Recent Advances in Ultrasound Diagnosis of Carpal Tunnel Syndrome


Abstract
:1. Introduction
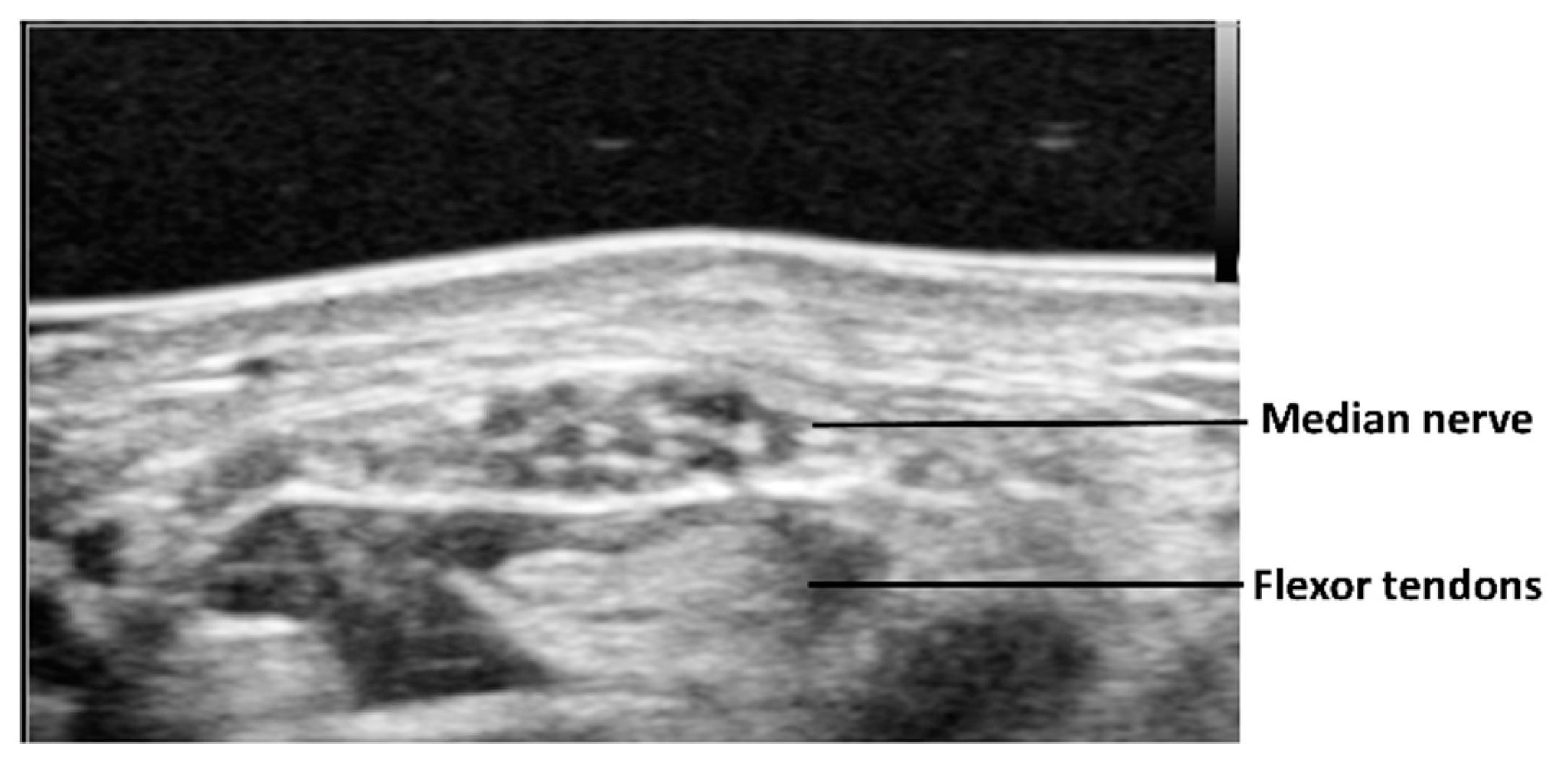
2. Static Cross-Sectional Ultrasound for CTS Assessment
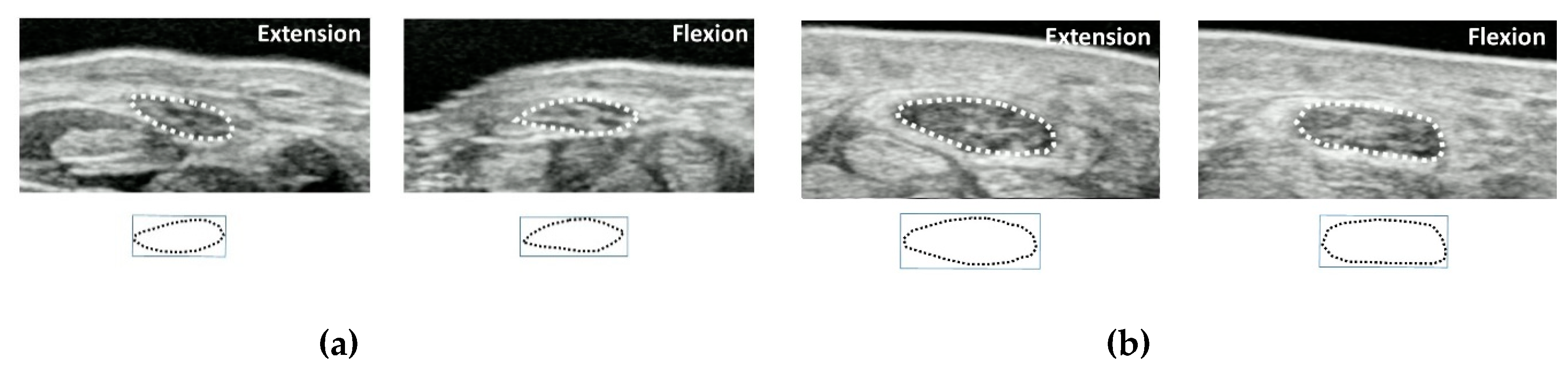
3. Dynamic Ultrasound for CTS Assessment
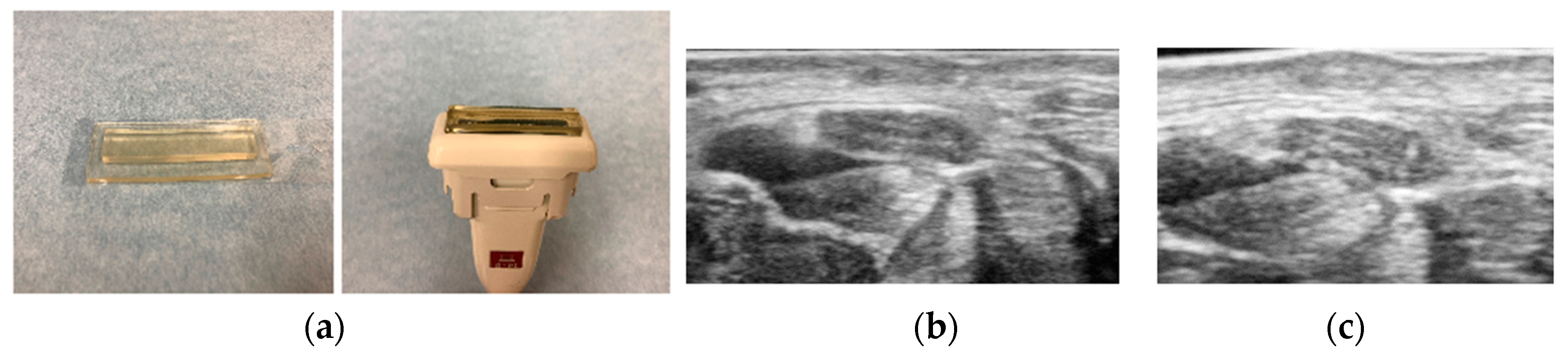
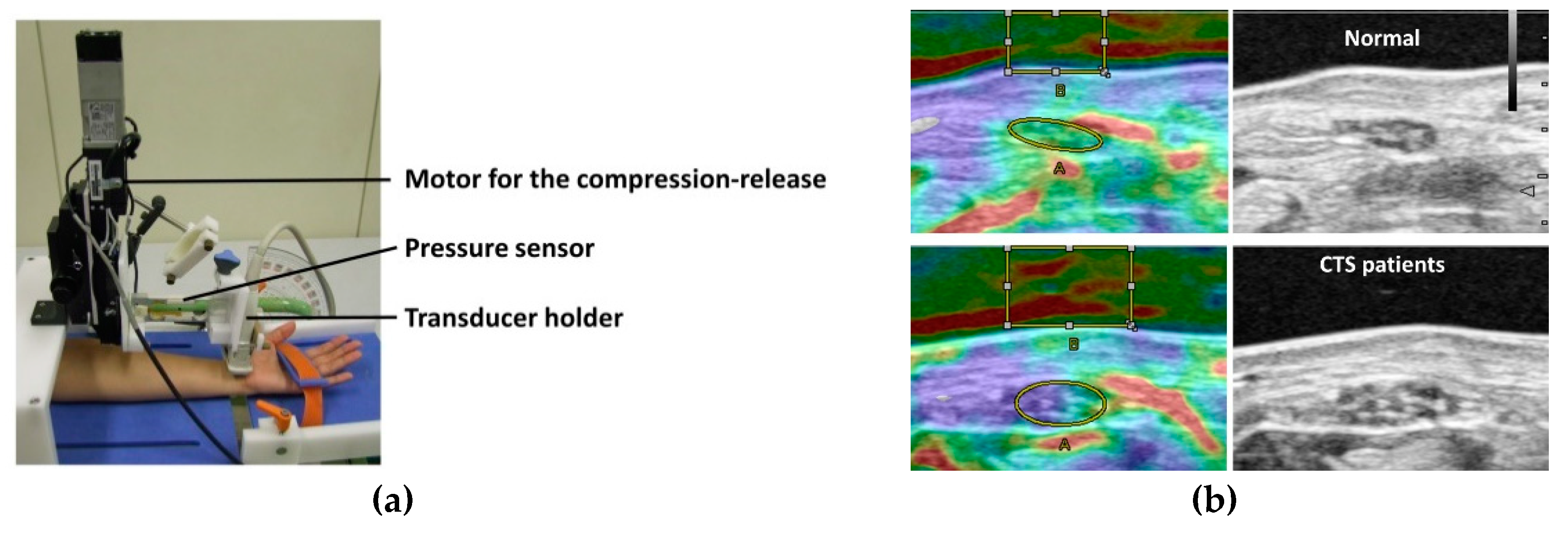
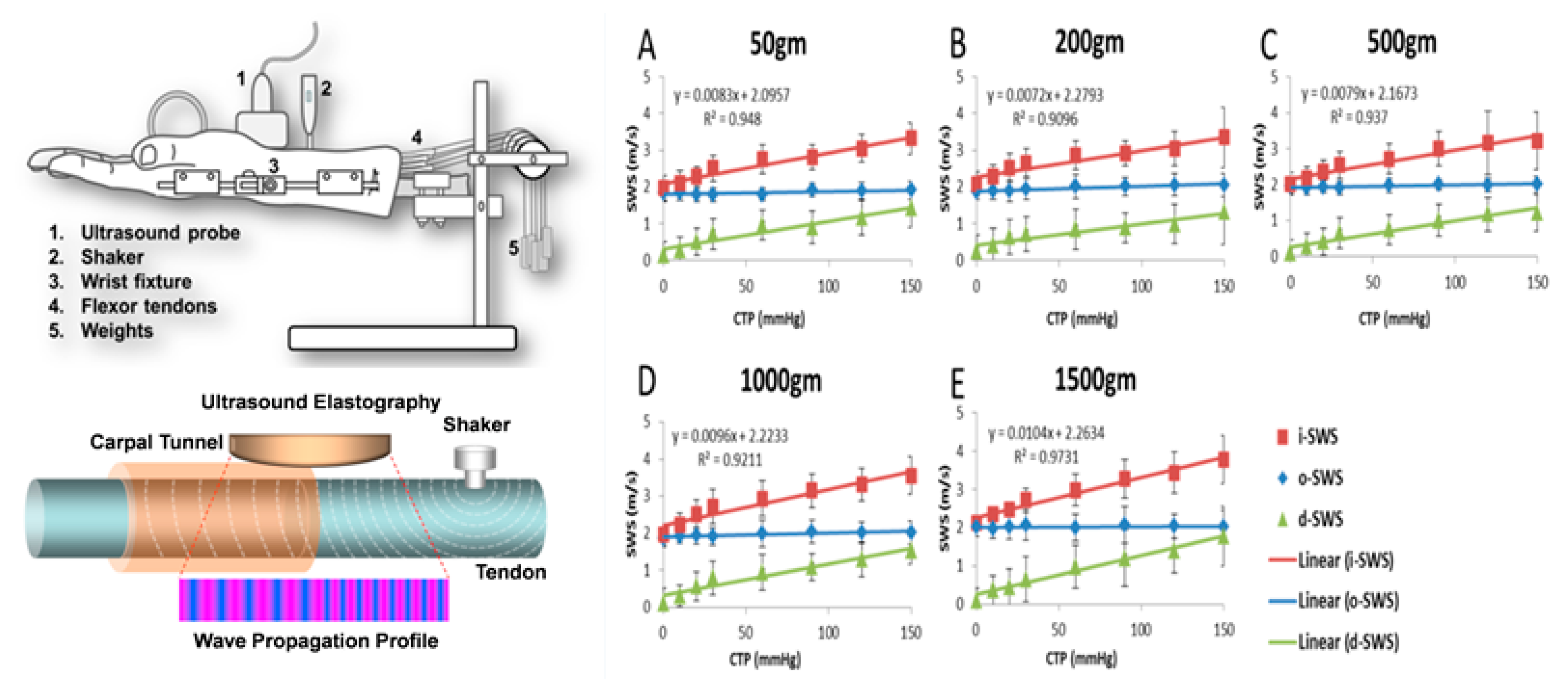
4. Ultrasound Elastography for CTS Assessment
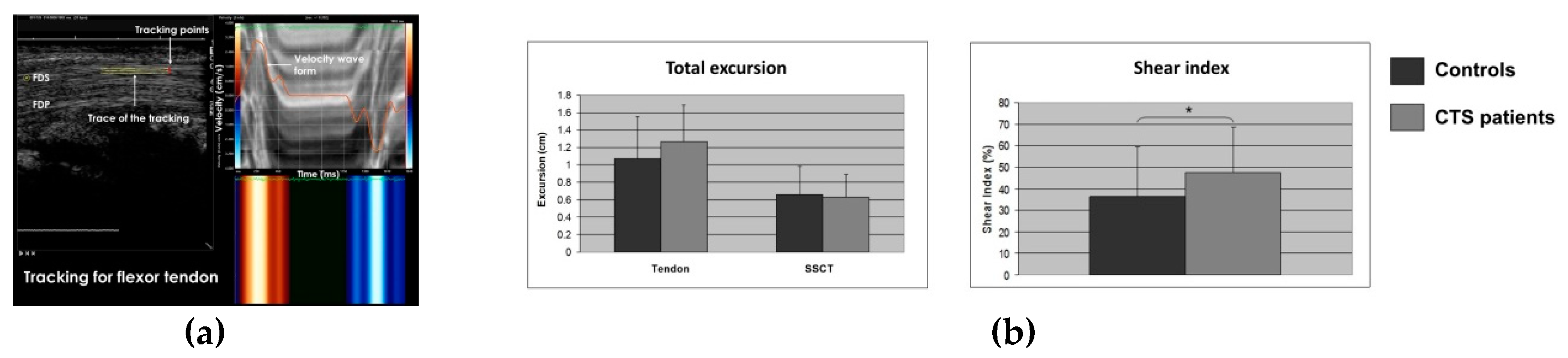
5. Speckle Tracking for CTS Assessment
6. Future Perspectives
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Paget, J. Lectures on Surgical Pathology, 2nd ed.; Lindsay & Blakiston: Philadelphia, PA, USA, 1854. [Google Scholar]
- Phalen, G.S. The carpal-tunnel syndrome. Seventeen years’ experience in diagnosis and treatment of six hundred fifty-four hands. J. Bone Joint Surg. Am. 1966, 48, 211–228. [Google Scholar] [CrossRef]
- Ibrahim, I.; Khan, W.S.; Goddard, N.; Smitham, P. Carpal tunnel syndrome: A review of the recent literature. Open Orthop. J. 2012, 6, 69–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atroshi, I.; Gummesson, C.; Johnsson, R.; Ornstein, E.; Ranstam, J.; Rosen, I. Prevalence of carpal tunnel syndrome in a general population. JAMA 1999, 282, 153–158. [Google Scholar] [CrossRef] [PubMed]
- De Krom, M.C.; Knipschild, P.G.; Kester, A.D.; Thijs, C.T.; Boekkooi, P.F.; Spaans, F. Carpal tunnel syndrome: Prevalence in the general population. J. Clin. Epidemiol. 1992, 45, 373–376. [Google Scholar] [CrossRef]
- Bland, J.D.; Rudolfer, S.M. Clinical surveillance of carpal tunnel syndrome in two areas of the United Kingdom, 1991–2001. J. Neurol. Neurosurg. Psychiatry 2003, 74, 1674–1679. [Google Scholar] [CrossRef] [Green Version]
- Witt, J.C.; Hentz, J.G.; Stevens, J.C. Carpal tunnel syndrome with normal nerve conduction studies. Muscle Nerve 2004, 29, 515–522. [Google Scholar] [CrossRef]
- Koyuncuoglu, H.R.; Kutluhan, S.; Yesildag, A.; Oyar, O.; Guler, K.; Ozden, A. The value of ultrasonographic measurement in carpal tunnel syndrome in patients with negative electrodiagnostic tests. Eur. J. Radiol. 2005, 56, 365–369. [Google Scholar] [CrossRef]
- Atroshi, I.; Gummesson, C.; Johnsson, R.; Ornstein, E. Diagnostic properties of nerve conduction tests in population-based carpal tunnel syndrome. BMC Musculoskelet. Disord. 2003, 4, 9. [Google Scholar] [CrossRef] [Green Version]
- AAEM Quality Assurance Committee; Jablecki, C.K.; Andary, M.T.; So, Y.T.; Wilkins, D.E.; Williams, F.H. Literature review of the usefulness of nerve conduction studies and electromyography for the evaluation of patients with carpal tunnel syndrome. Muscle Nerve 1993, 16, 1392–1414. [Google Scholar]
