
Mechanical Design and Analysis of the End-Effector Finger Rehabilitation Robot (EFRR) for Stroke Patients


Abstract
:1. Introduction
2. The Innovative Design of the EFRR
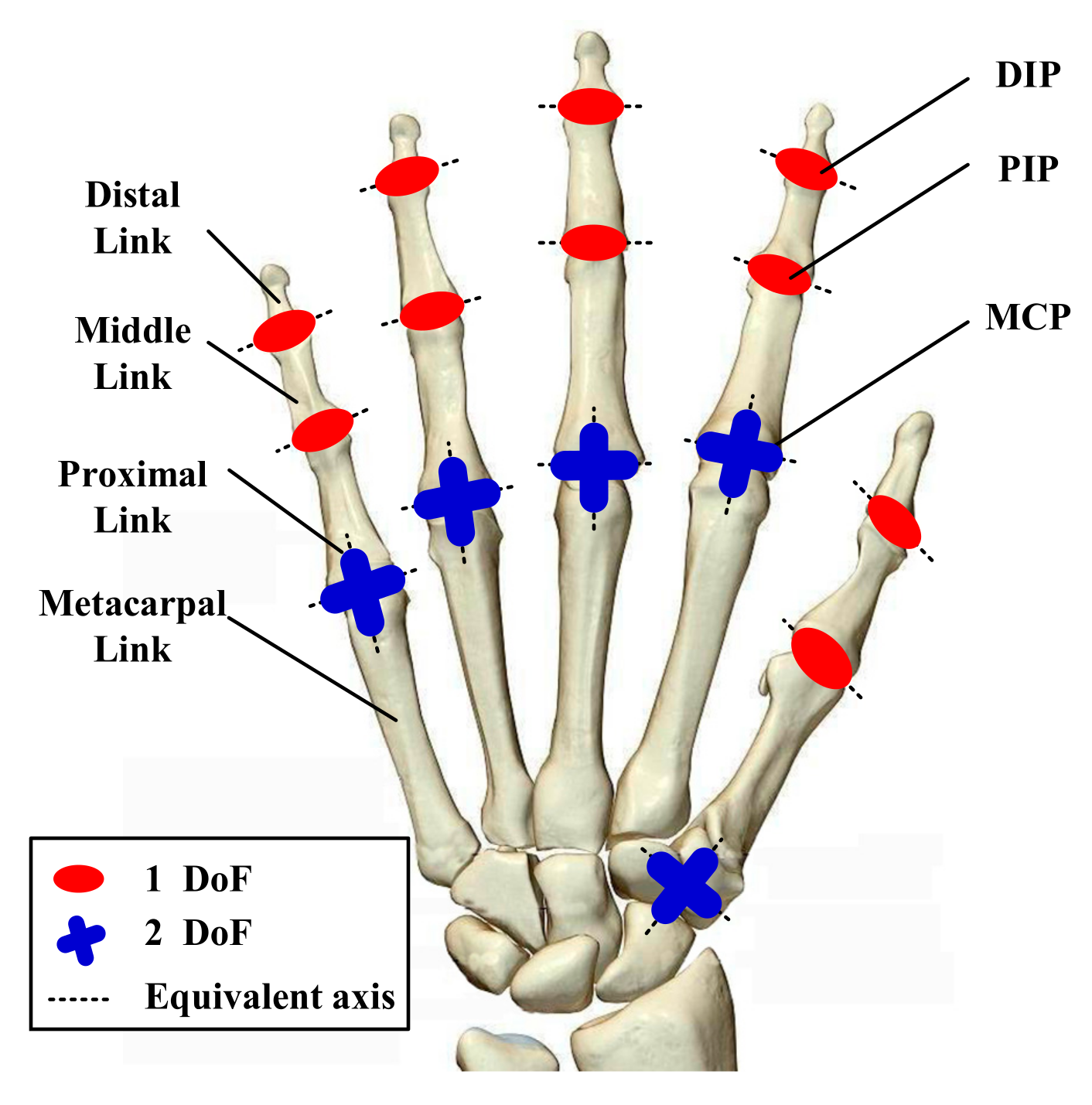
2.1. Anatomy-Based Finger Movement Analysis
2.2. Design Requirements and Preliminary Conception for the Prototype
- Rational finger F/E-coupled motion trajectory;
- Active A/A motion of the four fingers;
- Compliant control strategy that can ensure safety at all time;
- Easy-to-wear.
