Proteomics-Based Identification of Diagnostic Biomarkers Related to Risk Factors and Pathogenesis of Ischemic Stroke

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Identification and Quantification of Serum Proteins
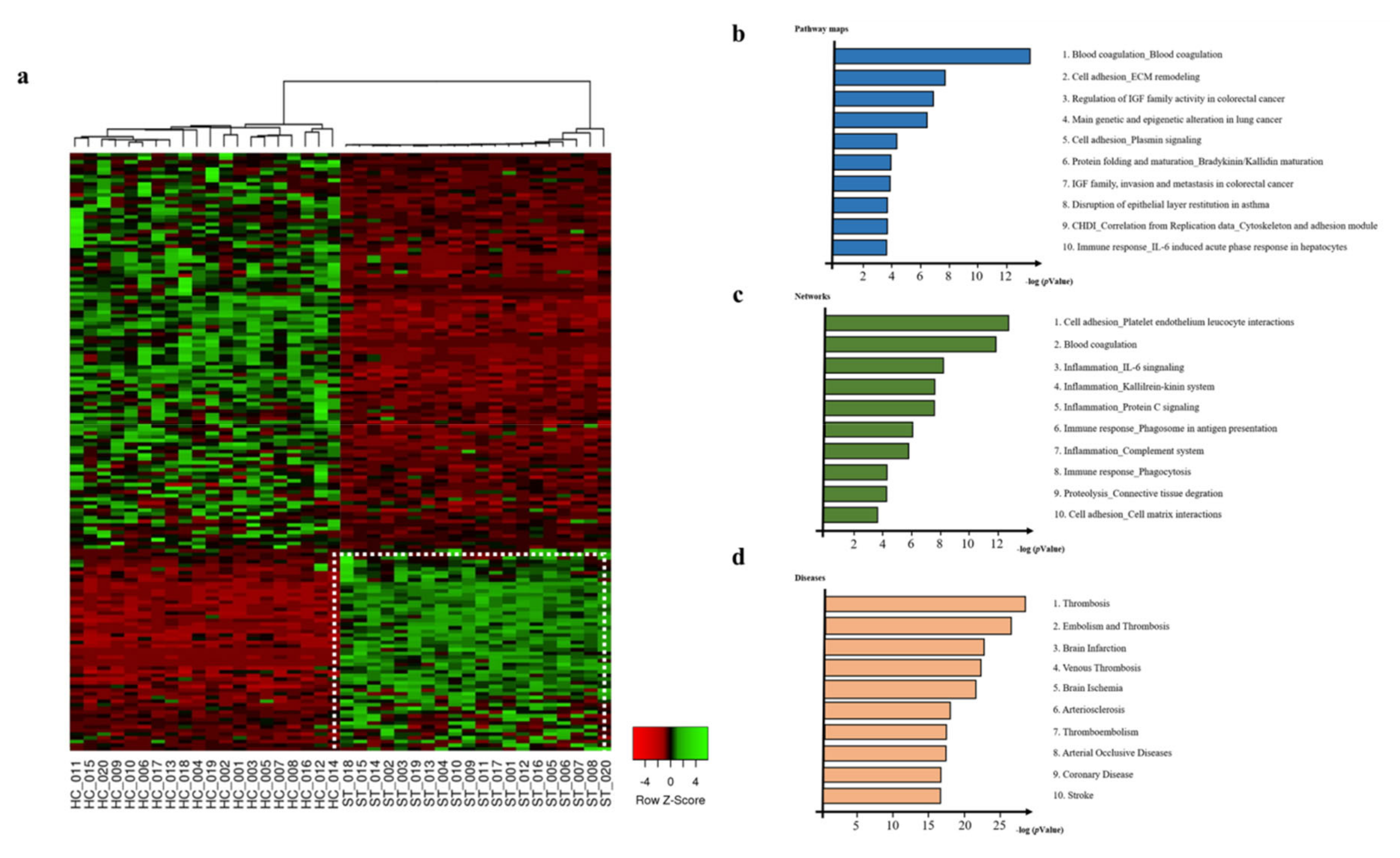
2.2. Differentially Expressed Proteins in Serum Proteins from Healthy Control and Ischemic Stroke Patients
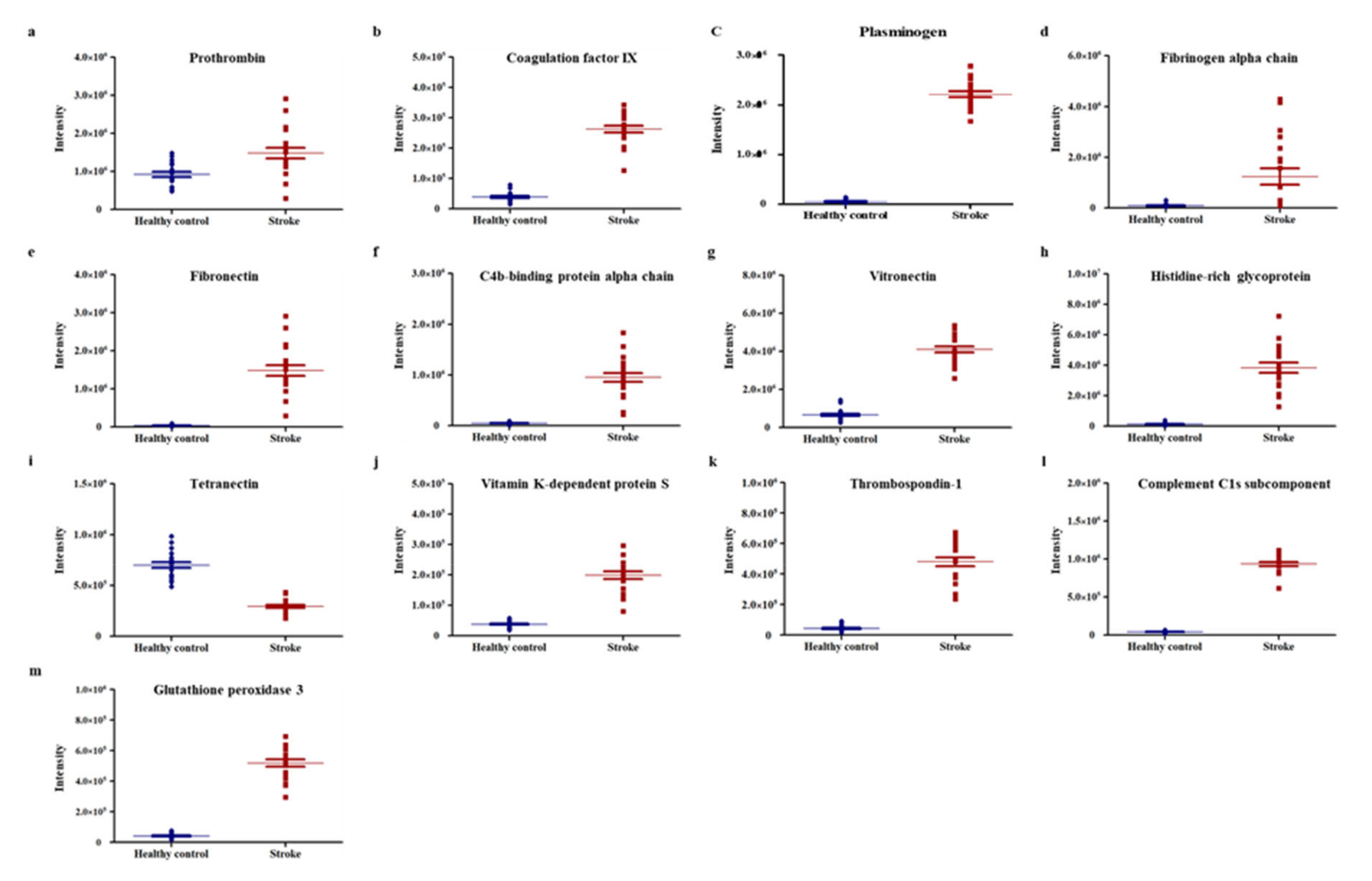
2.3. Selection of Potential Biomarker Candidates
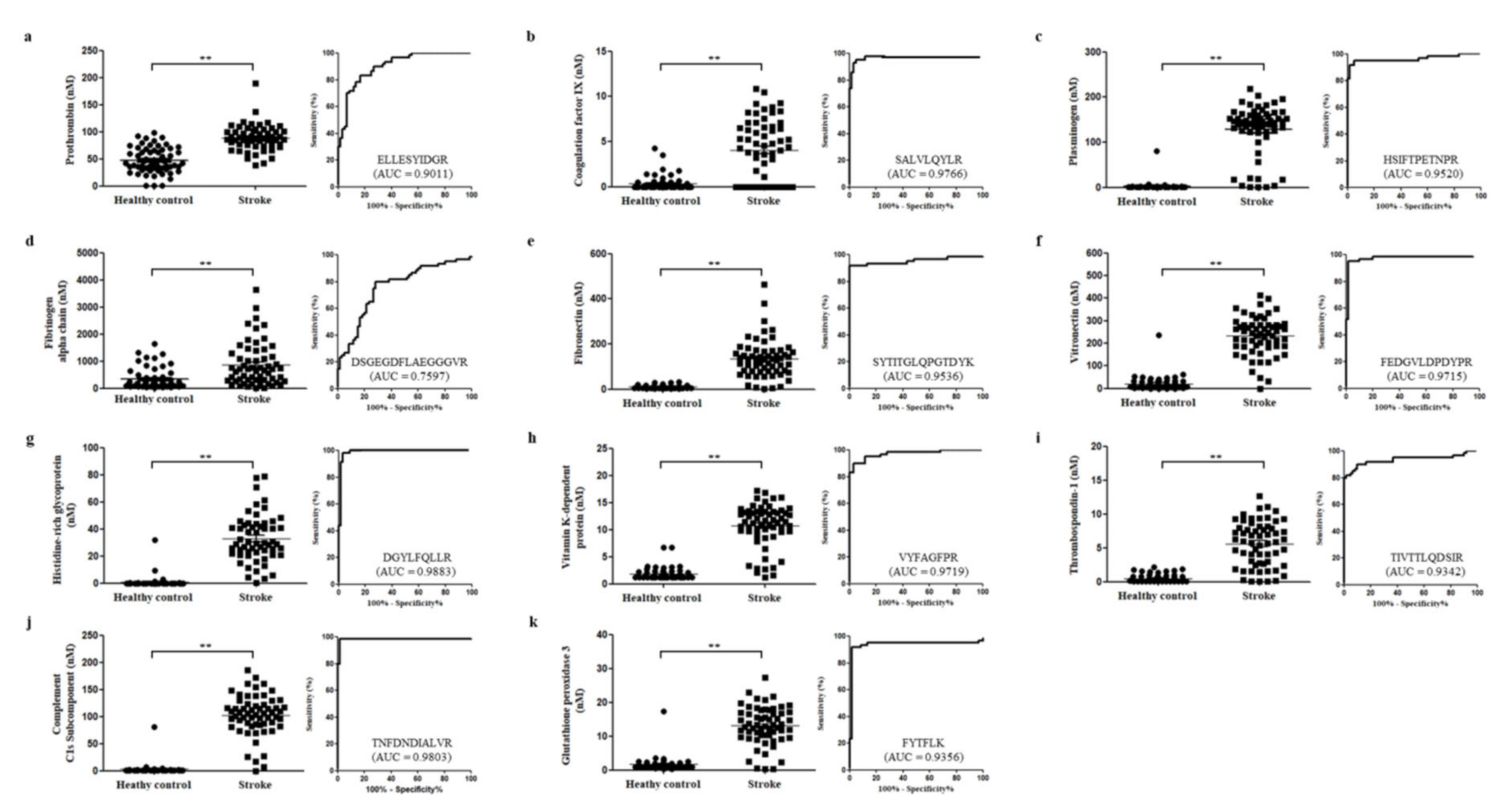
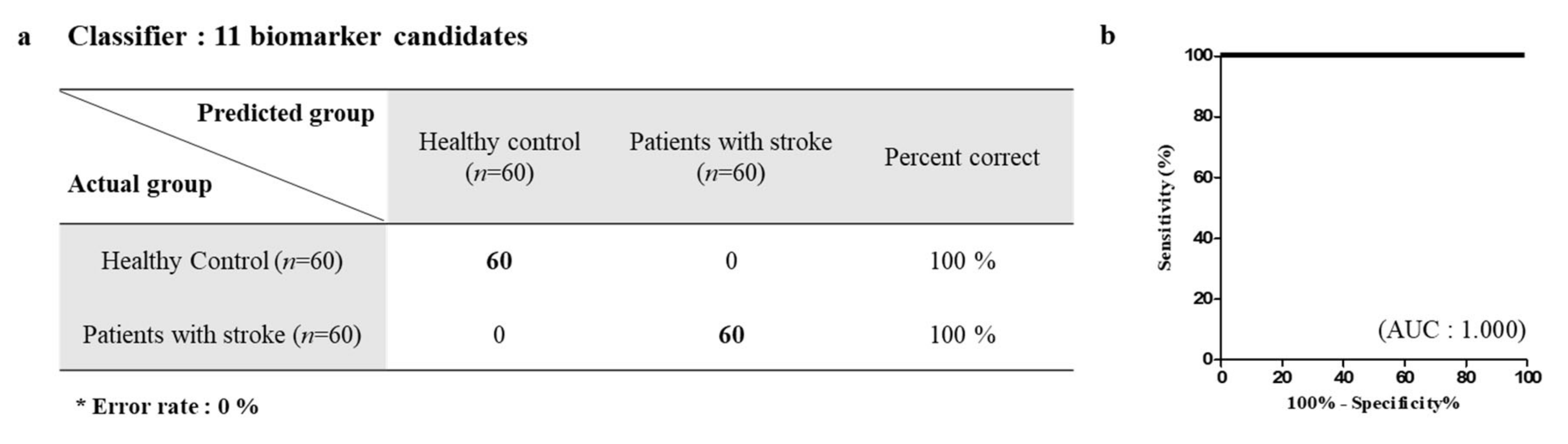
2.4. MRM Verification of Candidate Marker Proteins
2.5. Relationship of Candidate Marker and Ischemic Stroke Risk Factors/Ischemic Stroke Pathogenesis
3. Discussion
4. Materials and Methods
4.1. Participants and Serum Collection
4.2. Sample Preparation
4.3. HPLC-Triple 5600 Mass Spectrometry
4.4. Data-Dependent Analysis and SWATH Analysis
4.5. Database Exploration and Statistical Analysis
4.6. Multiple Reaction Monitoring Using Triple Quadrupole Mass Spectrometry
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Feigin, V.L.; Lawes, C.M.; Bennett, D.A.; Barker-Collo, S.L.; Parag, V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: A systematic review. Lancet Neurol. 2009, 8, 355–369. [Google Scholar] [CrossRef]
- Willmot, M.; Leonardi-Bee, J.; Bath, P.M. High blood pressure in acute stroke and subsequent outcome: A systematic review. Hypertension 2004, 43, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Ovbiagele, B.; Feng, W. Diabetes and stroke: Epidemiology, pathophysiology, pharmaceuticals and outcomes. Am. J. Med. Sci. 2016, 351, 380–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.P.; Fullerton, H.J. Heart disease and stroke statistics-2016 update a report from the American Heart Association. Circulation 2016, 133, e38–e48. [Google Scholar] [PubMed]
- Sporns, P.B.; Hanning, U.; Schwindt, W.; Velasco, A.; Minnerup, J.; Zoubi, T.; Heindel, W.; Jeibmann, A.; Niederstadt, T.U. Ischemic stroke: What does the histological composition tell us about the origin of the thrombus? Stroke 2017, 48, 2206–2210. [Google Scholar] [CrossRef] [PubMed]
