Site-Of-Care Viscoelastic Assay in Major Trauma Improves Outcomes and Is Cost Neutral Compared with Standard Coagulation Tests

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
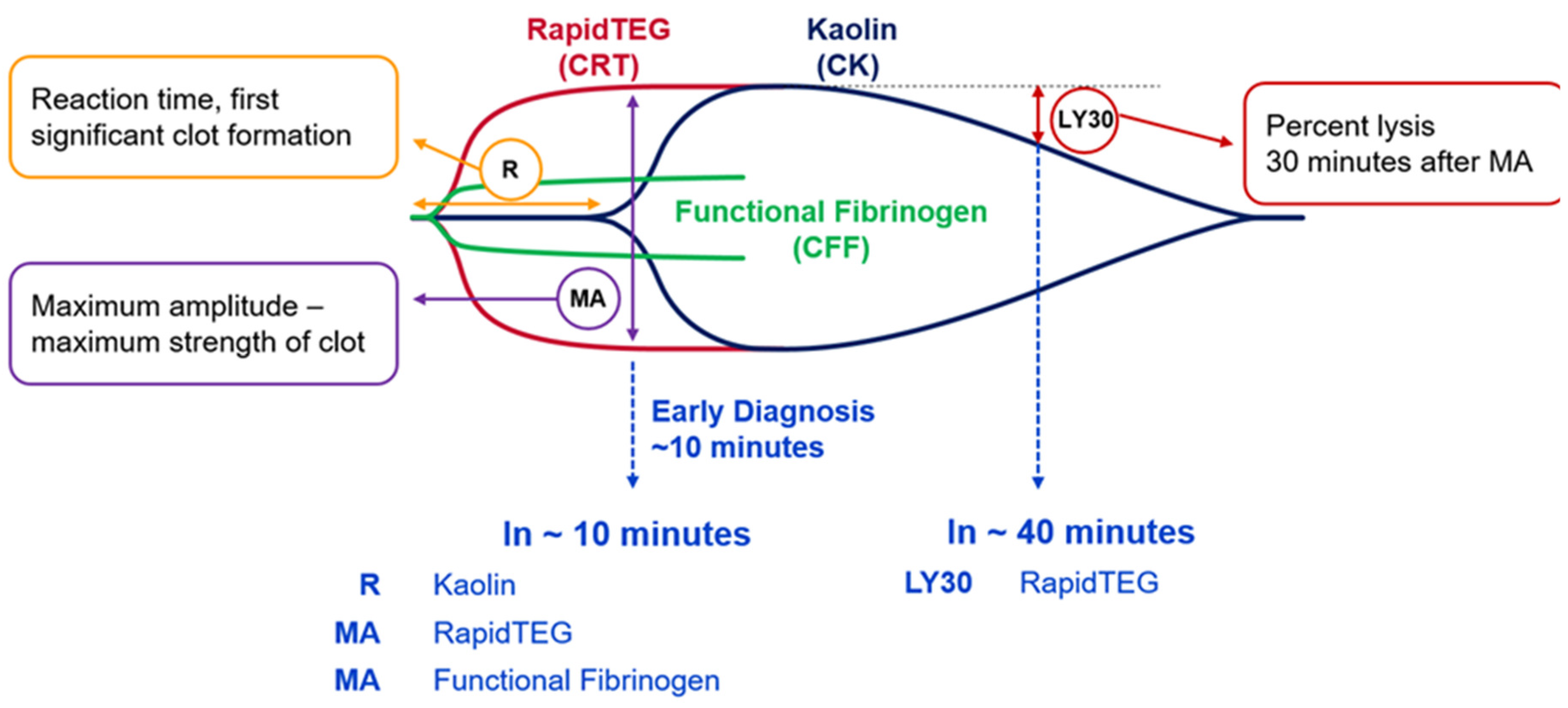
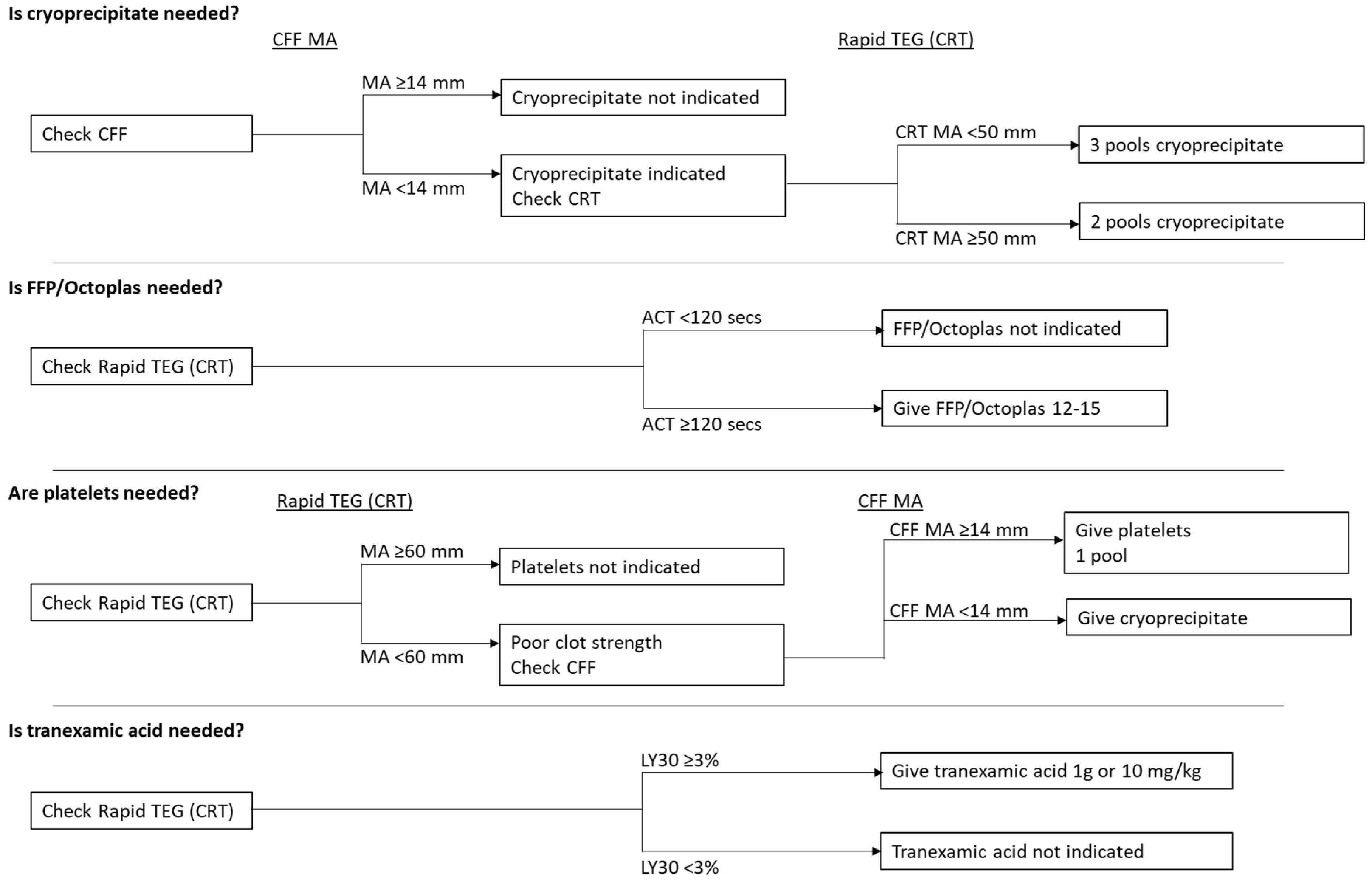
2.2. Thromboelastography
2.3. Massive Transfusion Protocol (MTP)
2.4. Pre-TEG Group
2.5. Post-TEG Group
2.6. Economic Analysis
2.7. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Mortality
3.3. Blood Product Usage
3.4. Cost Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brohi, K.; Cohen, M.J.; Davenport, R.A. Acute coagulopathy of trauma: Mechanism, identification and effect. Curr. Opin. Crit. Care 2007, 13, 680–685. [Google Scholar] [CrossRef]
- Brohi, K.; Cohen, M.J.; Ganter, M.T.; Schultz, M.J.; Levi, M.; Mackersie, R.C.; Pittet, J.F. Acute coagulopathy of trauma: Hypoperfusion induces systemic anticoagulation and hyperfibrinolysis. J. Trauma 2008, 64, 1211–1217. [Google Scholar] [CrossRef] [Green Version]
- Schochl, H.; Nienaber, U.; Hofer, G.; Voelckel, W.; Jambor, C.; Scharbert, G.; Kozek-Langenecker, S.; Solomon, C. Goal-directed coagulation management of major trauma patients using thromboelastometry (ROTEM)-guided administration of fibrinogen concentrate and prothrombin complex concentrate. Crit. Care 2010, 14, R55. [Google Scholar] [CrossRef] [Green Version]
- Holcomb, J.B.; del Junco, D.J.; Fox, E.E.; Wade, C.E.; Cohen, M.J.; Schreiber, M.A.; Alarcon, L.H.; Bai, Y.; Brasel, K.J.; Bulger, E.M.; et al. The prospective, observational, multicenter, major trauma transfusion (PROMMTT) study: Comparative effectiveness of a time-varying treatment with competing risks. JAMA Surg. 2013, 148, 127–136. [Google Scholar] [CrossRef]
- Holcomb, J.B.; Tilley, B.C.; Baraniuk, S.; Fox, E.E.; Wade, C.E.; Podbielski, J.M.; del Junco, D.J.; Brasel, K.J.; Bulger, E.M.; Callcut, R.A.; et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: The PROPPR randomized clinical trial. JAMA 2015, 313, 471–482. [Google Scholar] [CrossRef]
- Stainsby, D.; MacLennan, S.; Thomas, D.; Isaac, J.; Hamilton, P.J.; British Committee for Standards in Haematology. Guidelines on the management of massive blood loss. Br. J. Haematol. 2006, 135, 634–641. [Google Scholar] [CrossRef] [Green Version]