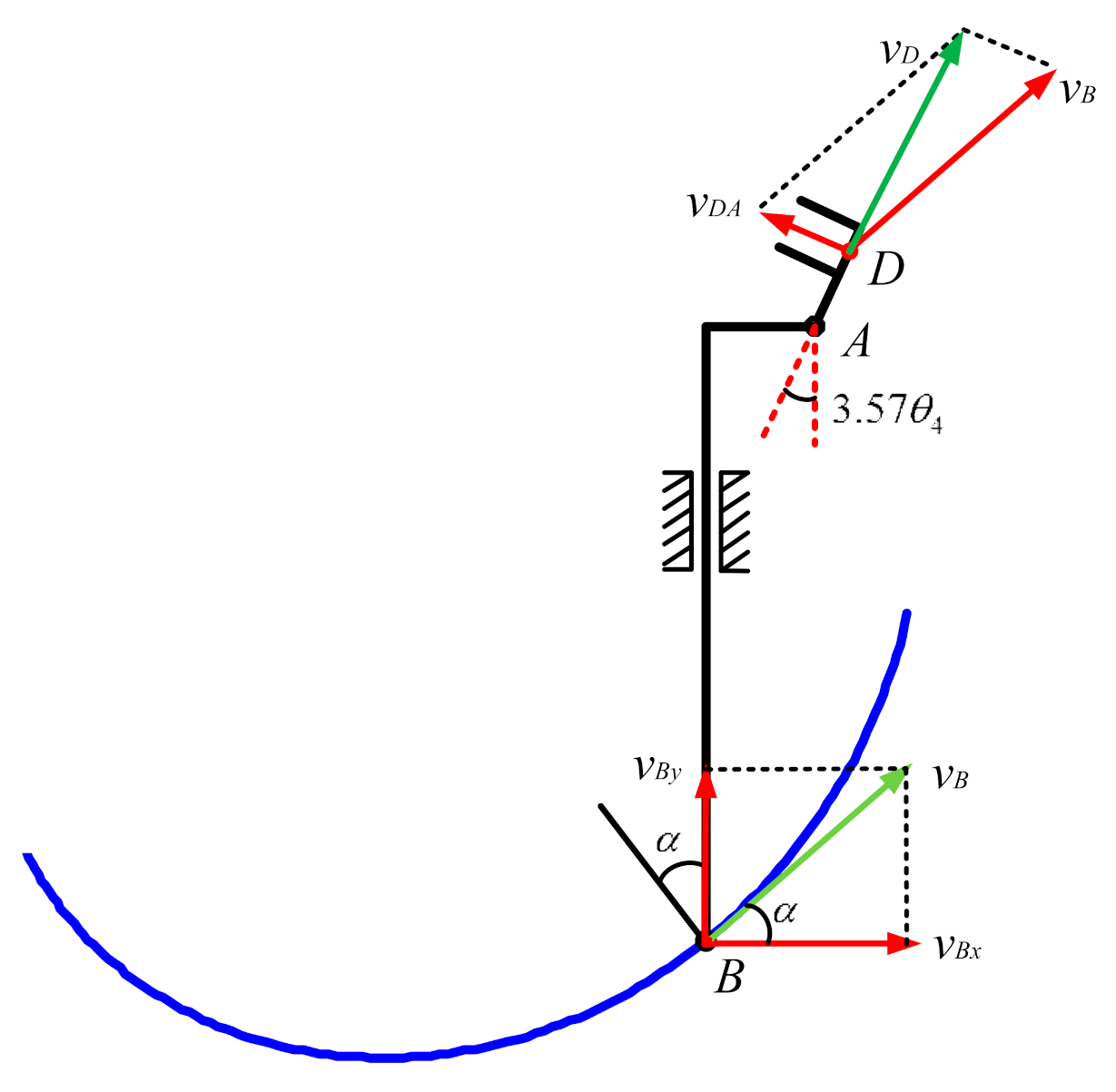
2.3. Kinematic Performance Analysis for the EFRR
2.4. Illustration of Mechnical Structure for The EFRR
3. Control Strategy of the EFRR
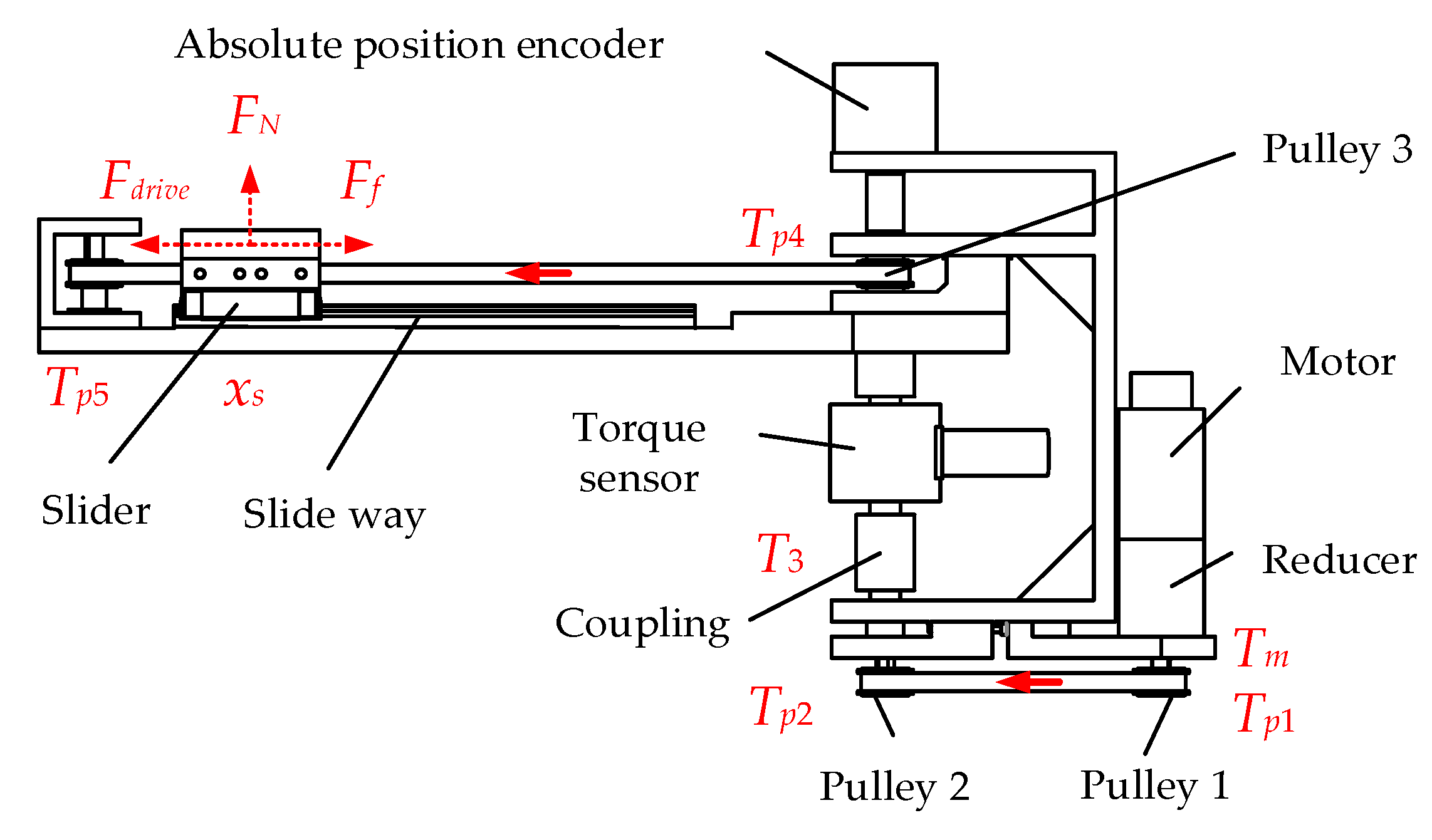
3.1. Dynamic Model Solution of Mechanical Part
3.2. Fuzzy PD Control Algorithm
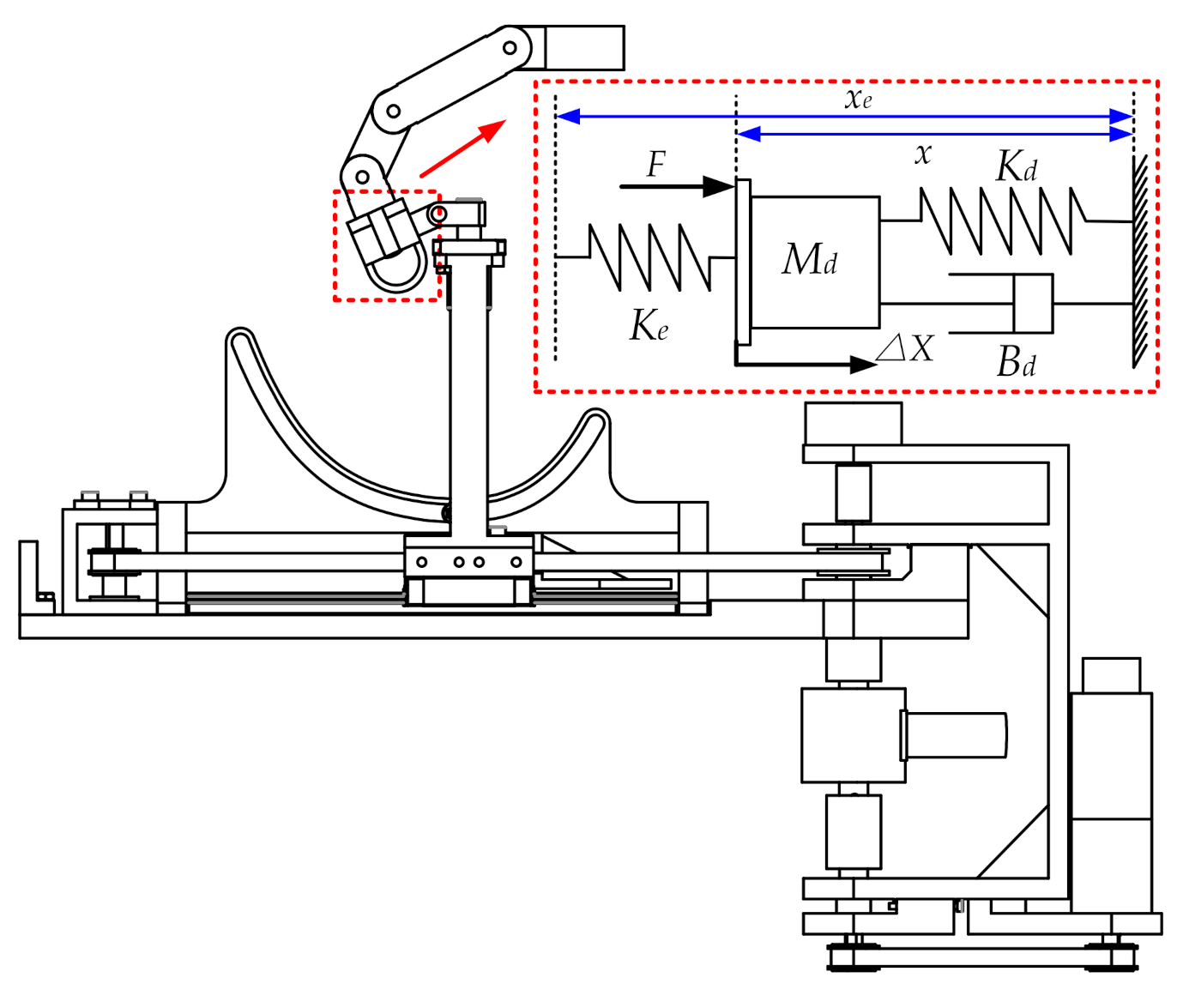
3.3. Adaptive Impedance Control Strategy
3.4. Safety Protection Model
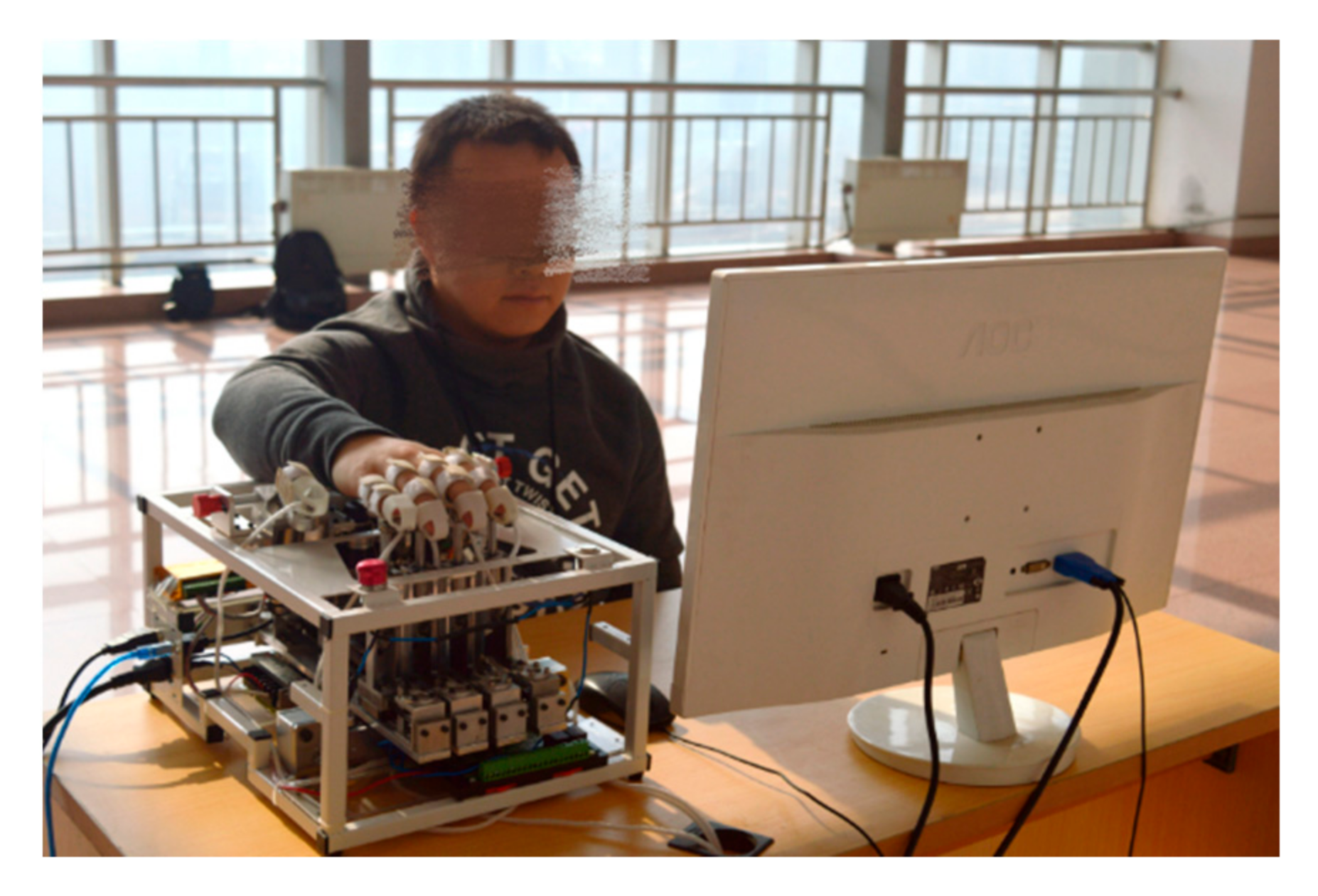
4. Preliminary Experimental Trial of the EFRR
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Mensah, G.A.; Norrving, B.; Murray, C.J.; Roth, G.A. Atlas of the Global Burden of Stroke (1990–2013): The GBD 2013 Study. Neuroepidemiology 2015, 45, 230–236. [Google Scholar] [CrossRef]
- Feigin, V.L.; Nguyen, G.; Cercy, K.; Johnson, C.O.; Alam, T.; Parmar, P.G.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abejie, A.N.; et al. Global, Regional, and Country-Specific Lifetime Risks of Stroke, 1990 and 2016. N. Engl. J. Med. 2018, 379, 2429–2437. [Google Scholar] [CrossRef] [PubMed]
- World Health Statistics 2020: Monitoring Health for the SDGs, Sustainable Development Goals. Available online: https://www.who.int/data/gho/publications/world-health-statistics (accessed on 26 April 2021).
- Hou, Z.; Zhao, X.; Cheng, L.; Wang, Q.; Wang, W. Recent Advances in Rehabilitation Robots and Intelligent Assistance Systems. ACTA Autom. Sin. 2016, 42, 1765–1779. [Google Scholar] [CrossRef]
- Krebs, H.I. Rehabilitation robotics: An academic engineer perspective. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 6709–6712. [Google Scholar]
- Suarez-Escobar, M.; Rendon-Velez, E. An overview of robotic/mechanical devices for post-stroke thumb rehabilitation. Disabil. Rehabil. Assist. Technol. 2018, 13, 683–703. [Google Scholar] [CrossRef] [PubMed]
- Aggogeri, F.; Mikolajczyk, T.; O’Kane, J. Robotics for rehabilitation of hand movement in stroke survivors. Adv. Mech. Eng. 2019, 11. [Google Scholar] [CrossRef]
