The Diagnostic Dilemma of Malignant Biliary Strictures


Abstract
:1. Introduction
2. Etiology
3. Presentation and Laboratory Markers
4. Biomarkers
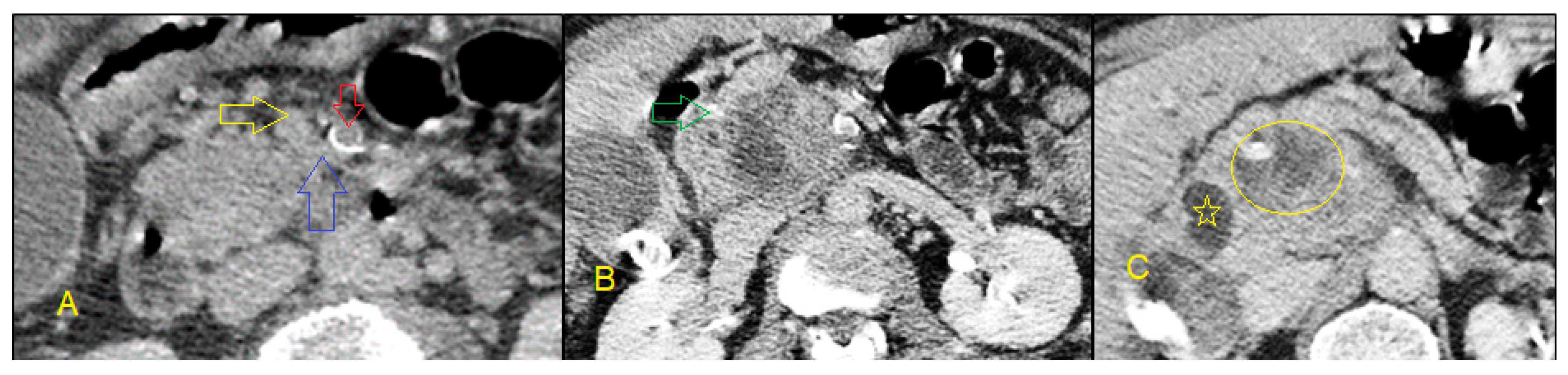
5. Non-Invasive Imaging Studies
6. Invasive Imaging Methods
6.1. Endoscopic Retrograde Cholangiopancreatography
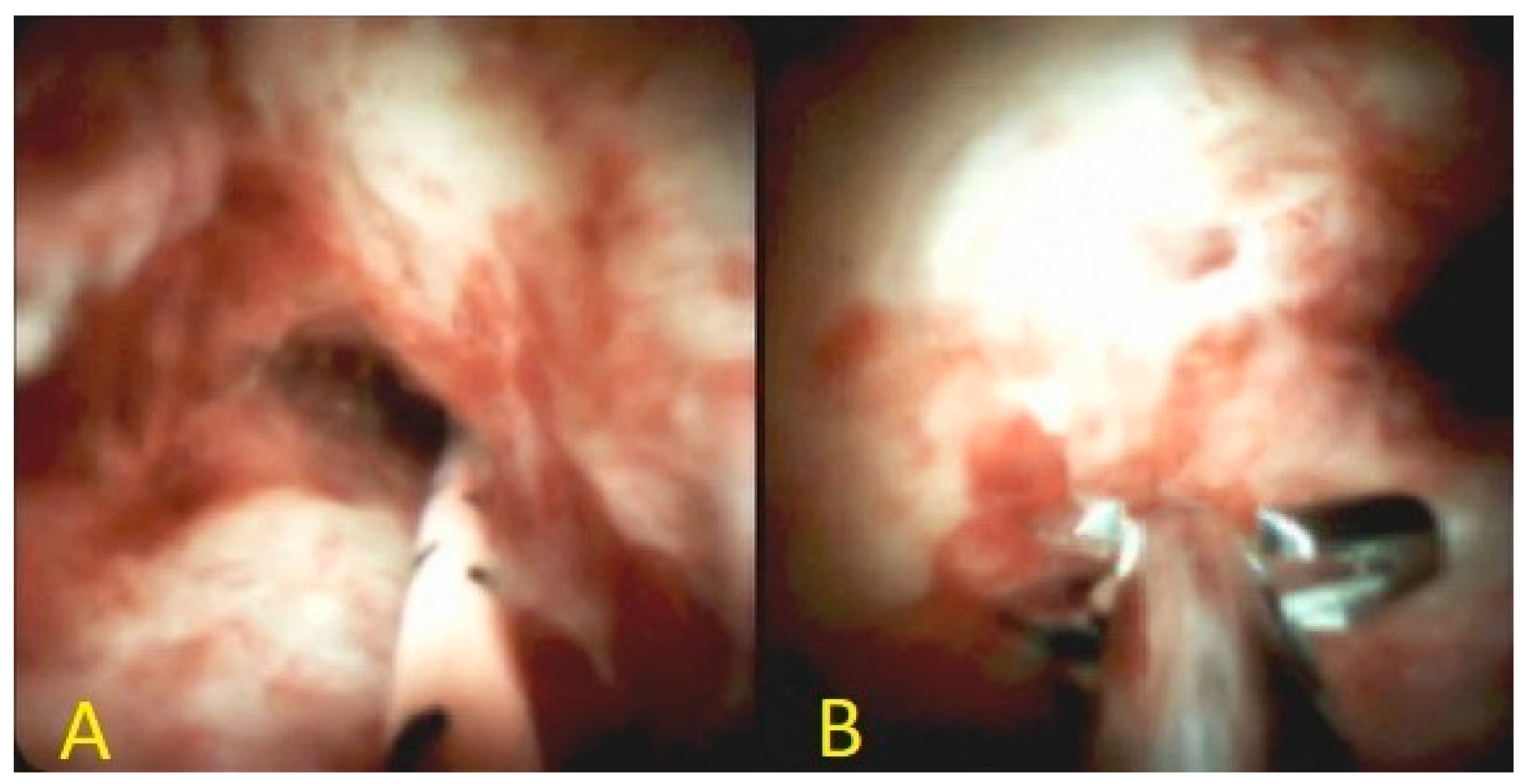
6.2. Cholangioscopy
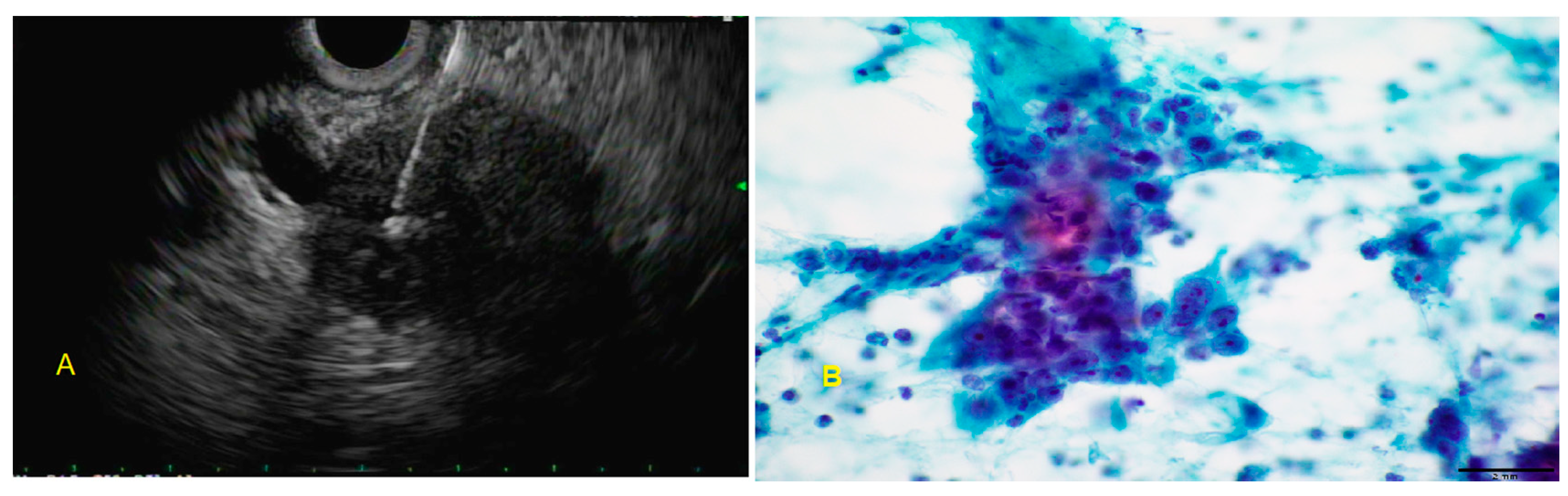
6.3. Endoscopic Ultrasound-Guided Fine-Needle Aspiration
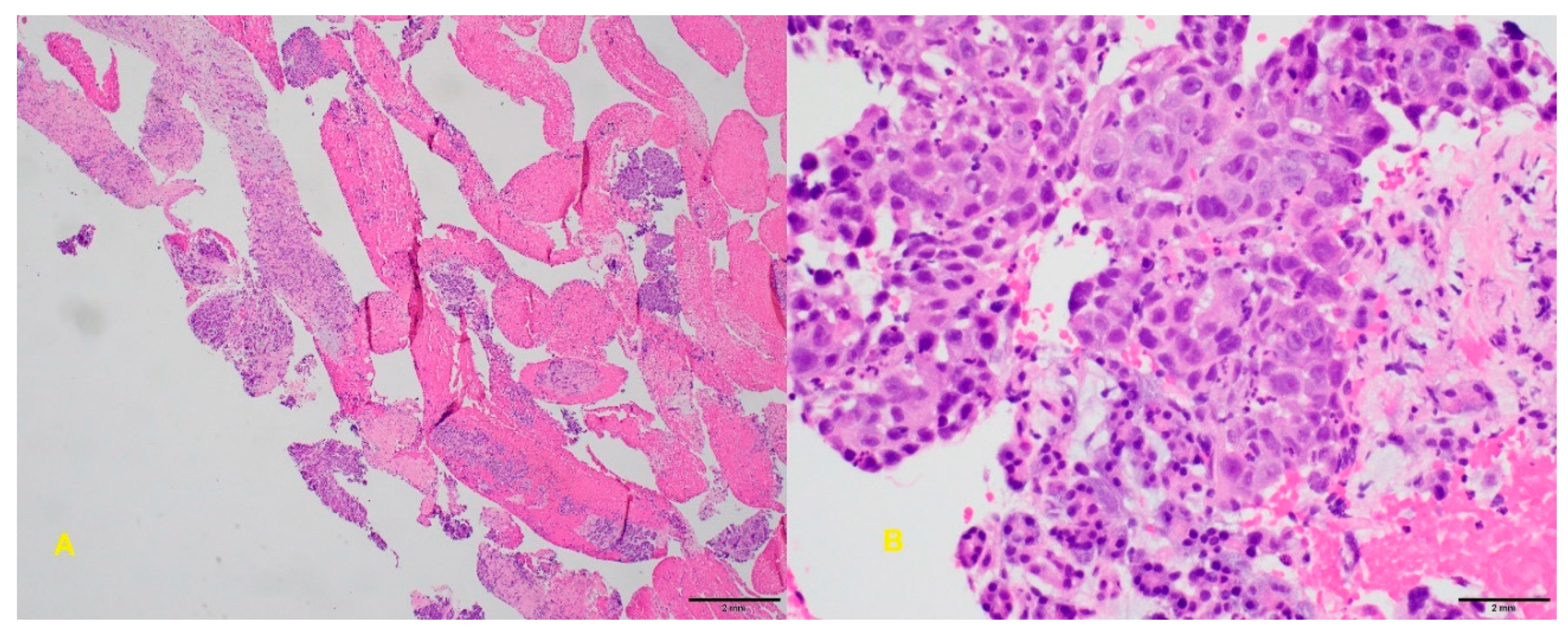
6.4. Endoscopic Ultrasound-Guided Fine-Needle Biopsy
6.5. Intraductal Ultrasound
6.6. Confocal Laser Endomicroscopy
6.7. Percutaneous Transhepatic Cholangiography
7. Conclusions
Funding
Conflicts of Interest
References
- Tummala, P.; Munigala, S.; Eloubeidi, M.A.; Agarwal, B. Patients with obstructive jaundice and biliary stricture±mass lesion on imaging: Prevalence of malignancy and potential role of EUS-FNA. J. Clin. Gastroenterol. 2013, 47, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Ballinger, A.; McHugh, M.; Catnach, S.; Alstead, E.; Clark, M. Symptom relief and quality of life after stenting for malignant bile duct obstruction. Gut 1994, 35, 467–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulay, B.R.; Birg, A. Malignant biliary obstruction: From palliation to treatment. World J. Gastrointest. Oncol. 2016, 8, 498. [Google Scholar] [CrossRef] [PubMed]
- Viesca, M.F.Y.; Arvanitakis, M. Early Diagnosis And Management Of Malignant Distal Biliary Obstruction: A Review On Current Recommendations And Guidelines. Clin. Exp. Gastroenterol. 2019, 12, 415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welzel, T.M.; Graubard, B.I.; El–Serag, H.B.; Shaib, Y.H.; Hsing, A.W.; Davila, J.A.; McGlynn, K.A. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma in the United States: A population-based case-control study. Clin. Gastroenterol. Hepatol. 2007, 5, 1221–1228. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, B.S.; Mauri, G.; Lorenz, J.M. Management of biliary strictures: State-of-the-art review. Radiology 2018, 289, 590–603. [Google Scholar] [CrossRef] [Green Version]
- Garcea, G.; Ngu, W.; Neal, C.P.; Dennison, A.R.; Berry, D.P. Bilirubin levels predict malignancy in patients with obstructive jaundice. HPB 2011, 13, 426–430. [Google Scholar] [CrossRef] [Green Version]
