Clinical Significance and Diagnostic Value of Pain Extent Extracted from Pain Drawings: A Scoping Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Identify the Research Question
2.2. Identify Relevant Studies
2.3. Study Selection
2.4. Chart Data
2.5. Data Mapping
2.6. Methodological Quality
3. Results
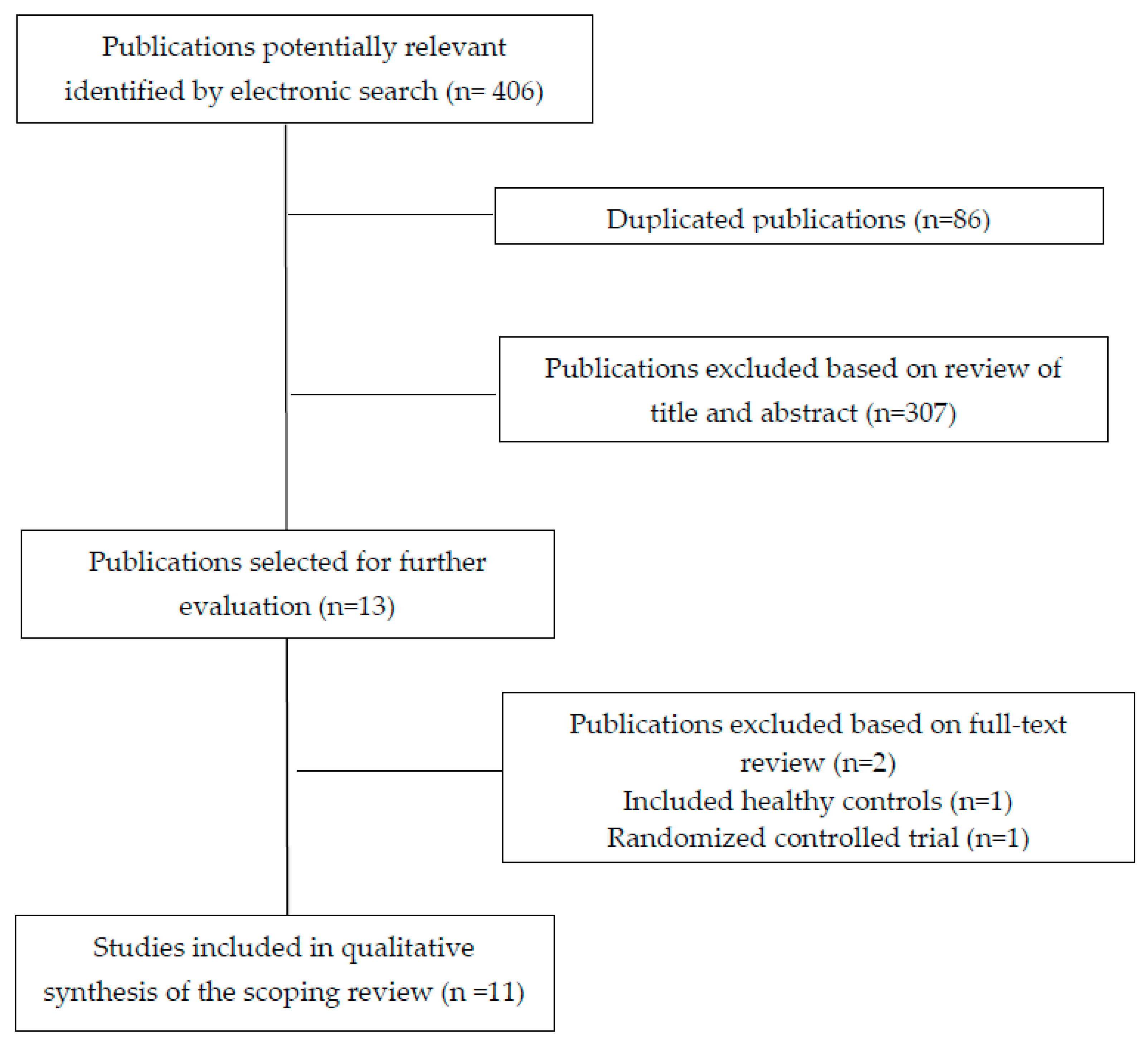
3.1. Study Selection
3.2. Study Characteristic
3.3. Methodological Quality
3.4. Summarizing Findings
4. Discussion
4.1. Literature Mapping
4.2. Limitations of Current Literature and Implications for Research
4.3. Strengths and Limitations of the Review
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Palmer, H. Pain charts: A description of a technique whereby functional pain may be diagnosed from organic pain. N. Z. Med. J. 1949, 48, 187–213. [Google Scholar] [PubMed]
- Schott, G.D. The cartography of pain: The evolving contribution of pain maps. Eur. J. Pain 2010, 14, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Carnes, D.; Ashby, D.; Underwood, M. A systematic review of pain drawing literature: Should pain drawings be used for psychologic screening? Clin. J. Pain 2006, 22, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Melzack, R. The McGill pain questionnaire: Major properties and scoring methods. Pain 1975, 1, 277–299. [Google Scholar] [CrossRef]
- Persson, A.L.; Garametsos, S.; Pedersen, J. Computer-aided surface estimation of pain drawings: Intra- and inter-rater reliability. J. Pain Res. 2011, 4, 135–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Reis, F.J.; de Barros ESilva, V.; de Lucena, R.N.; Mendes Cardoso, B.A.; Nogueira, L.C. Measuring the pain area: An intra- and inter-rater reliability study using image analysis software. Pain Pract. 2016, 16, 24–30. [Google Scholar] [CrossRef]
