Electronic Health Information Systems to Improve Disease Diagnosis and Management at Point-of-Care in Low and Middle Income Countries: A Narrative Review


Abstract
:1. Introduction
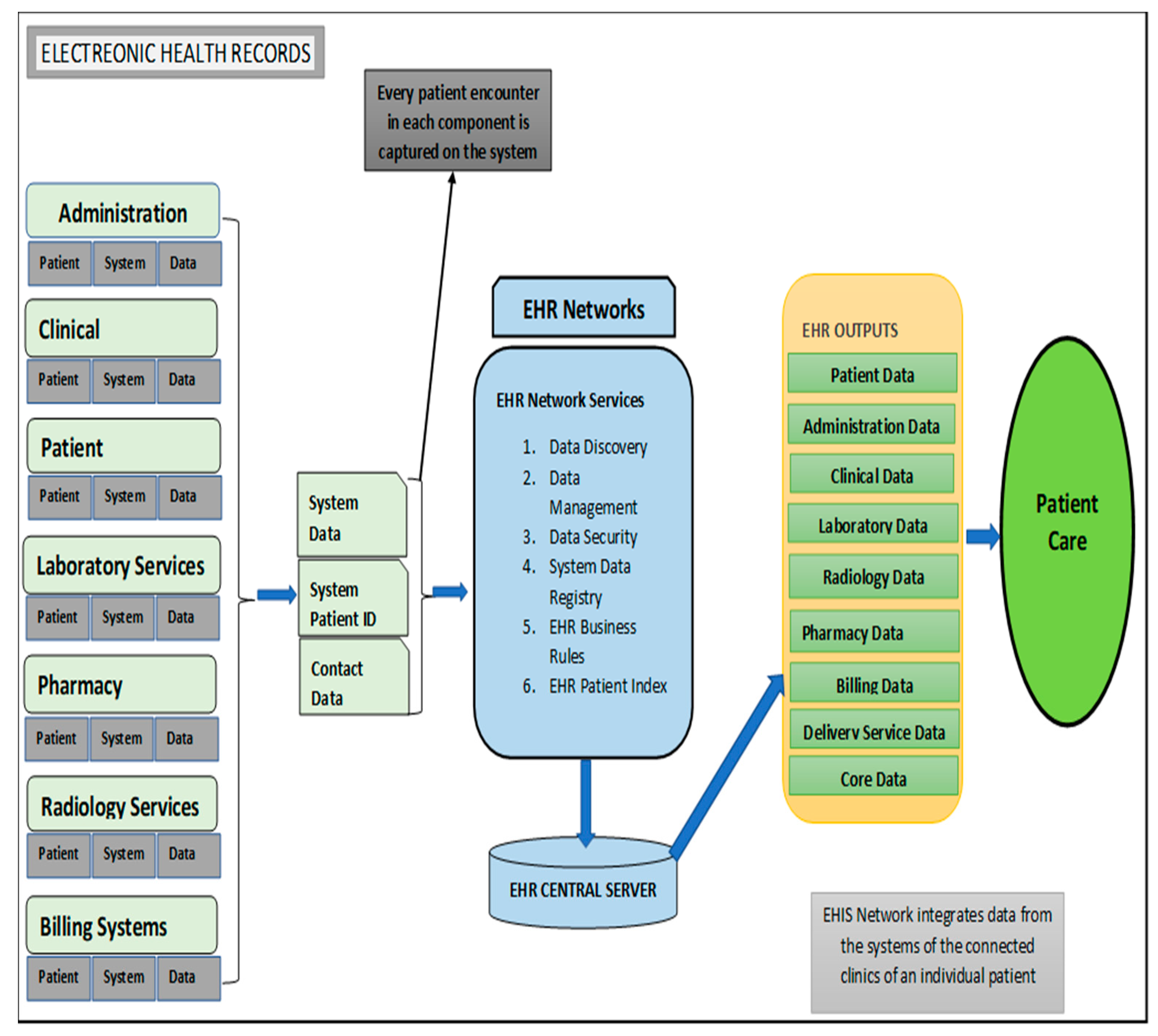
2. Characteristic of Electronic Health Information Systems
3. Opportunities Presented by EHIS in the LMICs
4. Enablers of EHIS Implementation in the LMICs
4.1. Financial Investment
4.2. Legislation
4.3. Staff Training
4.4. Political Leadership
4.5. Acceptability of Technology
5. Barriers and Challenges to Implemention of EHIS in the LMICs
5.1. Complexity of the Intervention and Lack of Technical Consensus
5.2. Limited Human Resource
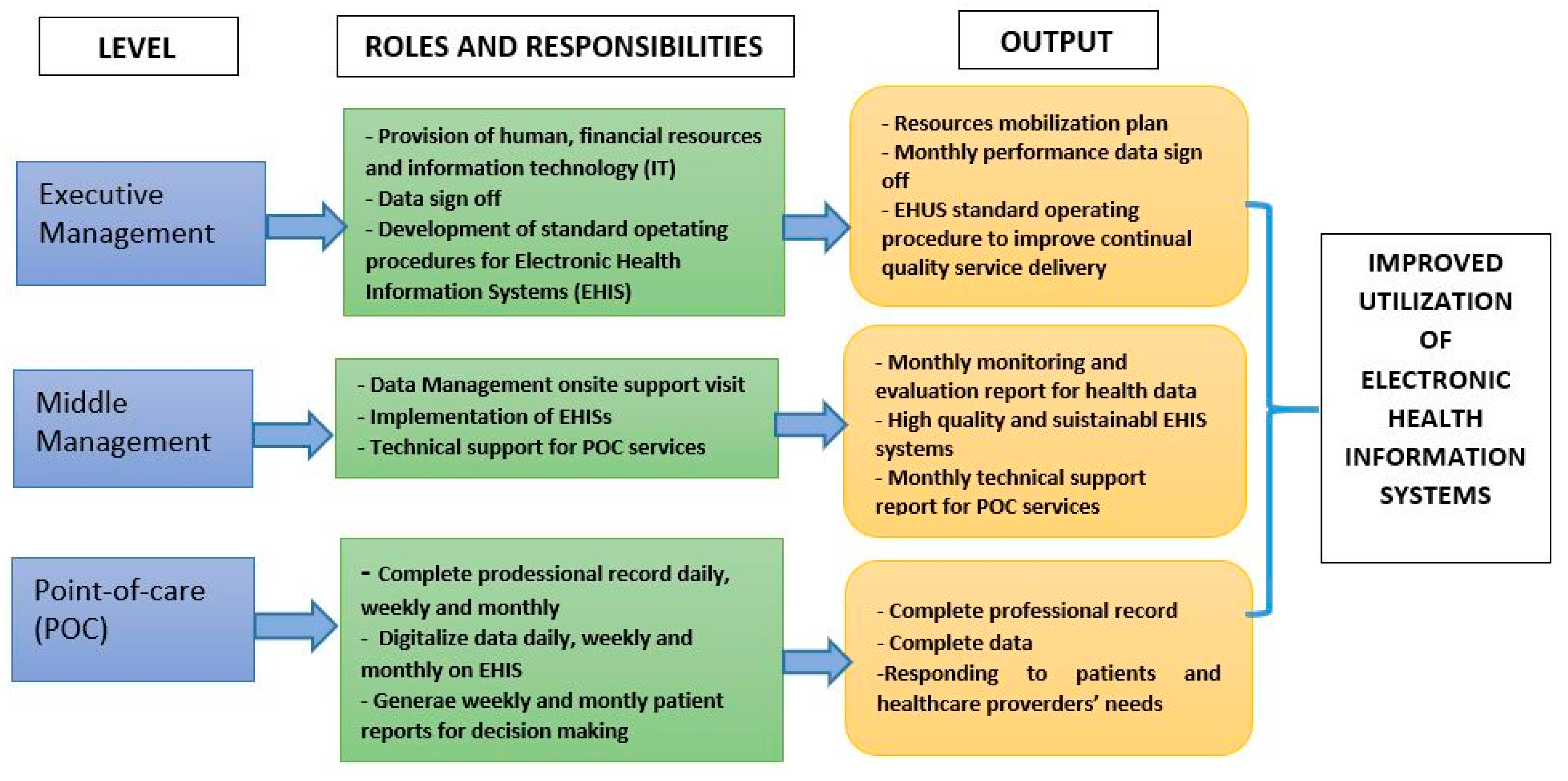
5.3. Lack of Management
5.4. Lack of Funds
5.5. Inadequate Health Systems Capacity
5.6. Poor Application of Proven Diffusion Techniques
5.7. Staff Resistance
5.8. Compromised Data Quality
6. Discussion
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Makanga, P.T.; Schuurman, N.; von Dadelszen, P.; Firoz, T. A scoping review of geographic information systems in maternal health. Int. J. Gynaecol. Obstet. 2016, 134, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Kyriacou, E.; Pavlopoulos, S.; Berler, A.; Neophytou, M.; Bourka, A.; Georgoulas, A.; Anagnostaki, A.; Karayiannis, D.; Schizas, C.; Pattichis, C.; et al. Multi-purpose HealthCare Telemedicine Systems with mobile communication link support. Biomed. Eng. Online 2003, 2, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, G.; Goldsmith, J.; Roller, P.S.; Widran, S.; Patterson, G.W.; Daugherty, J.R.; Van Antwerp, W.P. Medical Data Management System and Process. U.S. Patent 8, 313.433 B2, 20 November 2012. [Google Scholar]