- Nathan, P.A.; Keniston, R.C.; Meadows, K.D.; Lockwood, B.S. Predictive value of nerve conduction measurements at the carpal tunnel. Muscle Nerve 1993, 16, 1377–1382. [Google Scholar] [CrossRef]
- McDonagh, C.; Alexander, M.; Kane, D. The role of ultrasound in the diagnosis and management of carpal tunnel syndrome: A new paradigm. Rheumatology 2015, 54, 9–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Missere, M. Echography and the carpal tunnel syndrome. Radiol. Med. 1997, 94, 274. [Google Scholar] [PubMed]
- Ferrari, F.S.; Della Sala, L.; Cozza, S.; Guazzi, G.; Belcapo, L.; Mariottini, A.; Bolognini, A.; Stefani, P. High-resolution ultrasonography in the study of carpal tunnel syndrome. Radiol. Med. 1997, 93, 336–341. [Google Scholar] [PubMed]
- Buchberger, W.; Judmaier, W.; Birbamer, G.; Lener, M.; Schmidauer, C. Carpal tunnel syndrome: Diagnosis with high-resolution sonography. Am. J. Roentgenol. 1992, 159, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Duncan, I.; Sullivan, P.; Lomas, F. Sonography in the diagnosis of carpal tunnel syndrome. Am. J. Roentgenol. 1999, 173, 681–684. [Google Scholar] [CrossRef]
- Lee, C.H.; Kim, T.K.; Yoon, E.S.; Dhong, E.S. Correlation of high-resolution ultrasonographic findings with the clinical symptoms and electrodiagnostic data in carpal tunnel syndrome. Ann. Plast Surg. 2005, 54, 20–23. [Google Scholar] [CrossRef]
- Nakamichi, K.; Tachibana, S. Restricted motion of the median nerve in carpal tunnel syndrome. J. Hand Surg. Br. 1995, 20, 460–464. [Google Scholar] [CrossRef]
- Erel, E.; Dilley, A.; Greening, J.; Morris, V.; Cohen, B.; Lynn, B. Longitudinal sliding of the median nerve in patients with carpal tunnel syndrome. J. Hand Surg. Br. 2003, 28, 439–443. [Google Scholar] [CrossRef] [Green Version]
- Nakamichi, K.; Tachibana, S. Ultrasonographic measurement of median nerve cross-sectional area in idiopathic carpal tunnel syndrome: Diagnostic accuracy. Muscle Nerve 2002, 26, 798–803. [Google Scholar] [CrossRef]
- Cartwright, M.; Hobson-Webb, L.; Boon, A.; Alter, K.E.; Hunt, C.H.; Flores, V.H.; Werner, R.A.; Shook, S.J.; Thomas, T.D.; Primack, S.J.; et al. Evidence-based guideline: Neuromuscular ultrasound for the diagnosis of carpal tunnel syndrome. Muscle Nerve 2012, 46, 287–293. [Google Scholar] [CrossRef] [Green Version]
