Coronary Microvascular Dysfunction and the Role of Noninvasive Cardiovascular Imaging


Abstract
:1. Introduction
2. Overview of the Coronary Microvascular Circulation
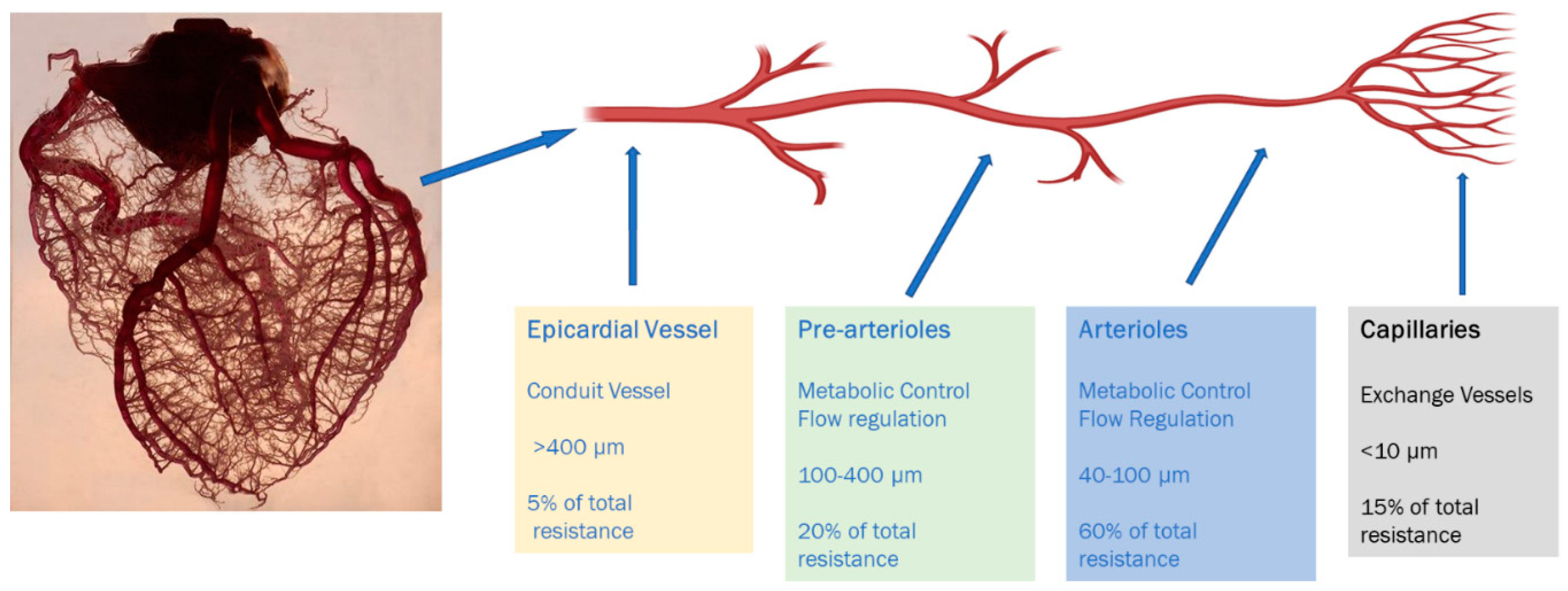
2.1. Anatomic and Physiological Considerations
2.2. Pathogenesis
3. Prognosis and Outcomes
4. Clinical Variants of CMD
- A.
- Primary CMD:
- B.
- Secondary CMD:This is further classified in to two categories.
- (i)
- CMD in the presence of obstructive CAD. Microvascular dysfunction can concomitantly exist with stable and unstable CAD.
- (ii)
- CMD in the presence of myocardial disease. Microvascular dysfunction can occur secondary to arterial remodeling, intimal hypertrophy along with interstitial and perivascular fibrosis resulting from various cardiomyopathies.
- C.