- Corrêa, L.A.; Bittencourt, J.V.; Ferreira, A.S.; Reis, F.J.J.D.; de Almeida, R.S.; Nogueira, L.A.C. The reliability and concurrent validity of PainMAP software for automated quantification of pain drawings on body charts of patients with low back pain. Pain Pract. 2020, 20, 462–470. [Google Scholar]
- Shaballout, N.; Neubert, T.A.; Boudreau, S.; Beissner, F. From paper to digital applications of the pain drawing: Systematic review of methodological milestones. JMIR Mhealth Uhealth 2019, 7, e14569. [Google Scholar] [CrossRef] [Green Version]
- Boudreau, S.A.; Royo, A.C.; Matthews, M.; Graven-Nielsen, T.; Kamavuako, E.N.; Slabaugh, G.; Thorborg, K.; Vicenzino, B.; Rathleff, M.S. Distinct patterns of variation in the distribution of knee pain. Sci. Rep. 2018, 8, 16522. [Google Scholar] [CrossRef] [Green Version]
- Barbero, M.; Moresi, F.; Leoni, D.; Gatti, R.; Egloff, M.; Falla, D. Test-retest reliability of pain extent and pain location using a novel method for pain drawing analysis. Eur. J. Pain 2015, 19, 1129–1138. [Google Scholar]
- Leoni, D.; Falla, D.; Heitz, C.; Capra, G.; Clijsen, R.; Egloff, M.; Cescon, C.; Baeyens, J.P.; Barbero, M. Test-retest reliability in reporting the pain induced by a pain provocation test: Further validation of a novel approach for pain drawing acquisition and analysis. Pain Pract. 2017, 17, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 1932. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar]
- Peters, M.D. In no uncertain terms: The importance of a defined objective in scoping reviews. JBI Database Syst. Rev. Implement Rep. 2016, 14, 14. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Tugwell, P.; O’Connell, D.; Welch, V.; Peterson, J.; Shea, B.; Losos, M. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Ontario; Canada. 2015. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 10 July 2020).
