Diagnostic Accuracy of Oral Fluids Biomarker Profile to Determine the Current and Future Status of Periodontal and Peri-Implant Diseases



Abstract
:1. Introduction
2. Diagnosis of Periodontal Diseases
3. Limitations of Traditional Methods for Diagnosis
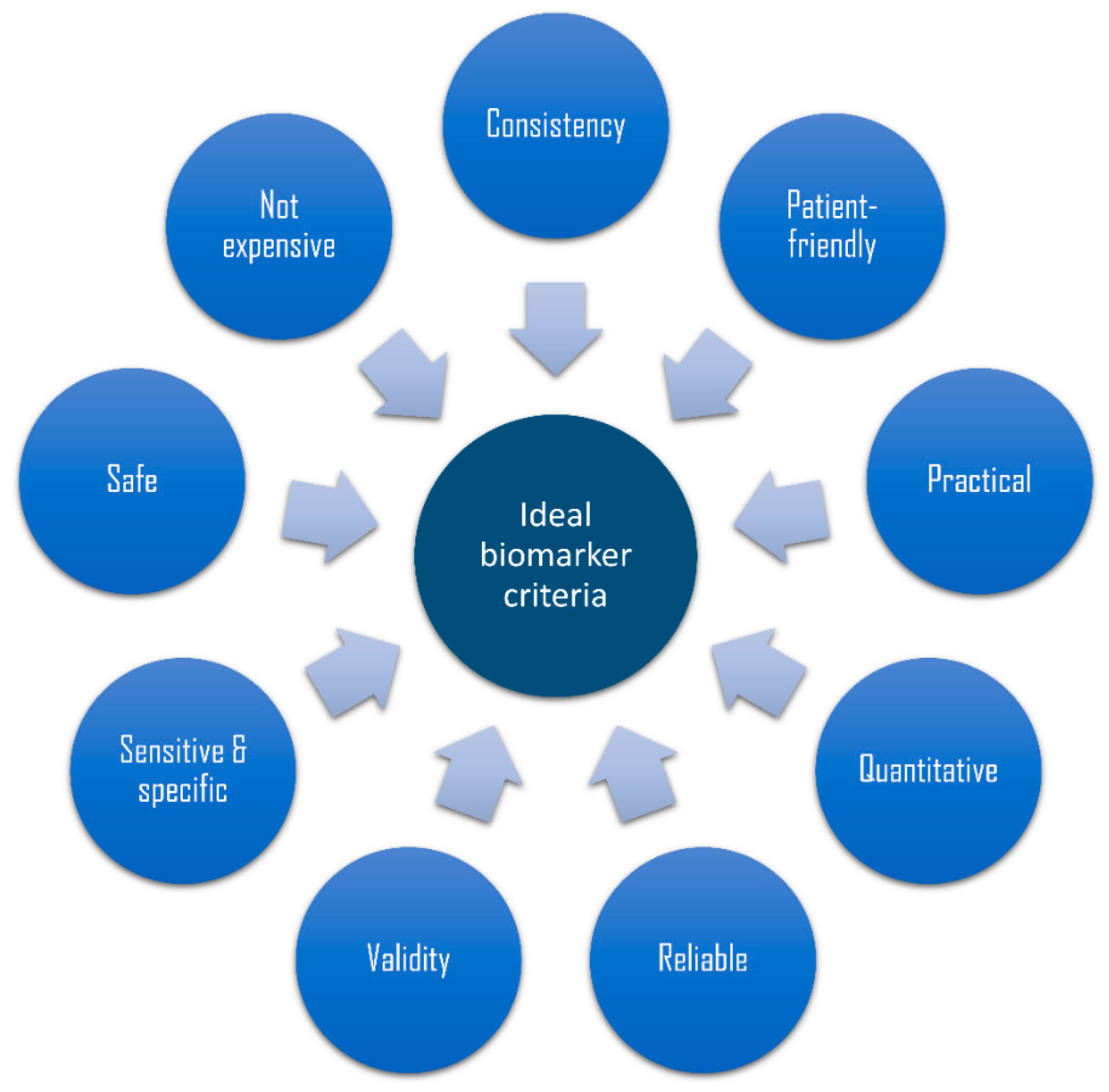
4. Need for Alternative Methods with Diagnostic and Prognostic Potential, Such as Use of Biomarkers
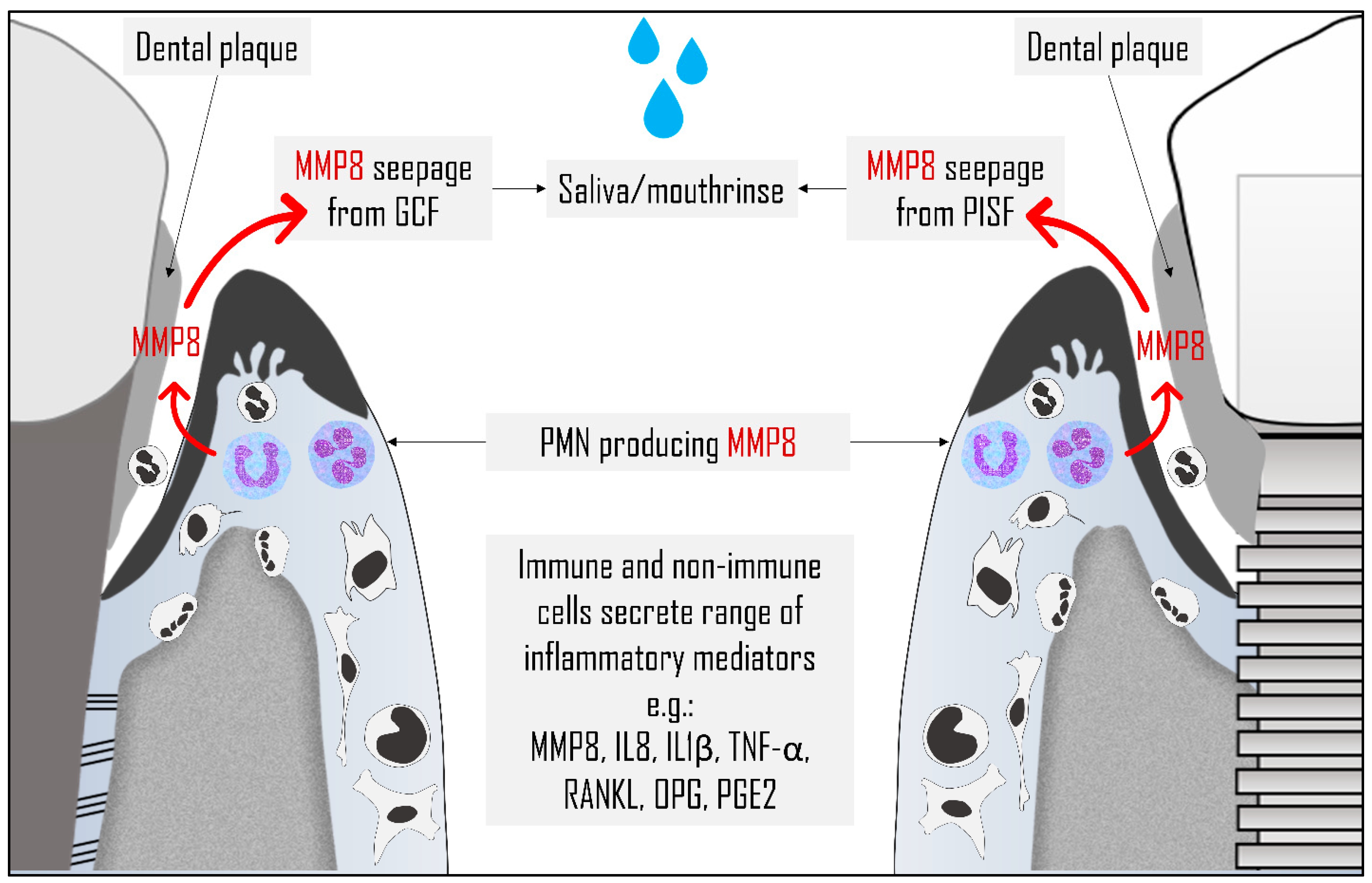
5. Sources of Biomarkers of Periodontal Disease in the Oral Cavity
6. Potential Biomarkers of Periodontal Diseases
6.1. IL1β
6.2. IL6
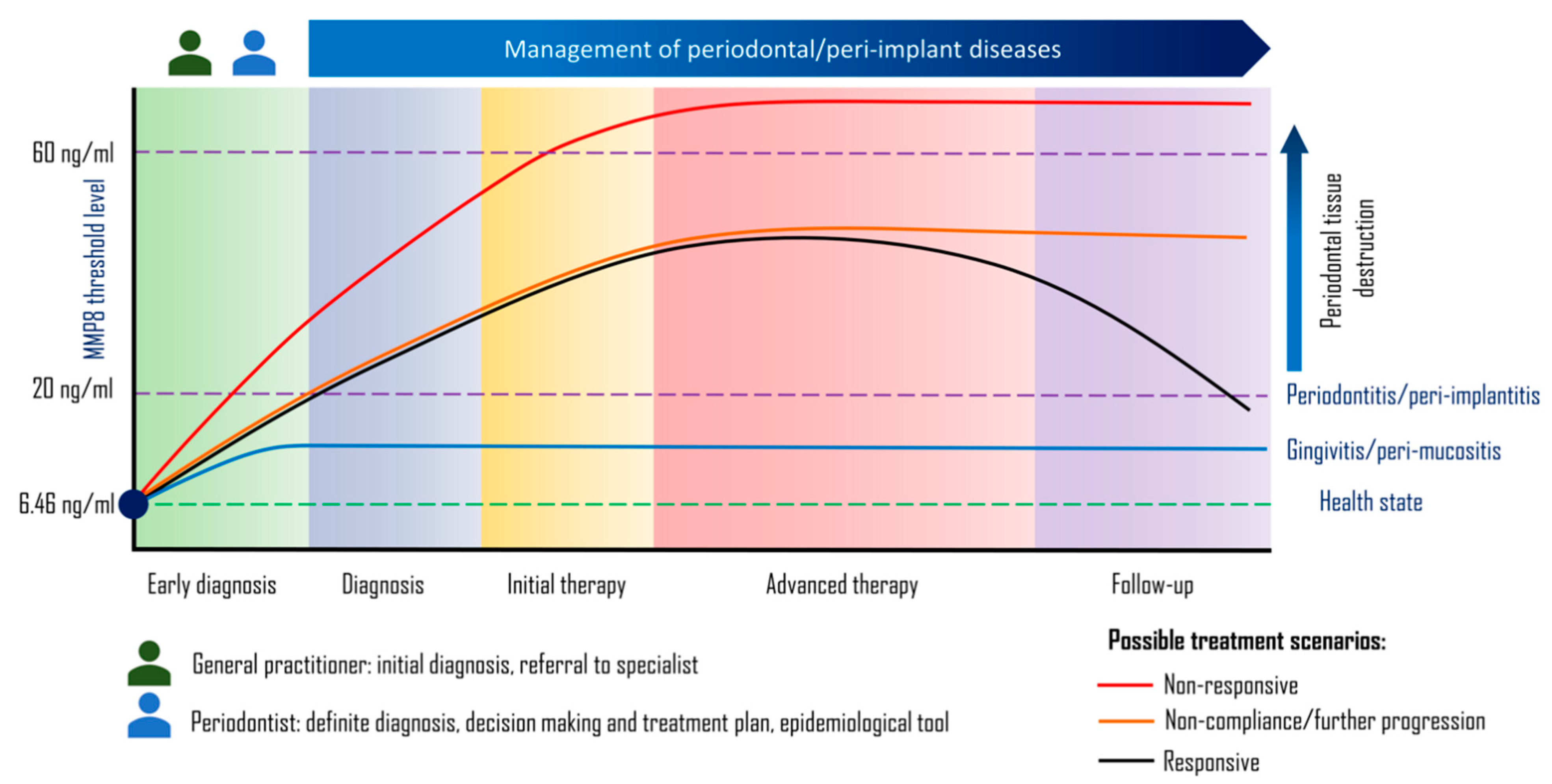
6.3. MMP8
6.4. Single vs Combination of Biomarkers
7. Detection Methods for Biomarkers in Periodontal Diseases
8. Periodontal Point-of-Care Test Kits
8.1. Microbiological Test Kits
8.2. Biochemical Test Kits
8.3. Genetic Test Kits
9. Clinical Implications and Challenges
10. Conclusions and Future Direction
Author Contributions
Funding
Conflicts of Interest
References
- Könönen, E.; Gursoy, M.; Gursoy, U.K. Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J. Clin. Med. 2019, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aral, C.A.; Kesim, S.; Greenwell, H.; Kara, M.; Çetin, A.; Yakan, B. Alveolar bone protective and hypoglycemic effects of systemic propolis treatment in experimental periodontitis and diabetes mellitus. J. Med. Food 2015, 18, 195–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genco, R.J.; Borgnakke, W.S. Diabetes as a potential risk for periodontitis: Association studies. Periodontol. 2000 2020, 83, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Molina, A.; Buhlin, K.; Klinge, B. Periodontal diseases and association with atherosclerotic disease. Periodontol. 2000 2020, 83, 66–89. [Google Scholar] [CrossRef]
- Nwizu, N.; Wactawski-Wende, J.; Genco, R.J. Periodontal disease and cancer: Epidemiologic studies and possible mechanisms. Periodontol. 2000 2020, 83, 213–233. [Google Scholar] [CrossRef]
- Dioguardi, M.; Gioia, G.D.; Caloro, G.A.; Capocasale, G.; Zhurakivska, K.; Troiano, G.; Russo, L.L.; Muzio, L.L. The Association between Tooth Loss and Alzheimer’s Disease: A Systematic Review with Meta-Analysis of Case Control Studies. Dent. J. 2019, 7, 49. [Google Scholar] [CrossRef] [Green Version]
- Murakami, S.; Mealey, B.L.; Mariotti, A.; Chapple, I.L.C. Dental plaque-induced gingival conditions. J. Periodontol. 2018, 89 (Suppl. 1), S17–S27. [Google Scholar] [CrossRef] [Green Version]
- Mendis, S.; Davis, S.; Norrving, B. Organizational update: The world health organization global status report on noncommunicable diseases 2014; one more landmark step in the combat against stroke and vascular disease. Stroke 2015, 46, e121–e122. [Google Scholar] [CrossRef]
- Marcenes, W.; Kassebaum, N.J.; Bernabé, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.J. Global burden of oral conditions in 1990–2010: A systematic analysis. J. Dent. Res. 2013, 92, 592–597. [Google Scholar] [CrossRef] [Green Version]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of severe periodontitis in 1990–2010: A systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef]
- Jin, L.J.; Lamster, I.B.; Greenspan, J.S.; Pitts, N.B.; Scully, C.; Warnakulasuriya, S. Global burden of oral diseases: Emerging concepts, management and interplay with systemic health. Oral Dis. 2016, 22, 609–619. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Buset, S.L.; Walter, C.; Friedmann, A.; Weiger, R.; Borgnakke, W.S.; Zitzmann, N.U. Are periodontal diseases really silent? A systematic review of their effect on quality of life. J. Clin. Periodontol. 2016, 43, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Lang, N.P. The diagnosis and treatment of peri-implantitis. Periodontol. 2000 1998, 17, 63–76. [Google Scholar] [CrossRef] [PubMed]
- McCrea, S.J. Advanced peri-implantitis cases with radical surgical treatment. J. Periodontal Implant. Sci. 2014, 44, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Mombelli, A.; Müller, N.; Cionca, N. The epidemiology of peri-implantitis. Clin. Oral Implants Res. 2012, 23 (Suppl. 6), 67–76. [Google Scholar] [CrossRef]
- Faveri, M.; Figueiredo, L.C.; Shibli, J.A.; Pérez-Chaparro, P.J.; Feres, M. Microbiological diversity of peri-implantitis biofilms. Adv. Exp. Med. Biol. 2015, 830, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L. Time to take periodontitis seriously. BMJ 2014, 348, g2645. [Google Scholar] [CrossRef]
- Listl, S.; Galloway, J.; Mossey, P.A.; Marcenes, W. Global Economic Impact of Dental Diseases. J. Dent. Res. 2015, 94, 1355–1361. [Google Scholar] [CrossRef] [PubMed]
- Mahato, N.; Wu, X.; Wang, L. Management of peri-implantitis: A systematic review, 2010–2015. SpringerPlus 2016, 5, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mombelli, A. Critical issues in periodontal diagnosis. Periodontol. 2000 2005, 39, 9–12. [Google Scholar] [CrossRef]
- Jenkins, W.M.; MacFarlane, T.W.; Gilmour, W.H. Longitudinal study of untreated periodontitis (I). Clinical findings. J. Clin. Periodontol. 1988, 15, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.J.; Oliver, R.C.; Löe, H. Periodontal diseases in the U.S. in 1981: Prevalence, severity, extent, and role in tooth mortality. J. Periodontol. 1989, 60, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Van der Velden, U.; Abbas, F.; Van Steenbergen, T.J.; De Zoete, O.J.; Hesse, M.; De Ruyter, C.; De Laat, V.H.; De Graaff, J. Prevalence of periodontal breakdown in adolescents and presence of Actinobacillus actinomycetemcomitans in subjects with attachment loss. J. Periodontol. 1989, 60, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C. Diagnosis of periodontal diseases. J. Periodontol. 2003, 74, 1237–1247. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S1–S8. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S149–S161. [Google Scholar] [CrossRef] [Green Version]
- Coli, P.; Christiaens, V.; Sennerby, L.; Bruyn, H.D. Reliability of periodontal diagnostic tools for monitoring peri-implant health and disease. Periodontol. 2000 2017, 73, 203–217. [Google Scholar] [CrossRef]
- Lang, N.P.; Joss, A.; Orsanic, T.; Gusberti, F.A.; Siegrist, B.E. Bleeding on probing. A predictor for the progression of periodontal disease? J. Clin. Periodontol. 1986, 13, 590–596. [Google Scholar] [CrossRef]
- Andrade, R.; Espinoza, M.; Gómez, E.M.; Rolando Espinoza, J.; Cruz, E. Intra- and inter-examiner reproducibility of manual probing depth. Braz. Oral Res. 2012, 26, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Lafzi, A.; Mohammadi, A.S.; Eskandari, A.; Pourkhamneh, S. Assessment of Intra- and Inter-examiner Reproducibility of Probing Depth Measurements with a Manual Periodontal Probe. J. Dent. Res. Dent. Clin. Dent. Prospects 2007, 1, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Goodson, J.M. Diagnosis of periodontitis by physical measurement: Interpretation from episodic disease hypothesis. J. Periodontol. 1992, 63, 373–382. [Google Scholar] [CrossRef]