- Iatrogenic CMD:
5. Assessment of Microvascular Blood Flow
6. Review of Non-Invasive Modalities for CMD Assessment
6.1. Echocardiography
6.2. Computerized Tomographic (CT) Angiography
6.3. Single-Photon Emission Computed Tomography
6.4. Positron Emission Tomography (PET)
6.5. Cardiac MRI
7. Treatment
8. Conclusions
Funding
Conflicts of Interest
References
- Shaw, L.J.; Shaw, R.E.; Merz, N.B.; Brindis, R.G.; Klein, L.W.; Nallamothu, B.; Douglas, P.S.; Krone, R.J.; McKay, C.R.; Block, P.C.; et al. Impact of Ethnicity and Gender Differences on Angiographic Coronary Artery Disease Prevalence and In-Hospital Mortality in the American College of Cardiology–National Cardiovascular Data Registry. Circulation 2008, 117, 1787–1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claudio, C.P.; Quesada, O.; Pepine, C.J.; Merz, N.B. Why names matter for women: MINOCA/INOCA (myocardial infarction/ischemia and no obstructive coronary artery disease). Clin. Cardiol. 2018, 41, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Kutty, S.; Moukagna, K.S.B.; Craft, M.; Shostrom, V.; Xie, F.; Porter, T.R. Clinical Outcome of Patients with Inducible Capillary Blood Flow Abnormalities during Demand Stress in the Presence or Absence of Angiographic Coronary Disease. Circ. Cardiovasc. Imaging 2018, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jespersen, L.; Hvelplund, A.; Abildstrøm, S.Z.; Pedersen, F.; Galatius, S.; Madsen, J.K.; Jørgensen, E.; Kelbaek, H.; Prescott, E.; Kelbæk, H. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur. Heart J. 2011, 33, 734–744. [Google Scholar] [CrossRef] [PubMed]
- Camici, P.G.; Crea, F. Microvascular angina: A women’s affair? Circ. Cardiovasc. Imaging 2015, 8, 8–11. [Google Scholar] [CrossRef] [Green Version]
- Feher, A.; Sinusas, A.J. Quantitative Assessment of Coronary Microvascular Function. Circ. Cardiovasc. Imaging 2017, 10, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Sucato, V.; Novo, G.; Saladino, A.; Evola, S.; Galassi, A.R. Coronary microvascular dysfunction. Minerva Cardioangiol. 2020, 68, 153–163. [Google Scholar] [CrossRef]
- Pries, A.R.; Reglin, B. Coronary microcirculatory pathophysiology: Can we afford it to remain a black box? Eur. Heart J. 2017, 38, 478–488. [Google Scholar] [CrossRef] [Green Version]
- Ishimori, M.L.; Martin, R.; Berman, D.S.; Goykhman, P.; Shaw, L.J.; Shufelt, C.L.; Slomka, P.J.; Thomson, L.E.; Schapira, J.; Yang, Y.; et al. Myocardial Ischemia in the Absence of Obstructive Coronary Artery Disease in Systemic Lupus Erythematosus. JACC Cardiovasc. Imaging 2011, 4, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Taqueti, V.R.; Ridker, P.M. Inflammation, coronary flow reserve, and microvascular dysfunction: Moving beyond cardiac syndrome X. JACC Cardiovasc. Imaging 2013, 6, 668–671. [Google Scholar] [CrossRef] [Green Version]
- Petersen, J.W.; Pepine, C.J. Microvascular coronary dysfunction and ischemic heart disease: Where are we in 2014? Trends Cardiovasc. Med. 2014, 25, 98–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camici, P.G.; D’Amati, G.; Rimoldi, O. Coronary microvascular dysfunction: Mechanisms and functional assessment. Nat. Rev. Cardiol. 2014, 12, 48–62. [Google Scholar] [CrossRef] [PubMed]