- Hwang, C.H.; Seong, J.W.; Son, D.S. Individual finger synchronized robot-assisted hand rehabilitation in subacute to chronic stroke: A prospective randomized clinical trial of efficacy. Clin. Rehabil. 2012, 26, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Pinter, D.; Pegritz, S.; Pargfrieder, C.; Reiter, G.; Wurm, W.; Gattringer, T.; Linderl-Madrutter, R.; Neuper, C.; Fazekas, F.; Grieshofer, P.; et al. Exploratory study on the effects of a robotic hand rehabilitation device on changes in grip strength and brain activity after stroke. Top. Stroke Rehabil. 2013, 20, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Dovat, L.; Lambercy, O.; Gassert, R.; Maeder, T.; Milner, T.; Leong, T.C.; Burdet, E. HandCARE: A cable-actuated rehabilitation system to train hand function after stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2008, 16, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Bouzit, M.; Burdea, G.; Popescu, G.; Boian, R. The Rutgers Master II-new design force-feedback glove. IEEE/ASME Trans. Mechatron. 2002, 7, 256–263. [Google Scholar] [CrossRef] [Green Version]
- Hesse, S.; Kuhlmann, H.; Wilk, J.; Tomelleri, C.; Kirker, S.G. A new electromechanical trainer for sensorimotor rehabilitation of paralysed fingers: A case series in chronic and acute stroke patients. J. Neuroeng. Rehabil. 2008, 5, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Tzvi, P.; Ma, Z. Sensing and Force-Feedback Exoskeleton (SAFE) Robotic Glove. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 992–1002. [Google Scholar] [CrossRef]
- Zhang, N.; Niu, B.; Wang, H.; Chen, F.; Yan, H.; Jin, Z. Design of active disturbance rejection controller finger rehabilitation robot structure and control system. Sci. Tech. Engrg. 2019, 19, 166–173. [Google Scholar] [CrossRef]
- Zheng, Y.; Chen, L.; Wang, G.; Liu, X.; Dong, X.; Wang, J. A Structure Optimal Design of Training Devices for the Under-Actuated Hand Rehabilitation. J. Xian Jiaotong Univ. 2015, 49, 151–156. [Google Scholar] [CrossRef]