- Muller-Staub, M. Evaluation of the Implementation of Nursing Diagnostics. A Study of the Use of Nursing Diagnoses, Interventions and Outcomes in Nursing Documentation; Blackwell Publishing LTD: Oxford, UK, 2007. [Google Scholar]
- Müller-Staub, M. Evaluation of the implementation of nursing diagnoses, interventions, and outcomes. Int. J. Nurs. Terminol. Classif. 2009, 20, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Hunt, D.L.; Haynes, R.B.; Hanna, S.E.; Smith, K.J.J. Effects of computer-based clinical decision support systems on physician performance and patient outcomes: A systematic review. JAMA 1998, 280, 1339–1346. [Google Scholar] [CrossRef] [PubMed]
- Brook, C. What is a Health Information System? Available online: https://digitalguardian.com/blog/what-health-information-system (accessed on 15 May 2020).
- HealthIT.Gov. What is an electronic health record (EHR)? National Coordinator for Health Information Technology 2018. Available online: https://www.healthit.gov/faq/what-electronic-health-record-ehr (accessed on 15 May 2020).
- Osler, M.; Hilderbrand, K.; Hennessey, C.; Arendse, J.; Goemaere, E.; Ford, N.; Boulle, A. A three-tier framework for monitoring antiretroviral therapy in high HIV burden settings. J. Int. Aids Soc. 2014, 17, 18908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elgujja, A.A. Impact of Information Technology on Patient Confidentiality Rights: A Perspectives. In Impacts of Information Technology on Patient Care and Empowerment; IGI Global: Hershey, PA, USA, 2020. [Google Scholar]
