Diagnostic Value of C-Reactive Protein in Discrimination between Uncomplicated and Complicated Parapneumonic Effusion

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Feller-Kopman, D.; Light, R. Pleural disease. N. Engl. J. Med. 2018, 378, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M.; Pardina, M.; Alemán, C.; Pallisa, E.; Light, R.W.; Bielsa, S. Computed tomography scoring system for discriminating between parapneumonic effusions eventually drained and those cured only with antibiotics. Respirology 2017, 22, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M. Distinguishing complicated from uncomplicated parapneumonic effusions. Curr. Opin. Pulm. Med. 2015, 21, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Falguera, M.; Carratalà, J.; Bielsa, S.; García-Vidal, C.; Ruiz-González, A.; Chica, I.; Gudiol, F.; Porcel, J.M. Predictive factors, microbiology and outcome of patients with parapneumonic effusion. Eur. Respir. J. 2011, 38, 1173–1179. [Google Scholar] [CrossRef] [Green Version]
- Porcel, J.M. Pleural fluid tests to identify complicated parapneumonic effusions. Curr. Opin. Pulm. Med. 2010, 16, 357–361. [Google Scholar] [CrossRef]
- Raymond, D. Surgical intervention for thoracic infections. Surg. Clin. N. Am. 2014, 94, 1283–1303. [Google Scholar] [CrossRef]
- Porcel, J.M.; Esquerda, A.; Vives, M.; Bielsa, S. Etiology of pleural effusions: Analysis of more than 3000 consecutive thoracenteses. Arch. Bronconeumol. 2014, 50, 161–165. [Google Scholar] [CrossRef]
- Bedawi, E.O.; Hassan, M.; Rahman, N.M. Recent developments in the management of pleural infection: A comprehensive review. Clin. Respir. J. 2018, 12, 2309–2320. [Google Scholar] [CrossRef] [PubMed]
- Ferreiro, L.; San José, M.E.; Valdés, L. Management of parapneumonic pleural effusion in adults. Arch. Bronconeumol. 2015, 51, 637–646. [Google Scholar] [CrossRef]
- Davies, H.E.; Davies, R.J.O.; Davies, C.W.H. On behalf of the BTS Pleural Disease Guideline Group. Management of pleural infection in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010, 65 (Suppl. S2), ii41–ii53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bielsa, S.; Valencia, H.; Ruiz-González, A.; Esquerda, A.; Porcel, J.M. Serum