- Jeffcoat, M.K. Radiographic methods for the detection of progressive alveolar bone loss. J. Periodontol. 1992, 63, 367–372. [Google Scholar] [CrossRef]
- Taba, M., Jr.; Kinney, J.; Kim, A.S.; Giannobile, W.V. Diagnostic biomarkers for oral and periodontal diseases. Dent. Clin. North. Am. 2005, 49, 551–571. [Google Scholar] [CrossRef] [Green Version]
- Serino, G.; Turri, A.; Lang, N.P. Probing at implants with peri-implantitis and its relation to clinical peri-implant bone loss. Clin. Oral Implants Res. 2013, 24, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Coli, P.; Sennerby, L. Is Peri-Implant Probing Causing Over-Diagnosis and Over-Treatment of Dental Implants? J. Clin. Med. 2019, 8, 1123. [Google Scholar] [CrossRef] [PubMed]
- Schou, S.; Holmstrup, P.; Stoltze, K.; Hjørting-Hansen, E.; Fiehn, N.E.; Skovgaard, L.T. Probing around implants and teeth with healthy or inflamed peri-implant mucosa/gingiva. A histologic comparison in cynomolgus monkeys (Macaca fascicularis). Clin. Oral Implants Res. 2002, 13, 113–126. [Google Scholar] [CrossRef]
- He, W.; You, M.; Wan, W.; Xu, F.; Li, F.; Li, A. Point-of-Care Periodontitis Testing: Biomarkers, Current Technologies, and Perspectives. Trends Biotechnol. 2018, 36, 1127–1144. [Google Scholar] [CrossRef]
- Dietrich, T.; Ower, P.; Tank, M.; West, N.X.; Walter, C.; Needleman, I.; Hughes, F.J.; Wadia, R.; Milward, M.R.; Hodge, P.J.; et al. Periodontal diagnosis in the context of the 2017 classification system of periodontal diseases and conditions—implementation in clinical practice. Br. Dent. J. 2019, 226, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Sorsa, T.; Alassiri, S.; Grigoriadis, A.; Räisänen, I.T.; Pärnänen, P.; Nwhator, S.O.; Gieselmann, D.R.; Sakellari, D. Active MMP-8 (aMMP-8) as a Grading and Staging Biomarker in the Periodontitis Classification. Diagnostics (Basel) 2020, 10. [Google Scholar] [CrossRef] [Green Version]
- Heikkinen, A.M.; Nwhator, S.O.; Rathnayake, N.; Mäntylä, P.; Vatanen, P.; Sorsa, T. Pilot Study on Oral Health Status as Assessed by an Active Matrix Metalloproteinase-8 Chairside Mouthrinse Test in Adolescents. J. Periodontol. 2016, 87, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Rathnayake, N.; Gieselmann, D.R.; Heikkinen, A.M.; Tervahartiala, T.; Sorsa, T. Salivary Diagnostics-Point-of-Care diagnostics of MMP-8 in dentistry and medicine. Diagnostics 2017, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sackmann, E.K.; Fulton, A.L.; Beebe, D.J. The present and future role of microfluidics in biomedical research. Nature 2014, 507, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.J.; Preshaw, P.M. Gingival crevicular fluid and saliva. Periodontol. 2000 2016, 70, 7–10. [Google Scholar] [CrossRef]
- Pradeep, A.R.; Daisy, H.; Hadge, P.; Garg, G.; Thorat, M. Correlation of gingival crevicular fluid interleukin-18 and monocyte chemoattractant protein-1 levels in periodontal health and disease. J. Periodontol. 2009, 80, 1454–1461. [Google Scholar] [CrossRef]
- Griffiths, G.S. Formation, collection and significance of gingival crevice fluid. Periodontol. 2000 2003, 31, 32–42. [Google Scholar] [CrossRef]
- Subbarao, K.C.; Nattuthurai, G.S.; Sundararajan, S.K.; Sujith, I.; Joseph, J.; Syedshah, Y.P. Gingival Crevicular Fluid: An Overview. J. Pharm. Bioallied Sci. 2019, 11, S135–S139. [Google Scholar] [CrossRef]
- Pradeep, A.R.; Daisy, H.; Hadge, P. Gingival crevicular fluid levels of monocyte chemoattractant protein-1 in periodontal health and disease. Arch. Oral Biol. 2009, 54, 503–509. [Google Scholar] [CrossRef]
- Pradeep, A.R.; Raghavendra, N.M.; Prasad, M.V.; Kathariya, R.; Patel, S.P.; Sharma, A. Gingival crevicular fluid and serum visfatin concentration: Their relationship in periodontal health and disease. J. Periodontol. 2011, 82, 1314–1319. [Google Scholar] [CrossRef]
- Nazar Majeed, Z.; Philip, K.; Alabsi, A.M.; Pushparajan, S.; Swaminathan, D. Identification of Gingival Crevicular Fluid Sampling, Analytical Methods, and Oral Biomarkers for the Diagnosis and Monitoring of Periodontal Diseases: A Systematic Review. Dis. Markers 2016, 2016, 1804727. [Google Scholar] [CrossRef] [Green Version]
- Malamud, D. Saliva as a diagnostic fluid. Dent. Clin. North. Am. 2011, 55, 159–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izawa, S.; Sugaya, N.; Kimura, K.; Ogawa, N.; Yamada, K.C.; Shirotsuki, K.; Mikami, I.; Hirata, K.; Nagano, Y.; Nomura, S. An increase in salivary interleukin-6 level following acute psychosocial stress and its biological correlates in healthy young adults. Biol. Psychol. 2013, 94, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Bhattarai, K.R.; Kim, H.R.; Chae, H.J. Compliance with Saliva Collection Protocol in Healthy Volunteers: Strategies for Managing Risk and Errors. Int. J. Med. Sci. 2018, 15, 823–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srivastava, N.; Nayak, P.A.; Rana, S. Point of Care- A Novel Approach to Periodontal Diagnosis-A Review. J. Clin. Diagn. Res. 2017, 11, Ze01–ze06. [Google Scholar] [CrossRef]
- Johnson, N.; Ebersole, J.L.; Kryscio, R.J.; Danaher, R.J.; Dawson, D., 3rd; Al-Sabbagh, M.; Miller, C.S. Rapid assessment of salivary MMP-8 and periodontal disease using lateral flow immunoassay. Oral Dis. 2016, 22, 681–687. [Google Scholar] [CrossRef] [Green Version]
- Group, B.D.W. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef]
- Parikh, R.; Mathai, A.; Parikh, S.; Chandra Sekhar, G.; Thomas, R. Understanding and using sensitivity, specificity and predictive values. Indian, J. Ophthalmol. 2008, 56, 45–50. [Google Scholar] [CrossRef]
- Takeuchi, O.; Akira, S. Pattern recognition receptors and inflammation. Cell 2010, 140, 805–820. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.; Chu, W.M.; Zhu, J.; Wu, Y.N.; Wang, Z.L. Interleukin-1β (3953/4) C→T polymorphism increases the risk of chronic periodontitis in Asians: Evidence from a meta-analysis of 20 case-control studies. Arch. Med. Sci. 2015, 11, 267–273. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Smith, C.; Duff, G.W. Microbiological parameters associated with IL-1 gene polymorphisms in periodontitis patients. J. Clin. Periodontol. 2000, 27, 810–818. [Google Scholar] [CrossRef]
- Mesa, F.; Lanza, E.; García, L.; Marfil-Alvarez, R.; Magan-Fernandez, A. Polymorphism IL-1RN rs419598 reduces the susceptibility to generalized periodontitis in a population of European descent. PLoS ONE 2017, 12, e0186366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, K.; Jian, F.; He, T.; Tang, H.; Huang, B.; Wei, N. Analysis of the association of TNF-α, IL-1A, and IL-1B polymorphisms with peri-implantitis in a Chinese non-smoking population. Clin. Oral Investig. 2020, 24, 693–699. [Google Scholar] [CrossRef]
- Offenbacher, S.; Barros, S.P.; Singer, R.E.; Moss, K.; Williams, R.C.; Beck, J.D. Periodontal disease at the biofilm-gingival interface. J. Periodontol. 2007, 78, 1911–1925. [Google Scholar] [CrossRef] [PubMed]