- Spahn, D.R.; Bouillon, B.; Cerny, V.; Duranteau, J.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Maegele, M.; Nardi, G.; Riddez, L.; et al. The European guideline on management of major bleeding and coagulopathy following trauma: Fifth edition. Crit. Care 2019, 23, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanworth, S.J.; Hyde, C.J.; Murphy, M.F. Evidence for indications of fresh frozen plasma. Transfus. Clin. Biol. 2007, 14, 551–556. [Google Scholar] [CrossRef]
- ACS TQIP Massive Transfusion in Trauma Guidelines. Available online: https://www.facs.org/-/media/files/quality-programs/trauma/tqip/transfusion_guildelines.ashx (accessed on 13 July 2020).
- Roullet, S.; de Maistre, E.; Ickx, B.; Blais, N.; Susen, S.; Faraoni, D.; Garrigue, D.; Bonhomme, F.; Godier, A.; Lasne, D.; et al. Position of the French Working Group on Perioperative Haemostasis (GIHP) on viscoelastic tests: What role for which indication in bleeding situations? Anaesth. Crit. Care Pain Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Davenport, R. Pathogenesis of acute traumatic coagulopathy. Transfusion 2013, 53, 23S–27S. [Google Scholar] [CrossRef] [PubMed]
- Di Benedetto, P.; Baciarello, M.; Cabetti, L.; Martucci, M.; Chiaschi, A.; Bertini, L. Thrombelastography. Present and future perspectives in clinical practice. Minerva Anestesiol. 2003, 69, 501–515. [Google Scholar] [PubMed]
- Dzik, W.H. Predicting hemorrhage using preoperative coagulation screening assays. Curr. Hematol. Rep. 2004, 3, 324–330. [Google Scholar] [PubMed]
- Enriquez, L.J.; Shore-Lesserson, L. Point-of-care coagulation testing and transfusion algorithms. Br. J. Anaesth. 2009, 103, i14–i22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Essell, J.H.; Martin, T.J.; Salinas, J.; Thompson, J.M.; Smith, V.C. Comparison of thromboelastography to bleeding time and standard coagulation tests in patients after cardiopulmonary bypass. J. Cardiothorac. Vasc. Anesth. 1993, 7, 410–415. [Google Scholar] [CrossRef]
- Levrat, A.; Gros, A.; Rugeri, L.; Inaba, K.; Floccard, B.; Negrier, C.; David, J.S. Evaluation of rotation thrombelastography for the diagnosis of hyperfibrinolysis in trauma patients. Br. J. Anaesth. 2008, 100, 792–797. [Google Scholar] [CrossRef] [Green Version]