C-reactive protein as an adjunct for identifying complicated parapneumonic effusions. Lung 2014, 192, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M. Pleural fluid biomarkers: Beyond the Light criteria. Clin. Chest Med. 2013, 34, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Rahman, N.M.; Mishra, E.K.; Davies, H.E.; Davies, R.J.; Lee, Y.C. Clinically important factors influencing the diagnostic measurement of pleural fluid pH and glucose. Am. J. Respir. Crit. Care Med. 2008, 178, 483–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maskell, N.A.; Gleesonm, F.V.; Darby, M.; Davies, R.J. Diagnostically significant variations in pleural fluid pH in loculated parapneumonic effusions. Chest 2004, 126, 2022–2024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.; Shen, Y.; Qin, J.; Wan, C.; Zeng, N.; Chen, L.; Dong, Y. Diagnostic performance of C-reactive protein for parapneumonic pleural effusion: A meta-analysis. Ann. Transl. Med. 2019, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Chen, W.; Hsu, W.H.; Yu, Y.H.; Shih, C.M. Role of pleural fluid C-reactive protein concentration in discriminating uncomplicated parapneumonic pleural effusions from complicated parapneumonic effusion and empyema. Lung 2006, 184, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M.; Galindo, C.; Esquerda, A.; Trujillano, J.; Ruiz-González, A.; Falguera, M.; Vives, M. Pleural fluid interleukin-8 and C-reactive protein for discriminating complicated non-purulent from uncomplicated parapneumonic effusions. Respirology 2008, 13, 58–62. [Google Scholar] [CrossRef]
- Porcel, J.M.; Vives, M.; Cao, G.; Bielsa, S.; Ruiz-González, A.; Martínez-Iribarren, A.; Esquerda, A. Biomarkers of infection for the differential diagnosis of pleural effusions. Eur. Respir. J. 2009, 34, 1383–1389. [Google Scholar] [CrossRef]
- Porcel, J.M.; Bielsa, S.; Esquerda, A.; Ruiz-González, A.; Falguera, M. Pleural fluid C-reactive protein contributes to the diagnosis and assessment of severity of parapneumonic effusions. Eur. J. Intern. Med. 2012, 23, 447–450. [Google Scholar] [CrossRef]