- Kinney, J.S.; Morelli, T.; Oh, M.; Braun, T.M.; Ramseier, C.A.; Sugai, J.V.; Giannobile, W.V. Crevicular fluid biomarkers and periodontal disease progression. J. Clin. Periodontol. 2014, 41, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaushik, R.; Yeltiwar, R.K.; Pushpanshu, K. Salivary interleukin-1β levels in patients with chronic periodontitis before and after periodontal phase I therapy and healthy controls: A case-control study. J. Periodontol. 2011, 82, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.S.; King, C.P., Jr.; Langub, M.C.; Kryscio, R.J.; Thomas, M.V. Salivary biomarkers of existing periodontal disease: A cross-sectional study. J. Am. Dent. Assoc. 2006, 137, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Reinhardt, R.A.; Stoner, J.A.; Golub, L.M.; Lee, H.M.; Nummikoski, P.V.; Sorsa, T.; Payne, J.B. Association of gingival crevicular fluid biomarkers during periodontal maintenance with subsequent progressive periodontitis. J. Periodontol. 2010, 81, 251–259. [Google Scholar] [CrossRef]
- Kajale, A.M.; Mehta, D.S. Interleukin-1β level in peri-implant crevicular fluid and its correlation with the clinical and radiographic parameters. J. Indian Soc. Periodontol. 2014, 18, 220–225. [Google Scholar] [CrossRef]
- Al-Askar, M.; Ajlan, S.; Alomar, N.; Al-Daghri, N.M. Clinical and Radiographic Peri-Implant Parameters and Whole Salivary Interleukin-1β and Interleukin-6 Levels among Type-2 Diabetic and Nondiabetic Patients with and without Peri-Implantitis. Med. Princ. Pract. 2018, 27, 133–138. [Google Scholar] [CrossRef]
- Yaghobee, S.; Khorsand, A.; Rasouli Ghohroudi, A.A.; Sanjari, K.; Kadkhodazadeh, M. Assessment of interleukin-1beta and interleukin-6 in the crevicular fluid around healthy implants, implants with peri-implantitis, and healthy teeth: A cross-sectional study. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 220–224. [Google Scholar] [CrossRef] [Green Version]
- Gabay, C. Interleukin-6 and chronic inflammation. Arthritis Res. Ther. 2006, 8 (Suppl. 2), S3. [Google Scholar] [CrossRef] [Green Version]
- Stadler, A.F.; Angst, P.D.; Arce, R.M.; Gomes, S.C.; Oppermann, R.V.; Susin, C. Gingival crevicular fluid levels of cytokines/chemokines in chronic periodontitis: A meta-analysis. J. Clin. Periodontol. 2016, 43, 727–745. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Guo, B.; Fu, M.; Guo, W.; Yuan, Y.; Yuan, H.; Zhang, S.; Yu, H. Interleukin-6-174G/C Polymorphism Contributes to Periodontitis Susceptibility: An Updated Meta-Analysis of 21 Case-Control Studies. Dis. Markers 2016, 2016, 9612421. [Google Scholar] [CrossRef] [PubMed]
- Batool, H.; Nadeem, A.; Kashif, M.; Shahzad, F.; Tahir, R.; Afzal, N. Salivary Levels of IL-6 and IL-17 Could Be an Indicator of Disease Severity in Patients with Calculus Associated Chronic Periodontitis. Biomed. Res. Int. 2018, 2018, 8531961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, V.; Mesquita, M.F.; Bernardo, M.A.; Casal, E.; Proença, L.; Mendes, J.J. IL-6 and TNF-α salivary levels according to the periodontal status in Portuguese pregnant women. PeerJ 2018, 6, e4710. [Google Scholar] [CrossRef]
- Syrjäläinen, S.; Gursoy, U.K.; Gursoy, M.; Pussinen, P.; Pietiäinen, M.; Jula, A.; Salomaa, V.; Jousilahti, P.; Könönen, E. Salivary Cytokine Biomarker Concentrations in Relation to Obesity and Periodontitis. J. Clin. Med. 2019, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtiş, B.; Develioğlu, H.; Taner, I.L.; Baloş, K.; Tekin, I.O. IL-6 levels in gingival crevicular fluid (GCF) from patients with non-insulin dependent diabetes mellitus (NIDDM), adult periodontitis and healthy subjects. J. Oral Sci. 1999, 41, 163–167. [Google Scholar] [CrossRef]
- Sorsa, T.; Tjäderhane, L.; Salo, T. Matrix metalloproteinases (MMPs) in oral diseases. Oral Dis. 2004, 10, 311–318. [Google Scholar] [CrossRef]
- Sorsa, T.; Gursoy, U.K.; Nwhator, S.; Hernandez, M.; Tervahartiala, T.; Leppilahti, J.; Gursoy, M.; Könönen, E.; Emingil, G.; Pussinen, P.J.; et al. Analysis of matrix metalloproteinases, especially MMP-8, in gingival creviclular fluid, mouthrinse and saliva for monitoring periodontal diseases. Periodontol. 2000 2016, 70, 142–163. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Mäntylä, P.; Tervahartiala, T.; Pussinen, P.J.; Gamonal, J.; Hernandez, M. MMP activation in diagnostics of periodontitis and systemic inflammation. J. Clin. Periodontol. 2011, 38, 817–819. [Google Scholar] [CrossRef]
- Sorsa, T.; Hernández, M.; Leppilahti, J.; Munjal, S.; Netuschil, L.; Mäntylä, P. Detection of gingival crevicular fluid MMP-8 levels with different laboratory and chair-side methods. Oral Dis. 2010, 16, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Al-Majid, A.; Alassiri, S.; Rathnayake, N.; Tervahartiala, T.; Gieselmann, D.R.; Sorsa, T. Matrix Metalloproteinase-8 as an Inflammatory and Prevention Biomarker in Periodontal and Peri-Implant Diseases. Int. J. Dent. 2018, 2018, 7891323. [Google Scholar] [CrossRef] [PubMed]
- Owen, C.A.; Hu, Z.; Lopez-Otin, C.; Shapiro, S.D. Membrane-bound matrix metalloproteinase-8 on activated polymorphonuclear cells is a potent, tissue inhibitor of metalloproteinase-resistant collagenase and serpinase. J. Immunol. 2004, 172, 7791–7803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorsa, T.; Tjäderhane, L.; Konttinen, Y.T.; Lauhio, A.; Salo, T.; Lee, H.M.; Golub, L.M.; Brown, D.L.; Mäntylä, P. Matrix metalloproteinases: Contribution to pathogenesis, diagnosis and treatment of periodontal inflammation. Ann. Med. 2006, 38, 306–321. [Google Scholar] [CrossRef]
- Ziebolz, D.; Schmalz, G.; Gollasch, D.; Eickholz, P.; Rinke, S. Microbiological and aMMP-8 findings depending on peri-implant disease in patients undergoing supportive implant therapy. Diagn. Microbiol. Infect. Dis. 2017, 88, 47–52. [Google Scholar] [CrossRef]
- Kiili, M.; Cox, S.W.; Chen, H.Y.; Wahlgren, J.; Maisi, P.; Eley, B.M.; Salo, T.; Sorsa, T. Collagenase-2 (MMP-8) and collagenase-3 (MMP-13) in adult periodontitis: Molecular forms and levels in gingival crevicular fluid and immunolocalisation in gingival tissue. J. Clin. Periodontol. 2002, 29, 224–232. [Google Scholar] [CrossRef]
- Gangbar, S.; Overall, C.M.; McCulloch, C.A.; Sodek, J. Identification of polymorphonuclear leukocyte collagenase and gelatinase activities in mouthrinse samples: Correlation with periodontal disease activity in adult and juvenile periodontitis. J. Periodontal Res. 1990, 25, 257–267. [Google Scholar] [CrossRef]
- Uitto, V.J.; Suomalainen, K.; Sorsa, T. Salivary collagenase. Origin, characteristics and relationship to periodontal health. J. Periodontal Res. 1990, 25, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Ramseier, C.A.; Eick, S.; Brönnimann, C.; Buser, D.; Brägger, U.; Salvi, G.E. Host-derived biomarkers at teeth and implants in partially edentulous patients. A 10-year retrospective study. Clin. Oral Implants Res. 2016, 27, 211–217. [Google Scholar] [CrossRef]