- Fuentes-Arderiu, X. What is a biomarker? It’s time for a renewed definition. Clin. Chem. Lab. Med. 2013, 51, 1689–1690. [Google Scholar] [CrossRef] [PubMed]
- Rifai, N.; Gillette, M.A.; Carr, S.A. Protein biomarker discovery and validation: The long and uncertain path to clinical utility. Nat. Biotechnol. 2006, 24, 971. [Google Scholar] [CrossRef]
- Moulder, R.; Goo, Y.A.; Goodlett, D.R. Label-free quantitation for clinical proteomics. Methods Mol. Biol. 2016, 1410, 65–76. [Google Scholar]
- Finnerty, C.C.; Jeschke, M.G.; Qian, W.-J.; Kaushal, A.; Xiao, W.; Liu, T.; Gritsenko, M.A.; Moore, R.J.; Camp, D.G. Determination of burn patient outcome by large-scale quantitative discovery proteomics. Crit. Care Med. 2013, 41, 1421. [Google Scholar] [CrossRef] [Green Version]
- Gustafsson, C.; Blombäck, M.; Britton, M.; Hamsten, A.; Svensson, J. Coagulation factors and the increased risk of stroke in nonvalvular atrial fibrillation. Stroke 1990, 21, 47–51. [Google Scholar] [CrossRef] [Green Version]
- Krishnaswamy, S. The transition of prothrombin to thrombin. J. Thromb. Haemost. 2013, 11, 265–276. [Google Scholar] [CrossRef] [Green Version]
- Di Scipio, R.G.; Hermodson, M.A.; Yates, S.G.; Davie, E.W. A comparison of human prothrombin, factor IX (Christmas factor), factor X (Stuart factor), and protein S. Biochemistry 1977, 16, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Lisman, T.; Weeterings, C.; de Groot, P.G. Platelet aggregation: Involvement of thrombin and fibrin (ogen). Front. Biosci. 2005, 10, 2504–2517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ercan, B.; Tamer, L.; Sucu, N.; Pekdemir, H.; Çamsarı, A.; Atik, U. Factor VLeiden and prothrombin G20210A gene polymorphisms in patients with coronary artery disease. Yonsei Med. J. 2008, 49, 237–243. [Google Scholar] [CrossRef] [Green Version]