- Yesildag, A.; Kutluhan, S.; Sengul, N.; Koyuncuoglu, H.R.; Oyar, O.; Guler, K.; Gulsoy, U.K. The role of ultrasonographic measurements of the median nerve in the diagnosis of carpal tunnel syndrome. Clin. Radiol. 2004, 59, 910–915. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.M.; Griffith, J.F.; Hui, A.C.; Lo, S.K.; Fu, M.; Wong, K.S. Carpal tunnel syndrome: Diagnostic usefulness of sonography. Radiology 2004, 232, 93–99. [Google Scholar] [CrossRef]
- Wong, S.M.; Griffith, J.F.; Hui, A.C.; Tang, A.; Wong, K.S. Discriminatory sonographic criteria for the diagnosis of carpal tunnel syndrome. Arthritis Rheumatol. 2002, 46, 1914–1921. [Google Scholar] [CrossRef] [PubMed]
- Pinilla, I.; Martín-Hervas, C.; Sordo, G.; Santiago, S. The usefulness of ultrasonography in the diagnosis of carpal tunnel syndrome. J. Hand Surg. Eur. 2008, 33, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Sernik, R.A.; Abicalaf, C.A.; Pimentel, B.F.; Braga-Baiak, A.; Braga, L.; Cerri, G.G. Ultrasound features of carpal tunnel syndrome: A prospective caseecontrol study. Skeletal Radiol. 2008, 37, 49–53. [Google Scholar] [CrossRef]
- Akcar, N.; Ozkan, S.; Mehmetoglu, O.; Calisir, C.; Adapinar, B. Value of power Doppler and gray-scale US in the diagnosis of carpal tunnel syndrome: Contribution of cross-sectional area just before the tunnel inlet as compared with the cross-sectional area at the tunnel. Korean J. Radiol. 2010, 11, 632–639. [Google Scholar] [CrossRef] [Green Version]
- Moran, L.; Perez, M.; Esteban, A.; Bellon, J.; Arranz, B.; del Cerro, M. Sonographic measurement of crosssectional area of the median nerve in the diagnosis of carpal tunnel syndrome: Correlation with nerve conduction studies. J. Clin. Ultrasound 2009, 37, 125–131. [Google Scholar] [CrossRef]
- Leonard, L.; Rangan, A.; Doyle, G.; Taylor, G. Carpal tunnel syndromedis high frequency ultrasound a useful diagnostic tool? J. Hand Surg. Br. 2003, 28, 77–79. [Google Scholar] [CrossRef]
- Ng, A.W.H.; Griffith, J.F.; Lee, R.K.L.; Tse, W.L.; Wong, C.W.Y.; Ho, P.C. Ultrasound carpal tunnel syndrome: Additional criteria for diagnosis. Clin. Radiol 2018, 73, 214.e11–214.e18. [Google Scholar] [CrossRef]
- Seror, P. Sonography and electrodiagnosis in carpal tunnel syndrome diagnosis, an analysis of the literature. Eur. J. Radiol. 2008, 67, 146–152. [Google Scholar] [CrossRef]
- Billakota, S.; Hobson-Webb, L.D. Standard median nerve ultrasound in carpal tunnel syndrome: A retrospective review of 1021 cases. Clin. Neurophysiol. Pract. 2017, 2, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, A.R.; Jali, R.; Moghtaderi, A.R.; Yazdani, A.H. The diagnostic value of ultrasonography in patients with electrophysiologicaly confirmed carpal tunnel syndrome. Electromyogr. Clin. Neurophysiol. 2009, 49, 3–8. [Google Scholar]