- Nyati, K.K.; Prasad, K.N. Role of Cytokines and Toll-Like Receptors in the Immunopathogenesis of Guillain-Barré Syndrome. Mediators Inflamm. 2014, 2014, 758639. [Google Scholar] [CrossRef]
- Yakob, M.; Meurman, J.H.; Sorsa, T.; Söder, B. Treponema denticola associates with increased levels of MMP-8 and MMP-9 in gingival crevicular fluid. Oral Dis. 2013, 19, 694–701. [Google Scholar] [CrossRef]
- Nieminen, M.T.; Listyarifah, D.; Hagström, J.; Haglund, C.; Grenier, D.; Nordström, D.; Uitto, V.J.; Hernandez, M.; Yucel-Lindberg, T.; Tervahartiala, T.; et al. Treponema denticola chymotrypsin-like proteinase may contribute to orodigestive carcinogenesis through immunomodulation. Br. J. Cancer 2018, 118, 428–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sexton, W.M.; Lin, Y.; Kryscio, R.J.; Dawson, D.R., 3rd; Ebersole, J.L.; Miller, C.S. Salivary biomarkers of periodontal disease in response to treatment. J. Clin. Periodontol. 2011, 38, 434–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorsa, T.; Gieselmann, D.; Arweiler, N.B.; Hernández, M. A quantitative point-of-care test for periodontal and dental peri-implant diseases. Nat. Rev. Dis. Primers 2017, 3, 17069. [Google Scholar] [CrossRef]
- Izadi Borujeni, S.; Mayer, M.; Eickholz, P. Activated matrix metalloproteinase-8 in saliva as diagnostic test for periodontal disease? A case-control study. Med. Microbiol. Immunol. 2015, 204, 665–672. [Google Scholar] [CrossRef]
- Heikkinen, A.M.; Raivisto, T.; Kettunen, K.; Kovanen, L.; Haukka, J.; Pakbaznejad Esmaeili, E.; Elg, J.; Gieselmann, D.R.; Rathnayake, N.; Ruokonen, H.; et al. Pilot Study on the Genetic Background of an Active Matrix Metalloproteinase-8 Test in Finnish Adolescents. J. Periodontol. 2017, 88, 464–472. [Google Scholar] [CrossRef]
- Nwhator, S.O.; Ayanbadejo, P.O.; Umeizudike, K.A.; Opeodu, O.I.; Agbelusi, G.A.; Olamijulo, J.A.; Arowojolu, M.O.; Sorsa, T.; Babajide, B.S.; Opedun, D.O. Clinical correlates of a lateral-flow immunoassay oral risk indicator. J. Periodontol. 2014, 85, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Mauramo, M.; Ramseier, A.M.; Mauramo, E.; Buser, A.; Tervahartiala, T.; Sorsa, T.; Waltimo, T. Associations of oral fluid MMP-8 with periodontitis in Swiss adult subjects. Oral Dis. 2018, 24, 449–455. [Google Scholar] [CrossRef]
- Gursoy, U.K.; Könönen, E.; Huumonen, S.; Tervahartiala, T.; Pussinen, P.J.; Suominen, A.L.; Sorsa, T. Salivary type I collagen degradation end-products and related matrix metalloproteinases in periodontitis. J. Clin. Periodontol. 2013, 40, 18–25. [Google Scholar] [CrossRef]
- Salminen, A.; Gursoy, U.K.; Paju, S.; Hyvärinen, K.; Mäntylä, P.; Buhlin, K.; Könönen, E.; Nieminen, M.S.; Sorsa, T.; Sinisalo, J.; et al. Salivary biomarkers of bacterial burden, inflammatory response, and tissue destruction in periodontitis. J. Clin. Periodontol. 2014, 41, 442–450. [Google Scholar] [CrossRef]
- Mäntylä, P.; Stenman, M.; Kinane, D.; Salo, T.; Suomalainen, K.; Tikanoja, S.; Sorsa, T. Monitoring periodontal disease status in smokers and nonsmokers using a gingival crevicular fluid matrix metalloproteinase-8-specific chair-side test. J. Periodontal Res. 2006, 41, 503–512. [Google Scholar] [CrossRef]
- Leppilahti, J.M.; Kallio, M.A.; Tervahartiala, T.; Sorsa, T.; Mäntylä, P. Gingival crevicular fluid matrix metalloproteinase-8 levels predict treatment outcome among smokers with chronic periodontitis. J. Periodontol. 2014, 85, 250–260. [Google Scholar] [CrossRef]
- Janska, E.; Mohr, B.; Wahl, G. Correlation between peri-implant sulcular fluid rate and expression of collagenase2 (MMP8). Clin. Oral Investig. 2016, 20, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, H.; Uehara, J.; Hara, E.S.; Sonoyama, W.; Kimura, A.; Kanyama, M.; Matsuka, Y.; Kuboki, T. Matrix metalloproteinase-8 is the major potential collagenase in active peri-implantitis. J. Prosthodont. Res. 2012, 56, 249–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, J.; Kitti, U.; Teronen, O.; Sorsa, T.; Husa, V.; Laine, P.; Rönkä, H.; Salo, T.; Lindqvist, C.; Konttinen, Y.T. Collagenases in different categories of peri-implant vertical bone loss. J. Dent. Res. 2000, 79, 1870–1873. [Google Scholar] [CrossRef]
- Ritzer, J.; Lühmann, T.; Rode, C.; Pein-Hackelbusch, M.; Immohr, I.; Schedler, U.; Thiele, T.; Stübinger, S.; Rechenberg, B.V.; Waser-Althaus, J.; et al. Diagnosing peri-implant disease using the tongue as a 24/7 detector. Nat. Commun. 2017, 8, 264. [Google Scholar] [CrossRef]
- Hong, I.; Pae, H.C.; Song, Y.W.; Cha, J.K.; Lee, J.S.; Paik, J.W.; Choi, S.H. Oral Fluid Biomarkers for Diagnosing Gingivitis in Human: A Cross-Sectional Study. J. Clin. Med. 2020, 9. [Google Scholar] [CrossRef]
- Alassiri, S.; Parnanen, P.; Rathnayake, N.; Johannsen, G.; Heikkinen, A.M.; Lazzara, R.; van der Schoor, P.; van der Schoor, J.G.; Tervahartiala, T.; Gieselmann, D.; et al. The Ability of Quantitative, Specific, and Sensitive Point-of-Care/Chair-Side Oral Fluid Immunotests for aMMP-8 to Detect Periodontal and Peri-Implant Diseases. Dis. Markers 2018, 2018, 1306396. [Google Scholar] [CrossRef]
- Räisänen, I.T.; Heikkinen, A.M.; Siren, E.; Tervahartiala, T.; Gieselmann, D.R.; van der Schoor, G.J.; van der Schoor, P.; Sorsa, T. Point-of-Care/Chairside aMMP-8 Analytics of Periodontal Diseases’ Activity and Episodic Progression. Diagnostics 2018, 8. [Google Scholar] [CrossRef] [Green Version]
- Yamazaki-Kubota, T.; Miyamoto, M.; Sano, Y.; Kusumoto, M.; Yonezu, T.; Sugita, K.; Okuda, K.; Yakushiji, M.; Ishihara, K. Analysis of matrix metalloproteinase (MMP-8 and MMP-2) activity in gingival crevicular fluid from children with Down’s syndrome. J. Periodontal Res. 2010, 45, 170–176. [Google Scholar] [CrossRef]
- Rai, B.; Kaur, J.; Jain, R.; Anand, S.C. Levels of gingival crevicular metalloproteinases-8 and -9 in periodontitis. Saudi Dent. J. 2010, 22, 129–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppilahti, J.M.; Ahonen, M.M.; Hernández, M.; Munjal, S.; Netuschil, L.; Uitto, V.J.; Sorsa, T.; Mäntylä, P. Oral rinse MMP-8 point-of-care immuno test identifies patients with strong periodontal inflammatory burden. Oral Dis. 2011, 17, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Kraft-Neumärker, M.; Lorenz, K.; Koch, R.; Hoffmann, T.; Mäntylä, P.; Sorsa, T.; Netuschil, L. Full-mouth profile of active MMP-8 in periodontitis patients. J. Periodontal. Res. 2012, 47, 121–128. [Google Scholar] [CrossRef]
- Ebersole, J.L.; Schuster, J.L.; Stevens, J.; Dawson, D., 3rd; Kryscio, R.J.; Lin, Y.; Thomas, M.V.; Miller, C.S. Patterns of salivary analytes provide diagnostic capacity for distinguishing chronic adult periodontitis from health. J. Clin. Immunol. 2013, 33, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Leppilahti, J.M.; Hernández-Ríos, P.A.; Gamonal, J.A.; Tervahartiala, T.; Brignardello-Petersen, R.; Mantyla, P.; Sorsa, T.; Hernández, M. Matrix metalloproteinases and myeloperoxidase in gingival crevicular fluid provide site-specific diagnostic value for chronic periodontitis. J. Clin. Periodontol. 2014, 41, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.H.; Hwang, S.J. Effect of smoking cessation for 1 year on periodontal biomarkers in gingival crevicular fluid. J. Periodontal Res. 2016, 51, 366–375. [Google Scholar] [CrossRef]
