307/316) | |
| CE (182/824 (22.1%)) | 0.912 | 0.43 | 95.1 (90.8–97.7) | 96.1 (94.3–97.5) | 87.4 (81.9–91.7) | 98.6 (97.3–99.3) | 95.9 (94.3–97.1) | 97.1 (168/173) |
| 0.909 | 0.27 | 96.7 (93.0–98.8) | 94.2 (92.1–95.9) | 82.6 (76.9–87.5) | 99.0 (97.9–99.6) | 94.8 (93.0–96.2) | 97.2 (307/316) | |
| NBI (146/180 (81.1%)) | 0.956 | 0.05-0.06 | 95.9 (91.3–98.5) | 94.1 (80.3–99.3) | 98.6 (95.0–99.8) | 84.2 (68.7–94.0) | 95.6 (91.4–98.1) | 96.4 (135/140) |
| 0.859 | 0.27 | 91.8 (86.1–95.7) | 94.1 (80.3–99.3) | 98.5 (94.8–99.8) | 72.7 (57.2–85.0) | 92.2 (87.3–95.7) | 97.0 (130/134) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsui, H.; Kamba, S.; Horiuchi, H.; Takahashi, S.; Nishikawa, M.; Fukuda, A.; Tonouchi, A.; Kutsuna, N.; Shimahara, Y.; Tamai, N.; et al. Detection Accuracy and Latency of Colorectal Lesions with Computer-Aided Detection System Based on Low-Bias Evaluation. Diagnostics 2021, 11, 1922. https://doi.org/10.3390/diagnostics11101922
Matsui H, Kamba S, Horiuchi H, Takahashi S, Nishikawa M, Fukuda A, Tonouchi A, Kutsuna N, Shimahara Y, Tamai N, et al. Detection Accuracy and Latency of Colorectal Lesions with Computer-Aided Detection System Based on Low-Bias Evaluation. Diagnostics. 2021; 11(10):1922. https://doi.org/10.3390/diagnostics11101922
Chicago/Turabian StyleMatsui, Hiroaki, Shunsuke Kamba, Hideka Horiuchi, Sho Takahashi, Masako Nishikawa, Akihiro Fukuda, Aya Tonouchi, Natsumaro Kutsuna, Yuki Shimahara, Naoto Tamai, and et al. 2021. "Detection Accuracy and Latency of Colorectal Lesions with Computer-Aided Detection System Based on Low-Bias Evaluation" Diagnostics 11, no. 10: 1922. https://doi.org/10.3390/diagnostics11101922