- Rugeri, L.; Levrat, A.; David, J.S.; Delecroix, E.; Floccard, B.; Gros, A.; Allaouchiche, B.; Negrier, C. Diagnosis of early coagulation abnormalities in trauma patients by rotation thrombelastography. J. Thromb. Haemost. 2007, 5, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Spahn, D.R.; Rossaint, R. Coagulopathy and blood component transfusion in trauma. Br. J. Anaesth. 2005, 95, 130–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, J.N.; Burke, P.A.; Agarwal, S.K.; Mantilla-Rey, N.; Quillen, K. A massive transfusion protocol incorporating a higher FFP/RBC ratio is associated with decreased use of recombinant activated factor VII in trauma patients. Am. J. Clin. Pathol. 2012, 137, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, J.; Walsh, M.; Grisoli, A.; Thomas, A.V.; Shariff, F.; McCauley, R.; Vande Lune, S.; Zackariya, N.; Patel, S.; Farrell, M.S.; et al. Diagnosis and treatment of trauma-induced coagulopathy by viscoelastography. Semin. Thromb. Hemost. 2020, 46, 134–146. [Google Scholar] [CrossRef]
- Gonzalez, E.; Moore, E.E.; Moore, H.B.; Chapman, M.P.; Chin, T.L.; Ghasabyan, A.; Wohlauer, M.V.; Barnett, C.C.; Bensard, D.D.; Biffl, W.L.; et al. Goal-directed hemostatic resuscitation of trauma-induced coagulopathy: A pragmatic randomized clinical trial comparing a viscoelastic assay to conventional coagulation assays. Ann. Surg. 2016, 263, 1051–1059. [Google Scholar] [CrossRef]
- Kaufmann, C.R.; Dwyer, K.M.; Crews, J.D.; Dols, S.J.; Trask, A.L. Usefulness of thrombelastography in assessment of trauma patient coagulation. J. Trauma 1997, 42, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, A.J.; Wade, C.E.; Jenkins, D.H.; Smith, K.A.; Noe, J.C.; Park, M.S.; Perkins, J.G.; Holcomb, J.B. A reduction in clot formation rate and strength assessed by thrombelastography is indicative of transfusion requirements in patients with penetrating injuries. J. Trauma 2008, 64, S64–S68. [Google Scholar] [CrossRef]
- Tapia, N.M.; Chang, A.; Norman, M.; Welsh, F.; Scott, B.; Wall, M.J., Jr.; Mattox, K.L.; Suliburk, J. TEG-guided resuscitation is superior to standardized MTP resuscitation in massively transfused penetrating trauma patients. J. Trauma Acute Care Surg. 2013, 74, 378–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurbel, P.A.; Bliden, K.P.; Tantry, U.S.; Monroe, A.L.; Muresan, A.A.; Brunner, N.E.; Lopez-Espina, C.G.; Delmenico, P.R.; Cohen, E.; Raviv, G.; et al. First report of the point-of-care TEG: A technical validation study of the TEG-6S system. Platelets 2016, 27, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Neal, M.D.; Moore, E.E.; Walsh, M.; Thomas, S.; Callcut, R.A.; Kornblith, L.Z.; Schreiber, M.; Ekeh, A.P.; Singer, A.J.; Lottenberg, L.; et