- Gul, S.S.; Douglas, C.W.; Griffiths, G.S.; Rawlinson, A. A pilot study of active enzyme levels in gingival crevicular fluid of patients with chronic periodontal disease. J. Clin. Periodontol. 2016, 43, 629–636. [Google Scholar] [CrossRef] [Green Version]
- Kumar, Y.; Jain, V.; Chauhan, S.S.; Bharate, V.; Koli, D.; Kumar, M. Influence of different forms and materials (zirconia or titanium) of abutments in peri-implant soft-tissue healing using matrix metalloproteinase-8: A randomized pilot study. J. Prosthet. Dent. 2017, 118, 475–480. [Google Scholar] [CrossRef]
- Gul, S.S.; Griffiths, G.S.; Stafford, G.P.; Al-Zubidi, M.I.; Rawlinson, A.; Douglas, C.W.I. Investigation of a Novel Predictive Biomarker Profile for the Outcome of Periodontal Treatment. J. Periodontol. 2017, 88, 1135–1144. [Google Scholar] [CrossRef]
- Borges, C.D.; Ricoldi, M.S.; Messora, M.R.; Palioto, D.B.; Souza, S.L.S.; Novaes Júnior, A.B.; Taba, M., Jr. Clinical attachment loss and molecular profile of inflamed sites before treatment. J. Appl. Oral Sci. 2019, 27, e20180671. [Google Scholar] [CrossRef]
- Karteva, T.; Manchorova-Veleva, N. Biomarker for Asymptomatic Apical Periodontitis in Gingival Crevicular Fluid: aMMP-8. Eur. J. Dent. 2020, 14, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Duan, D.; Ma, R.; Ding, Y.; Xu, Y.; Zhou, X.; Zhao, L.; Xu, X. The combined use of salivary biomarkers and clinical parameters to predict the outcome of scaling and root planing: A cohort study. J. Clin. Periodontol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rautava, J.; Gürsoy, U.K.; Kullström, A.; Könönen, E.; Sorsa, T.; Tervahartiala, T.; Gürsoy, M. An Oral Rinse Active Matrix Metalloproteinase-8 Point-of-Care Immunotest May Be Less Accurate in Patients with Crohn’s Disease. Biomolecules 2020, 10. [Google Scholar] [CrossRef] [Green Version]
- Hedenbjörk-Lager, A.; Bjørndal, L.; Gustafsson, A.; Sorsa, T.; Tjäderhane, L.; Åkerman, S.; Ericson, D. Caries correlates strongly to salivary levels of matrix metalloproteinase-8. Caries Res. 2015, 49, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Heikkinen, A.M.; Sorsa, T.; Pitkäniemi, J.; Tervahartiala, T.; Kari, K.; Broms, U.; Koskenvuo, M.; Meurman, J.H. Smoking affects diagnostic salivary periodontal disease biomarker levels in adolescents. J. Periodontol. 2010, 81, 1299–1307. [Google Scholar] [CrossRef]
- Gursoy, U.K.; Könönen, E.; Pradhan-Palikhe, P.; Tervahartiala, T.; Pussinen, P.J.; Suominen-Taipale, L.; Sorsa, T. Salivary MMP-8, TIMP-1, and ICTP as markers of advanced periodontitis. J. Clin. Periodontol. 2010, 37, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M. Host modulation therapy with anti-inflammatory agents. Periodontol. 2000 2018, 76, 131–149. [Google Scholar] [CrossRef] [PubMed]
- Golub, L.M.; Elburki, M.S.; Walker, C.; Ryan, M.; Sorsa, T.; Tenenbaum, H.; Goldberg, M.; Wolff, M.; Gu, Y. Non-antibacterial tetracycline formulations: Host-modulators in the treatment of periodontitis and relevant systemic diseases. Int. Dent. J. 2016, 66, 127–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramseier, C.A.; Kinney, J.S.; Herr, A.E.; Braun, T.; Sugai, J.V.; Shelburne, C.A.; Rayburn, L.A.; Tran, H.M.; Singh, A.K.; Giannobile, W.V. Identification of pathogen and host-response markers correlated with periodontal disease. J. Periodontol. 2009, 80, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Rathnayake, N.; Akerman, S.; Klinge, B.; Lundegren, N.; Jansson, H.; Tryselius, Y.; Sorsa, T.; Gustafsson, A. Salivary biomarkers of oral health: A cross-sectional study. J. Clin. Periodontol. 2013, 40, 140–147. [Google Scholar] [CrossRef]
- Gursoy, U.K.; Könönen, E.; Pussinen, P.J.; Tervahartiala, T.; Hyvärinen, K.; Suominen, A.L.; Uitto, V.J.; Paju, S.; Sorsa, T. Use of host- and bacteria-derived salivary markers in detection of periodontitis: A cumulative approach. Dis. Markers 2011, 30, 299–305. [Google Scholar] [CrossRef]
- Liukkonen, J.; Gürsoy, U.K.; Könönen, E.; Akhi, R.; Salminen, A.; Liljestrand, J.M.; Pradhan-Palikhe, P.; Pietiäinen, M.; Sorsa, T.; Persson, G.R.; et al. Immunological and Microbiological Profiling of Cumulative Risk Score for Periodontitis. Diagnostics 2020, 10, 560. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Mäntylä, P.; Rönkä, H.; Kallio, P.; Kallis, G.B.; Lundqvist, C.; Kinane, D.F.; Salo, T.; Golub, L.M.; Teronen, O.; et al. Scientific basis of a matrix metalloproteinase-8 specific chair-side test for monitoring periodontal and peri-implant health and disease. Ann. N. Y. Acad. Sci. 1999, 878, 130–140. [Google Scholar] [CrossRef]
- Yoshida, N. Purification of human neutrophil collagenase, establishment of its monoclonal antibodies and application to gingival crevicular neutrophils. Kokubyo Gakkai Zasshi 1993, 60, 121–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanelli, R.; Mancini, S.; Laschinger, C.; Overall, C.M.; Sodek, J.; McCulloch, C.A. Activation of neutrophil collagenase in periodontitis. Infect. Immun. 1999, 67, 2319–2326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lein, M.; Nowak, L.; Jung, K.; Koenig, F.; Lichtinghagen, R.; Schnorr, D.; Loening, S.A. Analytical aspects regarding the measurement of metalloproteinases and their inhibitors in blood. Clin. Biochem. 1997, 30, 491–496. [Google Scholar] [CrossRef]
- Ingman, T.; Tervahartiala, T.; Ding, Y.; Tschesche, H.; Haerian, A.; Kinane, D.F.; Konttinen, Y.T.; Sorsa, T. Matrix metalloproteinases and their inhibitors in gingival crevicular fluid and saliva of periodontitis patients. J. Clin. Periodontol. 1996, 23, 1127–1132. [Google Scholar] [CrossRef]
- Lee, W.; Aitken, S.; Sodek, J.; McCulloch, C.A. Evidence of a direct relationship between neutrophil collagenase activity and periodontal tissue destruction in vivo: Role of active enzyme in human periodontitis. J. Periodontal Res. 1995, 30, 23–33. [Google Scholar] [CrossRef]
- Yu, Q.; Stamenkovic, I. Cell surface-localized matrix metalloproteinase-9 proteolytically activates TGF-beta and promotes tumor invasion and angiogenesis. Genes Dev. 2000, 14, 163–176. [Google Scholar]
- Buduneli, N. Biomarkers in Periodontal Health and Disease. Rationale, Benefits, and Future Directions; Springer International Publishing: Basel, Switzerland, 2020; pp. 53–59. [Google Scholar]
- Yılmaz, B.; Yılmaz, F. Chapter 8—Lab-on-a-Chip Technology and Its Applications. In Omics Technologies and Bio-Engineering; Barh, D., Azevedo, V., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 145–153. [Google Scholar]