- Kelle, H.; Verheggen, R.; Bittermann, H.J.; Reimers, C.D. The potential value of ultrasonography in the evaluation of carpal tunnel syndrome. Neurology 2003, 61, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Nakamichi, K.I.; Tachibana, S. Enlarged median nerve in idiopathic carpal tunnel syndrome. Muscle Nerve 2000, 23, 1713–1718. [Google Scholar] [CrossRef]
- Sarría, L.; Cabada, T.; Cozcolluela, R.; Martínez-Berganza, T.; García, S. Carpal tunnel syndrome: Usefulness of sonography. Eur. Radiol. 2000, 10, 1920–1925. [Google Scholar] [CrossRef] [PubMed]
- Fowler, J.R.; Gaughan, J.P.; Ilyas, A.M. The sensitivity and specificity of ultrasound for the diagnosis of carpal tunnel syndrome: A meta-analysis. Clin. Orthop. Relat. Res. 2011, 469, 1089–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Costoso, A.; Martínez-Vizcaíno, V.; Álvarez-Bueno, C.; Ferri-Morales, A.; Cavero-Redondo, I. Accuracy of Ultrasonography for the diagnosis of carpal tunnel syndrome: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2018, 99, 758–765. [Google Scholar] [CrossRef]
- Hobson-Webb, L.D.; Massey, J.M.; Juel, V.C.; Sanders, D.B. The ultrasonographic wrist-to-forearm median nerve area ratio in carpal tunnel syndrome. Clin. Neurophysiol. 2008, 119, 1353–1357. [Google Scholar] [CrossRef]
- Mitchell, R.; Chesney, A.; Seal, S.; Mc Knight, L.; Thoma, A. Anatomical variations of the carpal tunnel structures. Can. J. Plast. Surg. 2009, 17, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Presazzi, A.; Bortolotto, C.; Zacchino, M.; Madonia, L.; Draghi, F. Carpal tunnel: Normal anatomy, anatomical variants and ultrasound technique. J. Ultrasound 2011, 14, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Ettema, A.M.; Amadio, P.C.; Zhao, C.; Wold, L.E.; An, K.N. A histological and immunohistochemical study of the subsynovial connective tissue in idiopathic carpal tunnel syndrome. J. Bone Joint Surg. Am. 2004, 86, 1458–1466. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Zhao, C.; Zobitz, M.E.; Wold, L.E.; An, K.N.; Amadio, P.C. Morphological changes of collagen fibrils in the subsynovial connective tissue in carpal tunnel syndrome. J. Bone Joint Surg. Am. 2006, 88, 824–831. [Google Scholar] [PubMed]
- Osamura, N.; Zhao, C.; Zobitz, M.E.; An, K.N.; Amadio, P.C. Evaluation of the material properties of the subsynovial connective tissue in carpal tunnel syndrome. Clin. Biomech. 2007, 22, 999–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshii, Y.; Villarraga, H.R.; Henderson, J.; Zhao, C.; An, K.N.; Amadio, P.C. Ultrasound assessment of the displacement and deformation of the median nerve in the human carpal tunnel with active finger motion. J. Bone Joint Surg. Am. 2009, 91, 2922–2930. [Google Scholar] [CrossRef] [Green Version]