al. A comparison between the TEG 6s and TEG 5000 analyzers to assess coagulation in trauma patients. J. Trauma Acute Care Surg. 2020, 88, 279–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, I.; Shakur, H.; Coats, T.; Hunt, B.; Balogun, E.; Barnetson, L.; Cook, L.; Kawahara, T.; Perel, P.; Prieto-Merino, D.; et al. The CRASH-2 trial: A randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol. Assess. 2013, 17, 1–79. [Google Scholar] [CrossRef]
- Bakaas-Aasen, K.; Van Dieren, S.; Balvers, K.; Juffermans, N.P.; Næss, P.A.; Rourke, C.; Eaglestone, S.; Ostrowski, S.R.; Stensballe, J.; Stanwoeth, S.; et al. Data-driven development of ROTEM and TEG algorithms for the management of trauma hemorrhage: A prospective observational multicenter study. Ann. Surg. 2019, 270, 1178–1185. [Google Scholar] [CrossRef]
- Whiting, D.; DiNardo, J.A. TEG and ROTEM: Technology and clinical applications. Am. J. Hematol. 2014, 89, 228–232. [Google Scholar] [CrossRef]
- Da Luz, L.T.; Nascimento, B.; Rizoli, S. Thrombelastography (TEG(R)): Practical considerations on its clinical use in trauma resuscitation. Scand. J. Trauma Resusc. Emerg. Med. 2013, 21, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doran, C.M.; Woolley, T.; Midwinter, M.J. Feasibility of using rotational thromboelastometry to assess coagulation status of combat casualties in a deployed setting. J. Trauma 2010, 69, S40–S48. [Google Scholar] [CrossRef]
- Perry, D.J.; Fitzmaurice, D.A.; Kitchen, S.; Mackie, I.J.; Mallett, S. Point-of-care testing in haemostasis. Br. J. Haematol. 2010, 150, 501–514. [Google Scholar] [CrossRef] [PubMed]
- Branco, B.C.; Inaba, K.; Ives, C.; Okoye, O.; Shulman, I.; David, J.S.; Schochl, H.; Rhee, P.; Demetriades, D. Thromboelastogram evaluation of the impact of hypercoagulability in trauma patients. Shock 2014, 41, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Da Luz, L.T.; Nascimento, B.; Shankarakutty, A.K.; Rizoli, S.; Adhikari, N.K. Effect of thromboelastography (TEG(R)) and rotational thromboelastometry (ROTEM(R)) on diagnosis of coagulopathy, transfusion guidance and mortality in trauma: Descriptive systematic review. Crit. Care 2014, 18, 518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashuk, J.L.; Moore, E.E.; Wohlauer, M.; Johnson, J.L.; Pezold, M.; Lawrence, J.; Biffl, W.L.; Burlew, C.C.; Barnett, C.; Sawyer, M.; et al. Initial experiences with point-of-care rapid thrombelastography for management of life-threatening postinjury coagulopathy. Transfusion 2012, 52, 23–33. [Google Scholar] [CrossRef]