- Ito, S.; Kawasaki, H.; Ishigure, Y.; Natsume, M.; Mouri, T.; Nishimoto, Y. A design of fine motion assist equipment for disabled hand in robotic rehabilitation system. J. Frankl. Inst. 2011, 348, 79–89. [Google Scholar] [CrossRef]
- Agarwal, P.; Deshpande, A.D. Series Elastic Actuators for Small-Scale Robotic Applications. J. Mech. Robot. 2017, 9. [Google Scholar] [CrossRef]
- Agarwal, P.; Fox, J.; Yun, Y.; O’Malley, M.K.; Deshpande, A.D. An index finger exoskeleton with series elastic actuation for rehabilitation: Design, control and performance characterization. Int. J. Robot. Res. 2015, 34, 1747–1772. [Google Scholar] [CrossRef]
- Sandoval-Gonzalez, O.; Jacinto-Villegas, J.; Herrera-Aguilar, I.; Portillo-Rodiguez, O.; Tripicchio, P.; Hernandez-Ramos, M.; Flores-Cuautle, A.; Avizzano, C. Design and Development of a Hand Exoskeleton Robot for Active and Passive Rehabilitation. Int. J. Adv. Robot. Syst. 2017, 13. [Google Scholar] [CrossRef] [Green Version]
- Cempini, M.; Cortese, M.; Vitiello, N. A Powered Finger–Thumb Wearable Hand Exoskeleton With Self-Aligning Joint Axes. IEEE/ASME Trans. Mechatron. 2015, 20, 705–716. [Google Scholar] [CrossRef]
- Choi, W.-H.; Takeda, Y. Geometric Design and Prototyping of a (2-RRU)-URR Parallel Mechanism for Thumb Rehabilitation Therapy. Machines 2021, 9, 50. [Google Scholar] [CrossRef]
- Cappello, L.; Meyer, J.T.; Galloway, K.C.; Peisner, J.D.; Granberry, R.; Wagner, D.A.; Engelhardt, S.; Paganoni, S.; Walsh, C.J. Assisting hand function after spinal cord injury with a fabric-based soft robotic glove. J. Neuroeng. Rehabil. 2018, 15, 59. [Google Scholar] [CrossRef]
- Yap, H.K.; Jeong Hoon, L.; Nasrallah, F.; Goh, J.C.H.; Yeow, R.C.H. A soft exoskeleton for hand assistive and rehabilitation application using pneumatic actuators with variable stiffness. In Proceedings of the 2015 IEEE International Conference on Robotics and Automation (ICRA), Seattle, DC, USA, 26–30 May 2015; pp. 4967–4972. [Google Scholar]
