A New Diagnostic Approach for Periprosthetic Acetabular Fractures Based on 3D Modeling: A Study Protocol


Abstract
:
1. Introduction
2. Methods and Results
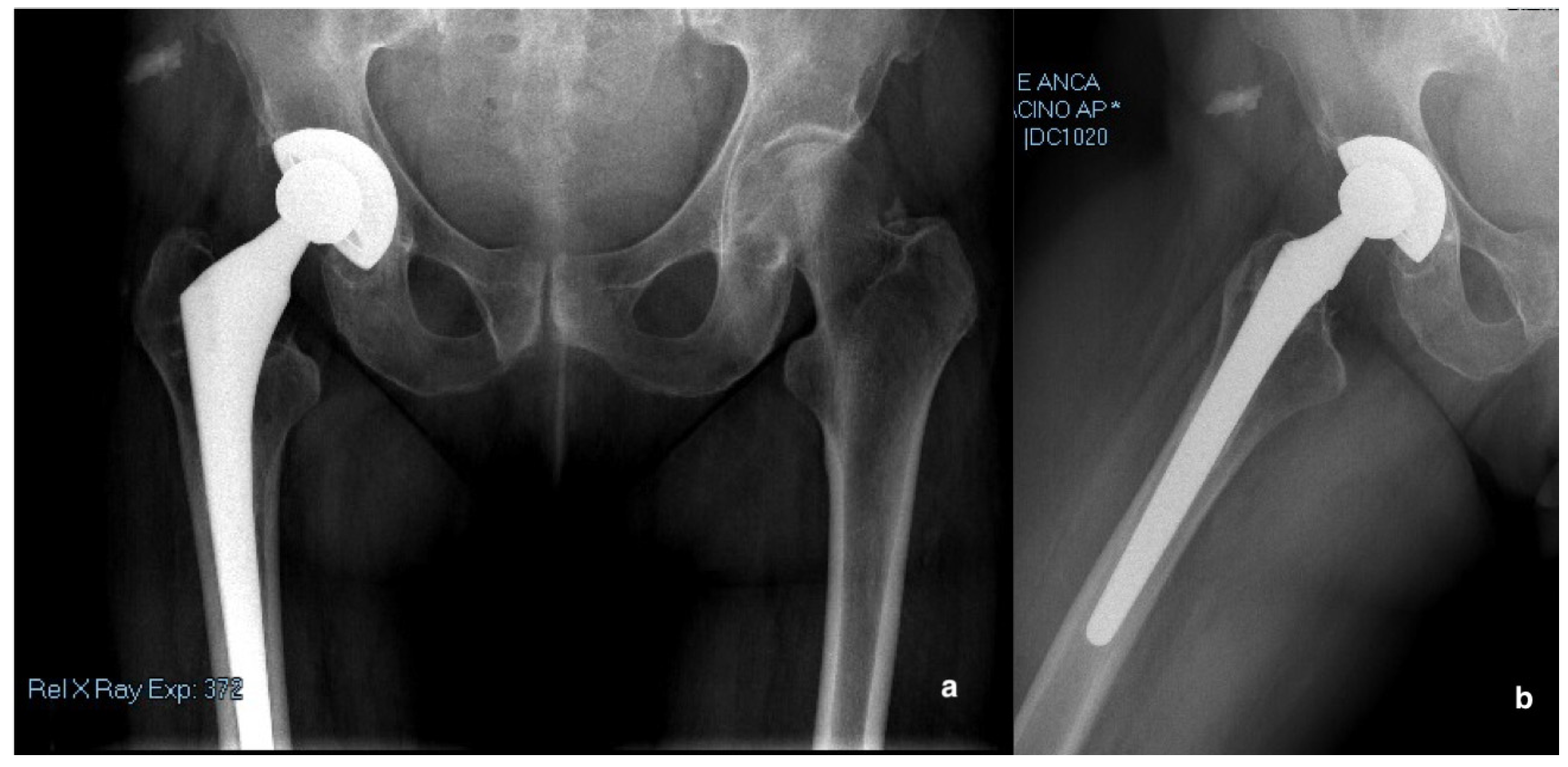
2.1. Case Report
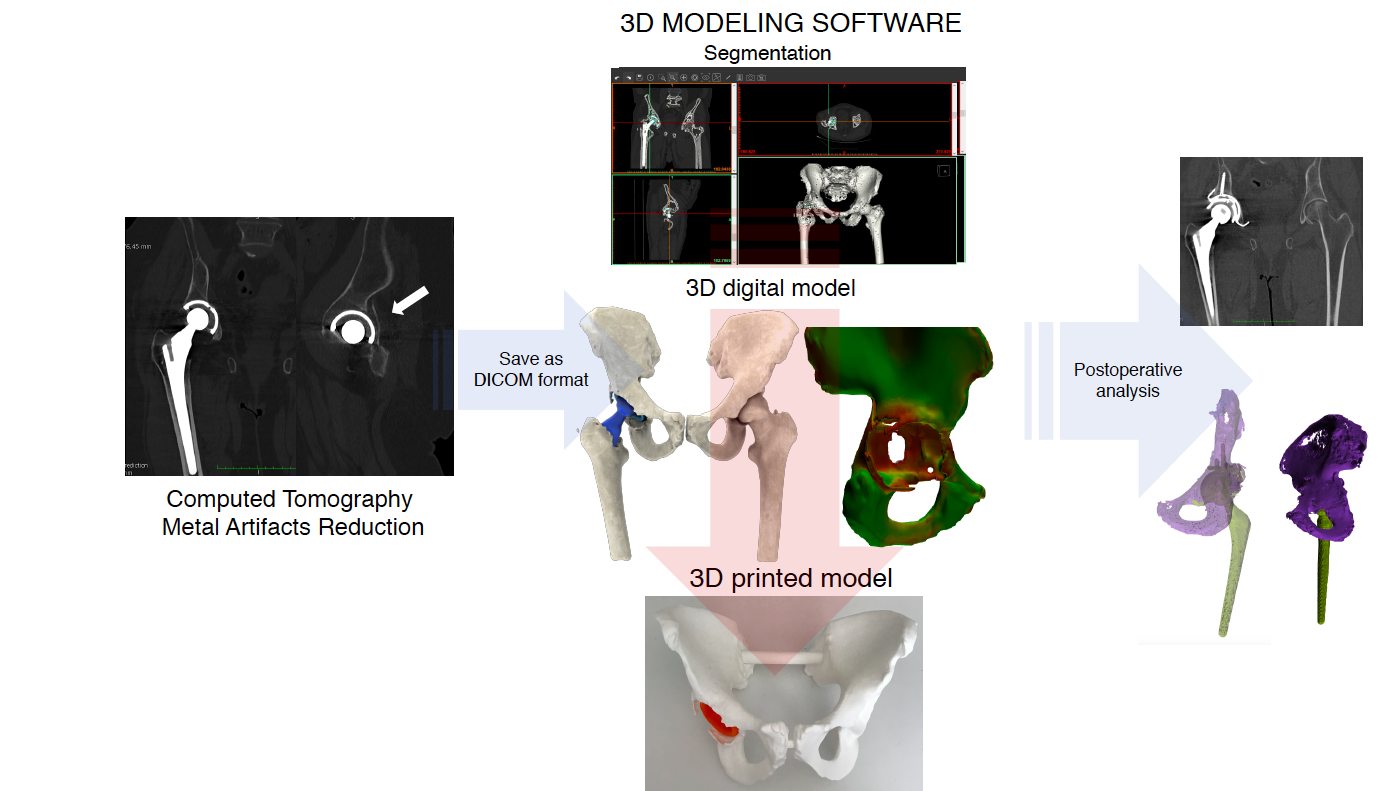
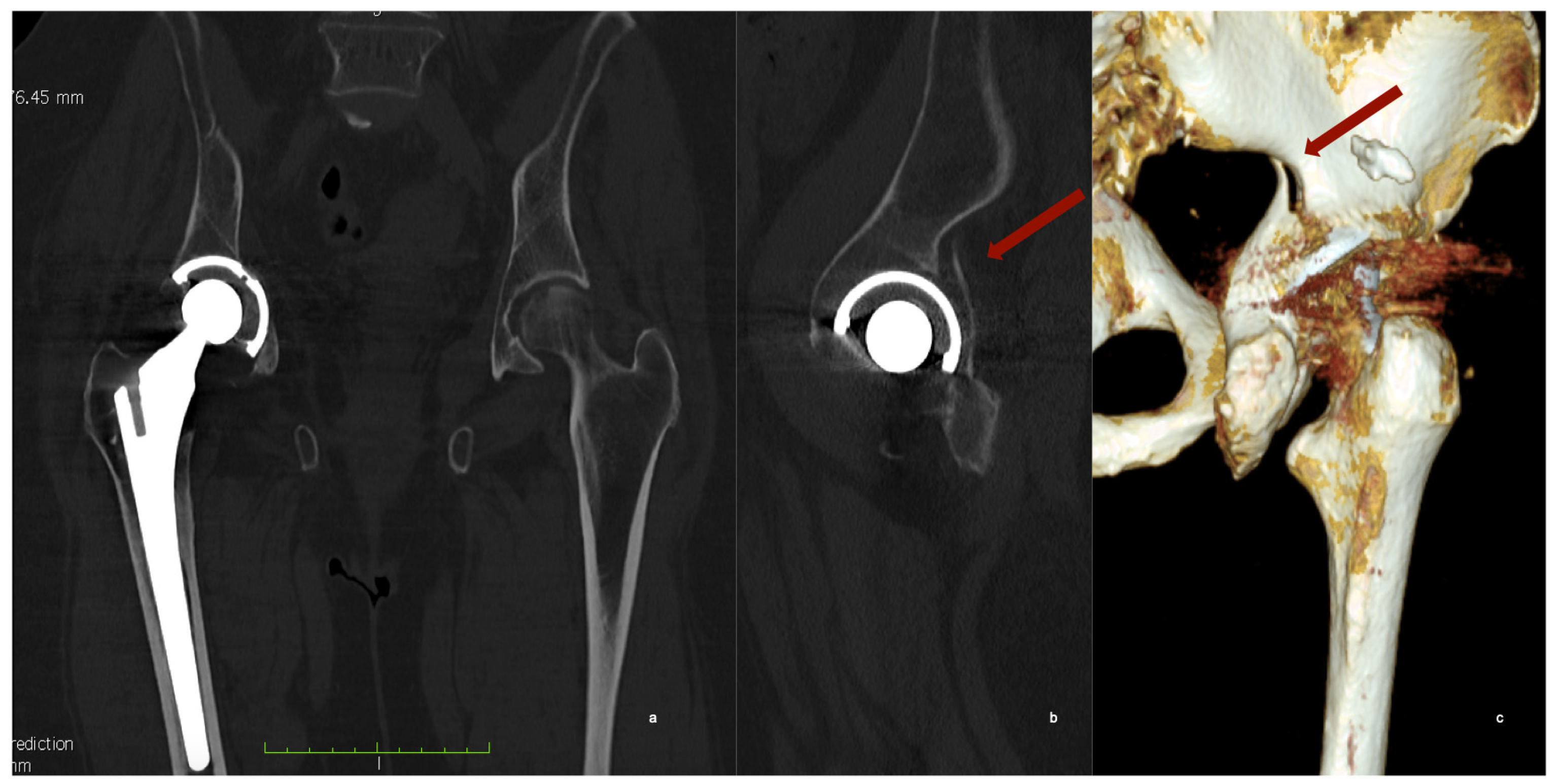
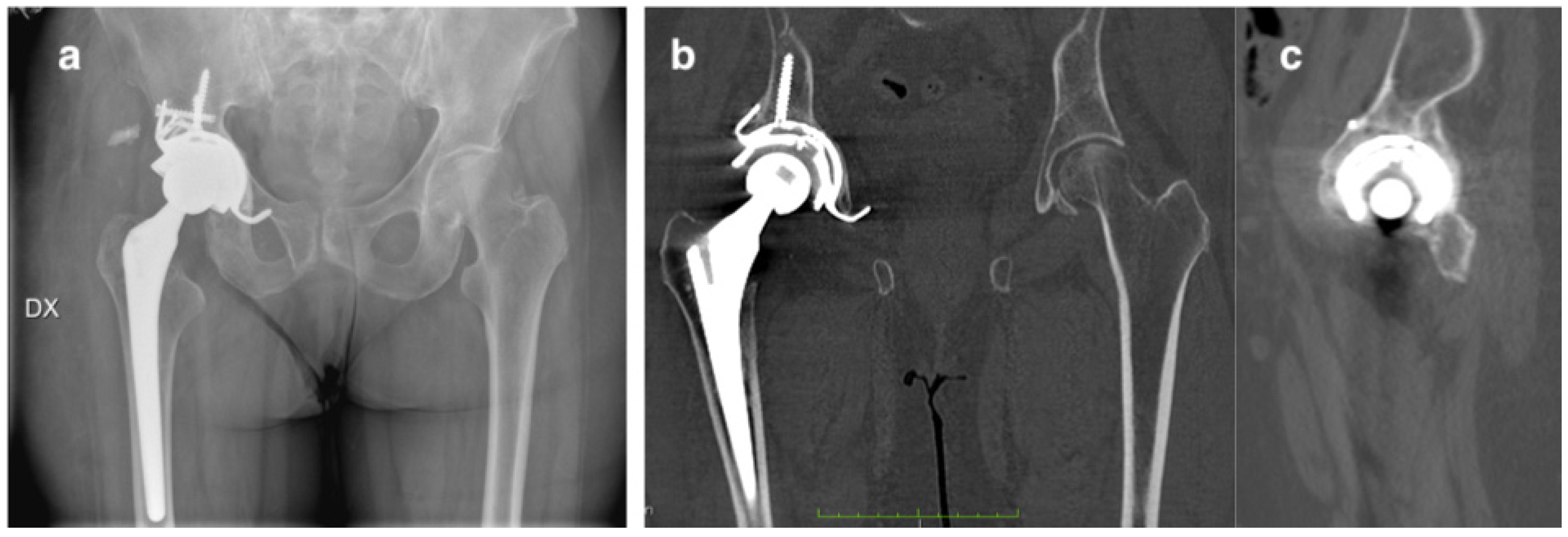
2.2. Computed Tomography with Metal Artefacts Reduction (MAR)
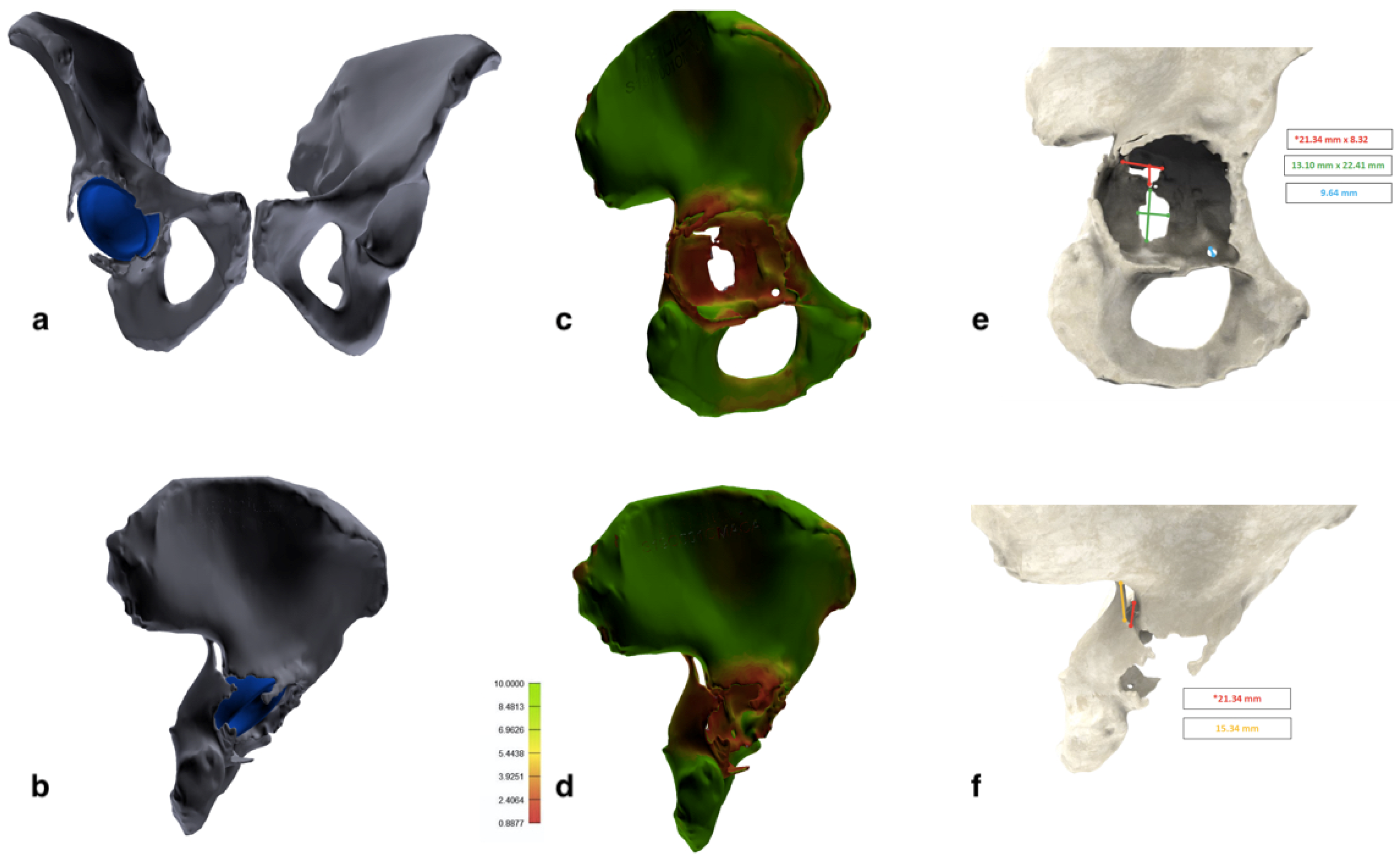
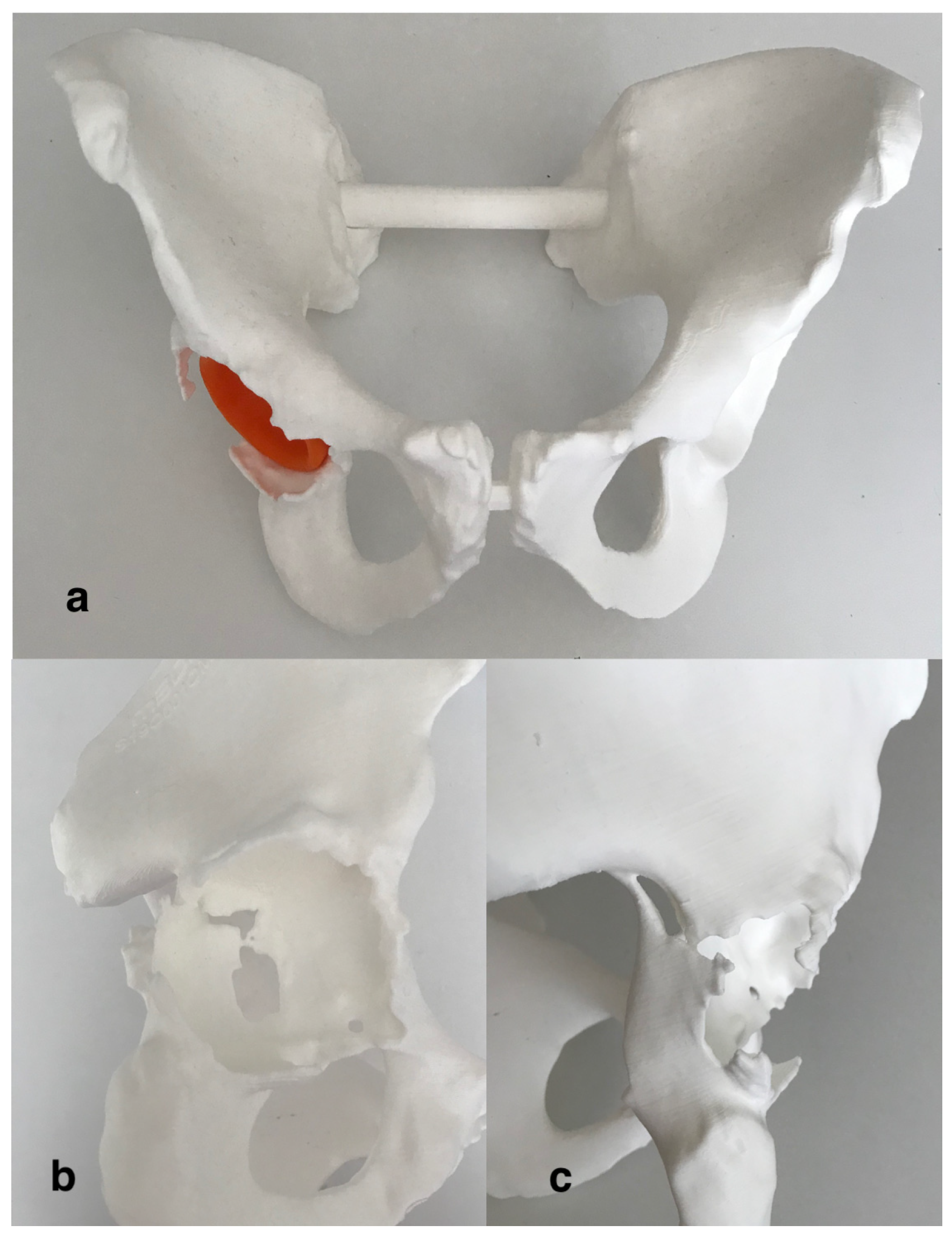
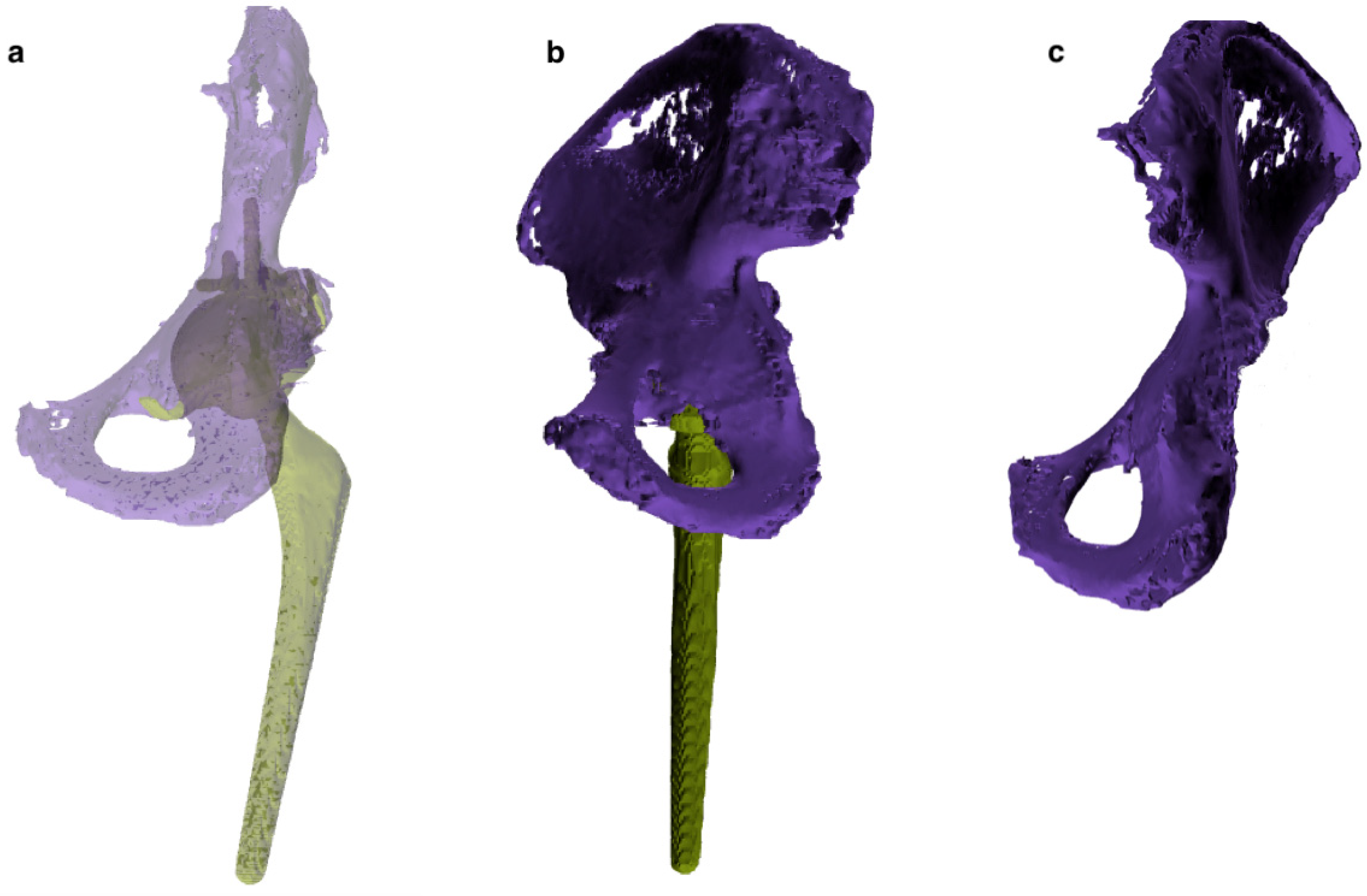
2.3. 3D Modeling and Rapid Prototyping Process
2.4. Classification, Planning and Surgical Procedure
2.5. Outcome
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Benazzo, F.; Formagnana, M.; Bargagliotti, M.; Perticarini, L. Periprosthetic acetabular fractures. Int. Orthop. SICOT 2015, 39, 1959–1963. [Google Scholar] [CrossRef]
- Capone, A.; Peri, M.; Mastio, M. Surgical treatment of acetabular fractures in the elderly: A systematic review of the results. EFORT Open Rev. 2017, 2, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, N.; Pappedemos, P.C.; Duffy, P.R.; Stepniewski, A.S.; Hopper, R.H.; Engh, C.A.; Engh, C.A. The Value of Anteroposterior Pelvic Radiographs for Evaluating