- Van Doesburg, M.H.; Henderson, J.; Yoshii, Y.; Mink van der Molen, A.B.; Cha, S.S.; An, K.N.; Amadio, P.C. Median nerve deformation in differential finger motions: Ultrasonographic comparison of carpal tunnel syndrome patients and healthy controls. J. Orthop. Res. 2012, 30, 643–648. [Google Scholar] [CrossRef]
- Yoshii, Y.; Ishii, T.; Tung, W.L.; Sakai, S.; Amadio, P.C. Median nerve deformation and displacement in the carpal tunnel during finger motion. J. Orthop. Res. 2013, 31, 1876–1880. [Google Scholar] [CrossRef]
- Yoshii, Y. Dynamic analysis of ultrasound image for the diagnosis of carpal tunnel syndrome. Kansetsugeka 2015, 34, 636–643. [Google Scholar]
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound Eeastography: Review of techniques and clinical applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef]
- Ophir, J.; Cespedes, I.; Ponnekanti, H.; Yazdi, T.; Li, X. Elastography: A quantitative method for imaging the elasticity of biological tissues. Ultrason. Imaging 1991, 2, 111–134. [Google Scholar] [CrossRef]
- Garra, B.S. Elastography: History, principles, and technique comparison. Abdom. Imaging 2015, 40, 680–697. [Google Scholar] [CrossRef]
- Carlsen, J.F.; Hansen, K.L.; Ewertsen, C.; Nielsen, M.B. Elastography in Breast Imaging. Ultraschall Med. 2019, 40, 688–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sporea, I.; Sirli, R.L. Hepatic elastography for the assessment of liver fibrosis–present and future. Ultraschall Med. 2012, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, M.; Fredberg, U.; Langberg, H. Sonoelastography as a diagnostic tool in the assessment of musculoskeletal alterations: A systematic review. Ultraschall Med. 2012, 33, 441–446. [Google Scholar] [CrossRef]
- Klauser, A.S.; Miyamoto, H.; Martinoli, C.; Tagliafico, A.S.; Szantkay, J.; Feuchtner, G.; Jaschke, W. Sonoelastographic findings of carpal tunnel injection. Ultraschall Med. 2015, 36, 618–622. [Google Scholar] [CrossRef]
- Ghajarzadeh, M.; Dadgostar, M.; Sarraf, P.; Emami-Razavi, S.Z.; Miri, S.; Malek, M. Application of ultrasound elastography for determining carpal tunnel syndrome severity. Jpn. J. Radiol. 2015, 33, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, H.; Halpern, E.J.; Kastlunger, M.; Gabl, M.; Arora, R.; Bellmann-Weiler, R.; Feuchtner, G.M.; Jaschke, W.R.; Klauser, A.S. Carpal tunnel syndrome: Diagnosis by means of median nerve elasticity-improved diagnostic accuracy of US with sonoelastography. Radiology 2014, 270, 481–486. [Google Scholar] [CrossRef]