- Hayat, J.; Loew, C.; Asrress, K.; McIntyre, A.; Gorard, D. Contrasting liver function test patterns in obstructive jaundice due to biliary structures and stones. Qjm 2005, 98, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Thomasset, S.C.; Saunders, D.; Holland, A.; Dennison, A.R.; Garcea, G. Malignant biliary strictures in patients with a normal bilirubin and/or normal liver enzymes. HPB 2015, 17, 969–974. [Google Scholar] [CrossRef] [Green Version]
- Hasan, S.; Jacob, R.; Manne, U.; Paluri, R. Advances in pancreatic cancer biomarkers. Oncol. Rev. 2019, 13, 410. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Yang, J.; Li, H.; Wu, Y.; Zhang, H.; Chen, W. Tumor markers CA19-9, CA242 and CEA in the diagnosis of pancreatic cancer: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 11683. [Google Scholar] [PubMed]
- Yue, T.; Partyka, K.; Maupin, K.A.; Hurley, M.; Andrews, P.; Kaul, K.; Moser, A.J.; Zeh, H.; Brand, R.E.; Haab, B.B. Identification of blood-protein carriers of the CA 19-9 antigen and characterization of prevalence in pancreatic diseases. Proteomics 2011, 11, 3665–3674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, E.; Zhou, S.; Bhat, K.; Ma, Q. CA 19-9 and pancreatic cancer. Clin. Adv. Hematol. Oncol. HO 2013, 11, 53. [Google Scholar]
- Sayed, M.M.; Elshafie, A.I.; Lotfy, M.; Abdelhakam, S.M.; Rushdy, M. Clinical significance of serum CA 19-9, CA 19-9/CRP ratio and CA19-9/total bilirubin ratio in differentiation between malignant and benign obstructive jaundice. Eur. Acad. Res. 2017, 12, 10271–10291. [Google Scholar]
- Greca, G.L.; Sofia, M.; Lombardo, R.; Latteri, S.; Ricotta, A.; Puleo, S.; Russello, D. Adjusting CA19-9 values to predict malignancy in obstructive jaundice: Influence of bilirubin and C-reactive protein. World J. Gastroenterol. WJGJ 2012, 18, 4150. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Baruah, M.; Yadav, A.K.; Das, A.K. Role of CA 19-9 and its Ratio with CRP and Total Bilirubin in Differentiating Malignant from Benign Obstructive Jaundice. J. Clin. Diagn. Res. 2019, 13, PC06–PC09. [Google Scholar] [CrossRef]
- Liu, W.; Liu, Q.; Wang, W.; Wang, P.; Chen, J.; Hong, T.; Zhang, N.; Li, B.; Qu, Q.; He, X. Differential diagnostic roles of the serum CA19-9, total bilirubin (TBIL) and the ratio of CA19-9 to TBIL for benign and malignant. J. Cancer 2018, 9, 1804. [Google Scholar] [CrossRef] [Green Version]