- Jeong, U.; In, H.-K.; Cho, K.-J. Implementation of various control algorithms for hand rehabilitation exercise using wearable robotic hand. Intell. Serv. Robot. 2013, 6, 181–189. [Google Scholar] [CrossRef]
- Butzer, T.; Lambercy, O.; Arata, J.; Gassert, R. Fully Wearable Actuated Soft Exoskeleton for Grasping Assistance in Everyday Activities. Soft Robot. 2021, 8, 128–143. [Google Scholar] [CrossRef] [PubMed]
- Nycz, C.J.; Butzer, T.; Lambercy, O.; Arata, J.; Fischer, G.S.; Gassert, R. Design and Characterization of a Lightweight and Fully Portable Remote Actuation System for Use With a Hand Exoskeleton. IEEE Robot. Autom. Lett. 2016, 1, 976–983. [Google Scholar] [CrossRef]
- Arata, J.; Ohmoto, K.; Gassert, R.; Lambercy, O.; Fujimoto, H.; Wada, I. A new hand exoskeleton device for rehabilitation using a three-layered sliding spring mechanism. In Proceedings of the 2013 IEEE International Conference on Robotics and Automation, Karlsruhe, Germany, 6–10 May 2013; pp. 3902–3907. [Google Scholar]
- Felix Orlando, M.; Behera, L.; Dutta, A.; Saxena, A. Optimal Design and Redundancy Resolution of a Novel Robotic Two-Fingered Exoskeleton. IEEE Trans. Med. Robot. Bionics 2020, 2, 59–75. [Google Scholar] [CrossRef]
- Cheng, L.; Chen, M.; Li, Z. Design and Control of a Wearable Hand Rehabilitation Robot. IEEE Access 2018, 6, 74039–74050. [Google Scholar] [CrossRef]
- Park, Y.; Jo, I.; Bae, J. Development of a dual-cable hand exoskeleton system for virtual reality. In Proceedings of the 2016 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Daejeon, Korea, 9–14 October 2016; pp. 1019–1024. [Google Scholar]
- Chiri, A.; Vitiello, N.; Giovacchini, F.; Roccella, S.; Vecchi, F.; Carrozza, M.C. Mechatronic Design and Characterization of the Index Finger Module of a Hand Exoskeleton for Post-Stroke Rehabilitation. IEEE/ASME Trans. Mechatron. 2012, 17, 884–894. [Google Scholar] [CrossRef]