- Yoshii, Y.; Ishii, T.; Tanaka, T.; Tung, W.L.; Sakai, S. Detecting median nerve strain changes with cyclic compression apparatus: A comparison of carpal tunnel syndrome patients and healthy controls. Ultrasound Med. Biol. 2015, 41, 669–674. [Google Scholar] [CrossRef]
- Liao, Y.Y.; Lee, W.N.; Lee, M.R.; Chen, W.S.; Chiou, H.J.; Kuo, T.T.; Yeh, C.K. Carpal tunnel syndrome: US strain imaging for diagnosis. Radiology 2015, 275, 205–214. [Google Scholar] [CrossRef]
- Kantarci, F.; Ustabasioglu, F.E.; Delil, S.; Olgun, D.C.; Korkmazer, B.; Dikici, A.S.; Tutar, O.; Nalbantoglu, M.; Uzun, N.; Mihmanli, I. Median nerve stiffness measurement by shear wave elastography: A potential sonographic method in the diagnosis of carpal tunnel syndrome. Eur. Radiol. 2014, 24, 434–440. [Google Scholar] [CrossRef]
- Zhang, C.; Li, M.; Jiang, J.; Zhou, Q.; Xiang, L.; Huang, Y.; Ban, W.; Peng, W. Diagnostic value of virtual touch tissue imaging quantification for evaluating median nerve stiffness in carpal tunnel syndrome. J. Ultrasound Med. 2017, 36, 1783–1791. [Google Scholar] [CrossRef]
- Paluch, L.; Pietruski, P.; Walecki, J.; Noszczyk, B.H. Wrist to forearm ratio as a median nerve shear wave elastography test in carpal tunnel syndrome diagnosis. J. Plast. Reconstr. Aesthet. Surg. 2018, 71, 1146–1152. [Google Scholar] [CrossRef] [PubMed]
- Orman, G.; Ozben, S.; Huseyinoglu, N.; Duymus, M.; Orman, K.G. Ultrasound elastographic evaluation in the diagnosis of carpal tunnel syndrome: Initial findings. Ultrasound Med. Biol. 2013, 39, 1184–1189. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.P.; Chen, I.J.; Chang, K.V.; Wu, W.T.; Özçakar, L. Utility of ultrasound elastography in evaluation of carpal tunnel syndrome: A systematic review and meta-analysis. Ultrasound Med. Biol. 2019, 45, 2855–2865. [Google Scholar] [CrossRef] [PubMed]
- Tatar, I.G.; Kurt, A.; Yavasoglu, N.G.; Hekimoglu, B. Carpal tunnel syndrome: Elastosonographic strain ratio and cross-sectional area evaluation for the diagnosis and disease severity. Med. Ultrasound 2016, 18, 305–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, M.J.; Cartwright, M.S. A pilot study of strain elastography in the diagnosis of carpal tunnel syndrome. J. Clin. Neurophysiol. 2017, 34, 114–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asadov, R.; Erdal, A.; Bugdayci, O.; Gunduz, O.H.; Ekinci, G. The effectiveness of ultrasonography and ultrasonographic elastography in the diagnosis of carpal tunnel syndrome and evaluation of treatment response after steroid injection. Eur. J. Radiol. 2018, 108, 172–176. [Google Scholar] [CrossRef]