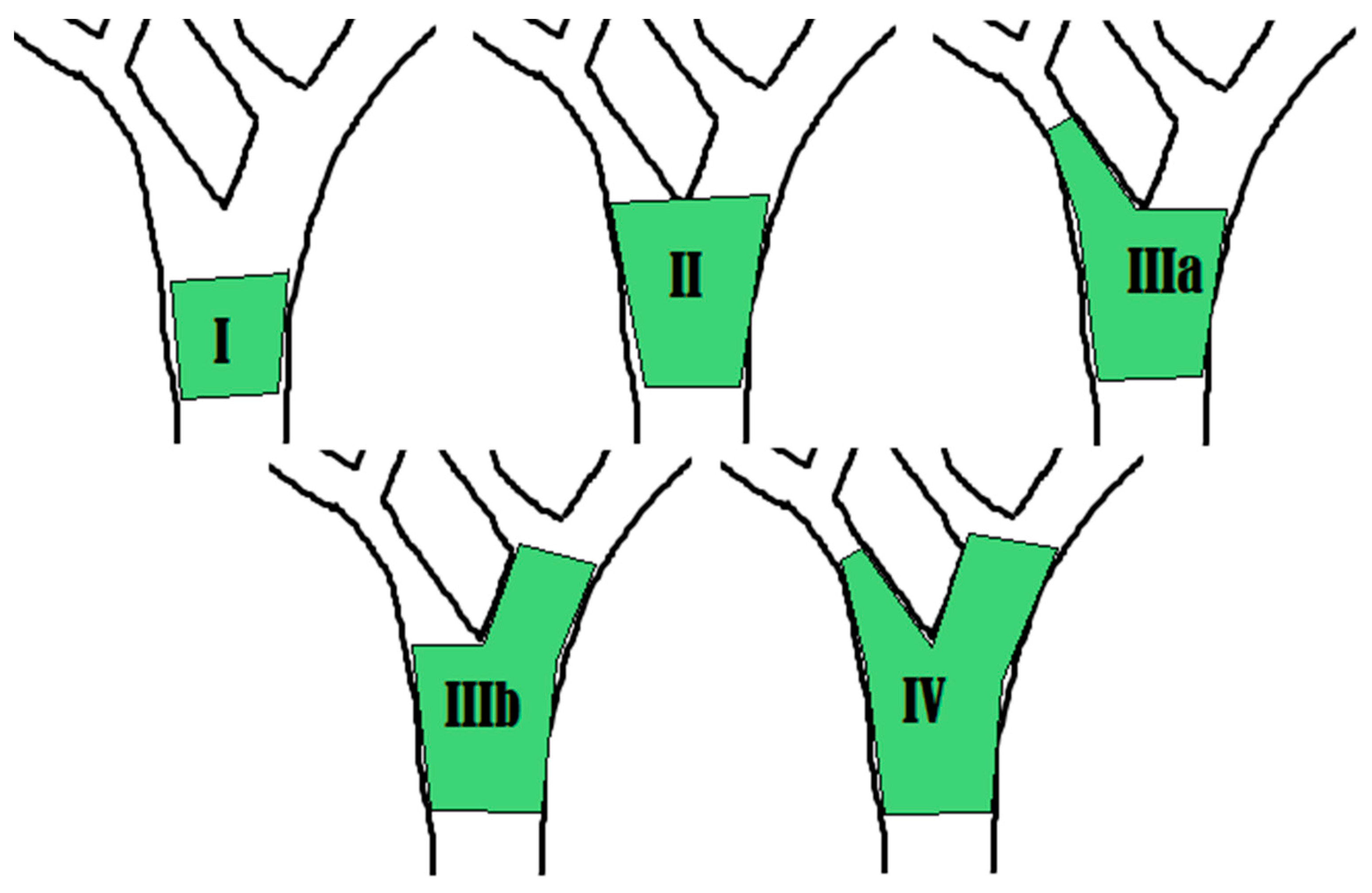
- Bismuth, H.; Majno, P.E. Biliary strictures: Classification based on the principles of surgical treatment. World J. Surg. 2001, 25, 1241–1244. [Google Scholar] [CrossRef]
- Blackbourne, L.H.; Earnhardt, R.C.; Sistrom, C.L.; Abbitt, P.; Jones, R. The sensitivity and role of ultrasound in the evaluation of biliary obstruction. Am. Surg. 1994, 60, 683–690. [Google Scholar]
- Harvey, R.T.; Miller, W.T., Jr. Acute biliary disease: Initial CT and follow-up US versus initial US and follow-up CT. Radiology 1999, 213, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Feldman, M.K.; Coppa, C.P. Noninvasive imaging of the biliary tree for the interventional radiologist. Tech. Vasc. Interv. Radiol. 2015, 18, 184–196. [Google Scholar] [CrossRef]
- Baron, R.L.; Tublin, M.E.; Peterson, M.S. Imaging the spectrum of biliary tract disease. Radiol. Clin. 2002, 40, 1325–1354. [Google Scholar] [CrossRef]
- Singh, A.; Gelrud, A.; Agarwal, B. Biliary strictures: Diagnostic considerations and approach. Gastroenterol. Rep. 2015, 3, 22–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rösch, T.; Meining, A.; Frühmorgen, S.; Zillinger, C.; Schusdziarra, V.; Hellerhoff, K.; Classen, M.; Helmberger, H. A prospective comparison of the diagnostic accuracy of ERCP, MRCP, CT, and EUS in biliary strictures. Gastrointest. Endosc. 2002, 55, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Štoos-Veić, T.; Bilić, B.; Kaić, G.; Ostović, K.T.; Babić, Ž.; Kujundžić, M. Biliary brush cytology for the diagnosis of malignancy: A single center experience. Coll. Antropol. 2010, 34, 139–143. [Google Scholar]
- Nakai, Y.; Isayamam, H.; Wang, H.P.; Rerknimitr, R.; Khor, C.; Yasuda, I.; Kogure, H.; Moon, J.H.; Lau, J.; Lakhtakia, S. International consensus statements for endoscopic management of distal biliary stricture. J. Gastroenterol. Hepatol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Roth, G.S.; Bichard, P.; Fior-Gozlan, M.; Roth, H.; Auroux, J.; Risse, O.; Letoublon, C.; Laverrière, M.H.; Bricault, I.; Leroy, V. Performance of bile aspiration plus brushing to diagnose malignant biliary strictures during endoscopic retrograde cholangiopancreatography. Endosc. Int. Open 2016, 4, E997–E1003. [Google Scholar] [CrossRef] [Green Version]