- Recio-Mayoral, A.; Mason, J.C.; Kaski, J.C.; Rubens, M.B.; Harari, O.A.; Camici, P.G. Chronic inflammation and coronary microvascular dysfunction in patients without risk factors for coronary artery disease. Eur. Heart J. 2009, 30, 1837–1843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennell, D.J.; Keenan, N. Coronary Microvascular Dysfunction in Systemic Lupus Erythematosus Identified by CMR Imaging. JACC Cardiovasc. Imaging 2011, 4, 34–36. [Google Scholar] [CrossRef] [Green Version]
- Taqueti, V.R.; Di Carli, M.F. Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic Options. J. Am. Coll. Cardiol. 2018, 72, 2625–2641. [Google Scholar] [CrossRef] [PubMed]
- Elgendy, I.Y.; Pepine, C.J. Heart Failure With Preserved Ejection Fraction: Is Ischemia Due to Coronary Microvascular Dysfunction a Mechanistic Factor? Am. J. Med. 2019, 132, 692–697. [Google Scholar] [CrossRef]
- Galiuto, L.; De Caterina, A.R.; Porfidia, A.; Paraggio, L.; Barchetta, S.; Locorotondo, G.; Rebuzzi, A.G.; Crea, F. Reversible coronary microvascular dysfunction: A common pathogenetic mechanism in Apical Ballooning or Tako-Tsubo Syndrome. Eur. Heart J. 2010, 31, 1319–1327. [Google Scholar] [CrossRef] [Green Version]
- Bajaj, N.S.; Osborne, M.T.; Gupta, A.; Tavakkoli, A.; Bravo, P.E.; Vita, T.; Bibbo, C.F.; Hainer, J.; Dorbala, S.; Blankstein, R.; et al. Coronary Microvascular Dysfunction and Cardiovascular Risk in Obese Patients. J. Am. Coll. Cardiol. 2018, 72, 707–717. [Google Scholar] [CrossRef]
- Taqueti, V.R.; Shaw, L.J.; Cook, N.R.; Murthy, V.L.; Shah, N.R.; Foster, C.R.; Hainer, J.; Blankstein, R.; Dorbala, S.; Di Carli, M.F. Excess Cardiovascular Risk in Women Relative to Men Referred for Coronary Angiography Is Associated With Severely Impaired Coronary Flow Reserve, Not Obstructive Disease. Circulation 2017, 135, 566–577. [Google Scholar] [CrossRef] [Green Version]
- Schindler, T.H. Coronary Microvascular Dysfunction. J. Am. Coll. Cardiol. 2018, 72, 718–720. [Google Scholar] [CrossRef]
- Maddox, T.M.; Stanislawski, M.A.; Grunwald, G.K.; Bradley, S.M.; Ho, P.M.; Tsai, T.T.; Patel, M.R.; Sandhu, A.; Valle, J.; Magid, D.J.; et al. Nonobstructive coronary artery disease and risk of myocardial infarction. JAMA 2014, 312, 1754–1763. [Google Scholar] [CrossRef]
- Murthy, V.L.; Naya, M.; Taqueti, V.R.; Foster, C.R.; Gaber, M.; Hainer, J.; Dorbala, S.; Blankstein, R.; Rimoldi, O.; Camici, P.G.; et al. Effects of Sex on Coronary Microvascular Dysfunction and Cardiac Outcomes. Circulation 2014, 129, 2518–2527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermeltfoort, I.A.C.; Teule, G.J.J.; Van Dijk, A.B.; Muntinga, H.J.; Raijmakers, P.G.H.M. Long-term prognosis of patients with cardiac syndrome X: A review. Neth. Heart J. 2012, 20, 365–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, T.J.; Ong, P.; Sechtem, U.; Beltrame, J.; Camici, P.G.; Crea, F.; Kaski, J.-C.; Bairey Merz, C.N.; Pepine, C.J.; Shimokawa, H.; et al. Assessment of Vascular Dysfunction in Patients Without Obstructive Coronary Artery Disease: Why, How, and When. JACC Cardiovasc. Interv. 2020, 13, 1847–1864. [Google Scholar] [CrossRef] [PubMed]
- A Kaufmann, P.; Camici, P.G. Myocardial blood flow measurement by PET: Technical aspects and clinical applications. J. Nucl. Med. 2005, 46, 75–88. [Google Scholar]
- Sinha, A.; Rahman, H.; Perera, D. Ischaemia without obstructive coronary artery disease. Curr. Opin. Cardiol. 2020. [Google Scholar] [CrossRef]