Pelvic Osteolysis. Clin. Orthop. Relat. Res. 2006, 453, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Egawa, H.; Powers, C.C.; Beykirch, S.E.; Hopper, R.H.; Engh, C.A.; Engh, C.A. Can the Volume of Pelvic Osteolysis be Calculated without Using Computed Tomography? Clin. Orthop. Relat. Res. 2009, 467, 181–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandgren, B.; Crafoord, J.; Garellick, G.; Carlsson, L.; Weidenhielm, L.; Olivecrona, H. Computed tomography vs. digital radiography assessment for detection of osteolysis in asymptomatic patients with uncemented cups: A proposal for a new classification system based on computer tomography. J. Arthroplast. 2013, 28, 1608–1613. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Subhas, N.; Primak, A.N.; Nittka, M.; Liu, K. Metal Artifact Reduction. Radiol. Clin. N. Am. 2015, 53, 531–547. [Google Scholar] [CrossRef]
- Capone, A. Periprosthetic fractures: Epidemiology and current treatment. Clin. Cases Miner. Bone Metab. 2017, 14, 189. [Google Scholar] [CrossRef]
- Horas, K.; Arnholdt, J.; Steinert, A.F.; Hoberg, M.; Rudert, M.; Holzapfel, B.M. Acetabular defect classification in times of 3D imaging and patient-specific treatment protocols. Orthopäde 2017, 46, 168–178. [Google Scholar] [CrossRef]