- Hendy, O.M.; Al Moneam, E.A.; Allam, M.; Soliman, S.; Kamal, A.; El Nasser, G.A. Frequency of thrombotic gene mutations in diabetic patients with and without coronary artery disease. Med. J. Cairo Univ. 2011, 79, 197–204. [Google Scholar]
- Kim, J.-A.; Kim, J.-E.; Song, S.H.; Kim, H.K. Influence of blood lipids on global coagulation test results. Ann. Lab. Med. 2015, 35, 15–21. [Google Scholar] [CrossRef]
- Di Napoli, M.; Singh, P. Is plasma fibrinogen useful in evaluating ischemic stroke patients? Why, how, and when. Stroke 2009, 40, 1549–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoshnam, S.E.; Winlow, W.; Farzaneh, M.; Farbood, Y.; Moghaddam, H.F. Pathogenic mechanisms following ischemic stroke. Neurol. Sci. 2017, 38, 1167–1186. [Google Scholar] [CrossRef] [PubMed]
- Jickling, G.C.; Liu, D.; Ander, B.P.; Stamova, B.; Zhan, X.; Sharp, F.R. Targeting neutrophils in ischemic stroke: Translational insights from experimental studies. J. Cereb. Blood Flow Metab. 2015, 35, 888–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podor, T.J.; Campbell, S.; Chindemi, P.; Foulon, D.M.; Farrell, D.H.; Walton, P.D.; Weitz, J.I.; Peterson, C.B. Incorporation of Vitronectin into Fibrin Clots evidence for a binding interaction between vitronectin and γA/γ′ fibrinogen. J. Biol. Chem. 2002, 277, 7520–7528. [Google Scholar] [CrossRef] [Green Version]
- Arroyo De Prada, N.; Schroeck, F.; Sinner, E.K.; Muehlenweg, B.; Twellmeyer, J.; Sperl, S.; Wilhelm, O.G.; Schmitt, M.; Magdolen, V. Interaction of plasminogen activator inhibitor type-1 (PAI-1) with vitronectin: Characterization of different PAI-1 mutants. Eur. J. Biochem. 2002, 269, 184–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cevik, O.; Baykal, A.T.; Sener, A. Platelets proteomic profiles of acute ischemic stroke patients. PLoS ONE 2016, 11, e0158287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekmekci, H.; Sonmez, H.; Ekmekci, O.B.; Ozturk, Z.; Domanic, N.; Kokoglu, E. Plasma vitronectin levels in patients with coronary atherosclerosis are increased and correlate with extent of disease. J. Thromb. Thromb. 