- McPheeters, M.L.; Kripalani, S.; Peterson, N.B.; Idowu, R.T.; Jerome, R.N.; Potter, S.A.; Andrews, J.C. Closing the quality gap: Revisiting the state of the science (vol. 3: Quality improvement interventions to address health disparities). Evid. Rep. Technol. Assess (Full Rep.) 2012, 2083, 1–475. [Google Scholar]
- Fernández-de-las-Peñas, C.; de-la-Llave-Rincón, A.I.; Cescon, C.; Barbero, M.; Arias-Buría, J.L.; Falla, D. Influence of clinical, psychological, and psychophysical variables on long-term treatment outcomes in carpal tunnel syndrome: Evidence from a randomized clinical trial. Pain Pract. 2019, 19, 644–655. [Google Scholar] [CrossRef]
- Lluch Girbés, E.; Dueñas, L.; Barbero, M.; Falla, D.; Baert, I.A.; Meeus, M.; Sánchez-Frutos, J.; Aguilella, L.; Nijs, J. Expanded distribution of pain as a sign of central sensitization in individuals with symptomatic knee osteoarthritis. Phys. Ther. 2016, 96, 1196–1207. [Google Scholar] [CrossRef] [Green Version]
- Falla, D.; Peolsson, A.; Peterson, G.; Ludvigsson, M.L.; Soldini, E.; Schneebeli, A.; Barbero, M. Perceived pain extent is associated with disability, depression and self-efficacy in individuals with whiplash-associated disorders. Eur. J. Pain 2016, 20, 1490–1501. [Google Scholar] [CrossRef] [Green Version]
- Palacios-Ceña, M.; Barbero, M.; Falla, D.; Ghirlanda, F.; Arend-Nielsen, L.; Fernández-de-Las-Peñas, C. Pain extent is associated with the emotional and physical burden of chronic tension-type headache, but not with depression or anxiety. Pain Med. 2017, 18, 2033–2039. [Google Scholar] [CrossRef] [PubMed]
- Barbero, M.; Fernández-de-las-Peñas, C.; Palacios-Ceña, M.; Cescon, C.; Falla, D. Pain extent is associated with pain intensity but not with widespread pressure or thermal pain sensitivity in women with fibromyalgia syndrome. Clin. Rheumatol. 2017, 36, 1427–1432. [Google Scholar] [CrossRef] [PubMed]
- Cruder, C.; Falla, D.; Mangili, F.; Azzimonti, L.; Araújo, L.S.; Williamon, A.; Barbero, M. Profiling the location and extent of musicians’ pain using digital pain drawings. Pain Pract. 2018, 18, 53–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-de-las-Peñas, C.; Falla, D.; Palacios-Ceña, M.; Fuensalida-Novo, S.; Arias-Buría, J.L.; Schneebeli, A.; Arend-Nielsen, L.; Barbero, M. Perceived pain extent is not associated with widespread pressure pain sensitivity, clinical features, related disability, anxiety, or depression in women with episodic migraine. Clin. J. Pain 2018, 34, 217–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-de-las-Peñas, C.; Falla, D.; Palacios-Ceña, M.; De-la-Llave-Rincón, A.I.; Schneebeli, A.; Barbero, M. Perceived pain extent is not associated with physical, psychological, or psychophysical outcomes in women with carpal tunnel syndrome. Pain Med. 2019, 20, 1185–1192. [Google Scholar]
- Abichandani, D.; Barbero, M.; Cescon, C.; Gallace, A.; Punt, D.; Sanchis-Sanchez, E.; Falla, D. Can people with chronic neck pain recognize their own digital pain drawing? Pain Physician 2020, 23, E231–E240. [Google Scholar]
- Willett, M.J.; Siebertz, M.; Petzke, F.; Erlenwein, J.; Rushton, A.; Soldini, E.; Barbero, M.; Falla, D. The extent of pain is associated with signs of central sensitization in patients with hip osteoarthritis. Pain Pract. 2020, 20, 277–288. [Google Scholar] [CrossRef]