- Wu, J.; Huang, J.; Wang, Y.; Xing, K. A Wearable Rehabilitation Robotic Hand Driven by PM-TS Actuators. In Proceedings of the Intelligent Robotics and Applications, Berlin/Heidelberg, Germany, 10–12 November 2010; pp. 440–450. [Google Scholar]
- Jones, C.L.; Wang, F.; Morrison, R.; Sarkar, N.; Kamper, D.G. Design and Development of the Cable Actuated Finger Exoskeleton for Hand Rehabilitation Following Stroke. IEEE ASME Trans. Mechatron. 2014, 19, 131–140. [Google Scholar] [CrossRef]
- Polygerinos, P.; Wang, Z.; Galloway, K.C.; Wood, R.J.; Walsh, C.J. Soft robotic glove for combined assistance and at-home rehabilitation. Robot. Auton. Syst. 2015, 73, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Bertelli, J.; Tavares, K. Little finger abduction and adduction testing in ulnar nerve lesions. Hand Surg. Rehabil. 2018, 37, 368–371. [Google Scholar] [CrossRef] [PubMed]
- Calais-Germain, B. Anatomy of Movement; Eastland Press: Seattle, DC, USA, 2015. [Google Scholar]
- Jianfeng, L.; Zhaojing, Z.; Leiyu, Z.; Chunjing, T.; Run, J.; Jinhong, F. Review of the Kinematic Compatibility Design of Hand Exoskelentons. J. Shanghai Jiao Tong Univ. 2018, 52, 729–742. [Google Scholar] [CrossRef]
- Lu, X.; Yang, Z.; Chen, Y.; Wang, J. Structure Design of a Wearable Device for Hand Rehabilitation. In Proceedings of the 2016 9th International Symposium on Computational Intelligence and Design (ISCID), Hangzhou, China, 10–11 December 2016; pp. 93–96. [Google Scholar]
- Hsu, T.-H.; Chiang, Y.-C.; Chan, W.-T.; Chen, S.-J. A Finger Exoskeleton Robot for Finger Movement Rehabilitation. Inventions 2017, 2, 12. [Google Scholar]
- Hernández-Santos, C.; Davizón, Y.A.; Said, A.R.; Soto, R.; Félix-Herrán, L.C.; Vargas-Martínez, A. Development of a Wearable Finger Exoskeleton for Rehabilitation. Appl. Sci. 2021, 11, 4145. [Google Scholar] [CrossRef]