- Kunio, N.R.; Differding, J.A.; Watson, K.M.; Stucke, R.S.; Schreiber, M.A. Thrombelastography-identified coagulopathy is associated with increased morbidity and mortality after traumatic brain injury. Am. J. Surg. 2012, 203, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Schochl, H.; Nienaber, U.; Maegele, M.; Hochleitner, G.; Primavesi, F.; Steitz, B.; Arndt, C.; Hanke, A.; Voelckel, W.; Solomon, C. Transfusion in trauma: Thromboelastometry-guided coagulation factor concentrate-based therapy versus standard fresh frozen plasma-based therapy. Crit. Care 2011, 15, R83. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, J.; Murphy, M.; Dias, J.D. Viscoelastic hemostatic assays: Moving from the laboratory to the site of care—A review of established and emerging technologies. Diagnostics 2020, 10, 118. [Google Scholar] [CrossRef] [Green Version]
- Kashuk, J.L.; Moore, E.E.; Le, T.; Lawrence, J.; Pezold, M.; Johnson, J.L.; Cothren, C.C.; Biffl, W.L.; Barnett, C.; Sabel, A. Noncitrated whole blood is optimal for evaluation of postinjury coagulopathy with point-of-care rapid thrombelastography. J. Surg. Res. 2009, 156, 133–138. [Google Scholar] [CrossRef]
- Davenport, R.; Manson, J.; De’Ath, H.; Platton, S.; Coates, A.; Allard, S.; Hart, D.; Pearse, R.; Pasi, K.J.; MacCallum, P.; et al. Functional definition and characterization of acute traumatic coagulopathy. Crit. Care Med. 2011, 39, 2652–2658. [Google Scholar] [CrossRef] [Green Version]
- Schochl, H.; Cotton, B.; Inaba, K.; Nienaber, U.; Fischer, H.; Voelckel, W.; Solomon, C. FIBTEM provides early prediction of massive transfusion in trauma. Crit. Care 2011, 15, R265. [Google Scholar] [CrossRef] [Green Version]
- Wohlauer, M.V.; Moore, E.E.; Thomas, S.; Sauaia, A.; Evans, E.; Harr, J.; Silliman, C.C.; Ploplis, V.; Castellino, F.J.; Walsh, M. Early platelet dysfunction: An unrecognized role in the acute coagulopathy of trauma. J. Am. Coll. Surg. 2012, 214, 739–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nekludov, M.; Bellander, B.M.; Blomback, M.; Wallen, H.N. Platelet dysfunction in patients with severe traumatic brain injury. J. Neurotrauma 2007, 24, 1699–1706. [Google Scholar] [CrossRef] [PubMed]