- Skouras, V.; Boultadakis, E.; Nikoulis, D.; Polychronopoulos, V.; Daniil, Z.; Kalomenidis, I.; Gourgoulianis, K.I. Prognostic value of C-reactive protein in parapneumonic effusions. Respirology 2012, 17, 308–314. [Google Scholar] [CrossRef]
- Porcel, J.M.; Valencia, H.; Bielsa, S. Factors influencing pleural drainage in parapneumonic effusions. Rev. Clin. Esp. 2016, 216, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Marinkovic, S.P.; Topuzovska, I.K.; Stevanovic, M.; Anastasovska, A. Features of Parapneumonic Effusions. Pril (Makedon. Akad. Nauk. Umet. Odd. Med. Nauk.) 2018, 39, 131–141. [Google Scholar] [CrossRef] [Green Version]
- Petrusevska-Marinkovic, S.; Kondova-Topuzovska, I.; Milenkovic, Z.; Kondov, G.; Anastasovska, A. Clinical, Laboratory and Radiographic Features of Patients with Pneumonia and Parapneumonic Effusions. Open Access Maced. J. Med. Sci. 2016, 4, 428–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, K.A.; Wu, C.C.; Liu, Y.C.; Hsueh, P.C.; Chin, C.Y.; Wang, C.L.; Chu, C.M.; Shih, L.J.; Yang, C.Y. Combined serum biomarkers in the noninvasive diagnosis of complicated parapneumonic effusions and empyema. BMC Pulm. Med. 2019, 19, 108. [Google Scholar] [CrossRef]