- Marinescu, M.A.; Loffler, A.I.; Ouellette, M.; Smith, L.; Kramer, C.M.; Bourque, J.M. Coronary microvascular dysfunction, microvascular angina, and treatment strategies. JACC Cardiovasc. Imaging 2015, 8, 210–220. [Google Scholar] [CrossRef] [Green Version]
- Shome, J.S.; Perera, D.; Plein, S.; Chiribiri, A. Current perspectives in coronary microvascular dysfunction. Microcirculation 2017, 24, e12340. [Google Scholar] [CrossRef]
- Mathew, R.C.; Bourque, J.M.; Salerno, M.; Kramer, C.M. Cardiovascular Imaging Techniques to Assess Microvascular Dysfunction. JACC Cardiovasc. Imaging 2019. [Google Scholar] [CrossRef]
- De Bruyne, B.; Pijls, N.H.; Kalesan, B.; Barbato, E.; Tonino, P.A.; Piroth, Z.; Jagic, N.; Möbius-Winkler, S.; Rioufol, G.; Witt, N.; et al. Fractional Flow Reserve–Guided PCI versus Medical Therapy in Stable Coronary Disease. N. Engl. J. Med. 2012, 367, 991–1001. [Google Scholar] [CrossRef] [Green Version]
- Michelsen, M.M.; Mygind, N.D.; Pena, A.; Olsen, R.H.; Christensen, T.E.; Ghotbi, A.A.; Hasbak, P.; Kjaer, A.; Gustafsson, I.; Hansen, T.; et al. Transthoracic Doppler echocardiography compared with positron emission tomography for assessment of coronary microvascular dysfunction: The iPOWER study. Int. J. Cardiol. 2017, 228, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Vogel, R.; Indermühle, A.; Reinhardt, J.; Meier, P.; Siegrist, P.T.; Namdar, M.; Kaufmann, P.A.; Seiler, C. The quantification of absolute myocardial perfusion in humans by contrast echocardiography. J. Am. Coll. Cardiol. 2005, 45, 754–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, K.; Jayaweera, A.R.; Firoozan, S.; Linka, A.; Skyba, D.M.; Kaul, S. Quantification of myocardial blood flow with ultrasound-induced destruction of microbubbles administered as a constant venous infusion. Circulation 1998, 97, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Porter, T.R.; Xie, F.; Kricsfeld, D.; Armbruster, R.W. Improved myocardial contrast with second harmonic transient ultrasound response imaging in humans using intravenous perfluorocarbon-exposed sonicated dextrose albumin. J. Am. Coll. Cardiol. 1996, 27, 1497–1501. [Google Scholar] [CrossRef] [Green Version]
- Caiati, C.; Montaldo, C.; Zedda, N.; Montisci, R.; Ruscazio, M.; Lai, G.; Cadeddu, M.; Meloni, L.; Iliceto, S. Validation of a new noninvasive method (contrast-enhanced transthoracic second harmonic echo Doppler) for the evaluation of coronary flow reserve. J. Am. Coll. Cardiol. 1999, 34, 1193–1200. [Google Scholar] [CrossRef]
- Saraste, M.; Koskenvuo, J.W.; Knuuti, J.; Toikka, J.O.; Laine, H.; Niemi, P.; Sakuma, H.; Hartiala, J.J. Coronary flow reserve: Measurement with transthoracic Doppler echocardiography is reproducible and comparable with positron emission tomography. Clin. Physiol. 2001, 21, 114–122. [Google Scholar] [CrossRef]
- Galiuto, L.; Sestito, A.; Barchetta, S.; Sgueglia, G.A.; Infusino, F.; La Rosa, C.; Lanza, G.; Crea, F. Noninvasive Evaluation of Flow Reserve in the Left Anterior Descending Coronary Artery in Patients With Cardiac Syndrome X. Am. J. Cardiol. 2007, 99, 1378–1383. [Google Scholar] [CrossRef]
