
Pentraxin-3 Is a Strong Biomarker of Sepsis Severity Identification and Predictor of 90-Day Mortality in Intensive Care Units via Sepsis 3.0 Definitions

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics Statement
2.2. Definitions
2.3. Sampling and Clinical Data Collection
2.4. Enzyme-Linked Immunosorbent Assay (ELISA)
2.5. Statistical Analysis
3. Results
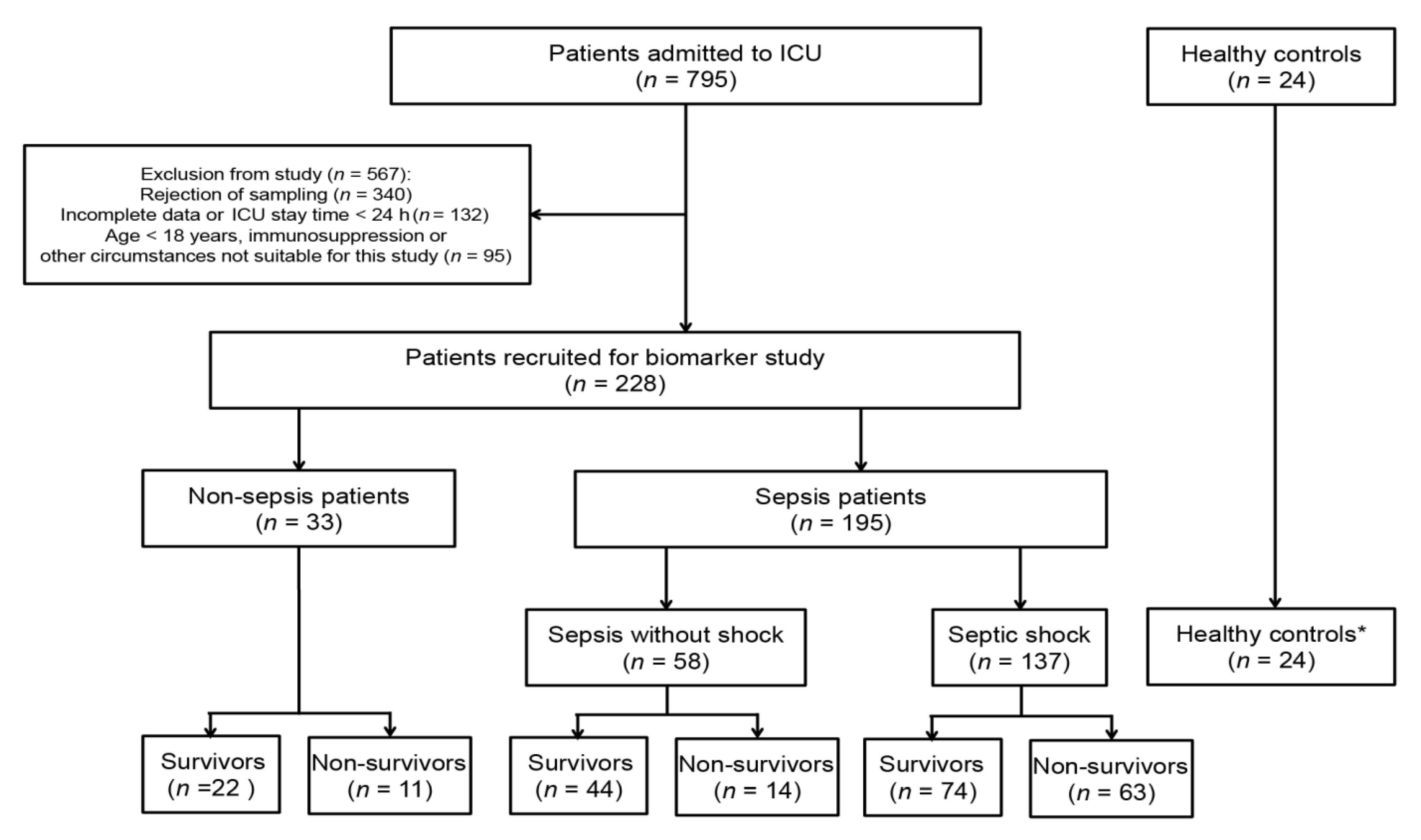
3.1. Clinical Characteristics in Sepsis, Septic Shock, and Non-Sepsis ICU Patients
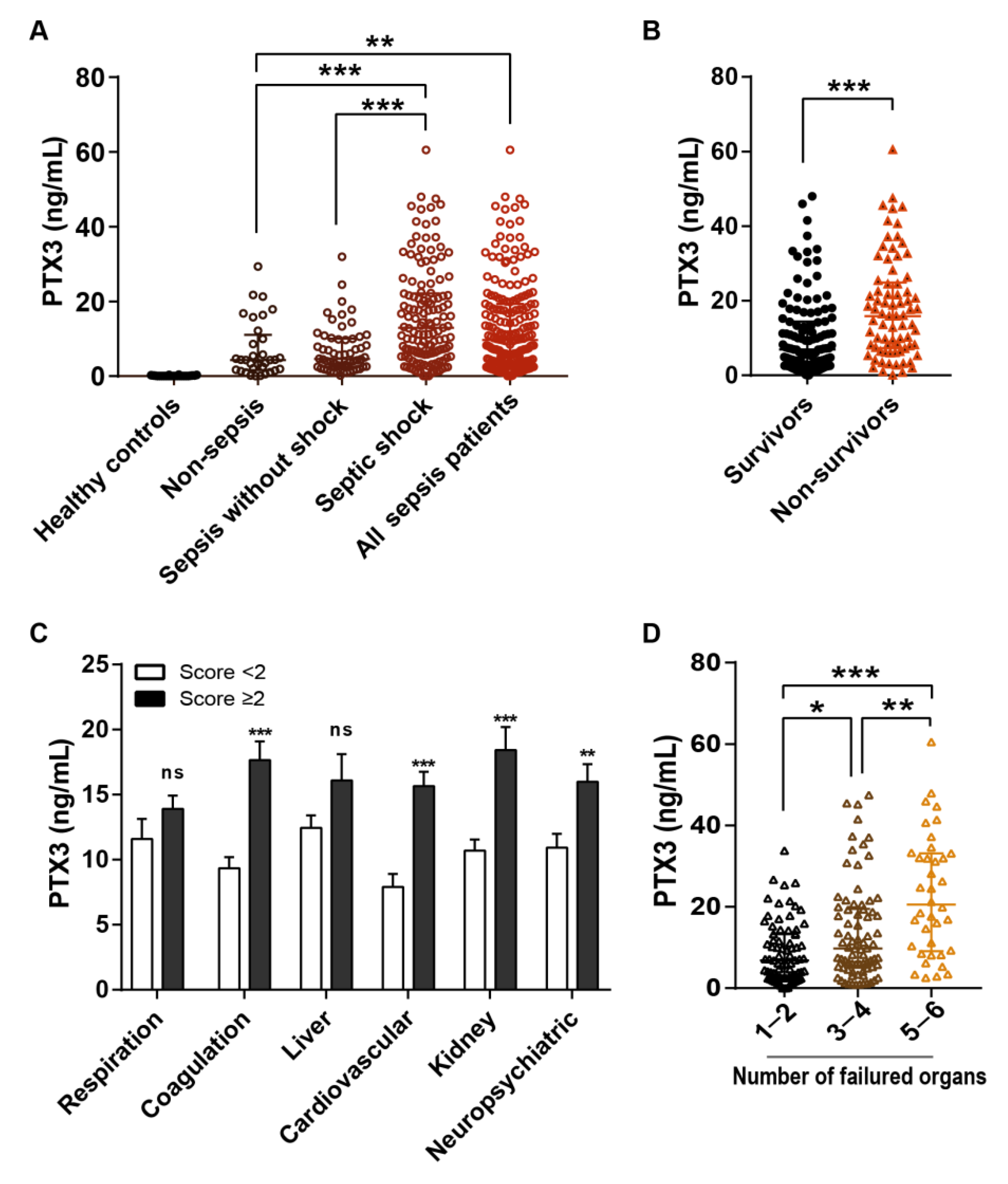
3.2. Distribution of Serum PTX3
3.3. Correlations of PTX3 with Other Disease Severity Associated Variables
3.4. Diagnostic Value of PTX3 in Discriminating Sepsis and Septic Shock according to the Sepsis 3.0 Definitions
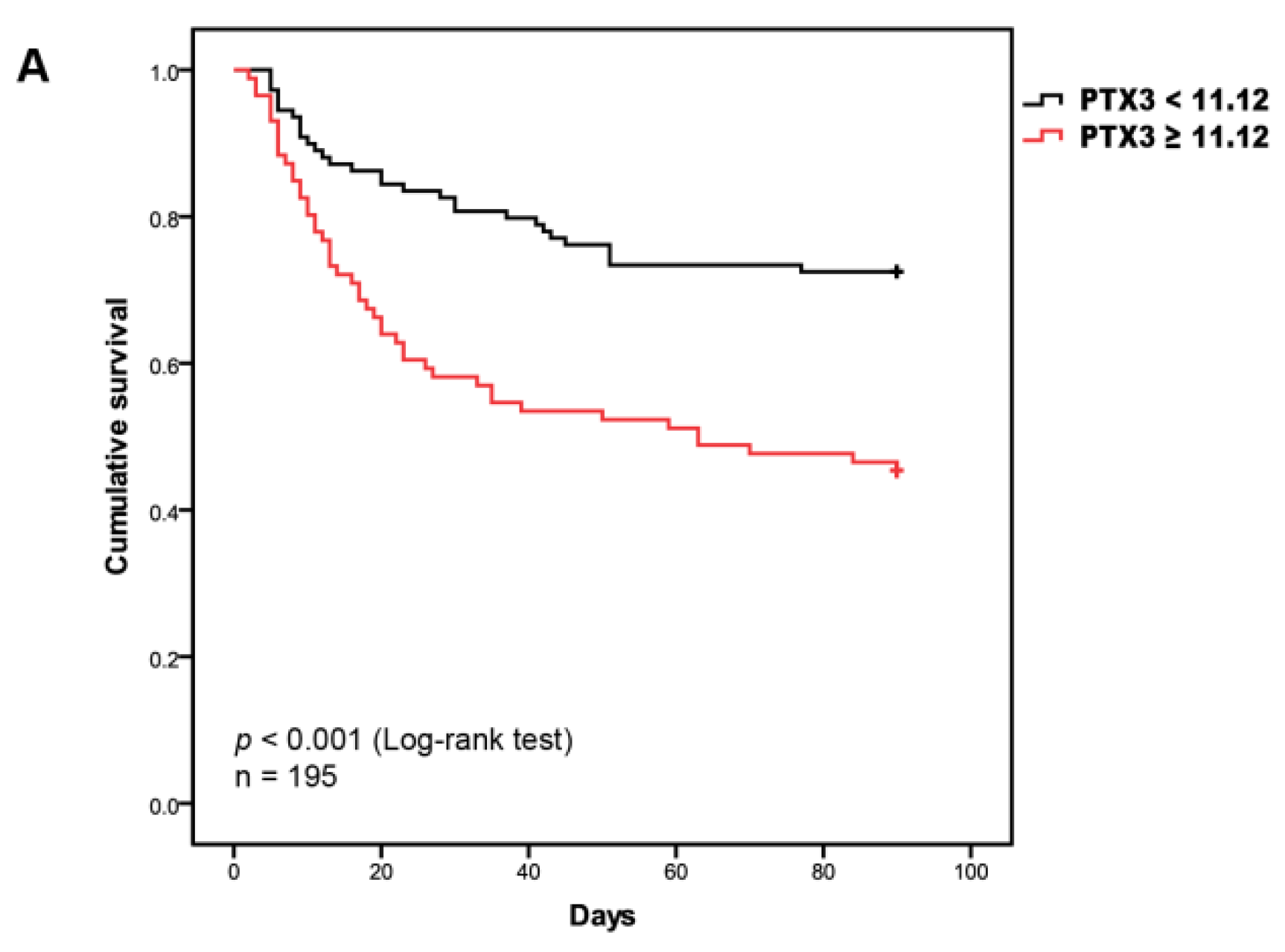
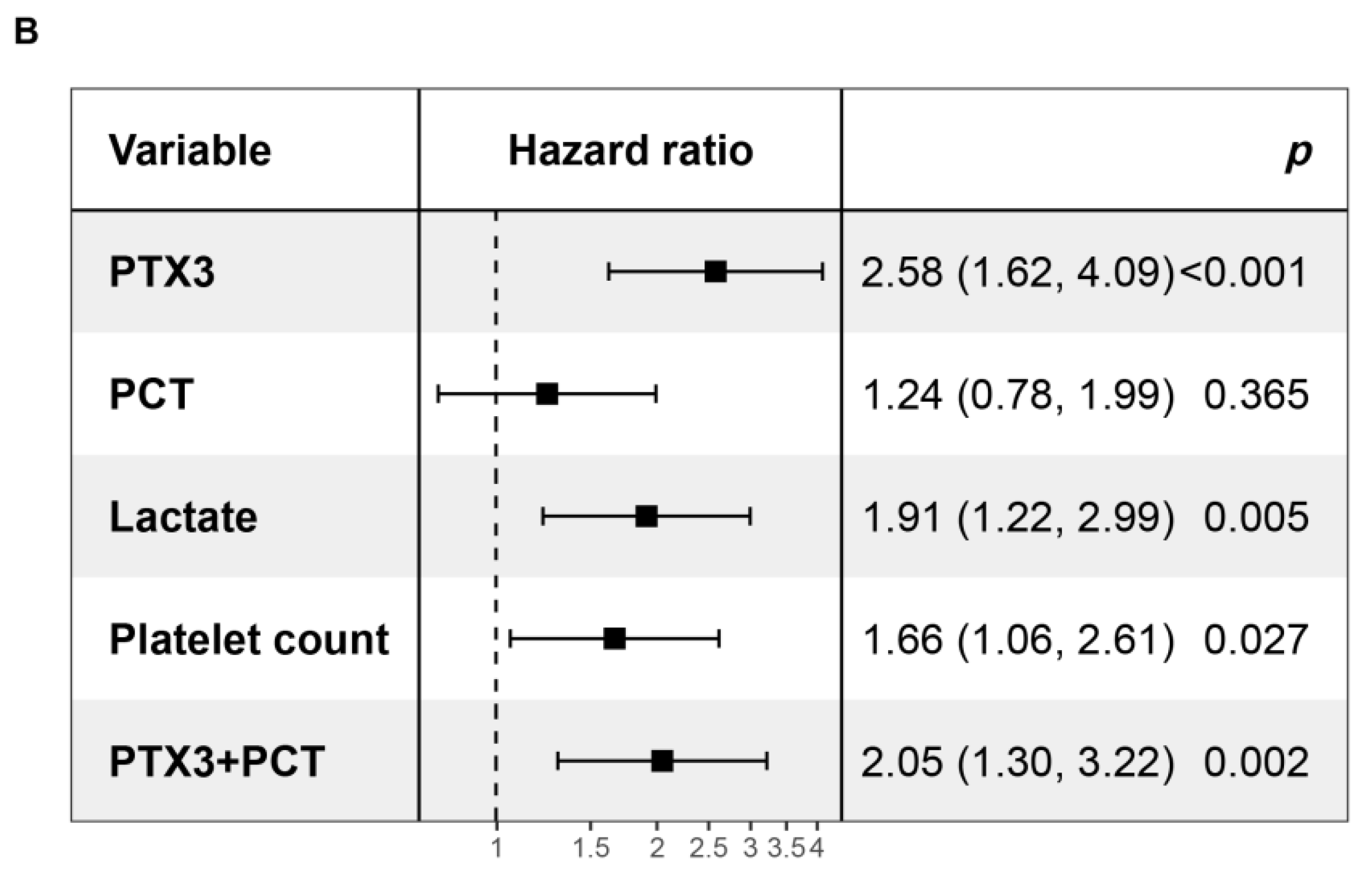
3.5. Prognostic Value of PTX3
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Singer, M.; Deutschman, C.S.; Seymour, C.C.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Weng, L.; Zeng, X.-Y.; Yin, P.; Wang, L.-J.; Wang, C.-Y.; Jiang, W.; Zhou, M.-G.; Du, B.; for the China Critical Care Clinical Trials Group (CCCCTG). Sepsis-related mortality in China: A descriptive analysis. Intensiv. Care Med. 2018, 44, 1071–1080. [Google Scholar] [CrossRef]
- Martin, G.S.; Mannino, D.; Eaton, S.; Moss, M. The Epidemiology of Sepsis in the United States from 1979 through 2000. New Engl. J. Med. 2003, 348, 1546–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longhitano, Y.; Zanza, C.; Thangathurai, D.; Taurone, S.; Kozel, D.; Racca, F.; Audo, A.; Ravera, E.; Migneco, A.; Piccioni, A.; et al. Gut Alterations in Septic Patients: A Biochemical Literature Review. Rev. Recent Clin. Trials 2021, 15, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Coopersmith, C.M.; De Backer, D.; Deutschman, C.S.; Ferrer, R.; Lat, I.; Machado, F.R.; Martin, G.S.; Martin-Loeches, I.; Nunnally, M.E.; Antonelli, M.; et al. Surviving sepsis campaign: Research priorities for sepsis and septic shock. Intensiv. Care Med. 2018, 44, 1400–1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvestre, J.; Povoa, P.; Coelho, L.; Almeida, E.; Moreira, P.; Fernandes, A.; Mealha, R.; Sabino, H. Is