- Gelaude, F.; Clijmans, T.; Delport, H. Quantitative Computerized Assessment of the Degree of Acetabular Bone Deficiency: Total radial Acetabular Bone Loss (TrABL). Adv. Orthop. 2011, 2011, 494382. [Google Scholar] [CrossRef] [Green Version]
- Won, S.H.; Lee, Y.K.; Ha, Y.C.; Suh, Y.S.; Koo, K.H. Improving pre-operative planning for complex total hip replacement with a Rapid Prototype model enabling surgical simulation. Bone Jt. J. 2013, 95, 1458–1463. [Google Scholar] [CrossRef]
- Hughes, A.J.; DeBuitleir, C.; Soden, P.; O’Donnchadha, B.; Tansey, A.; Abdulkarim, A.; McMahon, C.; Hurson, C.J. 3D Printing Aids Acetabular Reconstruction in Complex Revision Hip Arthroplasty. Adv. Orthop. 2017, 2017, 8925050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, R.; Zhai, Z.; Chang, Y.; Li, H. Clinical Applications of 3-Dimensional Printing Technology in Hip Joint. Orthop. Surg. 2019, 11, 533–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capone, A.; Bienati, F.; Torchia, S.; Podda, D.; Marongiu, G. Short stem total hip arthroplasty for osteonecrosis of the femoral head in patients 60 years or younger: A 3- to 10-year follow-up study. BMC Musculoskelet. Disord. 