- Nakahara, K.; Michikawa, Y.; Morita, R.; Suetani, K.; Morita, N.; Sato, J.; Tsuji, K.; Ikeda, H.; Matsunaga, K.; Watanabe, T. Diagnostic ability of endoscopic bile cytology using a newly designed biliary scraper for biliary strictures. Dig. Dis. Sci. 2019, 64, 241–248. [Google Scholar] [CrossRef]
- Le, N.; Fillinger, J.; Szanyi, S.; Wichmann, B.; Nagy, Z.; Ivády, G.; Burai, M.; Tarpay, Á.; Pozsár, J.; Pap, Á. Analysis of microRNA expression in brush cytology specimens improves the diagnosis of pancreatobiliary cancer. Pancreatology 2019, 19, 873–879. [Google Scholar] [CrossRef]
- Jang, S.I.; Kwon, N.H.; Lim, B.J.; Nahm, J.H.; Park, J.S.; Kang, C.M.; Park, S.R.; Sd, S.Y.L.; Kang, B.S.; Kim, S.; et al. A new staining method using methionyl-tRNA synthetase 1 antibody for brushing cytology of bile duct cancer. Gastrointest. Endosc. 2019. [Google Scholar] [CrossRef]
- Kushnir, V.M.; Mullady, D.K.; Das, K.; Lang, G.; Hollander, T.G.; Murad, F.M.; Jackson, S.A.; Toney, N.A.; Finkelstein, S.D.; Edmundowicz, S.A. The diagnostic yield of malignancy comparing cytology, FISH, and molecular analysis of cell free cytology brush supernatant in patients with biliary strictures undergoing endoscopic retrograde cholangiography (ERC): A prospective study. J. Clin. Gastroenterol. 2019, 53, 686. [Google Scholar] [CrossRef] [PubMed]
- Korc, P.; Sherman, S. ERCP tissue sampling. Gastrointest. Endosc. 2016, 84, 557–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayoub, F.; Yang, D.; Draganov, P.V. Cholangioscopy in the digital era. Transl. Gastroenterol. Hepatol. 2018, 3, 82. [Google Scholar] [CrossRef] [PubMed]
- Kulpatcharapong, S.; Pittayanon, R.; Kerr, S.J.; Rerknimitr, R. Diagnostic performance of different cholangioscopes in patients with biliary strictures: A systematic review. Endoscopy 2020, 52, 174–185. [Google Scholar] [CrossRef]
- Pérez-Cuadrado-Robles, E.; Deprez, P.H. Indications for Single-Operator Cholangioscopy and Pancreatoscopy: An Expert Review. Curr. Treat. Options Gastroenterol. 2019, 17, 408–419. [Google Scholar] [CrossRef]