- Peeling, R.W.; Holmes, K.K.; Mabey, D.; Ronald, A. Rapid tests for sexually transmitted infections (STIs): The way forward. Sex. Transm. Infect. 2006, 82 (Suppl. 5), v1–v6. [Google Scholar] [CrossRef]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Authors’ reply: Predictive diagnostic tests in periodontal diseases. Nat. Rev. Dis. Primers 2017, 3, 17070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenz, K.; Keller, T.; Noack, B.; Freitag, A.; Netuschil, L.; Hoffmann, T. Evaluation of a novel point-of-care test for active matrix metalloproteinase-8: Agreement between qualitative and quantitative measurements and relation to periodontal inflammation. J. Periodontal Res. 2017, 52, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Grigoriadis, A.; Sorsa, T.; Räisänen, I.; Pärnänen, P.; Tervahartiala, T.; Sakellari, D. Prediabetes/Diabetes Can Be Screened at the Dental Office by a Low-Cost and Fast Chair-Side/Point-of-Care aMMP-8 Immunotest. Diagnostics 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Räisänen, I.T.; Sorsa, T.; van der Schoor, G.J.; Tervahartiala, T.; van der Schoor, P.; Gieselmann, D.R.; Heikkinen, A.M. Active Matrix Metalloproteinase-8 Point-of-Care (PoC)/Chairside Mouthrinse Test vs. Bleeding on Probing in Diagnosing Subclinical Periodontitis in Adolescents. Diagnostics (Basel) 2019, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmalz, G.; Hübscher, A.E.; Angermann, H.; Schmidt, J.; Schmickler, J.; Legler, T.J.; Ziebolz, D. Associations of chairside salivary aMMP-8 findings with periodontal parameters, potentially periodontal pathogenic bacteria and selected blood parameters in systemically healthy adults. Diagn. Microbiol. Infect. Dis. 2019, 95, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Bacigalupo, J.; Könönen, M.; Pärnänen, P.; Räisänen, I.T. Host-Modulation Therapy and Chair-Side Diagnostics in the Treatment of Peri-Implantitis. Biosensors 2020, 10, 44. [Google Scholar] [CrossRef] [PubMed]
- Lähteenmäki, H.; Umeizudike, K.A.; Heikkinen, A.M.; Räisänen, I.T.; Rathnayake, N.; Johannsen, G.; Tervahartiala, T.; Nwhator, S.O.; Sorsa, T. aMMP-8 Point-of-Care/Chairside Oral Fluid Technology as a Rapid, Non-Invasive Tool for Periodontitis and Peri-Implantitis Screening in a Medical Care Setting. Diagnostics 2020, 10, 562. [Google Scholar] [CrossRef] [PubMed]
- Dincer, C.; Bruch, R.; Kling, A.; Dittrich, P.S.; Urban, G.A. Multiplexed Point-of-Care Testing–xPOCT. Trends Biotechnol. 2017, 35, 728–742. [Google Scholar] [CrossRef] [Green Version]
- Kinane, D.F. Regulators of tissue destruction and homeostasis as diagnostic aids in periodontology. Periodontol. 2000 2000, 24, 215–225. [Google Scholar] [CrossRef]
- Grover, V.; Kapoor, A.; Malhotra, R.; Kaur, G. Clinical Relevance of the Advanced Microbiologic and Biochemical Investigations in Periodontal Diagnosis: A Critical Analysis. J. Oral Dis. 2014, 2014, 785615. [Google Scholar] [CrossRef]
- Chapple, I.L. Periodontal diagnosis and treatment–where does the future lie? Periodontol. 2000 2009, 51, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M. Detection and diagnosis of periodontal conditions amenable to prevention. BMC Oral Health 2015, 15, S5. [Google Scholar]
- Baelum, V.; López, R. Periodontal disease epidemiology—learned and unlearned? Periodontol. 2000 2013, 62, 37–58. [Google Scholar] [CrossRef] [PubMed]
- de Morais, E.F.; Pinheiro, J.C.; Leite, R.B.; Santos, P.P.A.; Barboza, C.A.G.; Freitas, R.A. Matrix metalloproteinase-8 levels in periodontal disease patients: A systematic review. J. Periodontal Res. 2018, 53, 156–163. [Google Scholar] [CrossRef]
- Baelum, V.; Papapanou, P.N. CPITN and the epidemiology of periodontal disease. Community Dent. Oral Epidemiol. 1996, 24, 367–368. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Aim(s) | Study Groups | Oral Fluids Examined * | Biomarkers, Assays † | Clinical Criteria ¶ | Results |
|---|---|---|---|---|---|---|
| Ma et al., 2000 [105] | Investigate the correlation between GI, MMP8, and MMP13 level in PISF and amount of peri-implant bone loss | 13 patients having implants with different levels of bone resorption | PISF | MMP8 by time-resolved immunofluorometric assay and MMP13 by quantitative immunoblot | Peri-implant vertical bone loss was divided into: <1 mm, 1–3 mm, and >3mm Gingival inflammation recorded on scale from 0–3 | Both biomarkers potentially reflect osteolytic process but not GI |
| Yamazaki-Kubota et al., 2010 [110] | Investigate the level of MMP2, MMP8, and subgingival bacteria in children with Down’s syndrome | Children with DS (n = 15) Healthy controls (n = 14) | GCF | MMP2 and MMP8 (ELISA) | OHI, PPD, and BOP | Both collagenolytic enzymes were significantly higher in GCF of children with DS than controls even with low oral hygiene index score and absence of BOP. |
| Rai et al., 2010 [111] | Investigate the level of MMP8 and MMP9 in healthy periodontium and periodontitis | Periodontitis patients (n = 10) Healthy controls (n = 10) | GCF | Both MMPs measured by ELISA | At least 7 teeth with PPD >6 mm Having at least 12 posterior teeth | Significantly higher level of MMP8 and MMP9 in periodontitis vs healthy controls |
| Leppilahti et al., 2011 [112] | Assessing the ability of PoC MMP8- mouth rinse, measured by three assays, TIMP1, and elastase activity to distinguish subjects with different periodontal conditions. Comparing assaying methods for MMP8 | Randomly selected patients with periodontitis (n = 214) | Mouth rinse samples | MMP8 assayed by IFMA, DentoELISA and commercial ELISA. TIMP1 and elastase measured by ELISA | BOP, PPD ≥4 mm, and PIBI | MMP-8/TIMP-1 combination showed higher diagnostic accuracy DentoELISA showed higher sensitivity and specificity in detecting MMP8 |
| Kraft-Neumärker et al., 2012 [113] | Full-mouth analysis to investigate the correlation between clinical parameters and level of MMP8 | Females with periodontitis (n = 9) | GCF | MMP8 assayed by ELISA | GI, PI, BOP, and PPD (>30% of sites affected) | Increased PPD was associated with increased level of MMP8 |
| Ebersole et al., 2013 [114] | Investigating the level of selected biomarkers in periodontal health and periodontal disease | Healthy (n = 30) Periodontitis (n = 50) | Saliva | IL1β, IL6, TNFα, and IFNα assayed by human Luminex® multiplex assays MMP8, PGE2, and albumin assayed by ELISA | Healthy: BOP <10% of sites, PPD ≤6 mm in <2% of sites, CAL >2 mm in <1% of sites Periodontitis: PPD ≥5 mm, CAL ≥3 mm, BOP ≥2 in at least 5 sites | Salivary MMP8, IL1β, and IL6 showed the highest diagnostic potential |
| Leppilahti et al., 2014 [115] | Assess the accuracy of different biomarkers in diagnosing periodontitis Comparing two methods for assaying MMP8 | Healthy (n = 20 sites) Gingivitis (n = 19 sites) Periodontitis (n = 19 sites) | GCF | MPO, TIMP1 MMP13, and MMP14. Assayed by ELISA MMP8 Assayed by ELISA and IFMA | Healthy: PPD <3 mm, no CAL, no inflammation Gingivitis: BOP with no loss of attachment Periodontitis: PPD ≥5 mm, CAL ≥3 mm, >50% bone loss in radiograph | MPO and MMP8 can highly discriminate periodontitis. IFMA is more accurate than ELISA for assaying MMP8 |