C-reactive protein a good prognostic marker in septic patients? Intensiv. Care Med. 2009, 35, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Goyal, K.; Tomar, G.S.; Sengar, K.; Singh, G.P.; Aggarwal, R.; Soni, K.D.; Mathur, P.; Kedia, S.; Prabhakar, H. Prognostic Value of Serially Estimated Serum Procalcitonin Levels in Traumatic Brain Injury Patients With or Without Extra Cranial Injury on Early In-hospital Mortality: A Longitudinal Observational Study. Neurocritical Care 2021, 34, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Kibe, S.; Adams, K.; Barlow, G. Diagnostic and prognostic biomarkers of sepsis in critical care. J. Antimicrob. Chemother. 2011, 66, ii33–ii40. [Google Scholar] [CrossRef] [Green Version]
- Pierrakos, C.; Velissaris, D.; Bisdorff, M.; Marshall, J.C.; Vincent, J.-L. Biomarkers of sepsis: Time for a reappraisal. Crit. Care 2020, 24, 287. [Google Scholar] [CrossRef]
- Porte, R.; Davoudian, S.; Asgari, F.; Parente, R.; Mantovani, A.; Garlanda, C.; Bottazzi, B. The Long Pentraxin PTX3 as a Humoral Innate Immunity Functional Player and Biomarker of Infections and Sepsis. Front. Immunol. 2019, 10, 794. [Google Scholar] [CrossRef] [PubMed]
- Erreni, M.; Manfredi, A.A.; Garlanda, C.; Mantovani, A.; Rovere-Querini, P. The long pentraxin PTX3: A prototypical sensor of tissue injury and a regulator of homeostasis. Immunol. Rev. 2017, 280, 112–125. [Google Scholar] [CrossRef]
- Brunetta, E.; Folci, M.; Bottazzi, B.; De Santis, M.; Gritti, G.; Protti, A.; Mapelli, S.N.; Bonovas, S.; Piovani, D.; Leone, R.; et al. Macrophage expression and prognostic significance of the long pentraxin PTX3 in COVID-19. Nat. Immunol. 2021, 22, 19–24. [Google Scholar] [CrossRef]
- Garlanda, C.; Bottazzi, B.; Magrini, E.; Inforzato, A.; Mantovani, A. PTX3, a Humoral Pattern Recognition Molecule, in Innate Immunity, Tissue Repair, and Cancer. Physiol. Rev. 2018, 98, 623–639. [Google Scholar] [CrossRef] [Green Version]
- Bottazzi, B.; Doni, A.; Garlanda, C.; Mantovani, A. An Integrated View of Humoral Innate Immunity: Pentraxins as a Paradigm. Annu. Rev. Immunol. 2010, 28, 157–183. [Google Scholar] [CrossRef]