- Mashamba-Thompson, T.P.; Crayton, E.D. Blockchain and Artificial Intelligence Technology for Novel Coronavirus Disease-19 Self-Testing. Diagnostics 2020, 10, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowman, S. Impact of electronic health record systems on information integrity: Quality and safety implications. Perspect. Health Inf. Manag. 2013, 10, 1c. [Google Scholar] [PubMed]
- National Institutes of Health. Electronic health records overview. In National Center for Research Resources; National Institutes of Health: Bethesda, MD, USA, 2006. [Google Scholar]
- Basic Components of Electronic Health Record. Available online: https://rxvisor.com/2013/12/28/2013-12-28-basic-components-of-an-electronic-health-record/ (accessed on 15 May 2020).
- Hartzler, A.; McCarty, C.A.; Rasmussen, L.V.; Williams, M.S.; Brilliant, M.; Bowton, E.A.; Clayton, E.W.; Faucett, W.A.; Ferryman, K.; Field, J.R.; et al. Stakeholder engagement: A key component of integrating genomic information into electronic health records. Genet. Med. 2013, 15, 792. [Google Scholar] [CrossRef] [Green Version]
- Van de Velde, R.; Degoulet, P. Clinical Information Systems: A Component-Based Approach; Springer Science & Business Media: Berlin, Germany, 2003. [Google Scholar]
- UKEssays. General Components of an EHR System. Available online: https://www.ukessays.com/essays/information-technology/key-components-of-electronic-health-records-information-technology-essay.php?vref=1 (accessed on 15 May 2020).