| Liu and Hwang, 2016 [116] | Assessment of the effect of smoking cessation on periodontal tissue over 12 months | Male smokers joined smoking cessation clinic (n = 122) | GCF, Saliva | MMP8, MMP9, and IL1β measured by ELISA, nicotine and cotinine assayed by chromatography-tandem mass spectrometry | PI, GI Patients exhibiting sites >5.5 mm were excluded | The level of MMP8 did not change significantly within the monitoring period between smokers, quit-smokers, oscillators and nonsmokers |
| Ramseier et al., 2016 [89] | Assessment of biomarkers in PISF 10 years after implant placement | Implants (n = 504), adjacent teeth (n = 493) | GCF, PISF | MMP8, IL1β, MMP3, MMP1, and MMP1/TIMP1 measured by ELISA | PI, mGI, BOP, PPD, and CAL | Increased level of MMP8 was detected in 90% of sites with progressive inflammation around tooth/implant |
| Gul et al., 2016 [117] | To assess combined biomarkers compared with single biomarker for predicting the outcome of treatment | Periodontitis patients (n = 30) | GCF | Active MMP8, elastase, cathepsin G, trypsin like enzyme and sialidase measured by colorimetric assay | Full mouth PI, BOP, PPD and CAL | Combined active enzyme profiling could provide significant prediction of outcome of treatment. |
| Kumar et al., 2017 [118] | Evaluate the response of peri-implant connective tissue to titanium and zirconia abutments | Candidates for implant placement (n = 12) | PISF | MMP8 assayed by ELISA | GI, PI, and PPD measured by thermoplastic periodontal sensor probe | Titanium abutment induced higher expression of MMP8 at early stages than zirconia |
| Gul et al., 2017 [119] | Assess the ability of a novel combination of biomarkers to predict treatment outcome of patients with chronic periodontitis | Periodontitis patients (n = 77) | GCF and plaque | Active MMP8, elastase and sialidase measured by colorimetric assay, Pg, Tf and Td level determined by qPCR. | Full mouth PI, BOP, PPD and CAL | The ‘‘fingerprint’’ of GCF enzymes and bacteria offers a way to predict the outcome of non-surgical periodontal treatment on a site-specific basis. |
| Mauramo et al., 2018 [98] | Assessment of association between MMP8 level in oral fluids and periodontitis | Periodontitis patients (n = 258) | GCF, Saliva | MMP8 assayed by IFMA | DMFT, BOP, PPD, CAL | MMP8 in saliva and GCF was significantly associated with severity of periodontitis and PPD |
| Borges et al., 2019 [120] | Investigate attachment loss at sites with progressive periodontal disease following SRP | Periodontitis stage II grade B (n = 18) Healthy controls (n = 9) | Saliva, GCF | IL-10, MMP8, VEGF, RANKL, OPG and TGF-β1 by Multiplex Cytokine Profiling Assay MMP8 level measured by ELISA | PPD, BOP, and relative CAL | Attachment loss continued in some sites even after SRP. Action of MMP8 seems to be modulated by IL-10 |
| Hong et al., 2020 [107] | Comparing efficiency and accuracy of different biomarkers in diagnosing gingivitis | Healthy (n = 15) Gingivitis (n = 85) | Saliva and GCF | MMP8, MMP9, cystatin C, MPO, PAF, cathepsin B, lactoferrin, and ICTP ELISA | Gingivitis defined by BOP ≥10% | MMP8 and MPO were significantly and positively correlated with BOP. MMP8 was the most effective in diagnosis of gingivitis |
| Karteva and Manchorova-Veleva, 2020 [121] | Assessing the accuracy of active (a)MMP8 in diagnosis of asymptomatic apical periodontitis (AAP) | AAP (n = 31) Control (n = 31) | GCF | aMMP8 by ELISA | CBCT used to confirm the presence of the lesion | Statistically significant increase in aMMP8 level collected from teeth with AAP compared to healthy controls |
| Liu et al., 2020 [122] | Application of the combined use of baseline salivary biomarkers and clinical parameters in predicting the outcome of scaling and root planning | Advance periodontitis (n = 40) | Saliva | MMP8 and IL1β by ELISA, Pg, Aa, Pi and Tf by PCR. | PPD, BOP, and CAL | The combination of baseline salivary biomarkers and clinical parameters better predicted SRP outcomes than each alone |
| Author, Year | Aim(s) | Study Groups | Oral Fluid Examined | PoC/Chairside Test | Clinical Criteria ¶ | Results |
|---|---|---|---|---|---|---|
| Mäntylä et al., 2006 [101] | Evaluate the efficacy of MMP8- specific chair-side dip-stick test in longitudinal monitoring of periodontal status of smoker and non-smoker periodontitis patients | Periodontitis patients (n = 16) | GCF | MMP8 assayed by chair-side dipstick test | Have at least 20 teeth, BOP, PPD ≥4 mm at 5 or more sites, PI, and CAL | Persistent elevation of MMP8 in GCF may indicate sites at risk and poor response to conventional nonsurgical periodontal treatment |
| Sorsa et al., 2010 [81] | Comparing four methods to detect MMP8 in GCF | Periodontally healthy (n = 2), gingivitis (n = 2), moderate-severe periodontitis (n = 6) | GCF | IFMA, MMP-8 specific chair-side dip-stick test, Dento-Analyzer, and Amersham ELISA kit | PPD, AL | IFMA and Dento-Analyzer yielded comparable results, followed by chair-side dip-stick test, while Amersham ELISA results were not in line with other assays |
| Nwhator et al., 2014 [97] | Investigate the clinical correlates of aMMP8-immunotest with BOP, oral hygiene, and PPD | Periodontitis and healthy (n = 86), Final analysis included 76 patients | Mouth rinse samples | aMMP8 measured by Lateral flow mouth rinse test (PerioMarker®) | BOP, debris index and calculus index scores, and BPE, PPD was charted when BPE score> 3 | aMMP8 showed high sensitivity for at least two sites with BOP and two sites with periodontal pockets |
| Izadi Borujeni et al., 2015 [95] | To evaluate the sensitivity and specificity of aMMP8 PoC immunotest in detecting periodontitis | Untreated generalized periodontitis (n=30 equally distributed between moderate and severe cases) Healthy controls (n = 30) | Mouth rinse samples | aMMP8 measured by Lateral flow mouth rinse test (PerioMarker®) | Moderate periodontitis: PPD ≥3.5mm, CAL =3–4 mm at >30% of sites or ≥5 mm at <30% of sites Severe periodontitis: PPD ≥3.5 mm, CAL ≥5 mm at >30% of sites Healthy: PPD ≤3 mm, CAL ≤2 mm at <30% of sites | aMMP8 positively correlated with generalized periodontitis with diagnostic sensitivity = 87% and specificity = 60% |
| Heikkinen et al., 2016 [41] | Investigate the ability of PoC aMMP8-mouthrinse to identify adolescents with oral inflammatory burden | Adolescent subjects (n = 47) | Mouth rinse samples | aMMP8 measured by Lateral flow mouth rinse test | Full-mouth clinical parameters, including BOP, PI, PPD ≥4mm, and caries sites | aMMP-8 chairside test effectively differentiated adolescents with early initial signs of periodontitis. However, caries was less efficiently detected |
| Ritzer et al., 2017 [106] | Determine the efficiency of sensory chewing gums as 24/7 detector to differentiate between patients with peri-implant disease and healthy subjects | Peri-implantitis or mucositis group and healthy volunteers | PISF, Unstimulated saliva | aMMP-8 levels were assayed by DentoELISA, Dento-Analyzer, and peptide sensor (PCL ID #1c) | N/A | Level of MMP8 was significantly higher in patients with peri-implant diseases as compared to healthy controls |
