Cardiac Catheterization versus Echocardiography for Monitoring Pulmonary Pressure: A Prospective Study in Patients with Connective Tissue Disease-Associated Pulmonary Arterial Hypertension

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value
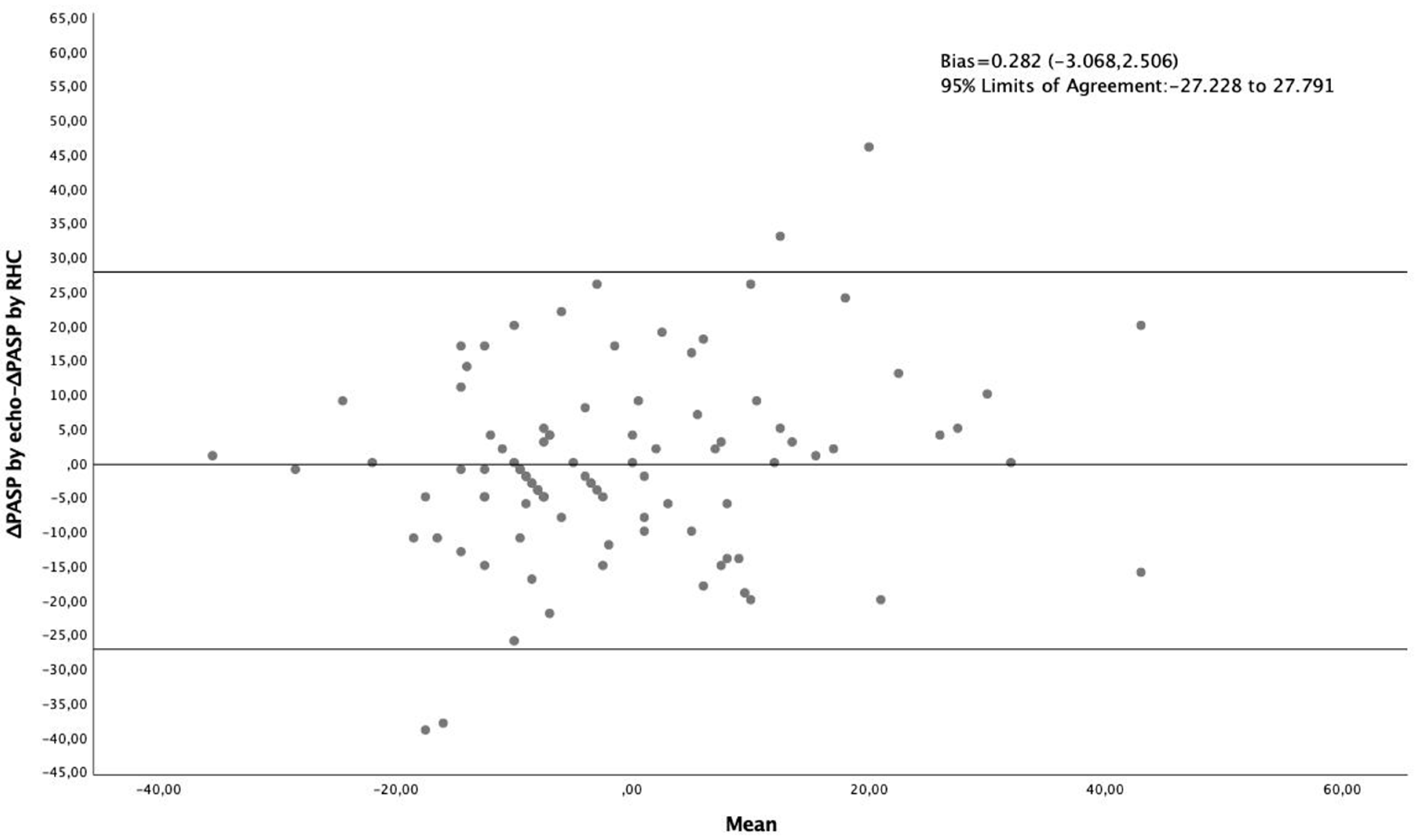
3.2. Bland Altman Analysis
3.3. Multivariate Binary Logistic Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sundaram, S.M.; Chung, L. An Update on Systemic Sclerosis-Associated Pulmonary Arterial Hypertension: A Review of the Current Literature. Curr. Rheumatol. Rep. 2018, 20, 10. [Google Scholar] [CrossRef]
- Vandecasteele, E.; Melsens, K.; Thevissen, K.; De Pauw, M.; Deschepper, E.; Decuman, S.; Piette, Y.; De Keyser, F.; Brusselle, G.; Smith, V. Prevalence and incidence of pulmonary arterial hypertension: 10-year follow-up of an unselected systemic sclerosis cohort. J. Scleroderma Relat. Disord. 2017, 2, 196–202. [Google Scholar] [CrossRef]
- Johnson, S.R.; Granton, J.T. Pulmonary hypertension in systemic sclerosis and systemic lupus erythematosus. Eur. Respir. Rev. 2011, 20, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Cano, M.J.; Escribano, P.; Alonso, R.; Delgado, J.; Carreira, P.; Velazquez, T.; Sanchez, M.A.G.; Sáenz de la Calzada, C. Comparison of Baseline Characteristics and Survival Between Patients With Idiopathic and Connective Tissue Disease–related Pulmonary Arterial Hypertension. J. Hear. Lung Transplant. 2009, 28, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Giordano, N.; Corallo, C.; Chirico, C.; Brazzi, A.; Marinetti, A.; Fioravanti, A.; Valenti, R.; Nuti, R.; Pecetti, G. Pulmonary arterial hypertension in systemic sclerosis: Diagnosis and treatment according to the European Society of Cardiology and European Respiratory Society 2015 guidelines. J. Scleroderma Relat. Disord. 2019, 4, 35–42. [Google Scholar] [CrossRef]
- Frost, A.; Badesch, D.; Gibbs, J.S.R.; Gopalan, D.; Khanna, D.; Manes, A.; Oudiz, R.; Satoh, T.; Torres, F.; Torbicki, A. Diagnosis of pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galiè, N.; Humbert, M.; Vachiery, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef] [PubMed]
- Mutlak, D.; Carasso, S.; Lessick, J.; Aronson, D.; Reisner, S.A.; Agmon, Y. Excessive respiratory variation in tricuspid regurgitation systolic velocities in patients with severe tricuspid regurgitation. Eur. Hear. J. Cardiovasc. Imaging 2013, 14, 957–962. [Google Scholar] [CrossRef] [Green Version]
- Boucly, A.; Weatherald, J.; Humbert, M.; Sitbon, O. Risk assessment in pulmonary arterial hypertension. Eur. Respir. J. 2018, 51, 1800279. [Google Scholar] [CrossRef]
- Humbert, M.; Weatherald, J. Right heart catheterisation is still a fundamental part of the follow-up assessment of pulmonary arterial hypertension. Eur. Respir. J. 2018, 52, 1800738. [Google Scholar] [CrossRef] [Green Version]