- Jiao, J.; Gao, M.; Zhang, H.; Wang, N.; Xiao, Z.; Liu, K.; Yang, M.; Wang, K.; Xiao, X. Identification of Potential Biomarkers by Serum Proteomics Analysis in Rats with Sepsis. Shock 2014, 42, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.T.; Gong, M.; Chau, A.; Wong, W.T.; Bazoukis, G.; Wong, S.H.; Lampropoulos, K.; Xia, Y.; Li, G.; Wong, M.C.; et al. Pentraxin-3 as a marker of sepsis severity and predictor of mortality outcomes: A systematic review and meta-analysis. J. Infect. 2018, 76, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Moon, S.; Park, D.W.; Cho, H.-J.; Kim, J.Y.; Park, J.; Cha, J.H. Biomarker combination and SOFA score for the prediction of mortality in sepsis and septic shock. Medicine 2020, 99, e20495. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Park, D.W.; Moon, S.; Cho, H.-J.; Park, J.H.; Seok, H.; Choi, W.S. Diagnostic and prognostic value of interleukin-6, pentraxin 3, and procalcitonin levels among sepsis and septic shock patients: A prospective controlled study according to the Sepsis-3 definitions. BMC Infect. Dis. 2019, 19, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vassalli, F.; Masson, S.; Meessen, J.; Pasticci, I.; Bonifazi, M.; Vivona, L.; Caironi, P.; Busana, M.; Giosa, L.; Macrì, M.M.; et al. Pentraxin-3, Troponin T, N-Terminal Pro-B-Type Natriuretic Peptide in Septic Patients. Shock 2020, 54, 675–680. [Google Scholar] [CrossRef]
- Martin, S.P.-S.; Suberviola, B.; Garcia-Unzueta, M.T.; Lavin, B.A.; Campos, S.; Santibañez, M. Prognostic value of plasma pentraxin 3 levels in patients with septic shock admitted to intensive care. PLoS ONE 2020, 15, e0243849. [Google Scholar] [CrossRef]
- Tian, R.; Wang, X.; Pan, T.; Li, R.; Wang, J.; Liu, Z.; Chen, E.; Mao, E.; Tan, R.; Chen, Y.; et al. Plasma PTX3, MCP1 and Ang2 are early biomarkers to evaluate the severity of sepsis and septic shock. Scand. J. Immunol. 2019, 90, e12823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccioni, A.; Saviano, A.; Cicchinelli, S.; Valletta, F.; Santoro, M.C.; de Cunzo, T.; Zanza, C.; Longhitano, Y.; Tullo, G.; Tilli, P.; et al. Proadrenomedullin in Sepsis and Septic Shock: A Role in the Emergency Department. Medicina 2021, 57, 920. [Google Scholar] [CrossRef] [PubMed]
