
Design and Preliminary Evaluation of a Soft Finger Exoskeleton Controlled by Isometric Grip Force


Abstract
:1. Introduction
2. Materials and Methods
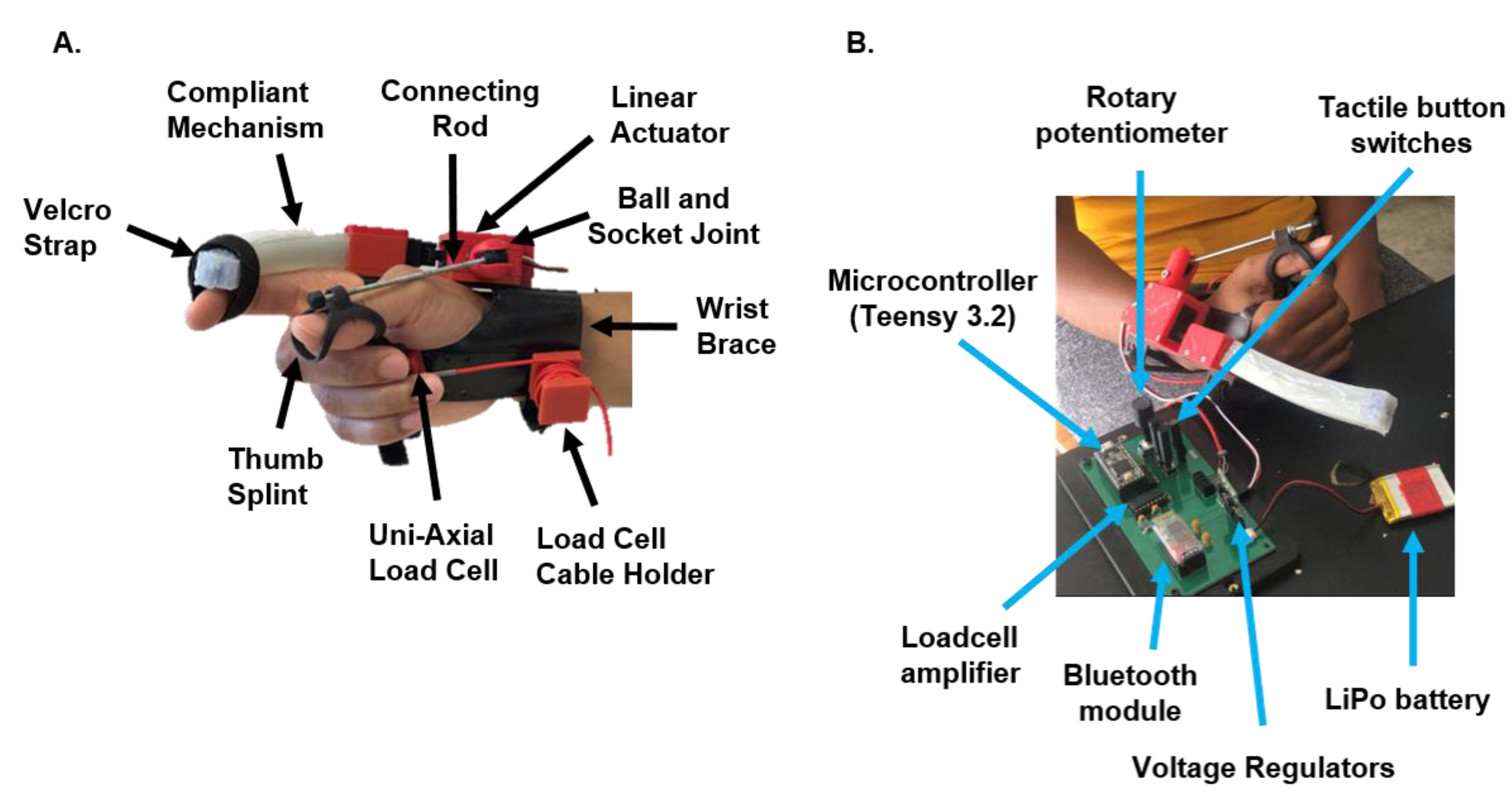
2.1. System Overview
2.2. Fabrication and Working Principle of Compliant Mechanism
2.3. Residual Isometric Grip Force Control Strategy
2.4. Compliant Mechanism Characterization and Preliminary Evaluation of IGripX Hand Exoskeleton Force Control
2.4.1. Measurement of Compliant Mechanism Impedance and Output Force
2.4.2. Participants
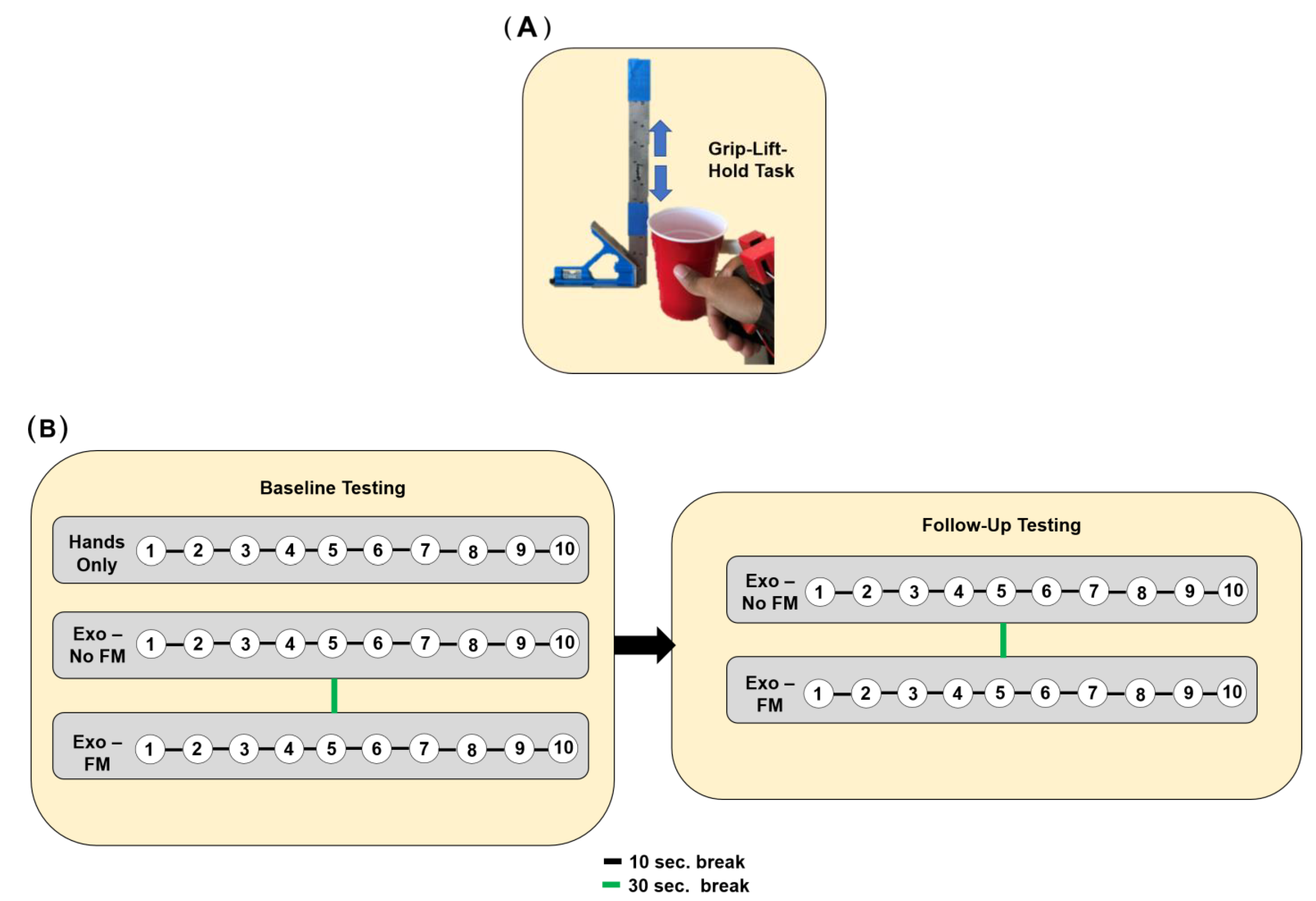
2.4.3. Experimental Protocol—Grip–Lift–Hold Task
2.4.4. Experimental Protocol—User Preference
3. Results
3.1. The Compliant Mechanism Exhibited Low Impedance and Could Exert a Moderate Amount of Force
3.2. Individuals Are Able to Rapidly Improve Task Performance When Using Isometric Force Control Strategy
3.3. Individuals Prefer a Voluntary Opening Strategy as Opposed to Voluntary Close While Preferences on Force Sensitivity Are Task Dependent
4. Discussion
4.1. A Novel Compliant Mechanism with Low Impedance and Moderate Force Production Capabilities
4.2. Feasibility of Isometric Force Control to Enable Robust Control of Finger Exoskeleton
4.3. Optimal Parameters for Improving Usability of Isometric Force Control Strategy
5. Limitations
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Barry, A.J.; Kamper, D.G.; Stoykov, M.E.; Triandafilou, K.; Roth, E. Characteristics of the severely impaired hand in survivors of stroke with chronic impairments. Top. Stroke Rehabil. 2022, 29, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, G.; Conrad, M.O.; Qiu, D.; Kamper, D.G. Contributions of voluntary activation deficits to hand weakness after stroke. Top. Stroke Rehabil. 2016, 23, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Triandafilou, K.; Lock, B.A.; Kamper, D.G. Impairment in Task-Specific Modulation of Muscle Coordination Correlates with the Severity of Hand Impairment following Stroke. PLoS ONE 2013, 8, e68745. [Google Scholar] [CrossRef]
- Triandafilou, K.M.; Kamper, D.G. Investigation of hand muscle atrophy in stroke survivors. Clin. Biomech. 2012, 27, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, P. The nature of hand motor impairment after stroke and its treatment. Curr. Treat. Options Cardiovasc. Med. 2007, 9, 221–228. [Google Scholar] [CrossRef]