- Yilmaz Turay, U.; Yildirim, Z.; Türköz, Y.; Biber, C.; Erdoğan, Y.; Keyf, A.I.; Uğurman, F.; Ayaz, A.; Ergun, P.; Harputluoglu, Y. Use of pleural fluid C-reactive protein in diagnosis of pleural effusions. Respir. Med. 2000, 94, 432–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elsammak, M.M.Y.; Morsi, T.S.; Khamis, H.I.; Ragab, M.S.; Zaki, M.A.; Abdel-Hadi, M.; Hassan, H.A. Osteopontin and C-reactive protein in Egyptian patients affected with tuberculous and malignant pleural effusion. Ann. Clin. Biochem. 2007, 44, 264–272. [Google Scholar] [CrossRef]
- Chierakul, N.; Kanitsap, A.; Chaiprasert, A.; Viriyataveekul, R. A simple C-reactive protein measurement for the differentiation between tuberculous and malignant pleural effusion. Respirology 2004, 9, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Kiropoulos, T.S.; Kostikas, K.; Oikonomidi, S.; Tsilioni, I.; Nikoulis, D.; Germenis, A.; Gourgoulianis, K.I. Acute phase markers for the differentiation of infectious and malignant pleural effusions. Respir. Med. 2007, 1015, 910–918. [Google Scholar] [CrossRef] [Green Version]
- Odeh, M.; Makhoul, B.; Sabo, E.; Srugo, I.; Oliven, A. The role of pleural fluid-serum gradient of tumor necrosis factor-alpha concentration in discrimination between complicated and uncomplicated parapneumonic effusion. Lung 2005, 183, 13–27. [Google Scholar] [CrossRef]
- Hutchinson, W.L.; Koenig, W.; Frohlich, M.; Sund, M.; Lowe, G.D.O.; Pepys, M.B. Immunoradiometric assay of circulating C-reactive protein: Age-related values in the adult general population. Clin. Chem. 2000, 46, 934–938. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | UCPPE (n = 86) | CPPE (n = 60) | p |
|---|---|---|---|
| Age (years) | 65.9 ± 18.1 | 74.1 ± 13.6 | <0.003 |
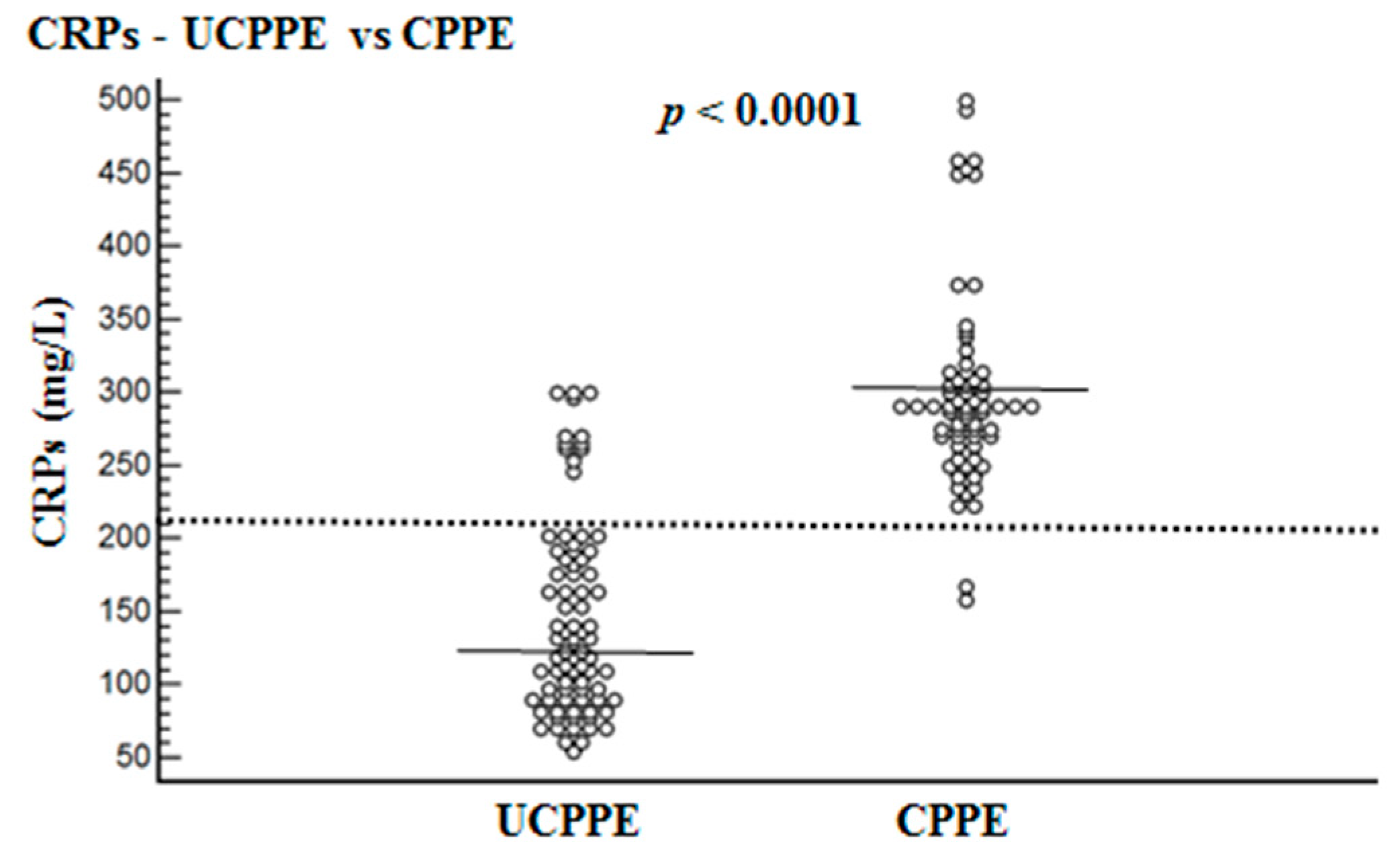
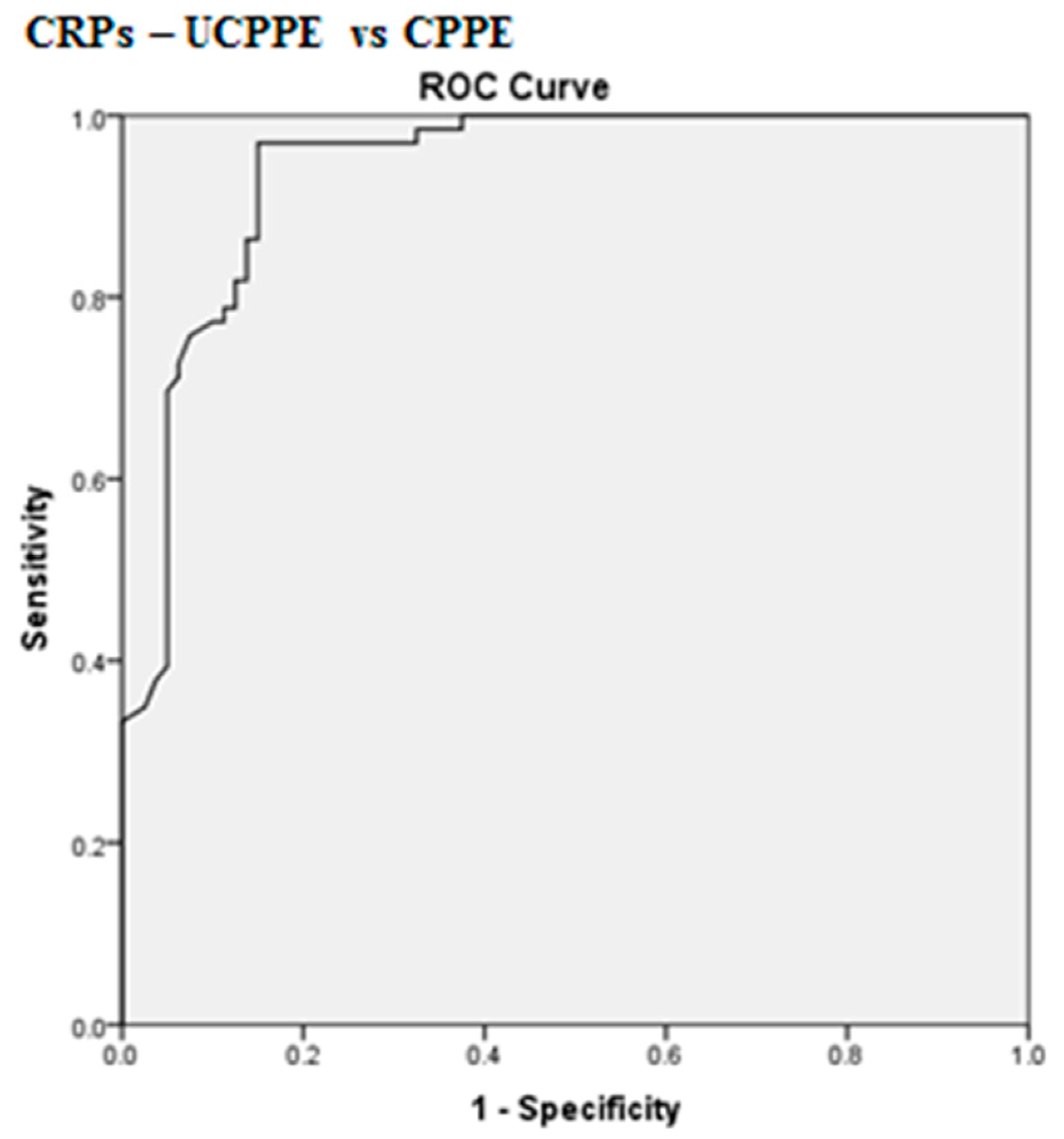
| CRPs (mg/L) 95% CI | 145.3 ± 67.6 130.5–160.1 | 302.2 ± 75.6 283.9–320.4 | <0.0001 |
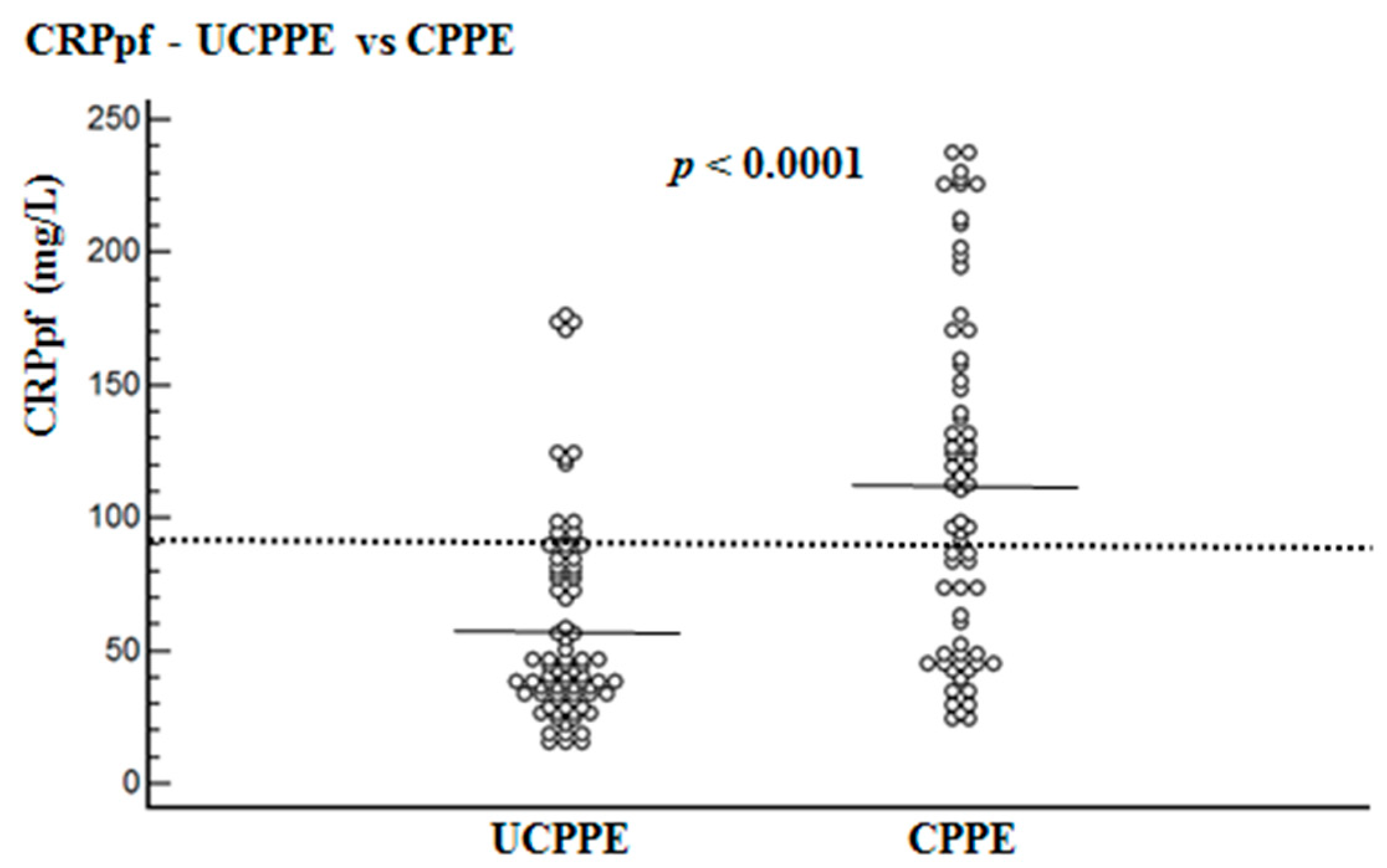
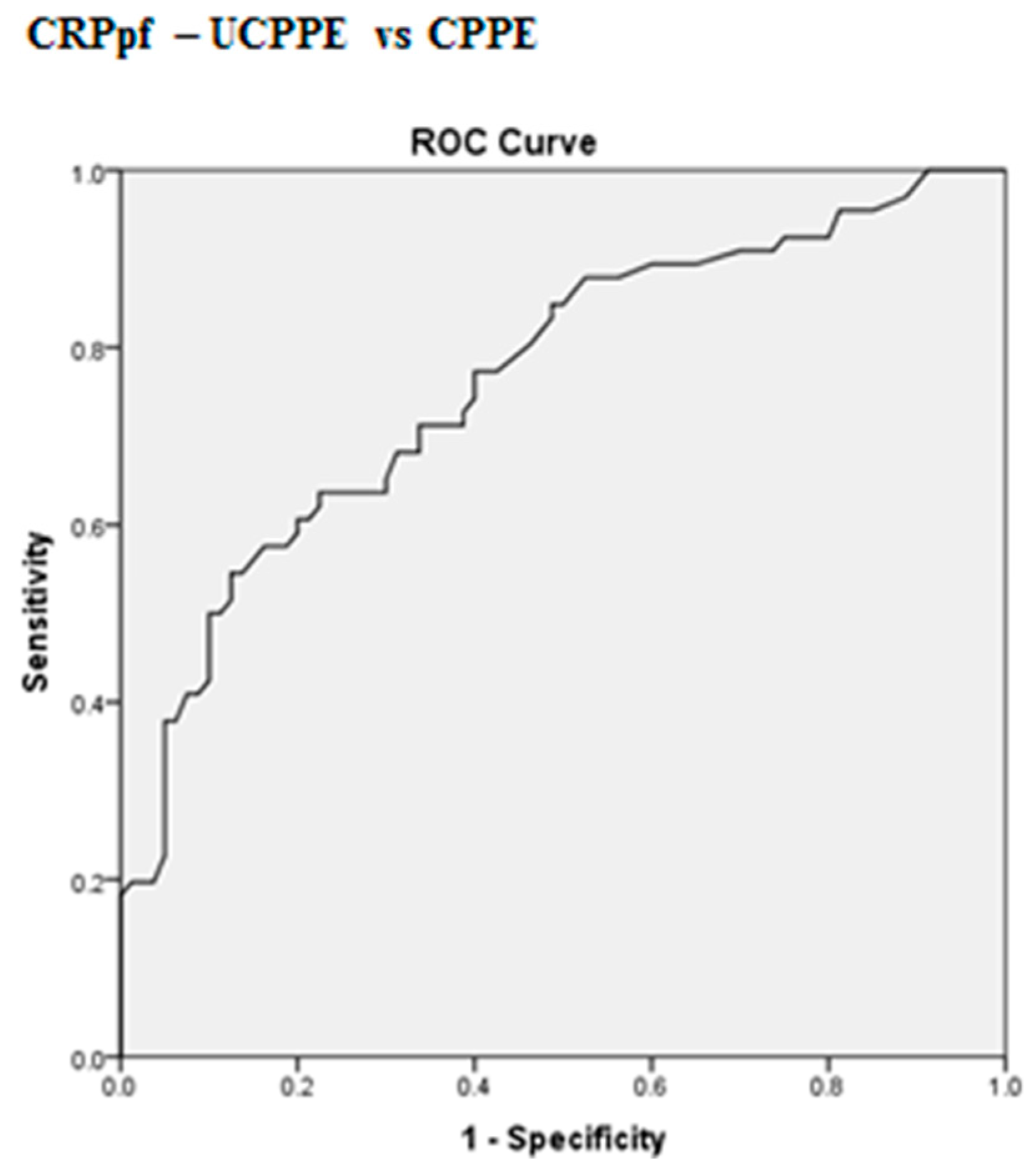