- Woolley, T.; Midwinter, M.; Spencer, P.; Watts, S.; Doran, C.; Kirkman, E. Utility of interim ROTEM(R) values of clot strength, A5 and A10, in predicting final assessment of coagulation status in severely injured battle patients. Injury 2013, 44, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Solomon, C.; Traintinger, S.; Ziegler, B.; Hanke, A.; Rahe-Meyer, N.; Voelckel, W.; Schochl, H. Platelet function following trauma. A multiple electrode aggregometry study. Thromb. Haemost. 2011, 106, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.; Al, M.; Westwood, M.; Ramos, I.C.; Ryder, S.; Armstrong, N.; Misso, K.; Ross, J.; Severens, J.; Kleijnen, J. Viscoelastic point-of-care testing to assist with the diagnosis, management and monitoring of haemostasis: A systematic review and cost-effectiveness analysis. Health Technol. Assess. 2015, 19, 1–228, v–vi. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Outcome | Category | Pre-TEG (n = 126) | Post-TEG (n = 175) | p-Value |
|---|---|---|---|---|
| Age | - | 47.2 ± 23.6 | 43.1 ± 20.2 | 0.11 |
| Sex | Male | 84 (67%) | 137 (78%) | 0.02 |
| Female | 42 (33%) | 38 (22%) | ||
| Shock index | - | 0.87 [0.69, 1.08] | 0.82 [0.65, 1.10] | 0.78 |
| GCS | - | 15 [8, 15] | 14 [8, 15] | 0.37 |
| Injury severity score | - | 25 [13, 33] | 22 [13, 34] | 0.75 |
| Mechanism of injury | Blunt | 107 (85%) | 149 (85%) | 0.96 |
| Penetrating | 19 (15%) | 26 (15%) | ||
| Injury site 1 | Head | 39 (35%) | 54 (31%) | 0.54 |
| Chest | 61 (54%) | 95 (55%) | 0.92 | |
| Abdominal | 42 (37%) | 71 (41%) | 0.54 | |
| Pelvis | 28 (25%) | 33 (19%) | 0.24 | |
| MSK | 65 (58%) | 103 (59%) | 0.78 | |
| Lactate | - | 3.4 [2.4, 5.6] | 3.0 [1.9, 4.5] | 0.06 |
| TEG cartridges | - | - | 1.8 ± 1.4 | - |
| TEG cartridges | 1 | - | 107 (61%) | - |
| (categorical) | 2 | - | 35 (20%) | |
| 3 | - | 17 (10%) | ||
| 4+ | - | 16 (9%) |
| Outcome | Pre-TEG (n = 126) | Post-TEG (n = 175) | p-Value |
|---|---|---|---|
| Total hospital LOS | 9 [3, 19] | 14 [6, 27] | <0.001 |
| 24 h mortality | 17 (13%) | 8 (5%) | 0.006 |
| 30 day mortality | 32 (25%) | 20 (11%) | 0.002 |
| Outcome | Pre-TEG (n = 126) | Post-TEG (n = 175) | p-Value |
|---|---|---|---|
| Units transfused | |||
| RBC | 3.6 ± 3.3 | 3.9 ± 4.0 | 0.91 |
| FFP/Octaplas | 2.5 ± 3.4 | 2.6 ± 3.8 | 0.98 |
| Platelets | 0.2 ± 0.5 | 0.4 ± 0.8 | 0.05 |
| Cryoprecipitate | 0.3 ± 1.0 | 0.5 ± 1.1 | 0.14 |
| All products combined | 6.7 ± 7.5 | 7.5 ± 8.8 | 0.94 |