- Yoshii, Y.; Tung, W.L.; Ishii, T. Measurement of Median Nerve Strain and Applied Pressure for the Diagnosis of Carpal Tunnel Syndrome. Ultrasound Med. Biol. 2017, 43, 1205–1209. [Google Scholar] [CrossRef]
- Cingoz, M.; Kandemirli, S.G.; Alis, D.C.; Samanci, C.; Kandemirli, G.C.; Adatepe, N.U. Evaluation of median nerve by shear wave elastography and diffusion tensor imaging in carpal tunnel syndrome. Eur. J. Radiol. 2018, 101, 59–64. [Google Scholar] [CrossRef]
- Kubo, K.; Zhou, B.; Cheng, Y.S.; Yang, T.H.; Qiang, B.; An, K.N.; Moran, S.L.; Amadio, P.C.; Zhang, X.; Zhao, C. Ultrasound elastography for carpal tunnel pressure measurement: A cadaveric validation study. J. Orthop. Res. 2018, 36, 477–483. [Google Scholar] [CrossRef]
- Cheng, Y.S.; Zhou, B.; Kubo, K.; An, K.N.; Moran, S.L.; Amadio, P.C.; Zhang, X.; Zhao, C. Comparison of two ways of altering carpal tunnel pressure with ultrasound surface wave elastography. J. Biomech. 2018, 74, 197–201. [Google Scholar] [CrossRef]
- Franchi-Abella, S.; Elie, C.; Correas, J.M. Ultrasound elastography: Advantages, limitations and artefacts of the different techniques from a study on a phantom. Diagn. Interv. Imaging 2013, 94, 497–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackinnon, S.E.; Dellon, A.L.; Hudson, A.R.; Hunter, D.A. Chronic nerve compression--an experimental model in the rat. Ann. Plast. Surg. 1984, 13, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Moharram, M.A.; Lamberts, R.R.; Whalley, G.; Williams, M.J.A.; Coffey, S. Myocardial tissue characterisation using echocardiographic deformation imaging. Cardiovasc. Ultrasound 2019, 17, 27. [Google Scholar] [CrossRef] [PubMed]
- Murtaza, G.; Virk, H.U.H.; Khalid, M.; Rahman, Z.; Sitwala, P.; Schoondyke, J.; Al-Balbissi, K. Role of speckle tracking echocardiography in dilated cardiomyopathy: A Review. Cureus 2017, 9, e1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muraru, D.; Niero, A.; Rodriguez-Zanella, H.; Cherata, D.; Badano, L. Three-dimensional speckle-tracking echocardiography: Benefits and limitations of integrating myocardial mechanics with three-dimensional imaging. Cardiovasc. Diagn. Ther. 2018, 8, 101–117. [Google Scholar] [CrossRef] [Green Version]
- Mondillo, S.; Galderisi, M.; Mele, D.; Cameli, M.; Lomoriello, V.S.; Zacà, V.; Ballo, P.; D’Andrea, A.; Muraru, D.; Losi, M.; et al. Speckle-tracking echocardiography: A new technique for assessing myocardial function. J. Ultrasound Med. 2011, 30, 71–83. [Google Scholar] [CrossRef]