- Ris, I.; Barbero, M.; Falla, D.; Larsen, M.H.; Kraft, M.N.; Søgaard, K.; Juul-Kristensen, B. Pain extent is more strongly associated with disability, psychological factors, and neck muscle function in people with non-traumatic versus traumatic chronic neck pain: A cross sectional study. Eur. J. Phys. Rehabil. Med. 2019, 55, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Arendt-Nielsen, L.; Graven-Nielsen, T. Translational musculoskeletal pain research. Best Pract. Res. Clin. Rheumatol. 2011, 25, 209–226. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef] [PubMed]
- Ohtori, S.; Orita, S.; Yamashita, M.; Ishikawa, T.; Ito, T.; Shigemura, T.; Nishiyama, H.; Konno, S.; Ohta, H.; Takaso, M.; et al. Existence of a neuropathic pain component in patients with osteoarthritis of the knee. Yonsei Med. J. 2012, 53, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, L.; Rosso, A.; Romeo, A.; Villafañe, J.H.; Guccione, A.A.; Pillastrini, P.; Vanti, C. The accuracy of pain drawing in identifying psychological distress in low back pain-systematic review and meta-analysis of diagnostic studies. J. Phys. Ther. Sci. 2015, 27, 3319–3324. [Google Scholar] [CrossRef] [Green Version]
- Fillingim, R.B.; Loeser, J.D.; Baron, R.; Edwards, R. Assessment of chronic pain: Domains, methods, and mechanisms. J. Pain 2016, 17, T10–T20. [Google Scholar] [PubMed] [Green Version]
- Arendt-Nielsen, L.; Morlion, B.; Perrot, S.; Dahan, A.; Dickenson, A.; Kress, H.G.; Wells, C.; Bouhassira, D.; Mohr Drewes, A. Assessment and manifestation of central sensitization across different pain conditions. Eur. J. Pain 2018, 22, 216–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masferrer, R.; Prendergast, V.; Hagell, P. Colored pain drawings: Preliminary observations in a neurosurgical practice. Eur. J. Pain 2003, 7, 213–217. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PubMed Search Formula #1 “Pain Drawing” [Title/Abstract] OR “Pain Draw” [Title/Abstract] OR “Pain Extent” [Title/Abstract] OR “Pain Chart” [Title/Abstract] OR “Pain Area” [Title/Abstract] OR “Pain Map” [Title/Abstract] #2 “Pain” [Mesh] OR “Related-disability” [Title/Abstract] OR “Function” [Title/Abstract] OR “Mobility” [Title/Abstract] OR “Quality of Life” [Title/Abstract] OR “Anxiety” [Mesh] OR “Depression” [Mesh] OR “Quantitative Sensory Testing” [Title/Abstract] OR “Pain Thresholds” [Mesh] #3 #1 AND #2 |
| CINAHL/Medline (via EBSCO) Search Formula #1 “Pain Drawing” OR “Pain Draw” OR “Pain Extent” OR “Pain Chart” OR “Pain Area” OR “Pain Map” #2 “Pain” OR “Related-disability” OR “Function” OR “Mobility” OR “Quality of Life” OR “Anxiety” OR “Depression” OR “Quantitative Sensory Testing” OR “Pain Thresholds” #3 #1 AND #2 |
| SCOPUS Search Formula TITLE-ABS-KEY (“Pain Drawing” OR “Pain Draw” OR “Pain Extent” OR “Pain Chart” OR “Pain Area” OR “Pain Map”) AND TITLE-ABS-KEY (“Pain” OR “Related-disability” OR “Function” OR “Mobility” OR “Quality of Life” OR “Anxiety” OR “Depression” OR “Quantitative Sensory Testing” OR “Pain Thresholds”) |
| WOS (EMBASE, AMED) Search Formula (“Pain Drawing” OR “Pain Draw” OR “Pain Extent” OR “Pain Chart” OR “Pain Area” OR “Pain Map”) AND (“Pain” OR “Related-disability” OR “Function” OR “Mobility” OR “Quality of Life” OR “Anxiety” OR “Depression” OR “Quantitative Sensory Testing” OR “Pain Thresholds”) |