- Hozumi, T.; Yoshida, K.; Akasaka, T.; Asami, Y.; Ogata, Y.; Takagi, T.; Kaji, S.; Kawamoto, T.; Ueda, Y.; Morioka, S. Noninvasive assessment of coronary flow velocity and coronary flow velocity reserve in the left anterior descending coronary artery by Doppler echocardiography. J. Am. Coll. Cardiol. 1998, 32, 1251–1259. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.J.; Lam, C.S.P.; Svedlund, S.; Saraste, A.; Hage, C.; Tan, R.-S.; Beussink-Nelson, L.; Ljung-Faxen, U.; Fermer, M.L.; Broberg, M.A.; et al. Prevalence and correlates of coronary microvascular dysfunction in heart failure with preserved ejection fraction: PROMIS-HFpEF. Eur. Heart J. 2018, 39, 3439–3450. [Google Scholar] [CrossRef]
- Hage, C.; Svedlund, S.; Saraste, A.; Faxén, U.L.; Benson, L.; Fermer, M.L.; Gan, L.-M.; Shah, S.J.; Lam, C.S.; Lund, L.H. Association of Coronary Microvascular Dysfunction with Heart Failure Hospitalizations and Mortality in Heart Failure with Preserved Ejection Fraction—A follow-up in the PROMIS-HFpEF study. J. Card. Fail. 2020. [Google Scholar] [CrossRef]
- Yu, L.; Tao, X.; Dai, X.; Liu, T.; Zhang, J. Dynamic CT Myocardial Perfusion Imaging in Patients without Obstructive Coronary Artery Disease: Quantification of Myocardial Blood Flow according to Varied Heart Rate Increments after Stress. Korean J. Radiol. 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, R.A.; Brown, R.K.J.; Corbett, J.R. Interpretation of SPECT/CT Myocardial Perfusion Images: Common Artifacts and Quality Control Techniques. Radiographics 2011, 31, 2041–2057. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.A.; Fonte, T.A.; Min, J.K. Computational Fluid Dynamics Applied to Cardiac Computed Tomography for Noninvasive Quantification of Fractional Flow Reserve. J. Am. Coll. Cardiol. 2013, 61, 2233–2241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danad, I.; Szymonifka, J.; Schulman-Marcus, J.; Min, J.K. Static and dynamic assessment of myocardial perfusion by computed tomography. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 836–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sand, N.P.R.; Veien, K.T.; Nielsen, S.S.; Nørgaard, B.L.; Larsen, P.; Johansen, A.; Hess, S.; Deibjerg, L.; Husain, M.; Junker, A.; et al. Prospective Comparison of FFR Derived From Coronary CT Angiography With SPECT Perfusion Imaging in Stable Coronary Artery Disease. JACC Cardiovasc. Imaging 2018, 11, 1640–1650. [Google Scholar] [CrossRef]
- Nørgaard, B.L.; Leipsic, J.; Gaur, S.; Seneviratne, S.; Ko, B.; Ito, H.; Jensen, J.M.; Mauri, L.; De Bruyne, B.; Bezerra, H.; et al. Diagnostic Performance of Noninvasive Fractional Flow Reserve Derived From Coronary Computed Tomography Angiography in Suspected Coronary Artery Disease. J. Am. Coll. Cardiol. 2014, 63, 1145–1155. [Google Scholar] [CrossRef] [Green Version]
- Grover, R.; Leipsic, J.; Mooney, J.; Kueh, S.-H.; Ohana, M.; Nørgaard, B.L.; Eftekhari, A.; Bax, J.J.; Murphy, D.; Hague, C.J.; et al. Coronary lumen volume to myocardial mass ratio in primary microvascular angina. J. Cardiovasc. Comput. Tomogr. 2017, 11, 423–428. [Google Scholar] [CrossRef]
- Tatineni, S.; Kern, M.J.; Deligonul, U.; Aguirre, F. The effects of ionic and nonionic radiographic contrast media on coronary hyperemia in patients during coronary angiography. Am. Heart J. 1992, 123, 621–627. [Google Scholar] [CrossRef]
- Canty, J.M.; Judd, R.M.; Brody, A.S.; Klocke, F.J. First-pass entry of nonionic contrast agent into the myocardial extravascular space. Effects on radiographic estimates of transit time and blood volume. Circulation 1991, 84, 2071–2078. [Google Scholar] [CrossRef] [Green Version]