- Blessberger, H.; Binder, T. NON-invasive imaging: Two dimensional speckle tracking echocardiography: Basic principles. Heart 2010, 96, 716–722. [Google Scholar] [CrossRef]
- Yoshii, Y.; Villarraga, H.R.; Henderson, J.; Zhao, C.; An, K.N.; Amadio, P.C. Speckle tracking ultrasound for assessment of the relative motion of flexor tendon and subsynovial connective tissue in the human carpal tunnel. Ultrasound Med. Biol. 2009, 35, 1973–1981. [Google Scholar] [CrossRef] [Green Version]
- Van Doesburg, M.H.; Yoshii, Y.; Henderson, J.; Villarraga, H.R.; Moran, S.L.; Amadio, P.C. Speckle-tracking sonographic assessment of longitudinal motion of the flexor tendon and subsynovial tissue in carpal tunnel syndrome. J. Ultrasound Med. 2012, 31, 1091–1098. [Google Scholar] [CrossRef] [Green Version]
- Chen, I.; Chang, K.; Lou, Y.; Wu, W.; Özçakar, L. Can ultrasound imaging be used for the diagnosis of carpal tunnel syndrome in diabetic patients? A systemic review and network meta-analysis. J. Neurol. 2020, 267, 1887–1895. [Google Scholar] [CrossRef]
- Takahashi, T.; Kato, A.; Ikegaya, N.; Takita, T.; Maruyama, Y.; Hishida, A.; Takahashi, M. Ultrasound changes of the carpal tunnel in patients receiving long-term hemodialysis: A cross-sectional and longitudinal study. Clin. Nephrol. 2002, 57, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Yoon, J.S.; Kim, S.J.; Won, S.J.; Jeong, J.S. Carpal tunnel syndrome: Clinical, electrophysiological, and ultrasonographic ratio after surgery. Muscle Nerve 2012, 45, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Kapuścińska, K.; Urbanik, A. Efficacy of high frequency ultrasound in postoperative evaluation of carpal tunnel syndrome treatment. J. Ultrason. 2016, 16, 16–24. [Google Scholar] [CrossRef]
- Yoshii, Y.; Tung, W.L.; Yuine, H.; Ishii, T. Postoperative diagnostic potentials of median nerve strain and applied pressure measurement after carpal tunnel release. BMC Musculoskelet. Disord. 2020, 21, 22. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshii, Y.; Zhao, C.; Amadio, P.C. Recent Advances in Ultrasound Diagnosis of Carpal Tunnel Syndrome. Diagnostics 2020, 10, 596. https://doi.org/10.3390/diagnostics10080596
Yoshii Y, Zhao C, Amadio PC. Recent Advances in Ultrasound Diagnosis of Carpal Tunnel Syndrome. Diagnostics. 2020; 10(8):596. https://doi.org/10.3390/diagnostics10080596
Chicago/Turabian StyleYoshii, Yuichi, Chunfeng Zhao, and Peter C. Amadio. 2020. "Recent Advances in Ultrasound Diagnosis of Carpal Tunnel Syndrome" Diagnostics 10, no. 8: 596. https://doi.org/10.3390/diagnostics10080596