Diagnosis of Hourglass-Like Constriction Neuropathy of the Radial Nerve Using High-Resolution Magnetic Resonance Neurography: A Report of Two Cases


Abstract
:1. Introduction
2. Case Presentation
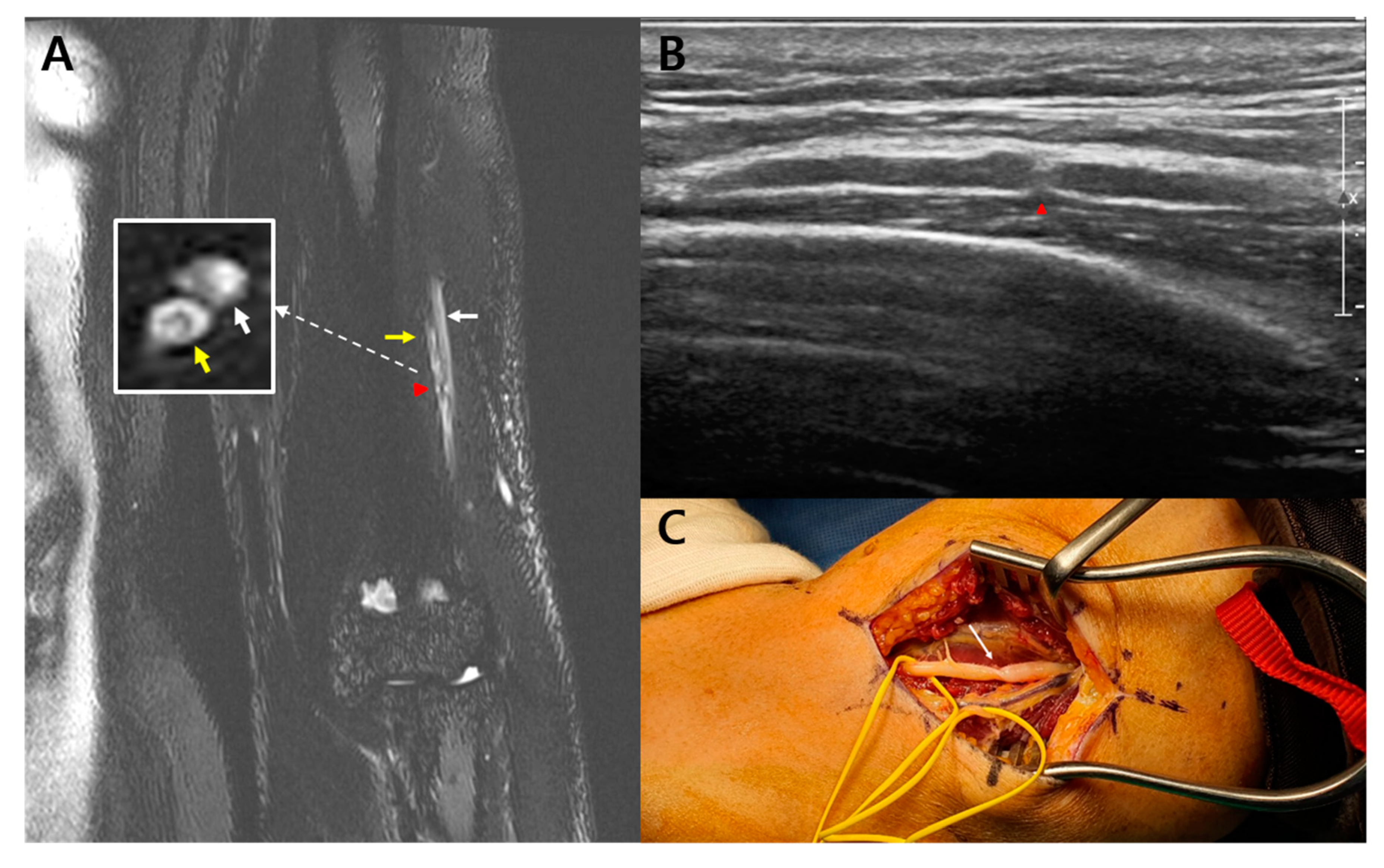
2.1. Patient 1
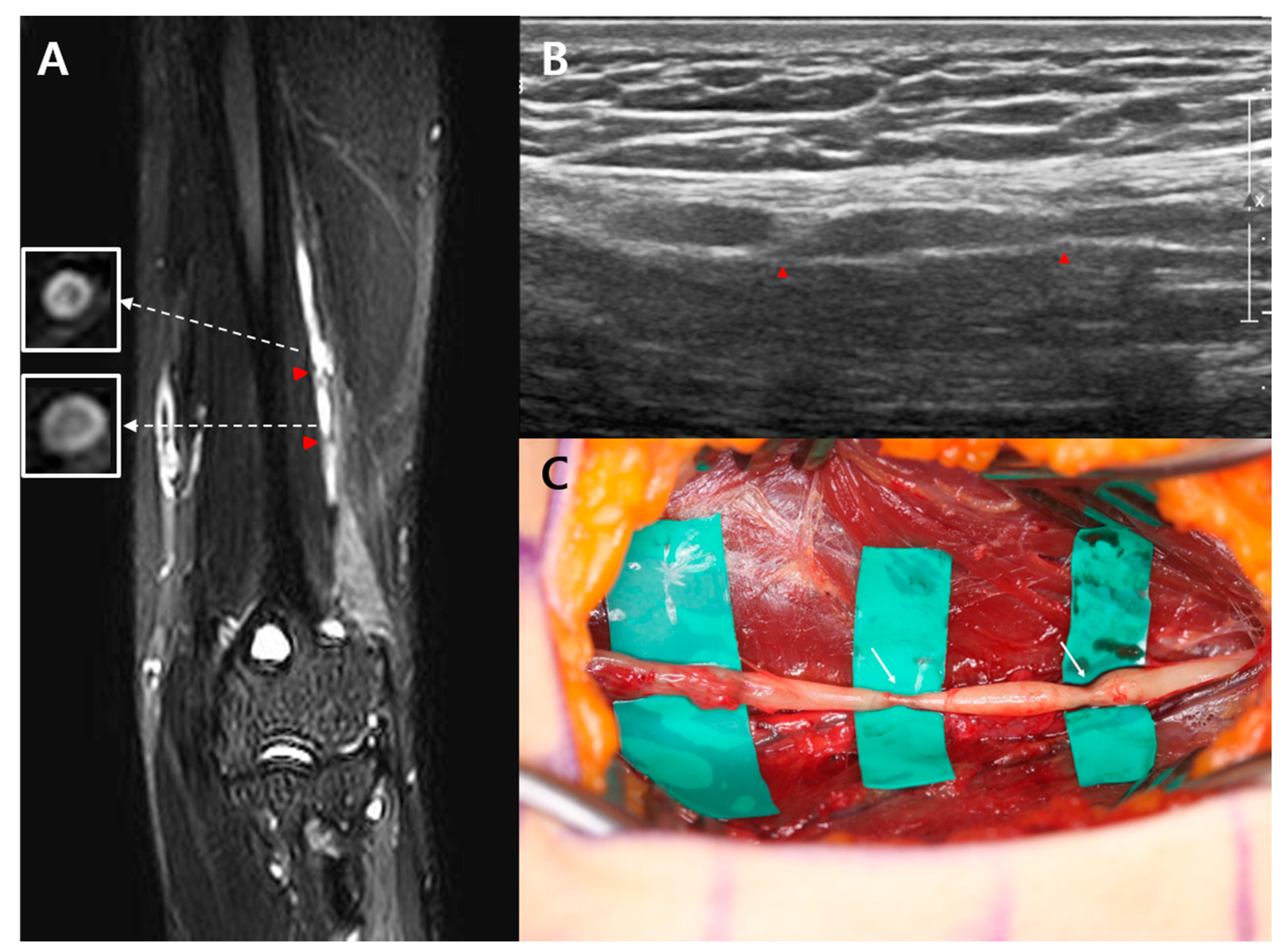
2.2. Patient 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kim, D.H.; Kim, J.; Sung., D.H. Hourglass-like constriction neuropathy of the suprascapular nerve detected by high-resolution magnetic resonance neurography: Report of three patients. Skeletal Radiol 2019, 48, 1451–1456. [Google Scholar] [CrossRef] [PubMed]
- Loizides, A.; Baur, E.M.; Plaikner, M.; Gruber, H. Triple hourglass-like fascicular constriction of the posterior interosseous nerve: a rare cause of PIN syndrome. Arch. Orthop. Trauma Surg. 2015, 135, 635–637. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, T.; Song, L.; Zhang, Z.; Zhang, Y.; Ni, J.; Lu, L. Spontaneous peripheral nerve palsy with hourglass-like fascicular constriction in the upper extremity. J. Neurosurg. 2019, 131, 1876–1886. [Google Scholar] [CrossRef] [PubMed]
- Arányi, Z.; Csillik, A.; Dévay, K.; Rosero, M.; Barsi, P.; Böhm, J.; Schelle, T. Ultrasonographic identification of nerve pathology in neuralgic amyotrophy: enlargement, constriction, ascicular entwinement, and torsion. Muscle Nerve 2015, 52, 503–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ArÁnyi, Z.; Csillik, A.; DéVay, K.; Rosero, M.; Barsi, P.; BÖhm, J.; Schelle, T. Ultrasonography in neuralgic myotrophy: sensitivity, spectrum of findings, and clinical correlations. Muscle Nerve 2017, 56, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Sneag, D.B.; Saltzman, E.B.; Meister, D.W.; Feinberg, J.H.; Lee, S.K.; Wolfe, S.W. MRI