- Blaya, J.A.; Fraser, H.S.; Holt, B. E-health technologies show promise in developing countries. Health Aff. (Millwood) 2010, 29, 244–251. [Google Scholar] [CrossRef]
- Hochgesang, M.; Zamudio-Haas, S.; Moran, L.; Nhampossa, L.; Packel, L.; Leslie, H.; Richard, J.; Shade, S.B. Scaling-up health information systems to improve HIV treatment: An assessment of initial patient monitoring systems in Mozambique. International journal of medical informatics. Int. J. Med. Inform. 2017, 97, 322–330. [Google Scholar] [CrossRef]
- Mabirizi, D.; Phulu, B.; Churfo, W.; Mwinga, S.; Mazibuko, G.; Sagwa, E.; Indongo, L.; Hafner, T. Implementing an Integrated Pharmaceutical Management Information System for Antiretrovirals and Other Medicines: Lessons From Namibia. Glob. Health Sci. Pract. 2018, 6, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Akhlaq, A.; McKinstry, B.; Muhammad, K.B.; Sheikh, A. Barriers and facilitators to health information exchange in low-and middle-income country settings: A systematic review. Health Policy Plan. 2016, 31, 1310–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, L.-S.; Liu, D.-W.; Guo, B. Progress of childhood immunization information management system in China in 2008. Zhongguo Yi Miao He Mian Yi 2009, 15, 367–370. [Google Scholar]
- Moucheraud, C.; Schwitters, A.; Boudreaux, C.; Giles, D.; Kilmarx, P.H.; Ntolo, N.; Bangani, Z.; St. Louis, M.E.; Bossert, T.J. Sustainability of health information systems: A three-country qualitative study in southern Africa. BMC health services research. BMC Health Serv. Res. 2017, 17, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hersh, W. Health and biomedical informatics: Opportunities and challenges for a twenty-first century profession and its education. Yearb Med. Inform. 2008, 17, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Acquah-Swanzy, M. Evaluating Electronic Health Record Systems in Ghana: The Case of Effia Nkwanta Regional Hospital. Master’s thesis, UiT Norges Arktiske Universitet, Tromsø, Norway, 2015. [Google Scholar]
- National Health Act 61 of 2003. Available online: https://www.gov.za/documents/national-health-act (accessed on 15 May 2020).
- National Digital Health Strategy for South Africa 2019–2024; The National Department of Health Republic of South Africa: Pretoria, South Africa, 2019.
- Ledikwe, J.H.; Reason, L.L.; Burnett, S.M.; Busang, L.; Bodika, S.; Lebelonyane, R.; Ludick, S.; Matshediso, E.; Mawandia, S.; Mmelesi, M.; et al. Establishing a health information workforce: Innovation for low-and middle-income countries. Hum. Resour. Health 2013, 11, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wandera, S.O.; Kwagala, B.; Nankinga, O.; Ndugga, P.; Kabagenyi, A.; Adamou, B.; Kachero, B. Facilitators, best practices and barriers to integrating family planning data in Uganda’s health management information system. BMC Health Serv. Res. 2019, 19, 327. [Google Scholar] [CrossRef]
- Ingebrigtsen, T.; Georgiou, A.; Clay-Williams, R.; Magrabi, F.; Hordern, A.; Prgomet, M.; Li, J.; Westbrook, J.; Braithwaite, J. The impact of clinical leadership on health information technology adoption: Systematic review. Int. J. Med. Inform. 2014, 83, 393–405. [Google Scholar] [CrossRef]
- Shiferaw, F.; Zolfo, M. The role of information communication technology (ICT) towards universal health coverage: The first steps of a telemedicine project in Ethiopia. Glob. Health Action 2012, 5, 1–8. [Google Scholar]
- Nchise, A.; Boateng, R.; Mbarika, V.; Saiba, E.; Johnson, O. The challenge of taking baby steps—Preliminary insights into telemedicine adoption in Rwanda. Health Policy Technol. 2012, 1, 207–213. [Google Scholar] [CrossRef]
- Hasanain, R.A.; Vallmuur, K.; Clark, M. Electronic medical record systems in Saudi Arabia: Knowledge and preferences of healthcare professionals. J. Health Inf. Dev. Ctries. 2015, 9, 1. [Google Scholar]
- Liu, C.-F.; Cheng, T.-J. Exploring critical factors influencing physicians’ acceptance of mobile electronic medical records based on the dual-factor model: A validation in Taiwan. BMC Med. Inf. Decis. Mak. 2015, 15, 4. [Google Scholar]