2002, 14, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Kanters, S.D.; Banga, J.-D.; Algra, A.; Frijns, R.C.; Beutler, J.J.; Fijnheer, R. Plasma levels of cellular fibronectin in diabetes. Diabetes Care 2001, 24, 323–327. [Google Scholar] [CrossRef] [Green Version]
- Keasey, M.P.; Jia, C.; Pimentel, L.F.; Sante, R.R.; Lovins, C.; Hagg, T. Blood vitronectin is a major activator of LIF and IL-6 in the brain through integrin–FAK and uPAR signaling. J. Cell Sci. 2018, 131, jcs202580. [Google Scholar] [CrossRef] [Green Version]
- Jones, A.L.; Hulett, M.D.; Parish, C.R. Histidine-rich glycoprotein: A novel adaptor protein in plasma that modulates the immune, vascular and coagulation systems. Immunol. Cell Biol. 2005, 83, 106–118. [Google Scholar] [CrossRef]
- Vu, T.T.; Stafford, A.R.; Leslie, B.A.; Kim, P.Y.; Fredenburgh, J.C.; Weitz, J.I. Histidine-rich glycoprotein binds fibrin (ogen) with high affinity and competes with thrombin for binding to the γ′-chain. J. Biol. Chem. 2011, 286, 30314–30323. [Google Scholar] [CrossRef] [Green Version]
- Lawler, J. The functions of thrombospondin-1 and-2. Curr. Opi. Cell Biol. 2000, 12, 634–640. [Google Scholar] [CrossRef]
- Cheng, C.; Yu, Z.; Zhao, S.; Liao, Z.; Xing, C.; Jiang, Y.; Yang, Y.-G.; Whalen, M.J.; Lo, E.H.; Sun, X. Thrombospondin-1 gene deficiency worsens the neurological outcomes of traumatic brain injury in mice. Int. J. Med. Sci. 2017, 14, 927. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Ye, Z.-N.; Liu, J.-P.; Zhang, Z.-H.; Zhou, C.-H.; Wang, Y.; Hang, C.-H. Elevated cerebrospinal fluid levels of thrombospondin-1 correlate with adverse clinical outcome in patients with aneurysmal subarachnoid hemorrhage. J. Neurol. Sci. 2016, 369, 126–130. [Google Scholar] [CrossRef]