- Calis, J.; Van Woensel, J.; Lemson, J.; De Blasi, R.A.; Angus, D.C.; Van Der Poll, T.; Moreira, J. Severe Sepsis and Septic Shock. New Engl. J. Med. 2013, 369, 2062–2063. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Li, J.; Yan, S.; Sun, H.; Tan, C.; Liu, M.; Liu, K.; Zhang, H.; Zou, M.; Xiao, X. Identification of pathogen(s) in infectious diseases using shotgun metagenomic sequencing and conventional culture: A comparative study. PeerJ 2021, 9, e11699. [Google Scholar] [CrossRef]
- Taylor, F.; Toh, C.-H.; Hoots, K.W.; Wada, H.; Levi, M. Towards Definition, Clinical and Laboratory Criteria, and a Scoring System for Disseminated Intravascular Coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef] [Green Version]
- Rhee, C.; Jones, T.M.; Hamad, Y.; Pande, A.; Varon, J.; O’Brien, C.; Anderson, D.J.; Warren, D.K.; Dantes, R.B.; Epstein, L.; et al. Prevalence, Underlying Causes, and Preventability of Sepsis-Associated Mortality in US Acute Care Hospitals. JAMA Netw. Open 2019, 2, e187571. [Google Scholar] [CrossRef] [Green Version]
- Hansen, C.B.; Olmos, R.B.; Kristensen, M.K.; Pilely, K.; Hellemann, D.; Garred, P. Complement related pattern recognition molecules as markers of short-term mortality in intensive care patients. J. Infect. 2020, 80, 378–387. [Google Scholar] [CrossRef]
- Wong, H.R.; Cvijanovich, N.Z.; Hall, M.; Allen, G.L.; Thomas, N.J.; Freishtat, R.J.; Anas, N.; Meyer, K.; Checchia, P.A.; Lin, R.; et al. Interleukin-27 is a novel candidate diagnostic biomarker for bacterial infection in critically ill children. Crit. Care 2012, 16, R213. [Google Scholar] [CrossRef] [Green Version]
- Lundberg, O.H.M.; Lengquist, M.; Spångfors, M.; Annborn, M.; Bergmann, D.; Schulte, J.; Levin, H.; Melander, O.; Frigyesi, A.; Friberg, H. Circulating bioactive adrenomedullin as a marker of sepsis, septic shock and critical illness. Crit. Care 2020, 24, 1–10. [Google Scholar] [CrossRef]