- Agostini, D.; Roule, V.; Nganoa, C.; Roth, N.; Baavour, R.; Parienti, J.-J.; Beygui, F.; Manrique, A. First validation of myocardial flow reserve assessed by dynamic 99mTc-sestamibi CZT-SPECT camera: Head to head comparison with 15O-water PET and fractional flow reserve in patients with suspected coronary artery disease. The WATERDAY study. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1079–1090. [Google Scholar] [CrossRef] [Green Version]
- Slomka, P.J.; Berman, D.S.; Alexanderson-Rosas, E.; Germano, G. The role of PET quantification in cardiovascular imaging. Clin. Transl. Imaging 2014, 2, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Nagamachi, S.; Czernin, J.; Kim, A.S.; Sun, K.T.; Böttcher, M.; Phelps, M.E.; Schelbert, H.R. Reproducibility of measurements of regional resting and hyperemic myocardial blood flow assessed with PET. J. Nucl. Med. 1996, 37, 1626–1631. [Google Scholar] [PubMed]
- Kaufmann, P.A.; Gnecchi-Ruscone, T.; Yap, J.T.; Rimoldi, O.; Camici, P.G. Assessment of the reproducibility of baseline and hyperemic myocardial blood flow measurements with 15O-labeled water and PET. J. Nucl. Med. 1999, 40, 1848–1856. [Google Scholar] [PubMed]
- Einstein, A.J.; Moser, K.W.; Thompson, R.C.; Cerqueira, M.D.; Henzlova, M.J. Radiation Dose to Patients From Cardiac Diagnostic Imaging. Circulation 2007, 116, 1290–1305. [Google Scholar] [CrossRef]
- Marroquin, O.C.; Holubkov, R.; Edmundowicz, D.; Rickens, C.; Pohost, G.; Buchthal, S.; Pepine, C.J.; Sopko, G.; Sembrat, R.C.; Meltzer, C.C.; et al. Heterogeneity of microvascular dysfunction in women with chest pain not attributable to coronary artery disease: Implications for clinical practice. Am. Heart J. 2003, 145, 628–635. [Google Scholar] [CrossRef]
- Di Carli, M.F.; Charytan, D.; McMahon, G.T.; Ganz, P.; Dorbala, S.; Schelbert, H.R. Coronary Circulatory Function in Patients with the Metabolic Syndrome. J. Nucl. Med. 2011, 52, 1369–1377. [Google Scholar] [CrossRef] [Green Version]
- Lortie, M.; Beanlands, R.S.B.; Yoshinaga, K.; Klein, R.; DaSilva, J.N.; Dekemp, R.A. Quantification of myocardial blood flow with 82Rb dynamic PET imaging. Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 1765–1774. [Google Scholar] [CrossRef]
- Liu, A.; Wijesurendra, R.S.; Liu, J.M.; Forfar, J.C.; Channon, K.M.; Jerosch-Herold, M.; Piechnik, S.K.; Neubauer, S.; Kharbanda, R.K.; Ferreira, V.M. Diagnosis of Microvascular Angina Using Cardiac Magnetic Resonance. J. Am. Coll. Cardiol. 2018, 71, 969–979. [Google Scholar] [CrossRef]
- Schwitter, J.; Wacker, C.M.; Wilke, N.; Al-Saadi, N.; Sauer, E.; Huettle, K.; Schönberg, S.O.; Luchner, A.; Strohm, O.; Ahlstrom, H.; et al. MR-IMPACT II: Magnetic Resonance Imaging for Myocardial Perfusion Assessment in Coronary artery disease Trial: Perfusion-cardiac magnetic resonance vs. single-photon emission computed tomography for the detection of coronary artery disease: A comparative multicentre, multivendor trial. Eur. Heart J. 2012, 34, 775–781. [Google Scholar] [CrossRef] [Green Version]
- Thomson, L.E.; Wei, J.; Agarwal, M.; Haft-Baradaran, A.; Shufelt, C.; Mehta, P.K.; Gill, E.B.; Johnson, B.D.; Kenkre, T.; Handberg, E.; et al. Cardiac magnetic resonance myocardial perfusion reserve index is reduced in women with coronary microvascular dysfunction. A National Heart, Lung, and Blood Institute-sponsored study from the Women’s Ischemia Syndrome Evaluation. Circ. Cardiovasc. Imaging 2015, 8, e002481. [Google Scholar] [CrossRef] [Green Version]