- Bonnefoy, A.; Hantgan, R.; Legrand, C.; Frojmovic, M.M. A model of platelet aggregation involving multiple interactions of thrombospondin-1, fibrinogen, and GPIIbIIIa receptor. J. Biol. Chem. 2001, 276, 5605–5612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.-L.; Jong, Y.-S.; Wu, Y.-W.; Wang, W.-J.; Hsieh, A.-R.; Chao, C.-L.; Chen, W.-J.; Yang, W.-S. Association of plasma thrombospondin-1 level with cardiovascular disease and mortality in hemodialysis patients. Acta Cardiol. Sin. 2015, 31, 113. [Google Scholar] [PubMed]
- Kong, P.; Cavalera, M.; Frangogiannis, N.G. The role of thrombospondin (TSP)-1 in obesity and diabetes. Adipocyte 2014, 3, 81–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collen, D. The plasminogen (fibrinolytic) system. Thromb. Haemost. 1999, 82, 259–270. [Google Scholar] [CrossRef]
- Thiebaut, A.M.; Gauberti, M.; Ali, C.; De Lizarrondo, S.M.; Vivien, D.; Yepes, M.; Roussel, B.D. The role of plasminogen activators in stroke treatment: Fibrinolysis and beyond. Lancet Neurol. 2018, 17, 1121–1132. [Google Scholar] [CrossRef]
- Lowe, G.; Danesh, J.; Lewington, S.; Walker, M.; Lennon, L.; Thomson, A.; Rumley, A.; Whincup, P. Tissue plasminogen activator antigen and coronary heart disease: Prospective study and meta-analysis. Eur. Heart J. 2004, 25, 252–259. [Google Scholar] [CrossRef]
- Geiger, M.; Binder, B. Plasminogen activation in diabetes mellitus. Enzyme 1988, 40, 149–157. [Google Scholar] [CrossRef]
- Dahlbäck, B.; Villoutreix, B.O. Regulation of blood coagulation by the protein C anticoagulant pathway: Novel insights into structure-function relationships and molecular recognition. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1311–1320. [Google Scholar] [CrossRef]
- Wang, Z.H.; Zhao, Z.J.; Xu, K.; Sun, G.B.; Song, L.; Yin, H.X.; Chen, X.Q. Hereditary protein S deficiency leads to ischemic stroke. Mol. Med. Rep. 2015, 12, 3279–3284. [Google Scholar] [CrossRef] [Green Version]