| Author | Population | Sample (Men/Women) | Mean Age (Years) | Outcome | Results Summary |
|---|---|---|---|---|---|
| Barbero et al. [10] | Neck Pain Low Back Pain | 56 (15/41) 51 (20/31) | 50.3 (15.0) 48.5 (14.1) | Pain Extent Clinical outcomes: BMI, age, pain duration, pain (VAS, 0–100), function (NDI, or RMDQ) Psychological outcomes: K-10, MoCa | Significant correlations were observed between pain extent and pain intensity in both conditions, between pain extent and disability in neck pain |
| Lluch-Girbés et al. [20] | Knee Osteoarthritis | 53 (19/34) | 70.2 (7.4) | Pain Extent Clinical outcomes: Pain (NPRS, 0–10), function (WOMAC) Psychological outcomes: PCS, PVAQ, CPAQ, TSK Psycho-physical outcomes: PPTs, CPM, CSI, PD-Q | Significant positive correlations between pain extent with pain and stiffness subscales of WOMAC and CSI score were found. Significant negative correlations between pain extent and PPTs were found |
| Falla et al. [21] | Whiplash-associated disorders | 205 (133/72) | 40.1 (11.4) | Pain Extent Clinical outcomes: Pain (VAS, 0–100), function (NDI, 0–100), PDI, EQ-5D Psychological outcomes: TSK, PCS, HADS-A, HADS-D, SES Others: Effort-Reward Imbalance Scale | Pain extent was influenced by sex, insurance status and worse financial situation. Positive significant associations between pain extent with NDI, HADS-D and PDI were found. A negative significant association between pain extent and SES was found |
| Palacios-Ceña et al. [22] | Chronic Tension-Type Headache | 99 (27/72) | 47 (44–50) | Pain Extent Clinical outcomes: Age, headache intensity, duration and frequency, HDI-E, HDI-P Psychological outcomes: HADS-A, HADS-D, STAI-T, STAI-S. Psycho-physical outcomes: PPTs | Significant positive associations were found between pain extent with age and the burden of the headache (HDI-E and HDI-P) |
| Barbero et al. [23] | Fibromyalgia | 30 (0/30) | 52 (12) Median | Pain Extent Clinical outcomes: Age, pain duration, pain (NPRS, 0–10), function (FIQ), tender point count Psycho-physical outcomes: PPTs, HPTs, CPTs | Significant negative correlations were observed between pain extent with age and pain duration A significant positive association between pain extent and worst level of pain was found |
| Cruder et al. [24] | Musicians | 158 (68/90) | 22.4 (3.6) | Pain extent Clinical outcomes: BMI, practicing (hours), pain intensity (1–5), function (QD Score, and QD score optional module) | Significant positive correlations between pain extent with pain intensity, QD and QD optional module were found |
| Fernández-de-las-Peñas et al. [25] | Episodic Migraine | 72 (0/72) | 42 (10.22) | Pain extent Clinical outcomes: Age, migraine intensity, duration and frequency Psychological outcomes: HADS-A, HADS-D, STAI-T, STAI-S. Psycho-physical outcomes: PPTs | No significant associations between pain extent with any clinical, psychological or psycho-physical variables were observed |
| Fernández-de-las-Peñas et al. [26] | Carpal Tunnel Syndrome | 140 (0/140) | 47 (13.5) median | Pain extent Clinical outcomes: Age, pain duration, pain (NPRS, 0–10), function (BCTQ, 0–5) Psycho-physical outcomes: PPTs, HPTs, CPTs | A significative positive correlation between pain extent and CPT over carpal tunnel was observed |