Bullseye sign: An indicator of peripheral nerve constriction in parsonage-turner syndrome. Muscle Nerve 2017, 56, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Yoneyama, M.; Takahara, T.; Kwee, T.C.; Nakamura, M.; Tabuchi, T. Rapid high resolution MR neurography with a diffusion-weighted pre-pulse. Magn. Reson. Med. Sci. 2013, 12, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasper, J.M.; Wadhwa, V.; Scott, K.M.; Rozen, S.; Xi, Y.; Chhabra, A. SHINKEI--a novel 3D isotropic MR neurography technique: technical advantages over 3DIRTSE-based imaging. Eur. Radiol. 2015, 25, 1672–1677. [Google Scholar] [CrossRef] [PubMed]
- Sneag, D.B.; Rancy, S.K.; Wolfe, S.W.; Lee, S.C.; Kalia, V.; Lee, S.K.; Feinberg, J.H. Brachial plexitis or neuritis? MRI features of lesion distribution in Parsonage–Turner syndrome. Muscle Nerve 2018, 58, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Latef, T.J.; Bilal, M.; Vetter, M.; Iwanaga, J.; Oskouian, R.J.; Tubbs, R.S. Injury of the Radial Nerve in the Arm: A Review. Cureus 2018, 10, e2199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, M.C. Neuralgic amyotrophy in the lower extremity diagnosed with gadolinium-enhanced lumbar magnetic resonance imaging: A case report. Neurology Asia 2017, 22, 377–379. [Google Scholar]
- Van Alfen, N.; van Eijk, J.J.; Ennik, T.; Flynn, S.O.; Nobacht, I.E.G.; Groothuis, J.T.; Pillen, S.; van de Laar, F.A. Incidence of neuralgic amyotrophy (parsonage turner syndrome) in a primary care setting—A prospective cohort study. PLoS ONE 2015, 10, e0128361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieba-Samal, D.; Jengojan, S.; Kasprian, G.; Wöber, C.; Bodner, G. Neuroimaging of classic neuralgic amyotrophy. Muscle Nerve 