- Mauri, T.; Bellani, G.; Patroniti, N.; Coppadoro, A.; Peri, G.; Cuccovillo, I.; Cugno, M.; Iapichino, G.; Gattinoni, L.; Pesenti, A.; et al. Persisting high levels of plasma pentraxin 3 over the first days after severe sepsis and septic shock onset are associated with mortality. Intensiv. Care Med. 2010, 36, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Caironi, P.; Masson, S.; Mauri, T.; Bottazzi, B.; Leone, R.; Magnoli, M.; Barlera, S.; Mamprin, F.; Fedele, A.; Mantovani, A.; et al. Pentraxin 3 in patients with severe sepsis or shock: The ALBIOS trial. Eur. J. Clin. Investig. 2017, 47, 73–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mjelva, Ø.R.; Pönitz, V.; Brügger-Andersen, T.; Grundt, H.; Staines, H.; Nilsen, D.W. Long-term prognostic utility of pentraxin 3 and D-dimer as compared to high-sensitivity C-reactive protein and B-type natriuretic peptide in suspected acute coronary syndrome. Eur. J. Prev. Cardiol. 2016, 23, 1130–1140. [Google Scholar] [CrossRef] [PubMed]
- Sjöberg, B.; Qureshi, A.R.; Heimbürger, O.; Stenvinkel, P.; Lind, L.; Larsson, A.; Bárány, P.; Ärnlöv, J. Association between levels of pentraxin 3 and incidence of chronic kidney disease in the elderly. J. Intern. Med. 2016, 279, 173–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ristagno, G.; Varpula, T.; Masson, S.; Greco, M.; Bottazzi, B.; Milani, V.; Aleksova, A.; Sinagra, G.; Assandri, R.; Tiainen, M.; et al. Elevations of inflammatory markers PTX3 and sST2 after resuscitation from cardiac arrest are associated with multiple organ dysfunction syndrome and early death. Clin. Chem. Lab. Med. 2015, 53, 1847–1857. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, G.A.; Rovere-Querini, P.; Blasi, M.; Sartorelli, S.; Di Chio, M.C.; Baldini, M.; De Lorenzo, R.; Bozzolo, E.P.; Leone, R.; Mantovani, A.; et al. PTX3 Intercepts Vascular Inflammation in Systemic Immune-Mediated Diseases. Front. Immunol. 2019, 10, 1135. [Google Scholar] [CrossRef]
- Dell’Oglio, M.P.; Simone, S.; Ciccone, M.; Corciulo, R.; Gesualdo, M.; Zito, A.; Cortese, F.; Castellano, G.; Gigante, M.; Gesualdo, L.; et al. Neutrophil-dependent pentraxin-3 and reactive oxygen species production modulate endothelial dysfunction in haemodialysis patients. Nephrol. Dial. Transplant. 2016, 32, gfw363–gfw1549. [Google Scholar] [CrossRef]