| Any transfusion | 108 (86%) | 136 (78%) | 0.08 |
| Massive transfusion 1 | 4 (3%) | 14 (8%) | 0.08 |
| Massive transfusion 2 | 27 (21%) | 41 (23%) | 0.68 |
| Outcome | Pre-TEG (n = 126) | Post-TEG (n = 129) | p-Value |
| Units wasted | |||
| RBC | 0.2 ± 0.7 | 0.1 ± 0.5 | 0.02 |
| FFP/Octaplas | 1.6 ± 2.0 | 0.9 ± 1.8 | 0.004 |
| Platelets | 0.0 ± 0.1 | 0.0 ± 0.1 | 0.58 |
| Cryoprecipitate | 0.0 ± 0.3 | 0.1 ± 0.5 | 0.10 |
| All products combined | 1.8 ± 2.1 | 1.1 ± 2.0 | 0.002 |
| Outcome | Pre-TEG Mean ± SD (n = 126) | Post-TEG Mean ± SD (n = 175) | Difference 1 Mean (95% CI) | p-Value |
|---|---|---|---|---|
| Units transfused | ||||
| RBC | 432 ± 401 | 472 ± 480 | 40 (−54, 133) | 0.42 |
| FFP/Octaplas | 142 ± 196 | 111 ± 191 | −30 (−67, 17) | 0.18 |
| Platelets | 41 ± 90 | 79 ± 152 | 38 (10, 68) | 0.008 |
| Cryoprecipitate | 10 ± 32 | 15 ± 36 | 5 (−3, 11) | 0.24 |
| All products combined | 625 ± 655 | 678 ± 786 | 53 (−91, 227) | 0.52 |
| TEG cartridges | - | 74 ± 59 | - | |
| Total cost 1 2 | 625 ± 655 | 753 ± 828 | 127 (−22, 308) | 0.14 |
| Units wasted | ||||
| RBC | 26 ± 80 | 10 ± 60 | −15 (−33, 1) | 0.07 |
| FFP/Octaplas | 99 ± 128 | 57 ± 112 | −42 (−69, −14) | 0.004 |
| Platelets | 2 ± 17 | 3 ± 24 | 1 (−3, 7) | 0.57 |
| Cryoprecipitate | 1 ± 8 | 3 ± 14 | 2 (0, 5) | 0.09 |
| All products combined | 127 ± 146 | 74 ± 133 | −53 (−91, −17) | 0.002 |
| Total cost 2 3 | 753 ± 651 | 830 ± 847 | 78 (−88, 304) | 0.41 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cochrane, C.; Chinna, S.; Um, J.Y.; Dias, J.D.; Hartmann, J.; Bradley, J.; Brooks, A. Site-Of-Care Viscoelastic Assay in Major Trauma Improves Outcomes and Is Cost Neutral Compared with Standard Coagulation Tests. Diagnostics 2020, 10, 486. https://doi.org/10.3390/diagnostics10070486
Cochrane C, Chinna S, Um JY, Dias JD, Hartmann J, Bradley J, Brooks A. Site-Of-Care Viscoelastic Assay in Major Trauma Improves Outcomes and Is Cost Neutral Compared with Standard Coagulation Tests. Diagnostics. 2020; 10(7):486. https://doi.org/10.3390/diagnostics10070486
Chicago/Turabian StyleCochrane, Catriona, Shalini Chinna, Ju Young Um, Joao D. Dias, Jan Hartmann, Jim Bradley, and Adam Brooks. 2020. "Site-Of-Care Viscoelastic Assay in Major Trauma Improves Outcomes and Is Cost Neutral Compared with Standard Coagulation Tests" Diagnostics 10, no. 7: 486. https://doi.org/10.3390/diagnostics10070486