- Kotecha, T.; Martinez-Naharro, A.; Boldrini, M.; Knight, D.; Hawkins, P.; Kalra, S.; Patel, D.; Coghlan, G.; Moon, J.; Plein, S.; et al. Automated Pixel-Wise Quantitative Myocardial Perfusion Mapping by CMR to Detect Obstructive Coronary Artery Disease and Coronary Microvascular Dysfunction. JACC Cardiovasc. Imaging 2019, 12, 1958–1969. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.; Wijesurendra, R.S.; Francis, J.M.; Robson, M.D.; Neubauer, S.; Piechnik, S.K.; Ferreira, V.M. Adenosine Stress and Rest T1 Mapping Can Differentiate Between Ischemic, Infarcted, Remote, and Normal Myocardium Without the Need for Gadolinium Contrast Agents. JACC Cardiovasc. Imaging 2016, 9, 27–36. [Google Scholar] [CrossRef]
- Piechnik, S.K.; Neubauer, S.; Ferreira, V.M. State-of-the-art review: Stress T1 mapping-technical considerations, pitfalls and emerging clinical applications. Magn. Reson. Mater. Phys. Boil. Med. 2017, 31, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.; Wijesurendra, R.S.; Liu, J.M.; Greiser, A.; Jerosch-Herold, M.; Forfar, J.C.; Channon, K.M.; Piechnik, S.K.; Neubauer, S.; Kharbanda, R.K.; et al. Gadolinium-Free Cardiac MR Stress T1-Mapping to Distinguish Epicardial From Microvascular Coronary Disease. J. Am. Coll. Cardiol. 2018, 71, 957–968. [Google Scholar] [CrossRef] [PubMed]
- Piechnik, S.K.; Ferreira, V.M.; Dall′armellina, E.; Cochlin, L.E.; Greiser, A.; Neubauer, S.; Robson, M.D. Shortened Modified Look-Locker Inversion recovery (ShMOLLI) for clinical myocardial T1-mapping at 1.5 and 3 T within a 9 heartbeat breathhold. J. Cardiovasc. Magn. Reson. 2010, 12, 69. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.M.; Liu, A.; Leal, J.; McMillan, F.; Francis, J.; Greiser, A.; Rider, O.J.; Myerson, S.G.; Neubauer, S.; Ferreira, V.M.; et al. Measurement of myocardial native T1 in cardiovascular diseases and norm in 1291 subjects. J. Cardiovasc. Magn. Reson. 2017, 19, 74. [Google Scholar] [CrossRef]
- Le, D.E.; Jayaweera, A.R.; Wei, K.; Coggins, M.P.; Lindner, J.R.; Kaul, S. Changes in myocardial blood volume over a wide range of coronary driving pressures: Role of capillaries beyond the autoregulatory range. Heart 2004, 90, 1199–1205. [Google Scholar] [CrossRef] [Green Version]
- Lindner, J.R.; Skyba, D.M.; Goodman, N.C.; Jayaweera, A.R.; Kaul, S. Changes in myocardial blood volume with graded coronary stenosis. Am. J. Physiol. Circ. Physiol. 1997, 272, H567–H575. [Google Scholar] [CrossRef]
- Detre, J.A.; Wang, J.; Wang, Z.; Rao, H. Arterial spin-labeled perfusion MRI in basic and clinical neuroscience. Curr. Opin. Neurol. 2009, 22, 348–355. [Google Scholar] [CrossRef]
- Wu, W.-C.; Mohler, E.; Ratcliffe, S.J.; Wehrli, F.W.; Detre, J.A.; Floyd, T.F. Skeletal Muscle Microvascular Flow in Progressive Peripheral Artery Disease. J. Am. Coll. Cardiol. 2009, 53, 2372–2377. [Google Scholar] [CrossRef] [Green Version]