- Sprong, T.; Peri, G.; Neeleman, C.; Mantovani, A.; Signorini, S.; van der Meer, J.W.; van Deuren, M. Pentraxin 3 and C-reactive protein in severe meningococcal disease. Shock 2009, 31, 28–32. [Google Scholar] [CrossRef]
- Uusitalo-Seppälä, R.; Huttunen, R.; Aittoniemi, J.; Koskinen, P.; Leino, A.; Vahlberg, T.; Rintala, E. Pentraxin 3 (PTX3) Is Associated with Severe Sepsis and Fatal Disease in Emergency Room Patients with Suspected Infection: A Prospective Cohort Study. PLoS ONE 2013, 8, e53661. [Google Scholar] [CrossRef] [Green Version]
- Bastrup-Birk, S.; Munthe-Fog, L.; Skjoedt, M.-O.; Ma, Y.J.; Nielsen, H.; Køber, L.; Nielsen, O.W.; Iversen, K.; Garred, P. Pentraxin-3 level at admission is a strong predictor of short-term mortality in a community-based hospital setting. J. Intern. Med. 2014, 277, 562–572. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Non-Sepsis Patients (n = 33) | Sepsis Patients | p Value (Non-Sepsis vs. Total Sepsis) | Healthy Controls (n = 24) | ||
|---|---|---|---|---|---|---|
| Total Sepsis Patients (n = 195) | Sepsis without Shock Patients (n = 58) | Septic Shock Patients (n = 137) | ||||
| Age (y), M (IQR) | 52 (36–72) | 60 (47–70) | 58 (47–70) | 62 (48–70) | 0.262 | 47 (40–50) |
| Male sex, n (%) | 16 (49) | 120 (62) | 35 (60) | 85 (62) | 0.157 | 14 (58) |
| Numbers of infection site, M (IQR) | 1 (0–1) | 2 (1–2) &&& | 2 (1–2) *** | 2 (1–2) *** # | <0.001 | — |
| Infection Site | ||||||
| Pulmonary, n (%) | 21 (64) | 140 (72) | 43 (74) | 97 (71) | 0.341 | — |
| Urinary, n (%) | 1 (3) | 41 (21) & | 11 (19) * | 30 (22) * | 0.013 | — |
| Intra-abdominal, n (%) | 4 (12) | 83 (43) && | 25 (43) ** | 58 (42) ** | 0.001 | — |
| Blood-borne, n (%) | 0 (0) | 54 (28) &&& | 8(14) *** | 46 (34) *** | <0.001 | — |
| Skin and soft tissue, n (%) | 3 (9) | 24 (12) | 6 (10) | 18 (13) | 0.775 | — |
| Underlying Diseases | ||||||
| Perioperative period, n (%) | 13 (39) | 107 (55) | 33 (57) | 74 (54) | 0.100 | — |
| Hypertension, n (%) | 11 (33) | 65 (33) | 20 (35) | 45 (33) | 1.000 | — |