- Gassert, R.; Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. NeuroEng. Rehabil. 2018, 15, 46. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, P. Upper Limb Motor Impairment after Stroke. Phys. Med. Rehabil. Clin. 2015, 26, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H. The role of the corticospinal tract in motor recovery in patients with a stroke: A review. NeuroRehabilitation 2009, 24, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Maraka, S.; Jiang, Q.; Jafari-Khouzani, K.; Li, L.; Malik, S.; Hamidian, H.; Zhang, T.; Lu, M.; Soltanian-Zadeh, H.; Chopp, M.; et al. Degree of corticospinal tract damage correlates with motor function after stroke. Ann. Clin. Transl. Neurol. 2014, 1, 891–899. [Google Scholar] [CrossRef]
- Lin, D.J.; Cloutier, A.M.; Erler, K.S.; Cassidy, J.M.; Snider, S.B.; Ranford, J.; Parlman, K.; Giatsidis, F.; Burke, J.F.; Schwamm, L.H.; et al. Corticospinal Tract Injury Estimated From Acute Stroke Imaging Predicts Upper Extremity Motor Recovery after Stroke. Stroke 2019, 50, 3569–3577. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Lang, C.E.; Zeiler, S.; Byblow, W.D. Advances and challenges in stroke rehabilitation. Lancet Neurol. 2020, 19, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Reinkensmeyer, D.J.; Dietz, V. (Eds.) Neurorehabilitation Technology; Springer International Publishing: Cham, Switzerland, 2016; ISBN 978-3-319-28601-3. [Google Scholar] [CrossRef]
- Allred, R.P.; Kim, S.Y.; Jones, T.A. Use it and/or lose it—Experience effects on brain remodeling across time after stroke. Front. Hum. Neurosci. 2014, 8. [Google Scholar] [CrossRef] [PubMed]
- Bakhti, K.; Mottet, D.; Schweighofer, N.; Froger, J.; Laffont, I. Quantification of learned non-use of the upper limb after a stroke. Ann. Phys. Rehabil. Med. 2015, 58, e4. [Google Scholar] [CrossRef]
- Molle Da Costa, R.D.; Luvizutto, G.J.; Martins, L.G.; Thomaz De Souza, J.; Regina Da Silva, T.; Alvarez Sartor, L.C.; Winckler, F.C.; Modolo, G.P.; Molle, E.R.D.S.D.; Dos Anjos, S.M.; et al. Clinical factors associated with the development of nonuse learned after stroke: A prospective study. Top. Stroke Rehabil. 2019, 26, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Lieber, J.; Dittli, J.; Lambercy, O.; Gassert, R.; Meyer-Heim, A.; van Hedel, H.J.A. Clinical utility of a pediatric hand exoskeleton: Identifying users, practicability, and acceptance, and recommendations for design improvement. J. NeuroEng. Rehabil. 2022, 19, 17. [Google Scholar] [CrossRef] [PubMed]