- Sethi, A.; Doukides, T.; Sejpal, D.V.; Pleskow, D.K.; Slivka, A.; Adler, D.G.; Shah, R.J.; Edmundowicz, S.A.; Itoi, T.; Petersen, B.T. Interobserver agreement for single operator choledochoscopy imaging: Can we do better? Diagn. Ther. Endosc. 2014, 2014, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Sethi, A.; Tyberg, A.; Slivka, A.; Adler, D.G.; Desai, A.P.; Sejpal, D.V.; Pleskow, D.K.; Bertani, H.; Gan, S.-I.; Shah, R. Digital Single-operator Cholangioscopy (DSOC) Improves Interobserver Agreement (IOA) and Accuracy for Evaluation of Indeterminate Biliary Strictures: The Monaco Classification. J. Clin. Gastroenterol. 2020. [Google Scholar] [CrossRef]
- Nguyen, N.Q.; Schoeman, M.N.; Ruszkiewicz, A. Clinical utility of EUS before cholangioscopy in the evaluation of difficult biliary strictures. Gastrointest. Endosc. 2013, 78, 868–874. [Google Scholar] [CrossRef]
- Sethi, A.; Chen, Y.K.; Austin, G.L.; Brown, W.R.; Brauer, B.C.; Fukami, N.N.; Khan, A.H.; Shah, R.J. ERCP with cholangiopancreatoscopy may be associated with higher rates of complications than ERCP alone: A single-center experience. Gastrointest. Endosc. 2011, 73, 251–256. [Google Scholar] [CrossRef]
- Yeo, S.J.; Cho, C.M.; Jung, M.K.; Seo, A.N.; Bae, H.I. Comparison of the Diagnostic Performances of Same-session Endoscopic Ultrasound-and Endoscopic Retrograde Cholangiopancreatography-guided Tissue Sampling for Suspected Biliary Strictures at Different Primary Tumor Sites. Korean J. Gastroenterol. 2019, 73, 213–218. [Google Scholar] [CrossRef]
- Wang, W.; Shpaner, A.; Krishna, S.G.; Ross, W.A.; Bhutani, M.S.; Tamm, E.P.; Raju, G.S.; Xiao, L.; Wolff, R.A.; Fleming, J.B. Use of EUS-FNA in diagnosing pancreatic neoplasm without a definitive mass on CT. Gastrointest. Endosc. 2013, 78, 73–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, M.M.; Andalib, I.; Novikov, A.; Dawod, E.; Gabr, M.; Gaidhane, M.; Tyberg, A.; Kahaleh, M. Endoscopic Therapy for Pancreatic Fluid Collections: A Definitive Management Using a Dedicated Algorithm. Clin. Endosc. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaguchi, M.; Fukuda, T.; Nakahara, M.; Amano, M.; Takei, D.; Kawashima, M.; Sumi, Y.; Amano, H.; Yonehara, S.; Hanada, K. Multicentric solid pseudopapillary neoplasms of the pancreas diagnosed by endoscopic ultrasound-guided fine needle aspiration: A case report. Surg. Case Rep. 2015, 1, 110. [Google Scholar] [CrossRef] [Green Version]