- Howard, L.S. Is right heart catheterisation still a fundamental part of the follow-up assessment of pulmonary arterial hypertension? The argument against. Eur. Respir. J. 2018, 52, 1800996. [Google Scholar] [CrossRef] [PubMed]
- Taleb, M.; Khuder, S.; Tinkel, J.; Khouri, S.J. The Diagnostic Accuracy of Doppler Echocardiography in Assessment of Pulmonary Artery Systolic Pressure: A Meta-Analysis. Echocardiography 2013, 30, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Finkelhor, R.S.; Lewis, S.A.; Pillai, D. Limitations and Strengths of Doppler/Echo Pulmonary Artery Systolic Pressure-Right Heart Catheterization Correlations: A Systematic Literature Review. Echocardiography 2015, 32, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Janda, S.; Shahidi, N.; Gin, K.; Swiston, J. Diagnostic accuracy of echocardiography for pulmonary hypertension: A systematic review and meta-analysis. Heart 2011, 97, 612–622. [Google Scholar] [CrossRef] [Green Version]
- Farber, H.W.; Foreman, A.J.; Miller, D.P.; McGoon, M.D. REVEAL Registry: Correlation of Right Heart Catheterization and Echocardiography in Patients With Pulmonary Arterial Hypertension. Congest. Hear. Fail. 2011, 17, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Denton, C.P.; Cailes, J.B.; Phillips, G.D.; Wells, A.U.; Black, C.M.; Bois, R.M. Comparison of Doppler echocardiography and right heart catheterization to assess pulmonary hypertension in systemic sclerosis. Br. J. Rheumatol. 1997, 36, 239–243. [Google Scholar] [CrossRef] [Green Version]
- Hsu, V.M.; Moreyra, A.E.; Wilson, A.C.; Shinnar, M.; Shindler, D.M.; Wilson, J.E.; Desai, A.; Seibold, J.R. Assessment of pulmonary arterial hypertension in patients with systemic sclerosis: Comparison of noninvasive tests with results of right-heart catheterization. J. Rheumatol. 2008, 35, 458–465. [Google Scholar]
- Weatherald, J.; Boucly, A.; Chemla, D.; Savale, L.; Peng, M.; Jevnikar, M.; Jaïs, X.; Taniguchi, Y.; O’Connell, C.; Parent, F.; et al. Prognostic Value of Follow-Up Hemodynamic Variables After Initial Management in Pulmonary Arterial Hypertension. Circulation 2018, 137, 693–704. [Google Scholar] [CrossRef]
- Weatherald, J.; Boucly, A.; Launay, D.; Cottin, V.; Prévot, G.; Bourlier, D.; Dauphin, C.; Chaouat, A.; Savale, L.; Jaïs, X.; et al. Haemodynamics and serial risk assessment in systemic sclerosis associated pulmonary arterial hypertension. Eur. Respir. J. 2018, 52, 1800678. [Google Scholar] [CrossRef] [Green Version]
- Mercurio, V.; Diab, N.; Peloquin, G.; Housten-Harris, T.; Damico, R.; Kolb, T.M.; Mathai, S.C.; Hassoun, P.M. Risk assessment in scleroderma patients with newly diagnosed pulmonary arterial hypertension: Application of the ESC/ERS risk prediction model. Eur. Respir. J. 2018, 52, 1800497. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, C.; Chan, J.; Bricknell, K.; Strudwick, M.; Marwick, T.H. Reproducibility of Right Ventricular Volumes and Ejection Fraction Using Real-time Three-Dimensional Echocardiography. Chest 2007, 131, 1844–1851. [Google Scholar] [CrossRef] [PubMed]