- Bützer, T.; Lambercy, O.; Arata, J.; Gassert, R. Fully Wearable Actuated Soft Exoskeleton for Grasping Assistance in Everyday Activities. Soft Robot. 2021, 8, 128–143. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; He, B.; Liang, Z.; Zhao, C.-G.; Chen, J.; Zhuo, Y.; Xu, G.; Xie, J.; Althoefer, K. An Attention-Controlled Hand Exoskeleton for the Rehabilitation of Finger Extension and Flexion Using a Rigid-Soft Combined Mechanism. Front. Neurorobotics 2019, 13, 34. [Google Scholar] [CrossRef] [PubMed]
- Polygerinos, P.; Wang, Z.; Galloway, K.C.; Wood, R.J.; Walsh, C.J. Soft robotic glove for combined assistance and at-home rehabilitation. Robot. Auton. Syst. 2015, 73, 135–143. [Google Scholar] [CrossRef]
- Kang, B.B.; Choi, H.; Lee, H.; Cho, K.-J. Exo-Glove Poly II: A Polymer-Based Soft Wearable Robot for the Hand with a Tendon-Driven Actuation System. Soft Robot. 2019, 6, 214–227. [Google Scholar] [CrossRef] [PubMed]
- Xiloyannis, M.; Cappello, L.; Khanh, D.B.; Yen, S.-C.; Masia, L. Modelling and design of a synergy-based actuator for a tendon-driven soft robotic glove. In Proceedings of the 2016 6th IEEE International Conference on Biomedical Robotics and Biomechatronics (BioRob), Singapore, 26–29 June 2016; pp. 1213–1219. [Google Scholar] [CrossRef]
- Gasser, B.W.; Bennett, D.A.; Durrough, C.M.; Goldfarb, M. Design and preliminary assessment of Vanderbilt hand exoskeleton. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 1537–1542. [Google Scholar] [CrossRef]
- Rose, C.G.; O’Malley, M.K. Hybrid Rigid-Soft Hand Exoskeleton to Assist Functional Dexterity. IEEE Robot. Autom. Lett. 2019, 4, 73–80. [Google Scholar] [CrossRef]
- Sanders, Q.; Okita, S.; Lobo-Prat, J.; Schwerz de Lucena, D.; Smith, B.; Reinkensmeyer, D. Design and Control of a Novel Grip Amplifier to Support Pinch Grip with a Minimal Soft Hand Exoskeleton. In Proceedings of the 2018 7th IEEE International Conference on Biomedical Robotics and Biomechatronics (Biorob), Enschede, The Netherlands, 26–29 August 2018; p. 1094. [Google Scholar] [CrossRef]
- Xiloyannis, M.; Cappello, L.; Binh, K.D.; Antuvan, C.W.; Masia, L. Preliminary design and control of a soft exosuit for assisting elbow movements and hand grasping in activities of daily living. J. Rehabil. Assist. Technol. Eng. 2017, 4. Available online: https://journals.sagepub.com/doi/full/10.1177/2055668316680315 (accessed on 29 February 2024). [CrossRef] [PubMed]