- De Moura, D.T.H.; De Moura, E.G.H.; Bernardo, W.M.; De Moura, E.T.H.; Baracat, F.I.; Kondo, A.; Matuguma, S.E.; Artifon, E.L.A. Endoscopic retrograde cholangiopancreatography versus endoscopic ultrasound for tissue diagnosis of malignant biliary stricture: Systematic review and meta-analysis. Endosc. Ultrasound 2018, 7, 10. [Google Scholar] [CrossRef]
- Ayres, L.R.; Kmiotek, E.K.; Lam, E.; Telford, J.J. A comparison of endoscopic ultrasound-guided fine-needle aspiration and fine-needle biopsy in the diagnosis of solid pancreatic lesions. Can. J. Gastroenterol. Hepatol. 2018, 2018, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Van Riet, P.A.; Larghi, A.; Attili, F.; Rindi, G.; Nguyen, N.Q.; Ruszkiewicz, A.; Kitano, M.; Chikugo, T.; Aslanian, H.; Farrell, J. A multicenter randomized trial comparing a 25-gauge EUS fine-needle aspiration device with a 20-gauge EUS fine-needle biopsy device. Gastrointest. Endosc. 2019, 89, 329–339. [Google Scholar] [CrossRef]
- Asokkumar, R.; Ka, C.Y.; Loh, T.; Ling, L.K.; San, T.G.; Ying, H.; Tan, D.; Khor, C.; Lim, T.; Soetikno, R. Comparison of tissue and molecular yield between fine-needle biopsy (FNB) and fine-needle aspiration (FNA): A randomized study. Endosc. Int. Open 2019, 7, E955–E963. [Google Scholar] [CrossRef]
- Facciorusso, A.; Bajwa, H.S.; Menon, K.; Buccino, V.R.; Muscatiello, N. Comparison between 22G aspiration and 22G biopsy needles for EUS-guided sampling of pancreatic lesions: A meta-analysis. Endosc Ultrasound. 2019, 10. [Google Scholar] [CrossRef]
- Khan, M.A.; Grimm, I.S.; Ali, B.; Nollan, R.; Tombazzi, C.; Ismail, M.K.; Baron, T.H. A meta-analysis of endoscopic ultrasound–fine-needle aspiration compared to endoscopic ultrasound–fine-needle biopsy: Diagnostic yield and the value of onsite cytopathological assessment. Endosc. Int. Open 2017, 5, E363–E375. [Google Scholar] [CrossRef] [Green Version]
- Valero, V., III; Saunders, T.J.; He, J.; Weiss, M.J.; Cameron, J.L.; Dholakia, A.; Wild, A.T.; Shin, E.J.; Khashab, M.A.; O’Broin-Lennon, A.M. Reliable detection of somatic mutations in fine needle aspirates of pancreatic cancer with next-generation sequencing: Implications for surgical management. Ann. Surg. 2016, 263, 153. [Google Scholar] [CrossRef]