2017, 18, 301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, L.; Zhang, X.; Zhang, S.; Li, K.; Cao, P.; Li, J.; Wu, G. Clinical feasibility and application value of computer virtual reduction combined with 3D printing technique in complex acetabular fractures. Exp. Med. 2019, 17, 3630–3636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lal, H.; Patralekh, M.K. 3D printing and its applications in orthopaedic trauma: A technological marvel. J. Clin. Orthop. Trauma 2018, 9, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Oftadeh, R.; Perez-Viloria, M.; Villa-Camacho, J.C.; Vaziri, A.; Nazarian, A. Biomechanics and mechanobiology of trabecular bone: A review. J. Biomech. Eng. 2015, 137, 010802. [Google Scholar] [CrossRef] [Green Version]
- Kasparek, M.F.; Töpker, M.; Lazar, M.; Weber, M.; Kasparek, M.; Mang, T.; Apfaltrer, P.; Kubista, B.; Windhager, R.; Ringl, H. Dual-energy CT and ceramic or titanium prostheses material reduce CT artifacts and provide superior image quality of total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1552–1561. [Google Scholar] [CrossRef] [Green Version]
- Della Valle, C.J.; Momberger, N.G.; Paprosky, W.G. Periprosthetic fractures of the acetabulum associated with a total hip arthroplasty. Instr. Course Lect. 2003, 52, 281–290. [Google Scholar]
- Simon, P.; von Roth, P.; Perka, C. Treatment algorithm of acetabular periprosthetic fractures. Int. Orthop. SICOT 2015, 39, 1995–2003. [Google Scholar] [CrossRef]
- Klässbo, M.; Larsson, E.; Mannevik, E. Hip disability and osteoarthritis outcome score. An extension of the Western Ontario and McMaster Universities Osteoarthritis Index. Scand. J. Rheumatol. 2003, 32, 46–51. [Google Scholar] [CrossRef]
- Salvi, M.; Caputo, F.; Piu, G.; Sanna, M.; Sanna, C.; Marongiu, G. The loss of extension test (LOE test): A new clinical sign for the anterior cruciate ligament insufficient knee. J. Orthopaed. Traumatol. 2013, 14, 185–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, W.H. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J. Bone Jt. Surg. Am. 1969, 51, 737–755. [Google Scholar] [CrossRef]
- Marongiu, G.; Podda, D.; Mastio, M.; Capone, A. Long-term results of isolated acetabular revisions with reinforcement rings: A 10- to 15-year follow-up. HIP Int. 2019, 29, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.; Xing, W.; Wu, Z.; Huang, H.; Huang, W. A combination of