- Ho, N.S.K.; Tong, K.Y.; Hu, X.L.; Fung, K.L.; Wei, X.J.; Rong, W.; Susanto, E.A. An EMG-driven exoskeleton hand robotic training device on chronic stroke subjects: Task training system for stroke rehabilitation. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–5. [Google Scholar] [CrossRef]
- Leonardis, D.; Chisari, C.; Bergamasco, M.; Frisoli, A.; Barsotti, M.; Loconsole, C.; Solazzi, M.; Troncossi, M.; Mazzotti, C.; Castelli, V.P.; et al. An EMG-Controlled Robotic Hand Exoskeleton for Bilateral Rehabilitation. IEEE Trans. Haptics 2015, 8, 140–151. [Google Scholar] [CrossRef]
- Sierotowicz, M.; Lotti, N.; Nell, L.; Missiroli, F.; Alicea, R.; Zhang, X.; Xiloyannis, M.; Rupp, R.; Papp, E.; Krzywinski, J.; et al. EMG-Driven Machine Learning Control of a Soft Glove for Grasping Assistance and Rehabilitation. IEEE Robot. Autom. Lett. 2022, 7, 1566–1573. [Google Scholar] [CrossRef]
- Ghassemi, M.; Kamper, D.G. A Hand Exoskeleton for Stroke Survivors’ Activities of Daily Life. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 6734–6737. [Google Scholar] [CrossRef]
- Bos, R.A.; Haarman, C.J.W.; Stortelder, T.; Nizamis, K.; Herder, J.L.; Stienen, A.H.A.; Plettenburg, D.H. A structured overview of trends and technologies used in dynamic hand orthoses. J. NeuroEng. Rehabil. 2016, 13, 62. [Google Scholar] [CrossRef] [PubMed]
- Gantenbein, J.; Dittli, J.; Meyer, J.T.; Gassert, R.; Lambercy, O. Intention Detection Strategies for Robotic Upper-Limb Orthoses: A Scoping Review Considering Usability, Daily Life Application, and User Evaluation. Front. Neurorobotics 2022, 16, 815693. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.; Jeong, S.; Herrin, K.R.; Desai, J.P. Review: Hand Exoskeleton Systems, Clinical Rehabilitation Practices, and Future Prospects. IEEE Trans. Med. Robot. Bionics 2021, 3, 606–622. [Google Scholar] [CrossRef]
- Xiloyannis, M.; Alicea, R.; Georgarakis, A.-M.; Haufe, F.L.; Wolf, P.; Masia, L.; Riener, R. Soft Robotic Suits: State of the Art, Core Technologies, and Open Challenges. IEEE Trans. Robot. 2022, 38, 1343–1362. [Google Scholar] [CrossRef]
- Singh, R.M.; Chatterji, S. Trends and Challenges in EMG Based Control Scheme of Exoskeleton Robots—A Review. Int. J. Sci. Eng. Res. 2012, 3, 933–940. [Google Scholar]