- Noris, M.; Remuzzi, G. Overview of complement activation and regulation. Semin. Nephrol. 2013, 33, 479–492. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Yang, N.; Gao, C. Is plasma C3 and C4 levels useful in young cerebral ischemic stroke patients? Associations with prognosis at 3 months. J. Thromb. Thromb. 2015, 39, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Brigelius-Flohe, R.; Maiorino, M. Glutathione peroxidases. Biochim. Biophys. Acta BBA Gen. Subj. 2013, 1830, 3289–3303. [Google Scholar] [CrossRef] [PubMed]
- Chehaibi, K.; Trabelsi, I.; Mahdouani, K.; Slimane, M.N. Correlation of oxidative stress parameters and inflammatory markers in ischemic stroke patients. J. Stroke Cerebrovasc. Dis. 2016, 25, 2585–2593. [Google Scholar] [CrossRef] [PubMed]
- Poh Loh, K.; Hong Huang, S.; De Silva, R.; Tan, H.; Benny, K.; Zhun Zhu, Y. Oxidative stress: Apoptosis in neuronal injury. Curr. Alzheimer Res. 2006, 3, 327–337. [Google Scholar] [CrossRef]
- Kuyumcu, F.; Aycan, A. Evaluation of oxidative stress levels and antioxidant enzyme activities in burst fractures. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2018, 24, 225. [Google Scholar] [CrossRef]
- Žitňanová, I.; Šiarnik, P.; Kollár, B.; Chomová, M.; Pazderová, P.; Andrezálová, L.; Ježovičová, M.; Koňariková, K.; Laubertová, L.; Krivošíková, Z. Oxidative stress markers and their dynamic changes in patients after acute ischemic stroke. Oxid. Med. Cell. Longev. 2016, 2016, 9761697. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, H.; Murakami, Y.; Inoue, S.; Ohta, Y.; Nakamura, K.; Katoh, H.; Sakne, T.; Takahashi, N.; Ohata, S.; Sugamori, T.; et al. High plasma brain natriuretic polypeptide level as a marker of risk for thromboembolism in patients with nonvalvular atrial fibrillation. Stroke 2002, 33, 1005–1010. [Google Scholar] [CrossRef] [Green Version]
- Tuttolomondo, A.; Di Sciacca, R.; Di Raimondo, D.; Serio, A.; D’Aguanno, G.; La Placa, S.; Pecoraro, R.; Arnao, V.; Marino, L.; Monaco, S.; et al. Plasma levels of inflammatory and thrombotic/fibrinolytic markers in acute ischemic strokes: Relationship with TOAST subtype, outcome and infarct site. J. Neuroimmunol. 2009, 215, 84–99. [Google Scholar] [CrossRef]