- Secciani, N.; Bianchi, M.; Ridolfi, A.; Vannetti, F.; Volpe, Y.; Governi, L.; Bianchini, M.; Allotta, B. Tailor-Made Hand Exoskeletons at the University of Florence: From Kinematics to Mechatronic Design. Machines 2019, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Choukou, M.-A.; Mbabaali, S.; Bani Hani, J.; Cooke, C. Haptic-Enabled Hand Rehabilitation in Stroke Patients: A Scoping Review. Appl. Sci. 2021, 11, 3712. [Google Scholar] [CrossRef]
- Shahid, T.; Gouwanda, D.; Nurzaman, S.G.; Gopalai, A.A. Moving toward Soft Robotics: A Decade Review of the Design of Hand Exoskeletons. Biomimetics 2018, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Tarvainen, T.V.J.; Fernandez-Vargas, J.; Yu, W. New Layouts of Fiber Reinforcements to Enable Full Finger Motion Assist with Pneumatic Multi-Chamber Elastomer Actuators. Actuators 2018, 7, 31. [Google Scholar] [CrossRef] [Green Version]
- Tarvainen, T.V.J.; Yu, W. Pneumatic Multi-Pocket Elastomer Actuators for Metacarpophalangeal Joint Flexion and Abduction-Adduction. Actuators 2017, 6, 27. [Google Scholar] [CrossRef] [Green Version]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Joints | DoF | Movement | Range (°) | Torque (N·m) | |
|---|---|---|---|---|---|
| Fingers | MCP | 2 | A/A | 0~45 | 0.16 |
| F/E | 0~70 | 0.29 | |||
| PIP | 1 | F/E | 0~110 | 0.29 | |
| DIP | 1 | F/E | 0~70 | \ | |
| Thumb | CM | 2 | A/A | 0~60 | 0.3 |
| F/E | 0~90 | 0.3 | |||
| MP | 1 | F/E | 0~60 | 0.26 | |
| IP | 1 | F/E | 0~70 | 0.26 |
| Symbols | Implication | Value (mm) |
|---|---|---|
| lCD | Length of the finger sleeve | 10 |
| lAD | Length of the finger sleeve nod | 15 |
| lAE | Length of horizontal linkage | 11 |
| lEB | Length of vertical connecting rod | 123 |
| Number | Symbols | Implication | Unit |
|---|---|---|---|
| 1 | Kt | Torque constant of the motor | \ |
| 2 | ia | Current of the motor | A |
| 3 | Tpi | Torque of the pulley i | N·m |
| 4 | T3 | Torque of the sensor | N·m |
| 5 | Js | Rotational inertia of the motor and reducer | kg·m2 |