2016, 54, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Noda, Y.; Sekiguchi, K.; Tokuoka, H.; Oda, T.; Hamaguchi, H.; Kanda, F.; Toda, T. Ultrasonographic findings of proximal median neuropathy: A case series of suspected distal neuralgic amyotrophy. J. Neurol. Sci. 2017, 377, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Van Rosmalen, M.; Lieba-Samal, D.; Pillen, S.; van Alfen, N. Ultrasound of peripheral nerves in neuralgic amyotrophy. Muscle Nerve 2019, 59, 55–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vigasio, A.; Marcoccio, I. Homolateral hourglass-like constrictions of the axillary and suprascapular nerves: case report. J. Hand Surg. Am. 2009, 34, 1815–1820. [Google Scholar] [CrossRef] [PubMed]
- Bäumer, P.; Kele, H.; Xia, A.; Weiler, M.; Schwarz, D.; Bendszus, M.; Pham, M. Posterior interosseous neuropathy: Supinator syndrome vs fascicular radial neuropathy. Neurology 2016, 87, 1884–1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGraw, I. Isolated spontaneous posterior interosseous nerve palsy: a review of aetiology and management. J. Hand Surg. Eur. Vol. 2019, 44, 310–316. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author, Year | Evaluation Tool | Summary |
|---|---|---|
| Van Rosmalen, 2019 [15] | US | 51 patients with NA (upper limb) vs. 50 control subjects Increased cross-sectional areas in the affected nerves. |
| Kim, 2019 [1] | MRN | 2 patients with SSN and 1 patient with SSN + RN Single focal constriction, multiple focal constrictions, diffuse swelling, and increased signal intensity |
| Sneag, 2018 [9] | MRN | 27 patients with NA in the brachial plexus Focal intrinsic constrictions (32 of 38 nerves) Bull’s eye sign |
| Sneag, 2017 [6] | MRN | 6 patients with NA SSN, AN, RN, AIN |