- Chaiyachati, K.H.; Loveday, M.; Lorenz, S.; Lesh, N.; Larkan, L.-M.; Cinti, S.; Friedland, G.H.; Haberer, J.E. A pilot study of an mHealth application for healthcare workers: Poor uptake despite high reported acceptability at a rural South African community-based MDR-TB treatment program. PLoS ONE 2013, 8, e64662. [Google Scholar] [CrossRef]
- Yamey, G. What are the barriers to scaling up health interventions in low and middle income countries? A qualitative study of academic leaders in implementation science. Glob. Health 2012, 8, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mudaly, T.; Moodley, D.; Pillay, A.; Seebregts, C.J. Architectural Frameworks for Developing National Health Information Systems in Low and Middle Income Countries. In Proceedings of the First International Conference on Enterprise Systems: ES 2013 IEEE, Cape Town, South Africa, 7–8 November 2013. [Google Scholar]
- Crichton, R.; Moodley, D.; Pillay, A.; Gakuba, R.; Seebregts, C.J. An architecture and reference implementation of an open health information mediator: Enabling interoperability in the Rwandan health information exchange. In Proceedings of the International Symposium on Foundations of Health Informatics Engineering and Systems, Paris, France, 27–28 August 2012. [Google Scholar]
- Ramesh, K.; Shaikh, B.T.; Chandio, A.K.; Jamil, A. Role of Health Management Information System in disease reporting at a rural district of Sindh. Pak. J. Health 2012, 2, 10–12. [Google Scholar]
- Botha, M.; Botha, A.; Herselman, M. The Benefits and Challenges of e-Health Applications: A Content Analysis of the South African Context. In Proceedings of the International Conference on Computer Science, Computer Engineering, and Social Media, Thessaloniki, Greece, 12–14 December 2014. [Google Scholar]
- Asangansi, I.; Macleod, B.; Meremikwu, M.; Arikpo, I.; Roberge, D.; Hartsock, B.; Ekinya, I. Improving the routine HMIS in Nigeria through mobile technology for community data collection. J. Health Inf. Dev. Ctries. 2013, 7, 1. [Google Scholar]
- Qazi, M.S.; Ali, M. Pakistan’s health management information system: Health managers’ perspectives. J. Pak. Med. Assoc. 2009, 59, 10. [Google Scholar]
- Mishra, A.; Vasisht, I.; Kauser, A.; Thiagarajan, S.; Mairembam, D.S. Determinants of Health Management Information Systems performance: Lessons from a district level assessment. BMC Proc. 2012, 6, 17. [Google Scholar] [CrossRef] [Green Version]
- Kapadia-Kundu, N.; Sullivan, T.M.; Safi, B.; Trivedi, G.; Velu, S. Understanding health information needs and gaps in the health care system in Uttar Pradesh, India. J. Health Commun. 2012, 17 (Suppl. 2), 30–45. [Google Scholar] [CrossRef] [Green Version]
- Oluoch, T.; de Keizer, N.F. Evaluation of Health IT in Low-Income Countries. Stud. Health Technol. Inform. 2016, 222, 324–335. [Google Scholar]
- Ghia, C.J.; Patil, A.S.; Ved, J.K.; Jha, R. Benefits of telemedicine and barriers to its effective implementation in rural India: A multicentric E-survey. Indian Med. Gaz. 2013, 146, 1–7. [Google Scholar]
- Leon, N.; Schneider, H.; Daviaud, E. Applying a framework for assessing the health system challenges to scaling up mHealth in South Africa. BMC Med. Inform. Decis. Mak. 2012, 12, 123. [Google Scholar] [CrossRef] [Green Version]
- Katuu, S.; Management, T.P. Transforming South Africa’s health sector: The eHealth Strategy, the implementation of electronic document and records management systems (EDRMS) and the utility of maturity models. J. Sci. Technol. Policy Manag. 2016, 7, 330–345. [Google Scholar] [CrossRef]
- Dornan, L.; Pinyopornpanish, K.; Jiraporncharoen, W.; Hashmi, A.; Dejkriengkraikul, N.; Angkurawaranon, C. Utilisation of Electronic Health Records for Public Health in Asia: A Review of Success Factors and Potential Challenges. BioMed Res. Int. 2019, 2019, 7341841. [Google Scholar] [CrossRef] [PubMed]
- Ahmadian, L.; Khajouei, R.; Nejad, S.S.; Ebrahimzadeh, M.; Nikkar, S. Prioritizing barriers to successful implementation of hospital information systems. J. Med. Syst. 2014, 38, 151. [Google Scholar] [CrossRef]