| Ris et al. [29] | Neck pain Traumatic Nek Pain Non-traumatic Neck Pain | 200 (75/125) 120 80 | 43.5 (11.4) 47.6 (11.4) | Pain Extent Clinical outcomes: Function (NDI), quality of life (SF36) Psychological outcomes: BDI-II, TSK Others: ROM, CCFT | Significative positive correlations between pain extent with NDI (all groups), BDI-II (all groups) and TSK (neck pain and nontraumatic pain groups) were seen Significative negative correlations between pain extent and muscle function (CCFT and CE) in neck pain and nontraumatic pain groups) were observed |
| Abichandani et al. [27] | Chronic Neck Pain | 20 (0/20) | 26 (2–32) Median | Pain Extent Recognition of pain drawing Clinical outcomes: age, pain duration, pain (NPRS, 0–10), NDI Psychological outcomes: PCS, DASS-42, MSPQ | A significative negative correlation was observed between recognition of pain drawing and MSPQ |
| Willet et al. [28] | Hip Osteoarthritis | 30 (15/15) | 61 (55.25–64) median | Pain extent Clinical outcomes: Age, function (Oxford Hip Score), pain (WPI), symptoms (FMS-SSS), PD-Q Psychological outcomes: DASS, TSK, PCS, CPAQ Psycho-physical outcomes: PTTs, CPTs, HPTs | Paint extent demonstrated significant association with WPI and PD-Q Pain extent was also associated with lower PPTs in the lower extremity, higher CPTs at the greater trochanter, reduced HPTs at the greater trochanter and reduced WDTs over the thenar eminence |
| Selection | Comparability | Exposure | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | Representativeness of Exposed Cohort | Selection of Non-Exposed Cohort | Ascertainment of Exposure | Outcome of Interest nor Present at Start | Study Controls for Age/Gender | Study Controls for Additional Factor | Assessment of Outcome | Long Enough Follow-Up | Adequate Follow-Up | Score |
| Barbero et al. [10] | ★ | ★ | ★ | 3/3 | ||||||
| Lluch-Girbés et al. [20] | ★ | ★ | ★ | 3/3 | ||||||
| Falla et al. [21] | ★ | ★ | ★ | 3/3 | ||||||
| Palacios-Ceña et al. [22] | ★ | ★ | ★ | 3/3 | ||||||
| Barbero et al. [23] | ★ | ★ | ★ | 3/3 | ||||||
| Cruder et al. [24] | ★ | ★ | ★ | 3/3 | ||||||
| Fernández-de-las-Peñas et al. [25] | ★ | ★ | ★ | 3/3 | ||||||
| Fernández-de-las-Peñas et al. [26] | ★ | ★ | ★ | 3/3 | ||||||
| Ris et al. [29] | ★ | ★ | ★ | 3/3 | ||||||
| Abichandani et al. [27] | ★ | ★ | 2/3 | |||||||
| Willet et al. [28] | ★ | ★ | ★ | 3/3 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbero, M.; Navarro-Santana, M.J.; Palacios-Ceña, M.; Ortega-Santiago, R.; Cescon, C.; Falla, D.; Fernández-de-las-Peñas, C. Clinical Significance and Diagnostic Value of Pain Extent Extracted from Pain Drawings: A Scoping Review. Diagnostics 2020, 10, 604. https://doi.org/10.3390/diagnostics10080604
Barbero M, Navarro-Santana MJ, Palacios-Ceña M, Ortega-Santiago R, Cescon C, Falla D, Fernández-de-las-Peñas C. Clinical Significance and Diagnostic Value of Pain Extent Extracted from Pain Drawings: A Scoping Review. Diagnostics. 2020; 10(8):604. https://doi.org/10.3390/diagnostics10080604
Chicago/Turabian StyleBarbero, Marco, Marcos J. Navarro-Santana, María Palacios-Ceña, Ricardo Ortega-Santiago, Corrado Cescon, Deborah Falla, and César Fernández-de-las-Peñas. 2020. "Clinical Significance and Diagnostic Value of Pain Extent Extracted from Pain Drawings: A Scoping Review" Diagnostics 10, no. 8: 604. https://doi.org/10.3390/diagnostics10080604