- Imaoka, H.; Sasaki, M.; Hashimoto, Y.; Watanabe, K.; Ikeda, M. New Era of Endoscopic Ultrasound-Guided Tissue Acquisition: Next-Generation Sequencing by Endoscopic Ultrasound-Guided Sampling for Pancreatic Cancer. J. Clin. Med. 2019, 8, 1173. [Google Scholar] [CrossRef] [Green Version]
- Sun, B.; Hu, B. The role of intraductal ultrasonography in pancreatobiliary diseases. Endosc. Ultrasound 2016, 5, 291. [Google Scholar]
- Heinzow, H.S.; Kammerer, S.; Rammes, C.; Wessling, J.; Domagk, D.; Meister, T. Comparative analysis of ERCP, IDUS, EUS and CT in predicting malignant bile duct strictures. World J. Gastroenterol. WJGJ 2014, 20, 10495. [Google Scholar] [CrossRef]
- Krishna, N.B.; Saripalli, S.; Safdar, R.; Agarwal, B. Intraductal US in evaluation of biliary strictures without a mass lesion on CT scan or magnetic resonance imaging: Significance of focal wall thickening and extrinsic compression at the stricture site. Gastrointest. Endosc. 2007, 66, 90–96. [Google Scholar] [CrossRef]
- Storm, A.C.; Lee, L.S. Is Seeing Really Believing? Probe-based Confocal Laser Endomicroscopy in the Evaluation of Pancreaticobiliary Disease. J. Clin. Gastroenterol. 2016, 50, 359–365. [Google Scholar] [CrossRef]
- Karia, K.; Kahaleh, M. A review of probe-based confocal laser endomicroscopy for pancreaticobiliary disease. Clin. Endosc. 2016, 49, 462. [Google Scholar] [CrossRef]
- Almadi, M.A.; Neumann, H. Probe based confocal laser endomicroscopy of the pancreatobiliary system. World J. Gastroenterol. 2015, 21, 12696. [Google Scholar] [CrossRef]
- Fugazza, A.; Gaiani, F.; Carra, M.C.; Brunetti, F.; Lévy, M.; Sobhani, I.; Azoulay, D.; Catena, F.; de’Angelis, G.L.; de’Angelis, N. Confocal laser endomicroscopy in gastrointestinal and pancreatobiliary diseases: A systematic review and meta-analysis. Biomed. Res. Int. 2016, 2016, 1–31. [Google Scholar] [CrossRef]
- Tabibian, J.H.; Visrodia, K.H.; Levy, M.J.; Gostout, C.J. Advanced endoscopic imaging of indeterminate biliary strictures. World J. Gastrointest. Endosc. 2015, 7, 1268. [Google Scholar] [CrossRef]
- Shimada, H.; Endo, I.; Shimada, K.; Matsuyama, R.; Kobayashi, N.; Kubota, K. The current diagnosis and treatment of benign biliary stricture. Surg. Today 2012, 42, 1143–1153. [Google Scholar] [CrossRef]
- Makary, M.S.; Farrell, J.J.; Khayat, M.; Chick, J.F.B.; Srinivasa, R.N. Biliary Endoscopy for Benign and Malignant Biliary Strictures. Tech. Vasc. Interv. Radiol. 2019, 22, 135–138. [Google Scholar] [CrossRef]