| CRPpf (mg/L) 95% CI | 58.5 ± 38.5 19.2–85.1 | 112.0 ± 65.0 96.0–128.0 | <0.0001 |
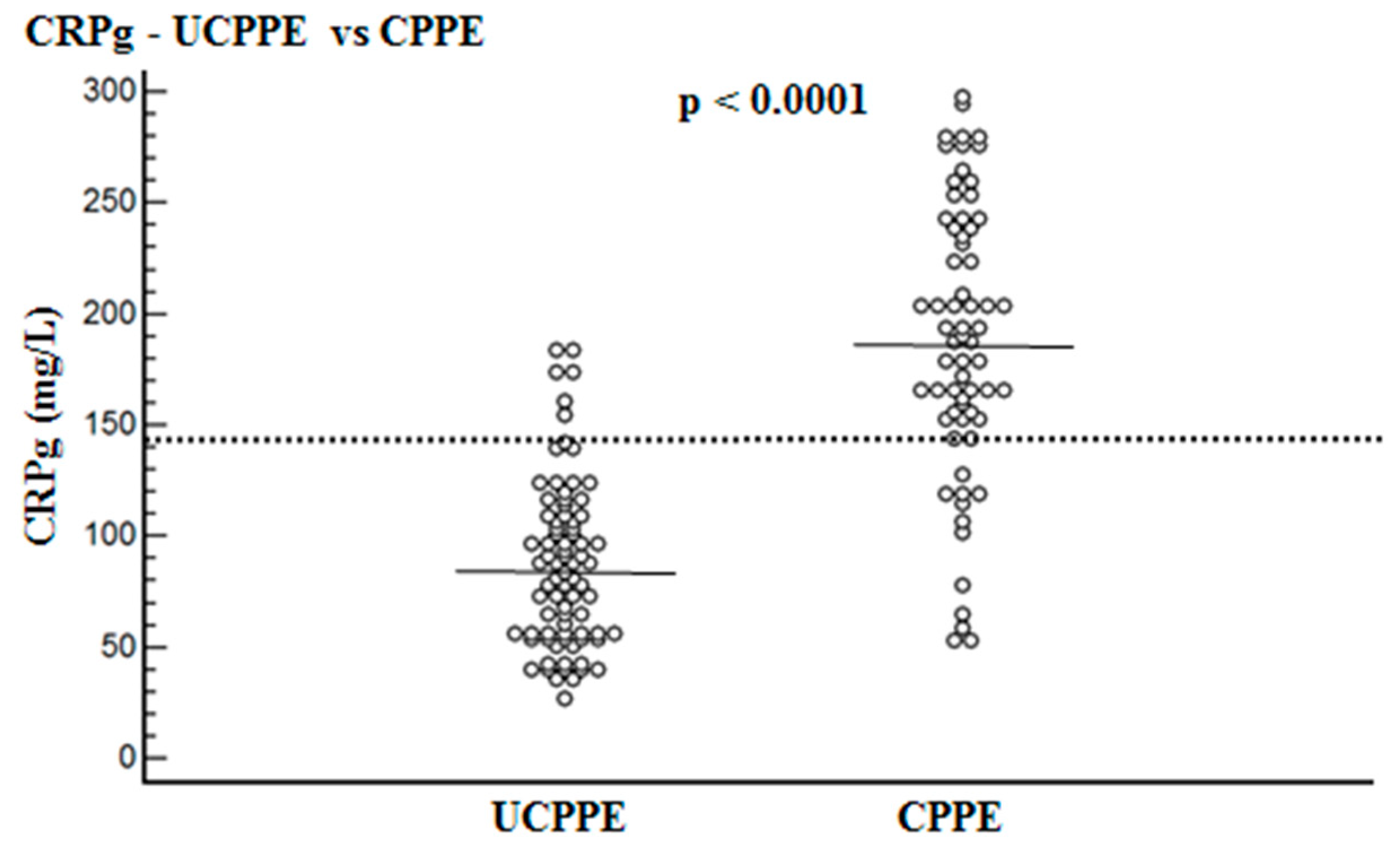
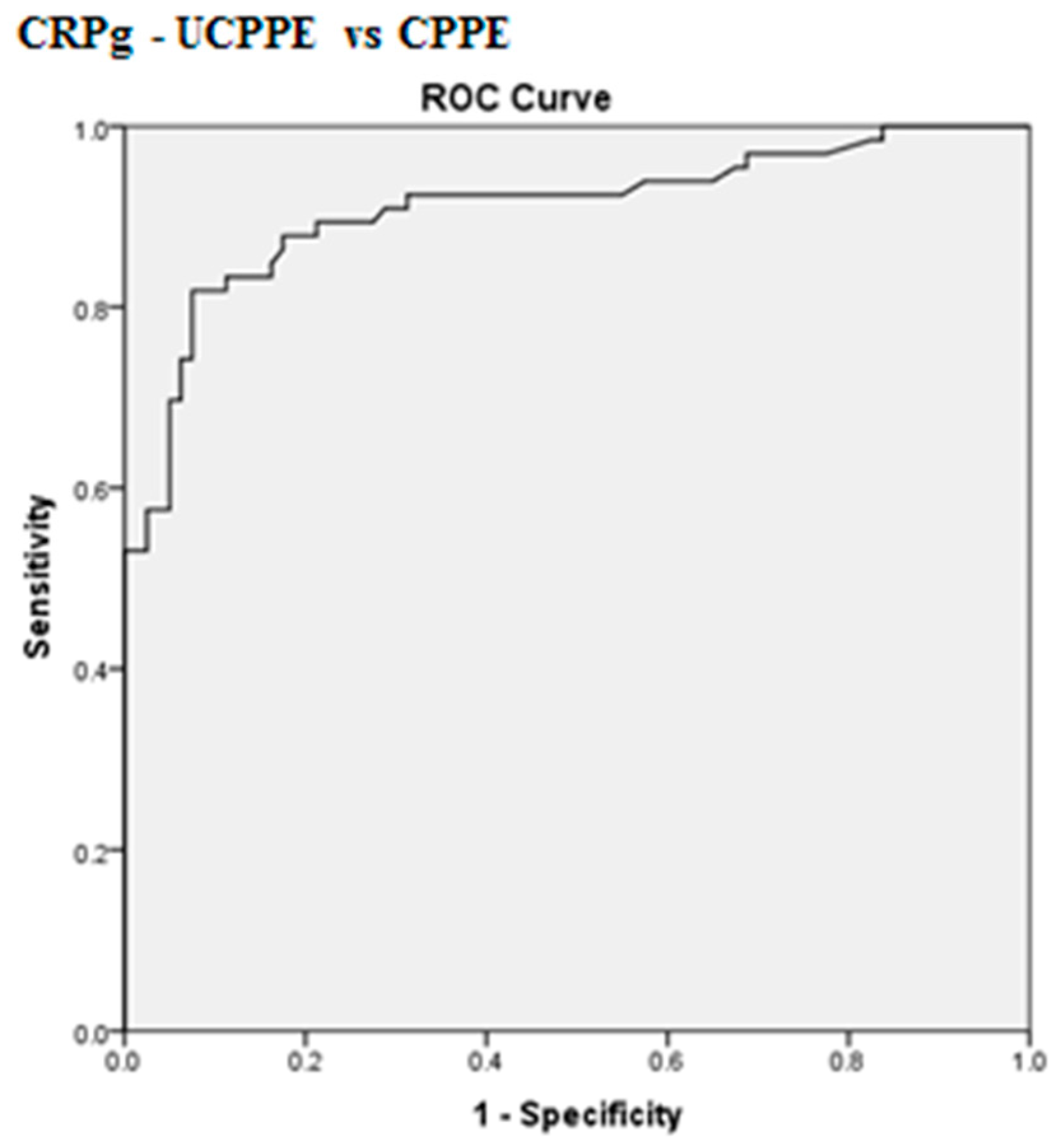
| CRPg (mg/L) 95% CI | 86.9 ± 37.3 48.6–99.2 | 188.3 ± 62.3 173.0–203.6 | <0.0001 |
| CRPr 95% CI | 0.39 ± 0.11 0.31–0.47 | 0.36 ± 0.19 0.25–0.39 | 0.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kogan, Y.; Sabo, E.; Odeh, M. Diagnostic Value of C-Reactive Protein in Discrimination between Uncomplicated and Complicated Parapneumonic Effusion. Diagnostics 2020, 10, 829. https://doi.org/10.3390/diagnostics10100829
Kogan Y, Sabo E, Odeh M. Diagnostic Value of C-Reactive Protein in Discrimination between Uncomplicated and Complicated Parapneumonic Effusion. Diagnostics. 2020; 10(10):829. https://doi.org/10.3390/diagnostics10100829
Chicago/Turabian StyleKogan, Yana, Edmond Sabo, and Majed Odeh. 2020. "Diagnostic Value of C-Reactive Protein in Discrimination between Uncomplicated and Complicated Parapneumonic Effusion" Diagnostics 10, no. 10: 829. https://doi.org/10.3390/diagnostics10100829