- Zhang, J.; Sheng, J.; O’Neill, C.T.; Walsh, C.J.; Wood, R.J.; Ryu, J.-H.; Desai, J.P.; Yip, M.C. Robotic Artificial Muscles: Current Progress and Future Perspectives. IEEE Trans. Robot. 2019, 35, 761–781. [Google Scholar] [CrossRef]
- Heo, P.; Gu, G.M.; Lee, S.; Rhee, K.; Kim, J. Current hand exoskeleton technologies for rehabilitation and assistive engineering. Int. J. Precis. Eng. Manuf. 2012, 13, 807–824. [Google Scholar] [CrossRef]
- Yap, H.K.; Lim, J.H.; Nasrallah, F.; Goh, J.C.H.; Yeow, R.C.H. A soft exoskeleton for hand assistive and rehabilitation application using pneumatic actuators with variable stiffness. In Proceedings of the 2015 IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015; pp. 4967–4972. [Google Scholar] [CrossRef]
- Cappello, L.; Meyer, J.T.; Galloway, K.C.; Peisner, J.D.; Granberry, R.; Wagner, D.A.; Engelhardt, S.; Paganoni, S.; Walsh, C.J. Assisting hand function after spinal cord injury with a fabric-based soft robotic glove. J. NeuroEng. Rehabil. 2018, 15, 59. [Google Scholar] [CrossRef]
- Cempini, M.; Cortese, M.; Vitiello, N. A Powered Finger–Thumb Wearable Hand Exoskeleton with Self-Aligning Joint Axes. IEEEASME Trans. Mechatron. 2015, 20, 705–716. [Google Scholar] [CrossRef]
- Sarac, M.; Solazzi, M.; Sotgiu, E.; Bergamasco, M.; Frisoli, A. Design and kinematic optimization of a novel underactuated robotic hand exoskeleton. Meccanica 2017, 52, 749–761. [Google Scholar] [CrossRef]
- Randazzo, L.; Iturrate, I.; Perdikis, S.; Millan, J.d.R. Mano: A Wearable Hand Exoskeleton for Activities of Daily Living and Neurorehabilitation. IEEE Robot. Autom. Lett. 2018, 3, 500–507. [Google Scholar] [CrossRef]
- Yang, S.-H.; Koh, C.-L.; Hsu, C.-H.; Chen, P.-C.; Chen, J.-W.; Lan, Y.-H.; Yang, Y.; Lin, Y.-D.; Wu, C.-H.; Liu, H.-K.; et al. An Instrumented Glove-Controlled Portable Hand-Exoskeleton for Bilateral Hand Rehabilitation. Biosensors 2021, 11, 495. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Liu, Y.; Pancheri, F.; Lueth, T.C. LARG: A Lightweight Robotic Gripper with 3-D Topology Optimized Adaptive Fingers. IEEEASME Trans. Mechatron. 2022, 27, 2026–2034. [Google Scholar] [CrossRef]
- Zhang, N.; Ge, L.; Xu, H.; Zhu, X.; Gu, G. 3D printed, modularized rigid-flexible integrated soft finger actuators for anthropomorphic hands. Sens. Actuators Phys. 2020, 312, 112090. [Google Scholar] [CrossRef]
- Feix, T.; Romero, J.; Schmiedmayer, H.-B.; Dollar, A.M.; Kragic, D. The GRASP Taxonomy of Human Grasp Types. IEEE Trans. Hum.-Mach. Syst. 2016, 46, 66–77. [Google Scholar] [CrossRef]