three-dimensional printing and computer-assisted virtual surgical procedure for preoperative planning of acetabular fracture reduction. Injury 2016, 47, 2223–2227. [Google Scholar] [CrossRef] [PubMed]
- Maini, L.; Verma, T.; Sharma, A.; Sharma, A.; Mishra, A.; Jha, S. Evaluation of accuracy of virtual surgical planning for patient-specific pre-contoured plate in acetabular fracture fixation. Arch. Orthop. Trauma Surg. 2018, 138, 495–504. [Google Scholar] [CrossRef]
- Li, Y.T.; Hung, C.C.; Chou, Y.C.; Chen, J.E.; Wu, C.C.; Shen, H.C.; Yeh, T.T. Surgical Treatment for Posterior Dislocation of Hip Combined with Acetabular Fractures Using Preoperative Virtual Simulation and Three-Dimensional Printing Model-Assisted Precontoured Plate Fixation Techniques. BioMed Res. Int. 2019, 2019, 3971571. [Google Scholar] [CrossRef] [Green Version]
- Kavalerskiy, G.; Murylev, V.; Rukin, Y.; Elizarov, P.; Lychagin, A.; Tselisheva, E. Three-dimensional models in planning of revision hip arthroplasty with complex acetabular defects. Indian J. Orthop. 2018, 52, 625. [Google Scholar]