- Kim, E.H.; Kim, H.-J.; Oh, H.-C.; Lee, K.H.; Jung, J.Y.; Kim, S.; Lee, S.S.; Seo, D.W.; Kim, M.-H.; Lee, S.K. The usefulness of percutaneous transhepatic cholangioscopy for identifying malignancies in distal commom bile duct strictures. J. Korean Med. Sci. 2008, 23, 579–585. [Google Scholar] [CrossRef] [Green Version]
- Oliver, J.B.; Burnett, A.S.; Ahlawat, S.; Chokshi, R.J. Cost-effectiveness of the evaluation of a suspicious biliary stricture. J. Surg. Res. 2015, 195, 52–60. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnostics of Malignant Biliary Strictures | |||
|---|---|---|---|
| Modality | Sensitivity (%) | Specificity (%) | Reference |
| Lab markers | |||
| CA 19-9 | 80 | 89–90 | Hasan et al. [10] |
| CEA | 30–68 | 75–95 | Yue et al. [12] |
| Non-invasive imaging | |||
| MRCP | 38–90 | 70–85 | Singh et al. [23] |
| CT | 75–80 | 60–80 | Singh et al. [23] |
| US | 90–95 | 30–70 | Kapoor et al. [6] |
| Invasive Imaging | |||
| PTHC | 71 | 48 | Kim et al. [62] |
| ERCP | |||
| Brushing cytology | 23–56 | 95 | Singh et al. [23] |
| Fluoroscopic biopsy | 33–65 | 95 | Singh et al. [23] |
| Brushing + fluoroscopic biopsy | 60–70 | 95 | Singh et al. [23] |
| Brushing + bile fluid | 84 | 95 | Roth et al. [27] |
| Brushing + miRNA | 54–85 | 95 | Le et al. [29] |
| Brushing + FISH | 50–60 | 95 | Kushnir et al. [31] |
| Brushing + MP | 56 | 95 | Kushnir et al. [31] |
| Brushing + FISH + MP | 66–69 | 95 | Kushnir et al. [31] |
| EUS–FNA | 80 | 97 | Nakai et al. [26] |
| Cholangioscopy | 88.9 | 97.6 | Kulpatcharapong et al. [34] |
| Cholangioscopy directed biopsy | 71–100 | 96.7–100 | Ayoub et al. [33] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dorrell, R.; Pawa, S.; Zhou, Y.; Lalwani, N.; Pawa, R. The Diagnostic Dilemma of Malignant Biliary Strictures. Diagnostics 2020, 10, 337. https://doi.org/10.3390/diagnostics10050337
Dorrell R, Pawa S, Zhou Y, Lalwani N, Pawa R. The Diagnostic Dilemma of Malignant Biliary Strictures. Diagnostics. 2020; 10(5):337. https://doi.org/10.3390/diagnostics10050337
Chicago/Turabian StyleDorrell, Robert, Swati Pawa, Yi Zhou, Neeraj Lalwani, and Rishi Pawa. 2020. "The Diagnostic Dilemma of Malignant Biliary Strictures" Diagnostics 10, no. 5: 337. https://doi.org/10.3390/diagnostics10050337