| Heikkinen et al., 2017 [96] | Determination of genetic background for initial periodontitis and caries by PoC aMMP8 immunotest | Adolescent subjects (n = 47) | Oral fluid samples | aMMP8 measured by Lateral flow mouth rinse test (PerioSafe®) | BOP ≥20% of sites, PPD, PI, and caries status | Genetic polymorphisms of MMP3 and VDR significantly associated with aMMP8 level |
| Räisänen et al., 2018 [109] | Investigate the effectiveness of aMMP8 PoC immunotest in determining cost-effective treatment(s) | Adolescents (n = 47) Adults (n = 70) | Mouth rinse samples | aMMP8 measured by Lateral flow mouth rinse test | Treatment need defined by CPITN scores | Results from aMMP8 PoC immunotest were consistent with CPITN codes for treatment needs |
| Grigoriadis et al., 2019 [145] | Using aMMP8 PoC immunotest for screening prediabetes and diabetes state in periodontal patients | Healthy (n = 21) Periodontitis: Stage I/II, grade A-C (n = 48) | Mouth rinse samples Capillary blood | aMMP8 assayed by Lateral flow mouth rinse immunoassay test and digital reader ORALyzer® Blood sugar by HbA1c test | PPD and BOP were measured | HbA1c and aMMP8 PoC test can provide dentists with opportunity to diagnose prediabetic and diabetic patients |
| Räisänen et al., 2019 [146] | Comparing the effectiveness of aMMP8 PoC mouthwash vs BOP in detection pre-/subclinical periodontitis in adolescents | 47 adolescents (30 male and 17 female) | Mouth rinse samples | aMMP8 Lateral flow immunoassay test (PerioSafe®) | BOP (20% of sites), PPD≥ 4mm, PI, bitewing radiographs for premolars and molars | aMMP8 was twice higher in terms of sensitivity and more accurate than BOP in detecting early stages than BOP |
| Schmalz et al., 2019 [147] | Investigate the association of aMMP8 with severity of periodontitis, periodontal bacteria, and blood parameters | Periodontitis patients (n = 188): Mild (n = 50) Moderate (n = 111) Severe (n = 27) | Mouth rinse samples, blood | aMMP8 measured by Lateral flow immunoassay test (Periomarker®) | Based on PPD and CAL, severity of periodontitis was divided into mild, moderate, and severe | aMMP8 was positively associated with severity of periodontitis and anaerobes highly involved in periodontal destruction |
| Rautava et al., 2020 [123] | Compare the accuracy of aMMP8 PoC immunotest in subjects with and without Crohn’s disease (CD) | Controls (n = 47) CD (n = 41) | Mouth rinse samples | Lateral flow mouth rinse test (PerioSafe®) | Oral mucosal examination for CD-related lesions Caries prevalence by DMFS Gingivitis defined by BOP ≥15% of sites with no CAL or PPD Periodontitis defined by: PPD ≥4 mm, CAL ≥2 mm with or without BOP | Discrimination accuracy of aMMP8 PoC immunotest reduced and diagnosis of periodontitis was compromised with CD patients |
| Sorsa et al., 2020 [40] | Assessing the usefulness of aMMP8 point of care (PoC) mouthwash in the interpretation of the “Staging” and “Grading” of the new classification system for periodontal disease | Healthy (n = 31) Periodontitis (n = 119) | Mouth rinse samples | Lateral flow mouth rinse test (PerioSafe®) and ORALyzer® | Healthy: BOP <10% of sites Periodontitis: Defined according to the new classification system 2018 | aMMP8 PoC mouthwash can be integrated for staging and grading of periodontitis |
| Sorsa et al., 2020 [148] | Investigate the effectiveness of aMMP8 PoC mouthwash in diagnosing peri-implantitis | Healthy subjects (n = 20) Peri-implantitis (n = 20) | Mouth rinse samples | aMMP8 Lateral flow immunoassay test (ImplantSafe®) | Peri-implantitis, diagnosed clinically and radiographically | aMMP8 PoC test correctly diagnosed all healthy and Peri-implantitis cases |
| Lähteenmäki et al., 2020 [149] | Assessing the accuracy aMMP-8 PISF POC test (ImplantSafe) as compared to other biomarkers of peri-implantitis. Evaluating the value of aMMP-8 lateral-flow PoC technologies in non-invasively monitoring periodontal treatment outcomes | Patients with peri-implantitis (n = 26) Healthy control (n = 26) Periodontitis patients (n = 15) | PISF, mouth rinse samples | aMMP8 Lateral flow immunoassay test (ImplantSafe®), (PerioSafe®) | Peri-implantitis, diagnosed by presence of PPD ≥4mm, BOP, radiographic bone loss ≥2 mm, PI, FI, mobility index Self-reported oral health (SROH)-questionnaires | aMMP8 PoC test discriminated health from peri-implantitis with higher accuracy than BOP, PMN-elastase, MMP9, TIMP1, and myeloperoxidase SROH can be used as adjunctive diagnostic method but not as alternative for oral fluid biomarkers |
| Assay | Commercial Kit | Sample | Target? |
|---|---|---|---|
| Microbial test kit | PerioScan | Subgingival plaque | Utilizes the BANA test for bacterial trypsin-like proteases |
| IAI Pado test | Subgingival plaque | Aa, Pg, Tf, and Td | |
| Evalusite test | Subgingival plaque, GCF | Aa, Pi, and Pg | |
| TOPAS | Subgingival plaque, GCF | Toxins derived from anaerobic metabolism and measures GCF protein level | |
| Omnigene® diagnosctics | Saliva | Pg, Pi, Aa, Fn, Tf, Td, Ec, and Cr | |
| Biochemical test | Prognostik | GCF | Serine proteinases and elastase |
| Pocketwatch | GCF | Detects aspartate aminotransferase through colorimetric detection | |
| Periogard | GCF | Detects the presence of aspartate aminotransferase | |
| Periocheck | GCF | Detects presence of neutral proteinases (collagenase) | |
| Progno-Stik | GCF | Elastase | |
| PerioMarker® | GCF | Activated MMP8 | |
| Dip Stick | GCF | MMP8 | |
| Perio 2000 | GCF, Subgingival plaque | Sulfides in periodontal pockets | |
| PerioSafe® | GCF, Mouth rinse | Activated MMP8 | |
| ImplantSafe® | GCF, PISF | Activated MMP8 | |
| ORALyzer® | GCF, Mouth rinse, Saliva | Activated MMP8 | |
| Integrated microfluidic platform for oral diagnostics | Saliva | MMP8 | |
| Oral Fluid NanoSensor test | Saliva | IL-1 and IL-8 | |
| Electronic taste chip | Saliva | C reactive protien | |
| Genetic test kits | GenoType®PST® | Saliva | Interleukin (IL-1α and IL-1β) genes polymorphism |
| MyperioID | Saliva | Genetic variation/polymorphism within the IL-1 gene |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gul, S.S.; Abdulkareem, A.A.; Sha, A.M.; Rawlinson, A. Diagnostic Accuracy of Oral Fluids Biomarker Profile to Determine the Current and Future Status of Periodontal and Peri-Implant Diseases. Diagnostics 2020, 10, 838. https://doi.org/10.3390/diagnostics10100838
Gul SS, Abdulkareem AA, Sha AM, Rawlinson A. Diagnostic Accuracy of Oral Fluids Biomarker Profile to Determine the Current and Future Status of Periodontal and Peri-Implant Diseases. Diagnostics. 2020; 10(10):838. https://doi.org/10.3390/diagnostics10100838
Chicago/Turabian StyleGul, Sarhang S., Ali A. Abdulkareem, Aram M. Sha, and Andrew Rawlinson. 2020. "Diagnostic Accuracy of Oral Fluids Biomarker Profile to Determine the Current and Future Status of Periodontal and Peri-Implant Diseases" Diagnostics 10, no. 10: 838. https://doi.org/10.3390/diagnostics10100838