- Vonk Noordegraaf, A.; Chin, K.M.; Haddad, F.; Hassoun, P.M.; Hemnes, A.R.; Hopkins, S.R.; Kawut, S.M.; Langleben, D.; Lumens, J.; Naeije, R. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: An update. Eur. Respir. J. 2019, 53, 1801900. [Google Scholar] [CrossRef] [PubMed]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.R.; Forfia, P.R.; Chamera, E.; Housten-Harris, T.; Champion, H.C.; Girgis, R.E.; Corretti, M.C.; Hassoun, P.M. Accuracy of Doppler echocardiography in the hemodynamic assessment of pulmonary hypertension. Am. J. Respir. Crit. Care Med. 2009, 179, 615–621. [Google Scholar] [CrossRef]
- Thalhammer, C.; Aschwanden, M.; Odermatt, A.; Baumann, U.A.; Imfeld, S.; Bilecen, D.; Marsch, S.C.; Jaeger, K.A. Noninvasive central venous pressure measurement by controlled compression sonography at the forearm. J. Am. Coll. Cardiol. 2007, 50, 1584–1589. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| N (%) | Age (Years) | Echo-Derived PASP (mmHg) | RHC-Derived PASP (mmHg) | PVR (WU) | Cardiac Index | RAP (mmHg) | NT-pro-BNP (pg/mL) | 6mWD (m) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Underlying disease | SSc | 58 (84) | 61.45 ± 11.68 | 65.72 ± 17.01 | 59.02 ± 16.23 | 6.41 ± 2.96 (n = 55) | 2.50 ± 0.63 | 6.62 ± 3.52 | 1848.69 ± 2643.41 (n = 45) | 357.74 ± 124.69 (n = 43) |
| MCTD | 6 (9) | 63.17 ± 8.75 | 61.67 ± 27.66 | 60.50 ± 13.66 | 6.35 ± 3.39 | 2.40 ± 2.4 | 8.17 ± 3.54 | 1493.67 ± 1540.89 (n = 3) | 378.0 ± 75.78 | |
| SLE | 5 (7) | 49.00 ± 13.3 | 64.20 ± 19.38 | 73.40 ± 17.57 | 7.05 ± 2.79 (n = 4) | 2.42 ± 0.10 | 9.0 ± 4.53 | 4142.75 ± 5678.68 (n = 4) | 290.0 ± 262.11 (n = 3) | |
| Gender | female | 59 (86) | 61.64 ± 11.95 | 63.58 ± 17.82 | 59.31 ± 16.81 | 6.42 ± 3.12 (n = 57) | 2.51 ± 0.58 | 6.82 ± 3.71 | 2129.72 ± 3053.44 (n = 46) | 351.94 ± 132.31 (n = 48) |
| male | 10 (14) | 55.10 ± 10.47 | 75.2 ± 16.14 | 65.4 ± 12.57 | 6.55 ± 1.24 (n = 8) | 2.32 ± 0.59 | 7.6 ± 2.99 | 1046.0 ± 814.72 (n = 4) | 407.0 ± 19.90 (n = 4) | |
| NYHA stage | I | 0 | - | - | - | - | - | - | - | - |
| II | 22 (32) | 56.91 ± 12.01 | 55.45 ± 13.43 * | 56.77 ± 13.49 | 5.55 ± 1.7 | 2.56 ± 0.33 | 6.18 ± 2.36 | 723.76 ± 1013.77 (n = 17) | 442.6 ± 69.80 ** (n = 20) | |
| III | 37 (54) | 62.38 ± 11.85 | 65.57 ± 16.94 * | 57.72 ± 16.31 | 5.95 ± 2.79 (n = 34) | 2.57 ± 0.66 | 6.49 ± 3.62 | 1657.48 ± 2004.25 (n = 27) | 348.62 ± 65.98 ** (n = 26) | |
| IV | 10 (14) | 62.80 ± 10.94 | 85.7 ± 12.92 * | 76.8 ± 12.88 # | 10.49 ± 2.89 # (n = 9) | 2.00 ± 0.51 # | 10.2 ± 4.37 # | 5897.37 ± 4717.60 # (n = 8) | 100.83 ± 135.44 ** (n = 6) | |
