1. Introduction
According to the 2019 global health estimate report [
1], stroke is the second leading cause of death in humans. As a result of stroke, most patients’ limbs have different degrees of motor dysfunction. According to the theory of plasticity in the brain, a certain number of functional reorganizations of rehabilitation, combined with effective rehabilitation control strategies, can restore limb movement function [
2,
3]. Clinical studies have shown [
4] that rehabilitation robots can effectively improve the motor function of the patient’s limb, and even restore daily life movements.
For patients with motor dysfunction, the rehabilitation process mainly repeats a movement for a long time, in order to strengthen the movement function of the damaged parts of the body. However, continuing the same movement for a long time is exhausting, and may make the patients produce negative attitudes, leading to a decrease in the level of attention, and thus a reduction in the effectiveness of rehabilitation therapy [
5]. How to promote patients’ active participation and improve their attention [
6] has become a hot topic in the field of neural rehabilitation research [
7].
One of the most critical research areas of rehabilitation robotics is the development of control strategies that can regulate physical interaction with patients to facilitate patient neuroplasticity so that patients with muscle weakness caused by nerve injury can improve or recover movement [
8]. Rehabilitation robots can provide repeatable and function orientation training, an important factor to enhance nervous system restoration. This plays a significant effect in the treatment process, but [
6] suggests that the rehabilitation robot consistently interacts with patients in a passive motor manner, with no significant improvement in the later stages of stroke patients. This suggests that improving patient motor recovery requires active patient involvement. For patients with partial movement ability, the minimum assistance controller strategy has proved to have more effective results through active assistance movement, providing patients with a minimum assistance controller. This is called an “assist-as-needed” (AAN) controller [
8,
9], and is usually operated by a force field control or impedance control based on the position error to achieve [
9]. Nonetheless, ANN’s disadvantage is that it cannot tell what position the patient is currently in, and it is easy to provide assistance when the patient does not need assistance, leading to the patient’s state of slackness.
The AAN controller is adjusted according to the limb’s ability to then adjust the intervention of the assistance, and different techniques have been used to identify the patient’s remaining ability to input this into the control strategies. In the paper [
10], before controlling the robot, muscle electromyography signals are used to estimate the subjects’ torque and then used as an input to the controller. However, because electromyography signal processing has some difficulties, electromyography signals are most effective when used to trigger specific actions. In the paper [
5,
7], electroencephalogram signals are used to identify the patient’s intent, and through the analysis of electroencephalogram signals, the human thinking mechanism can be obtained to monitor in real-time the state of the patients, which can further adjust the training strategy, so as to improve the patient’s attention and speed up the recovery. Nonetheless, the electroencephalogram is vulnerable to the interference of environmental factors. Moreover, the attendance requirement of the subjects is relatively high. At present, physical information during human-computer interaction is commonly used to estimate the subject torque, such as force sensor information [
11] and position information [
12,
13] to estimate the input of the subjects or physical information in different motion states of robot interaction with the external environment to design different stability control strategies in stages [
14]. However, the force sensor needs to select the maximum, minimum and average value of force information combined with EMG information as the mechanical signal characteristics and location information needs to be assisted by visual display, along with tracking error adjustment for patients, so the input estimation of subjects by the controller designed above cannot express the intention of subjects.
Technologies, such as machine learning, artificial neural networks, and fuzzy logic systems have been considered as feasible technologies for developing adaptive control systems. In order to solve the shortcomings of the current AAN control strategy, this paper implements the AAN control strategy based on the Gaussian Mixture Model (GMM), an AAN controller that changes the control strategy according to the degree of task completion by patients, will be proposed. By learning and calculating the interaction information between the patients and the robot, the corresponding assist strategy is designed.
GMM is a type of probability density function that requires less data to obtain good results and does not require any prior knowledge, compared with other commonly used techniques, such as a neural network [
15] providing faster regression [
16], which is widely used in data modeling. The model can parameterize a set of data points and its underlying functions into a weighted sum of the Gaussian component density, each of which has its own mean and covariance. Due to the simplicity of Gaussian functions, strong adaptability and the advantages of generative modeling, GMM has been widely used in robot demonstration learning (LFD) [
17,
18,
19].
In order to prove the effectiveness of the proposed control strategy, we carried out experiments on the developed end-effector upper limb mirror rehabilitation robot, and the relevant contributions are as follows:
- (a)
In order to restore the upper limbs of patients with motor dysfunction, we developed a new end-effector upper limb mirror rehabilitation robot. Patients can use the robot’s arm to provide rehabilitation trajectory for the patient’s impaired limb (PIL), making patients have the maximum freedom with the rehabilitation trajectory, meanwhile, the movement trajectory of the robot’s side mechanical arm can more accurately reflect the patient’s movement intention.