- Luna, D.; Almerares, A.; Mayan, J.C.; Gonzalez Bernaldo de Quiros, F.; Otero, C. Health informatics in developing countries: Going beyond pilot practices to sustainable implementations: A review of the current challenges. Healthc Inform Res. 2014, 20, 3–10. [Google Scholar] [CrossRef]
- Ohuabunwa, E.C.; Sun, J.; Jubanyik, K.J.; Wallis, L. Electronic Medical Records in low to middle income countries: The case of Khayelitsha Hospital, South Africa. Afr. J. Emerg. Med. 2016, 6, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Marutha, N.S.; Ngulube, P. Electronic records management in the public health sector of the Limpopo province in South Africa. Inform. Dev. 2012, 45, 39–67. [Google Scholar]
- Kgasi, M.; Kalema, B. Assessment E-health readiness for rural South African areas. J. Ind. Intell. Inf. 2014, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Skiti, V. Qualitative Assessment of the Utilisation of Tier.Net Health Information among facility and programme managers In Ekurhuleni district, Gauteng. Available online: http://hdl.handle.net/11394/5942 (accessed on 15 May 2020).



{kind=link}
{kind=link}
| EHIS Component | Function | Benefit to Patient Care |
|---|---|---|
| Patient Management EHIS | Patient registration, admission, transfer and discharge (ADT) functionality. Patient registration includes key patient information such as demographics, insurance information and contact information [14] | Populations and their needs are analyzed at a point of care to determine the services to be rendered to them [15] |
| Activity EHIS | Flow processed from when a client is entering the point of service till data is digitized on the system [15,16] | Traceability of health data |
| Clinical EHIS | Habitation of multiple sub-components, e.g., computerized provide order entry (CPOE), electronic documentation, nursing component [14] | Electronic clinical documentation systems enhance the value of EHRs by providing electronic capture of clinical notes; patient assessments; and clinical reports, such as medication administration records (MAR) [13] |
| Pharmacy EHIS | Islands of automation, such as pharmacy robots for filling prescriptions or payer formularies, that typically are not integrated with EHRs [13] | Improve efficiency of pharmacy services |
| Laboratory EHIS | Consists of two subcomponents: capturing results from lab machines; and integration with orders, billing and lab machines. The lab component may either be integrated with the EHR or exist as a standalone product [14,17] | Improve efficiency of pathology laboratory services |
| Radiology Information System and Picture Archiving & Communications System (PACS) | Manages patient workflow, ordering process and results [14] | Enables improved service delivery |
| The billing system (hospital and professional billing) | Captures all charges generated in the process of taking care of patients. These charges generate claims, which are subsequently submitted to insurance companies, tracked and completed [14] | Tracking of patient data and quality assurance |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khubone, T.; Tlou, B.; Mashamba-Thompson, T.P. Electronic Health Information Systems to Improve Disease Diagnosis and Management at Point-of-Care in Low and Middle Income Countries: A Narrative Review. Diagnostics 2020, 10, 327. https://doi.org/10.3390/diagnostics10050327
Khubone T, Tlou B, Mashamba-Thompson TP. Electronic Health Information Systems to Improve Disease Diagnosis and Management at Point-of-Care in Low and Middle Income Countries: A Narrative Review. Diagnostics. 2020; 10(5):327. https://doi.org/10.3390/diagnostics10050327
Chicago/Turabian StyleKhubone, Thokozani, Boikhutso Tlou, and Tivani Phosa Mashamba-Thompson. 2020. "Electronic Health Information Systems to Improve Disease Diagnosis and Management at Point-of-Care in Low and Middle Income Countries: A Narrative Review" Diagnostics 10, no. 5: 327. https://doi.org/10.3390/diagnostics10050327