| Diabetes, n (%) | 3 (9) | 43 (22) | 14 (24) | 29 (21) | 0.103 | — |
| Chronic lung disease, n (%) | 4 (12) | 21 (11) | 7 (12) | 14 (10) | 0.767 | — |
| Chronic liver disease, n (%) | 6 (18) | 9 (5) && | 2 (4) * | 7 (5) * | 0.004 | — |
| Chronic kidney disease, n (%) | 6 (18) | 24 (12) | 7 (12) | 17 (12) | 0.356 | — |
| Dyslipidemia, n (%) | 3 (9) | 42 (22) | 14 (24) | 28 (20) | 0.153 | — |
| Neoplasm, n (%) | 4 (12) | 34 (17) | 10 (17) | 24 (18) | 0.615 | — |
| Infection and Inflammation-Associated Laboratory Markers | ||||||
| PCT(ng/mL), M (IQR) | 0.94 (0.50–3.71) | 12.38 (2.64–43.84) &&& | 3.65 (1.08–15.48) | 16.00 (4.75–62.39) *** ### | <0.001 | — |
| CRP(mg/L), M (IQR) | 132.9 (32.8–188.2) | 168.3 (71.5–200.0) | 89.3 (37.9–200.0) | 170.8 (83.2–200.0) | 0.099 | — |
| Lactate(mmol/L), M (IQR) | 1.8 (1.1–3.1) | 3.0 (2.1–5.1) &&& | 2.3 (1.4–3.1) | 3.6 (2.4–6.4) *** ### | <0.001 | — |
| Bilirubin(μmol/L), M (IQR) | 13.9 (6.1–21.3) | 19.1 (9.6–34.9) && | 16.7 (7.3–24.23) | 20.7 (9.8–42.8) ** | 0.009 | — |
| Creatinine(μmol/L), M (IQR) | 75 (64–224) | 123 (75–255) | 91 (63–181) | 137 (88–265) # | 0.075 | — |
| WBC count (109/L), M (IQR) | 12.15 (9.13–14.01) | 11.43 (7.78–17.95) | 11.11 (7.41–15.02) | 12.40 (7.81–18.25) | 0.709 | — |
| Platelet count (1012/L), M (IQR) | 169 (118–205) | 107 (62–183) && | 136 (91–202) | 93 (41–173) ** # | 0.004 | — |
| D-dimer(mg/L), M (IQR) | 3.82 (1.84–8.11) | 6.45 (3.64–11.43) && | 5.78 (2.72–9.94) | 6.97 (3.87–12.23) ** | 0.007 | — |
| MAP, M (IQR) | 95 (80–108) | 78 (67–92) &&& | 91 (80–106) | 75 (65–85) | <0.001 | — |
| DIC score, M (IQR) | 2 (0–3) | 3 (2–5) && | 2 (1–4) | 4 (2–5) *** ## | 0.003 | — |
| APACHE II score, M (IQR) | 14 (9–20) | 19 (13–24) && | 16 (12–20) | 20 (15–25) ** # | 0.008 | — |
| SOFA score, M(IQR) | 4 (3–7) | 10 (6–13) && | 6 (5–9) | 11 (8–14) *** ### | <0.001 | — |
| Mechanical ventilation, n (%) | 22 (66.7) | 158 (81) | 42 (72.4) | 116 (84.7) # | 0.061 | — |
| ICU stay (h), M (IQR) | 96 (62–189) | 142 (87–281) & | 182 (93–253) * | 139 (85–284) | 0.040 | — |
| 90-day mortality, n (%) | 11 (33) | 77 (40) | 14 (24) | 63 (46) * # | 0.502 | — |