| Arányi, 2017 [5] | US | 53 patients with NA with 70 affected nerves AIN (23%), RN (17%), LTN (17%), SSN (11%), accessory nerve (9%), and AN (7%) Sensitivity of US: 74% Swelling without constriction, incomplete constriction, complete constriction |
| Noda, 2017 [14] | US | 6 patients with segmental swelling (larger cross-sectional diameter) Involved nerves: LTN, SN, MN, MCN, and PIN |
| Lieba-samal, 2016 [13] | US | 4 patients with distal NA in AIN Swelling or hypertrophy of the involved nerves. |
| Arányi, 2015 [4] | US | 14 patients with NA RN, PIN, AIN, SSN, MCN, LTN, MCN, and AN Four types of abnormalities: (1) focal or diffuse nerve/fascicle enlargement; (2) incomplete nerve constriction; (3) complete nerve constriction with torsion (hourglass-like appearance); and (4) fascicular entwinement. The types of abnormalities had no correlation with the prognosis. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.H.; Sung, D.H.; Chang, M.C. Diagnosis of Hourglass-Like Constriction Neuropathy of the Radial Nerve Using High-Resolution Magnetic Resonance Neurography: A Report of Two Cases. Diagnostics 2020, 10, 232. https://doi.org/10.3390/diagnostics10040232
Kim DH, Sung DH, Chang MC. Diagnosis of Hourglass-Like Constriction Neuropathy of the Radial Nerve Using High-Resolution Magnetic Resonance Neurography: A Report of Two Cases. Diagnostics. 2020; 10(4):232. https://doi.org/10.3390/diagnostics10040232
Chicago/Turabian StyleKim, Du Hwan, Duk Hyun Sung, and Min Cheol Chang. 2020. "Diagnosis of Hourglass-Like Constriction Neuropathy of the Radial Nerve Using High-Resolution Magnetic Resonance Neurography: A Report of Two Cases" Diagnostics 10, no. 4: 232. https://doi.org/10.3390/diagnostics10040232