- Aprato, A.; Olivero, M.; Iannizzi, G.; Bistolfi, A.; Sabatini, L.; Masse, A. Pelvic discontinuity in acetabular revisions: Does CT scan overestimate it? A comparative study of diagnostic accuracy of 3D-modeling and traditional 3D CT scan. Musculoskelet. Surg. 2019. [Google Scholar] [CrossRef]
- Baauw, M.; van Hellemondt, G.G.; Spruit, M. A Custom-made Acetabular Implant for Paprosky Type 3 Defects. Orthopedics 2017, 40, e195–e198. [Google Scholar]
- Pierce, T.P.; Cherian, J.J.; Jauregui, J.J.; Elmallah, R.D.K.; Mont, M.A. Outcomes of post-operative periprosthetic acetabular fracture around total hip arthroplasty. Expert Rev. Med. Devices 2015, 12, 307–315. [Google Scholar] [CrossRef]
- Marongiu, G.; Capone, A. Atypical periprosthetic acetabular fracture in long-term alendronate therapy. Clin. Cases Min. Bone Metab. 2016, 13, 209–213. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Components | Materials | Elastic Modulus (MPa) | Density | Hounsfield Unit (HU) Values | |
|---|---|---|---|---|---|
| Cortical bone | Cortical bone | 17,300 | 1.6–2 g/mm3 (porosity 10%) | 1500 | |
| Cancellous bone | Cancellous bone | 400 | 0.05–0.3 g/mm3 (porosity 70%) | 200–700 | |
| Femoral prosthesis (Osteonics, Omnifit, Stryker) | Titanium alloy + Hidroxyapatite | 110,600 | 4.43 g/cm3 | 3071 | |
| Acetabular cup (Osteonics, Omnifit, Stryker) | Titanium alloy + Hidroxyapatite | 110,600 | 4.43 g/cm3 | 3071 | |