- Conrad, M.O.; Kamper, D.G. Isokinetic strength and power deficits in the hand following stroke. Clin. Neurophysiol. 2012, 123, 1200–1206. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, P.G.; Roche, N.; Robertson, J.; Roby-Brami, A.; Bussel, B.; Maier, M.A. Affected and unaffected quantitative aspects of grip force control in hemiparetic patients after stroke. Brain Res. 2012, 1452, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Rowe, J.B.; Reinkensmeyer, D.J. Real-time slacking as a default mode of grip force control: Implications for force minimization and personal grip force variation. J. Neurophysiol. 2018, 120, 2107–2120. [Google Scholar] [CrossRef] [PubMed]
- Sensinger, J.W.; Lipsey, J.; Thomas, A.; Turner, K. Design and evaluation of voluntary opening and voluntary closing prosthetic terminal device. J. Rehabil. Res. Dev. 2015, 52, 63–76. [Google Scholar] [CrossRef] [PubMed]
- Hajian, A.Z.; Howe, R.D. Identification of the Mechanical Impedance at the Human Finger Tip. J. Biomech. Eng. 1997, 119, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Ciullo, A.S.; Catalano, M.G.; Bicchi, A.; Ajoudani, A. A Supernumerary Soft Robotic Limb for Reducing Hand-Arm Vibration Syndromes Risks. Front. Robot. AI 2021, 8, 650613. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Max Speed (no load) | 10 mm/s |
| Max Force (lifted) | 50 N |
| Stroke Length | 20 mm |
| Input Voltage | 6 V |
| Mass | 19 g |
| Operating Mode | Force Sensitivity | Time (s) |
|---|---|---|
| Voluntary Open | Low Gain | 11.5 ± 2.6 |
| High Gain | 10.4 ± 3.1 | |
| Voluntary Close | Low Gain | 10.6 ± 3.0 |
| High Gain | 9.1 ± 2.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanders, Q.; Reinkensmeyer, D.J. Design and Preliminary Evaluation of a Soft Finger Exoskeleton Controlled by Isometric Grip Force. Machines 2024, 12, 230. https://doi.org/10.3390/machines12040230
Sanders Q, Reinkensmeyer DJ. Design and Preliminary Evaluation of a Soft Finger Exoskeleton Controlled by Isometric Grip Force. Machines. 2024; 12(4):230. https://doi.org/10.3390/machines12040230
Chicago/Turabian StyleSanders, Quentin, and David J. Reinkensmeyer. 2024. "Design and Preliminary Evaluation of a Soft Finger Exoskeleton Controlled by Isometric Grip Force" Machines 12, no. 4: 230. https://doi.org/10.3390/machines12040230