- Fenchel, M.; Martirosian, P.; Langanke, J.; Giersch, J.; Miller, S.; Stauder, N.I.; Kramer, U.; Claussen, C.D.; Schick, F. Perfusion MR Imaging with FAIR True FISP Spin Labeling in Patients with and without Renal Artery Stenosis: Initial Experience. Radiology 2006, 238, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Mathew, R.C.; Kramer, C.M. Recent advances in magnetic resonance imaging for peripheral artery disease. Vasc. Med. 2018, 23, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zun, Z.; Varadarajan, P.; Pai, R.G.; Wong, E.C.; Nayak, K.S. Arterial Spin Labeled CMR Detects Clinically Relevant Increase in Myocardial Blood Flow With Vasodilation. JACC Cardiovasc. Imaging 2011, 4, 1253–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iannino, N.; Fischer, K.; Friedrich, M.; Hafyane, T.; Mongeon, F.-P.; White, M. Myocardial Vascular Function Assessed by Dynamic Oxygenation-sensitive Cardiac Magnetic Resonance Imaging Long-term Following Cardiac Transplantation. Transplantation 2020. [Google Scholar] [CrossRef] [PubMed]
- Guethlin, M.; Kasel, A.M.; Coppenrath, K.; Ziegler, S.; Delius, W.; Schwaiger, M. Delayed response of myocardial flow reserve to lipid-lowering therapy with fluvastatin. Circulation 1999, 99, 475–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, N.R.; Cheezum, M.K.; Veeranna, V.; Horgan, S.J.; Taqueti, V.R.; Murthy, V.L.; Foster, C.; Hainer, J.; Daniels, K.M.; Rivero, J.; et al. Ranolazine in Symptomatic Diabetic Patients Without Obstructive Coronary Artery Disease: Impact on Microvascular and Diastolic Function. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef]
- Merz, N.B.; Handberg, E.; Shufelt, C.L.; Mehta, P.K.; Minissian, M.B.; Wei, J.; Thomson, L.E.; Berman, D.S.; Shaw, L.J.; Petersen, J.W.; et al. A randomized, placebo-controlled trial of late Na current inhibition (ranolazine) in coronary microvascular dysfunction (CMD): Impact on angina and myocardial perfusion reserve. Eur. Heart J. 2015, 37, 1504–1513. [Google Scholar] [CrossRef]
- Quercioli, A.; Montecucco, F.; Pataky, Z.; Thomas, A.; Ambrosio, G.; Staub, C.; Di Marzo, V.; Ratib, O.; Mach, F.; Golay, A.; et al. Improvement in coronary circulatory function in morbidly obese individuals after gastric bypass-induced weight loss: Relation to alterations in endocannabinoids and adipocytokines. Eur. Heart J. 2013, 34, 2063–2073. [Google Scholar] [CrossRef]
- Park, S.-J.; Park, J.J.; Choi, D.-J.; Chun, E.J.; Choi, S.I.; Kim, S.M.; Jang, S.Y.; Ahn, S.; Choe, Y.H. Understanding of chest pain in microvascular disease proved by cardiac magnetic resonance image (UMPIRE): Study protocol for a randomized controlled trial. Trials 2014, 15, 1–9. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imaging Modality | Availability | Accuracy | Reproducibility | Prognostic Validation | Diagnostic Parameter | Cost |
|---|---|---|---|---|---|---|
| Echocardiography | ++++ | ++ | +++ | +++ | CFVR | $ |
| Cardiac CT | +++ | + | + | n/a | V/M | $$ |
| SPECT | ++++ | + | ++ | + | CFR | $$ |
| PET | ++ | ++++ | ++++ | ++++ | CFR | $$$ |
| CMR | ++ | +++ | +++ | ++ | MPRI | $$$ |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayub, M.T.; Kalra, D. Coronary Microvascular Dysfunction and the Role of Noninvasive Cardiovascular Imaging. Diagnostics 2020, 10, 679. https://doi.org/10.3390/diagnostics10090679
Ayub MT, Kalra D. Coronary Microvascular Dysfunction and the Role of Noninvasive Cardiovascular Imaging. Diagnostics. 2020; 10(9):679. https://doi.org/10.3390/diagnostics10090679
Chicago/Turabian StyleAyub, Muhammad Talha, and Dinesh Kalra. 2020. "Coronary Microvascular Dysfunction and the Role of Noninvasive Cardiovascular Imaging" Diagnostics 10, no. 9: 679. https://doi.org/10.3390/diagnostics10090679