- Fornage, M.; Chiang, Y.A.; O’Meara, E.S.; Psaty, B.M.; Reiner, A.P.; Siscovick, D.S.; Tracy, R.P.; Longstreth, W.T., Jr. Biomarkers of inflammation and MRI-Defined small vessel disease of the brain: The cardiovascular health study. Stroke 2008, 39, 1952–1959. [Google Scholar] [CrossRef] [Green Version]
- Suwanwela, N.C.; Chutinet, A.; Phanthumchinda, K. Inflammatory markers and conventional atherosclerotic risk factors in acute ischemic stroke: Comparative study between vascular disease subtypes. J. Med. Assoc. Thail. Chotmaihet Thangphaet 2006, 89, 2021–2027. [Google Scholar]
- Alvarez-Perez, F.J.; Castelo-Branco, M.; Alvarez-Sabin, J. Usefulness of measurement of fibrinogen, D-dimer, D-dimer/fibrinogen ratio, C reactive protein and erythrocyte sedimentation rate to assess the pathophysiology and mechanism of ischaemic stroke. J. Neurol. Neurosurg. Psychiatry 2011, 82, 986–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, D.F.; Li, H.; Jeffries, N.; Wright, V.; Cooper, R.A., Jr.; Elkahloun, A.; Gelderman, M.P.; Zudaire, E.; Blevins, G.; Yu, H.; et al. Using peripheral blood mononuclear cells to determine a gene expression profile of acute ischemic stroke: A pilot investigation. Circulation 2005, 111, 212–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jickling, G.C.; Xu, H.; Stamova, B.; Ander, B.P.; Zhan, X.; Tian, Y.; Liu, D.; Turner, R.J.; Mesias, M.; Verro, P.; et al. Signatures of cardioembolic and large-vessel ischemic stroke. Ann. Neurol. 2010, 68, 681–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jickling, G.C.; Stamova, B.; Ander, B.P.; Zhan, X.; Tian, Y.; Liu, D.; Xu, H.; Johnston, S.C.; Verro, P.; Sharp, F.R. Profiles of lacunar and nonlacunar stroke. Ann. Neurol. 2011, 70, 477–485. [Google Scholar] [CrossRef]
- Jickling, G.C.; Stamova, B.; Ander, B.P.; Zhan, X.; Liu, D.; Sison, S.M.; Verro, P.; Sharp, F.R. Prediction of cardioembolic, arterial, and lacunar causes of cryptogenic stroke by gene expression and infarct location. Stroke 2012, 43, 2036–2041. [Google Scholar] [CrossRef]