| Variable | Severity | AUC (95% CI) | Cut-Off Value | Sensitivity | Specificity | p Value | True Positive Rate * | True Negative Rate * |
|---|---|---|---|---|---|---|---|---|
| Univariate analysis | ||||||||
| PTX3 | Sepsis | 0.68 (0.58–0.78) | 5.84 | 0.667 | 0.697 | 0.001 | 0.467 | 0.758 |
| (ng/mL) | Septic shock | 0.73 (0.66–0.80) | 11.12 | 0.555 | 0.828 | <0.001 | 0.526 | 0.828 |
| PCT | Sepsis | 0.79 (0.70–0.88) | 1.62 | 0.815 | 0.697 | <0.001 | 0.344 | 0.879 |
| (ng/mL) | Septic shock | 0.73 (0.65–0.80) | 7.27 | 0.328 | 0.672 | <0.001 | 0.409 | 0.879 |
| Lactate | Sepsis | 0.70 (0.60–0.80) | 2.3 | 0.723 | 0.621 | <0.001 | 0.405 | 0.848 |
| (mmol/L) | Septic shock | 0.73 (0.66–0.81) | 3.9 | 0.453 | 0.914 | <0.001 | 0.423 | 0.914 |
| Platelet count | Sepsis | 0.66 (0.57–0.74) | 132 | 0.585 | 0.727 | 0.004 | 0.677 | 0.545 |
| (×1012/L) | Septic shock | 0.63 (0.55–0.71) | 87 | 0.460 | 0.828 | 0.004 | 0.664 | 0.431 |
| Multivariate analysis | ||||||||
| PTX3 + PCT | Sepsis | 0.74 (0.65–0.82) | 85.5 | 0.621 | 0.818 | <0.001 | 0.682 | 0.667 |
| (score) | Septic shock | 0.77 (0.70–0.84) | 74.8 | 0.569 | 0.897 | <0.001 | 0.693 | 0.724 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.; Li, T.; Yan, S.; Liu, M.; Liu, K.; Zhang, H.; Gao, M.; Xiao, X. Pentraxin-3 Is a Strong Biomarker of Sepsis Severity Identification and Predictor of 90-Day Mortality in Intensive Care Units via Sepsis 3.0 Definitions. Diagnostics 2021, 11, 1906. https://doi.org/10.3390/diagnostics11101906
Chen H, Li T, Yan S, Liu M, Liu K, Zhang H, Gao M, Xiao X. Pentraxin-3 Is a Strong Biomarker of Sepsis Severity Identification and Predictor of 90-Day Mortality in Intensive Care Units via Sepsis 3.0 Definitions. Diagnostics. 2021; 11(10):1906. https://doi.org/10.3390/diagnostics11101906
Chicago/Turabian StyleChen, Huan, Tao Li, Shanshan Yan, Meidong Liu, Ke Liu, Huali Zhang, Min Gao, and Xianzhong Xiao. 2021. "Pentraxin-3 Is a Strong Biomarker of Sepsis Severity Identification and Predictor of 90-Day Mortality in Intensive Care Units via Sepsis 3.0 Definitions" Diagnostics 11, no. 10: 1906. https://doi.org/10.3390/diagnostics11101906