| 6 | Jpi | Rotational inertia of the pulley i | kg·m2 |
| 7 | J3 | Rotational inertia of the torque sensor | kg·m2 |
| 8 | mt | Mass of the slider and the object on it | kg |
| 9 | d | Radius of the pulleys | m |
| 10 | Bs | Motor damping factor (converted to reducer) | \ |
| 11 | µv | Coefficient of viscous friction of slide way | \ |
| 12 | µc | Coulomb friction coefficient of slide way | \ |
| e/de | NB | NM | NS | ZO | PS | PM | PB |
|---|---|---|---|---|---|---|---|
| NB | PB | PB | PM | PM | PS | ZO | ZO |
| NM | PB | PB | PM | PS | PS | ZO | NS |
| NS | PM | PM | PM | PS | ZO | NS | NS |
| ZO | PM | PS | PS | ZO | NS | NM | NM |
| PS | PS | ZO | ZO | NS | NS | NM | NM |
| PM | PS | NS | NS | NM | NM | NM | NB |
| PB | ZO | NM | NM | NM | NM | NB | NB |
| e/de | NB | NM | NS | ZO | PS | PM | PB |
|---|---|---|---|---|---|---|---|
| NB | PS | NS | NB | NB | NB | NM | PS |
| NM | PS | NS | NB | NM | NM | NS | ZO |
| NS | ZO | NS | NM | NM | NS | NS | ZO |
| ZO | ZO | NS | NS | NS | NS | NS | ZO |
| PS | ZO | ZO | ZO | ZO | PB | ZO | ZO |
| PM | PB | PS | PS | PS | PS | PB | PB |
| PB | PB | PM | PM | PS | PS | PB | PB |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, Y.; Wang, H.; Niu, B.; Zhang, Y.; Du, J.; Niu, J.; Sun, L. Mechanical Design and Analysis of the End-Effector Finger Rehabilitation Robot (EFRR) for Stroke Patients. Machines 2021, 9, 110. https://doi.org/10.3390/machines9060110
Tian Y, Wang H, Niu B, Zhang Y, Du J, Niu J, Sun L. Mechanical Design and Analysis of the End-Effector Finger Rehabilitation Robot (EFRR) for Stroke Patients. Machines. 2021; 9(6):110. https://doi.org/10.3390/machines9060110
Chicago/Turabian StyleTian, Yu, Hongbo Wang, Baoshan Niu, Yongshun Zhang, Jiazheng Du, Jianye Niu, and Li Sun. 2021. "Mechanical Design and Analysis of the End-Effector Finger Rehabilitation Robot (EFRR) for Stroke Patients" Machines 9, no. 6: 110. https://doi.org/10.3390/machines9060110