| Total cohort | 69 (100) | 60.70 ± 11.90 | 65.26 ± 17.95 | 60.19 ± 16.33 | 6.44 ± 2.95 | 2.48 ± 0.59 | 6.93 ± 3.61 | 2004.67 ± 2900.68 | 356.17 ± 127.96 | |
| 1st Follow-up | 2nd Follow-up | ||
|---|---|---|---|
| N (%) | 69 (100%) | 27 (39%) | |
| Age (years) | 61.35 ± 12.25 | 61.80 ± 11.85 | |
| Female gender (%) | 59 (86) | 24 (89) | |
| Underlying disease | SSc | 58 (84) | 24 (89) |
| MCTD | 6 (9) | 1 (4) | |
| SLE | 5 (7) | 2 (7) | |
| Time to follow-up (months) | 9.47 ± 7.29 | 8.29 ± 4.36 | |
| NYHA stage (%) | I | 2 (3) | - |
| II | 32 (46) | 14 (52) | |
| III | 33 (48) | 13 (48) | |
| IV | 2 (3) | - | |
| Echo-derived PASP (mmHg) | 62.65 ± 20.30 | 68.70 ± 26.90 | |
| RHC-derived PASP (mmHg) | 56.65 ± 16.5 | 65.30 ± 18.63 | |
| PVR (wood units) | 6.02 ± 3.04 | 7.34 ± 3.15 | |
| Cardiac Index | 2.68 ± 0.59 | 2.51 ± 0.37 | |
| RAP (mmHg) | 7.33 ± 4.3 | 7.26 ± 4.06 | |
| NT-pro-BNP (pg/mL) | 1197.89 ± 1507.77 (n = 54) | 1356.4 ± 1300.64 (n = 20) | |
| 6mWD (m) | 389.20 ± 83.94 (n = 46) | 412.0 ± 79.28 (n = 16) | |
| RHC-Derived PASP | ||||
|---|---|---|---|---|
| Deteriorated ≥ 10% | Stable or Improved ≥ 10% | Total | ||
| Echo-derived PASP | Deteriorated ≥ 10% | 17 | 10 | 27 |
| stable or improved ≥ 10% | 12 | 57 | 69 | |
| total | 29 | 67 | 96 | |
| RHC-Derived PASP | ||||
|---|---|---|---|---|
| Deteriorated ≥ 10% | Stable or Improved ≥ 10% | Total | ||
| Echo-derived PASP | Deteriorated ≥ 10% | 11 | 4 | 15 |
| stable or improved ≥ 10% | 4 | 39 | 43 | |
| total | 15 | 43 | 58 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bournia, V.K.; Tsangaris, I.; Rallidis, L.; Konstantonis, D.; Frantzeskaki, F.; Anthi, A.; Orfanos, S.E.; Demerouti, E.; Karyofillis, P.; Voudris, V.; et al. Cardiac Catheterization versus Echocardiography for Monitoring Pulmonary Pressure: A Prospective Study in Patients with Connective Tissue Disease-Associated Pulmonary Arterial Hypertension. Diagnostics 2020, 10, 49. https://doi.org/10.3390/diagnostics10010049
Bournia VK, Tsangaris I, Rallidis L, Konstantonis D, Frantzeskaki F, Anthi A, Orfanos SE, Demerouti E, Karyofillis P, Voudris V, et al. Cardiac Catheterization versus Echocardiography for Monitoring Pulmonary Pressure: A Prospective Study in Patients with Connective Tissue Disease-Associated Pulmonary Arterial Hypertension. Diagnostics. 2020; 10(1):49. https://doi.org/10.3390/diagnostics10010049
Chicago/Turabian StyleBournia, Vasiliki Kalliopi, Iraklis Tsangaris, Loukianos Rallidis, Dimitrios Konstantonis, Frantzeska Frantzeskaki, Anastasia Anthi, Stylianos E. Orfanos, Eftychia Demerouti, Panagiotis Karyofillis, Vassilis Voudris, and et al. 2020. "Cardiac Catheterization versus Echocardiography for Monitoring Pulmonary Pressure: A Prospective Study in Patients with Connective Tissue Disease-Associated Pulmonary Arterial Hypertension" Diagnostics 10, no. 1: 49. https://doi.org/10.3390/diagnostics10010049