| Acetabular revision cup (Delta Revision TT, Lima) | Trabecular Titanium | 8963 | 4.43 g/cm3 (porosity 60%) | 2840–3071 | |
| Screws | Titanium alloy | 110,600 | 4.43 g/cm3 | 3071 | |
| Polyethilene insert | Ultra-High-Molecular-Weight Polyethylene | 1500 | 0.93 g/cm3 | 19–53 | |
| Metallic femoral head | Cobalt–chromium alloy | 230,000 | 8.2 g/cm3 | 3071 | |
| Ceramic femoral head | Alumina | 350,000 | 4.1 g/cm3 | 3071 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marongiu, G.; Prost, R.; Capone, A. A New Diagnostic Approach for Periprosthetic Acetabular Fractures Based on 3D Modeling: A Study Protocol. Diagnostics 2020, 10, 15. https://doi.org/10.3390/diagnostics10010015
Marongiu G, Prost R, Capone A. A New Diagnostic Approach for Periprosthetic Acetabular Fractures Based on 3D Modeling: A Study Protocol. Diagnostics. 2020; 10(1):15. https://doi.org/10.3390/diagnostics10010015
Chicago/Turabian StyleMarongiu, Giuseppe, Roberto Prost, and Antonio Capone. 2020. "A New Diagnostic Approach for Periprosthetic Acetabular Fractures Based on 3D Modeling: A Study Protocol" Diagnostics 10, no. 1: 15. https://doi.org/10.3390/diagnostics10010015