- Harbeck, N.; Sotlar, K.; Wuerstlein, R.; Doisneau-Sixou, S. Molecular and protein markers for clinical decision making in breast cancer: Today and tomorrow. Cancer Treat. Rev. 2014, 40, 434–444. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Accession No. | Protein Name | Risk Factors | Pathogenesis | |||||
|---|---|---|---|---|---|---|---|---|
| Hypertension | Cardiovascular Disease | Diabetes | High Cholesterol | Immune Response | Oxidative Stress | Apoptosis | ||
| P00734 | Prothrombin | √ | √ | |||||
| P00740 | Coagulation factor IX | √ | √ | |||||
| P00747 | Plasminogen | √ | ||||||
| P02671 | Fibrinogen alpha chain | √ | √ | √ | √ | √ | ||
| P02751 | Fibronectin | √ | √ | √ | ||||
| P04004 | Vitronectin | √ | √ | √ | √ | |||
| P04196 | Histidine-rich glycoprotein | √ | √ | √ | ||||
| P07225 | Vitamin K-dependent protein S | √ | √ | √ | ||||
| P07996 | Thrombospondin-1 | √ | √ | √ | √ | √ | √ | √ |
| P09871 | Complement C1s subcomponent | √ | ||||||
| P22352 | Glutathione peroxidase 3 | √ | √ | √ | √ | √ | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Park, A.; Mun, S.; Kim, H.-J.; Son, H.; Choi, H.; Kim, D.; Lee, S.J.; Kim, J.G.; Kang, H.-G. Proteomics-Based Identification of Diagnostic Biomarkers Related to Risk Factors and Pathogenesis of Ischemic Stroke. Diagnostics 2020, 10, 340. https://doi.org/10.3390/diagnostics10050340
Lee J, Park A, Mun S, Kim H-J, Son H, Choi H, Kim D, Lee SJ, Kim JG, Kang H-G. Proteomics-Based Identification of Diagnostic Biomarkers Related to Risk Factors and Pathogenesis of Ischemic Stroke. Diagnostics. 2020; 10(5):340. https://doi.org/10.3390/diagnostics10050340
Chicago/Turabian StyleLee, Jiyeong, Arum Park, Sora Mun, Hyo-Jin Kim, Hyunsong Son, Hyebin Choi, Doojin Kim, Soo Joo Lee, Jae Guk Kim, and Hee-Gyoo Kang. 2020. "Proteomics-Based Identification of Diagnostic Biomarkers Related to Risk Factors and Pathogenesis of Ischemic Stroke" Diagnostics 10, no. 5: 340. https://doi.org/10.3390/diagnostics10050340