- (b)
The AAN control strategy based on GMM was developed. The strategy can determine the stage at which the patients need assistance depending on how much the patients complete the task each time, and give appropriate assistance in the next task. If it appears in the process that the patients in rehabilitation are not comfortable, we can at any time change the PIL trajectory using the patient’s functional limb (PFL), and prevent secondary damage to patients, to achieve the best results of rehabilitation.
- (c)
We specifically verified the proposed control strategy method to evaluate the participants’ ability to participate in the task, and used EMG signals to obtain the activation degree of the subjects’ muscles during the task, and verified the effectiveness of the AAN control strategy based on GMM for rehabilitation through the study of the subjects.
3. Experiment
3.1. The Subjects
In this paper, the study involved three healthy male subjects (mean age of 25, mean height of 175 cm) with no known neurological impairment. All procedures were carried out in accordance with the standards set out in the Declaration of Helsinki for medical research involving humans, and the study was approved by the local medical ethics committee.
3.2. Rehabilitation Robot Experimental Platform
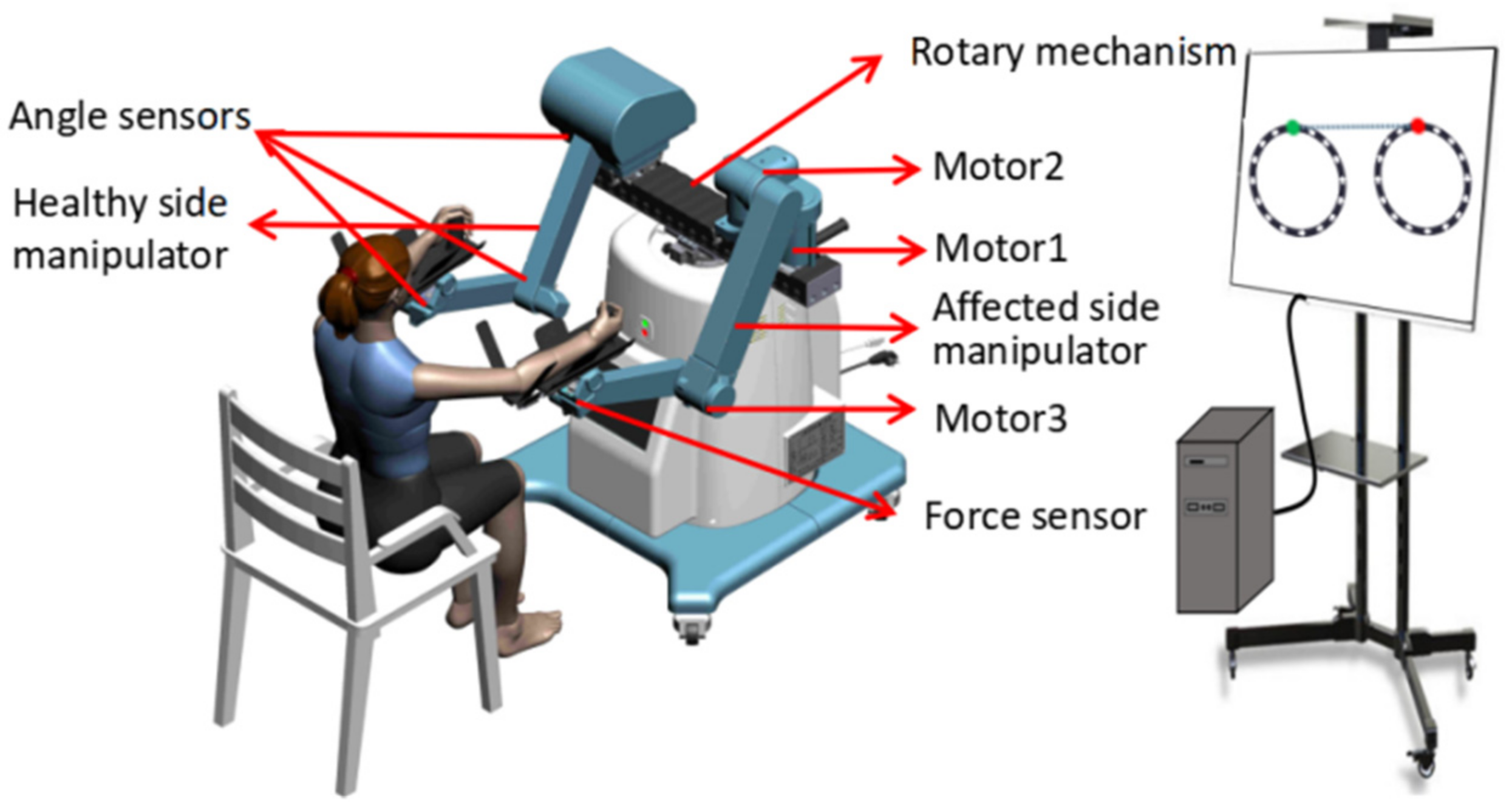
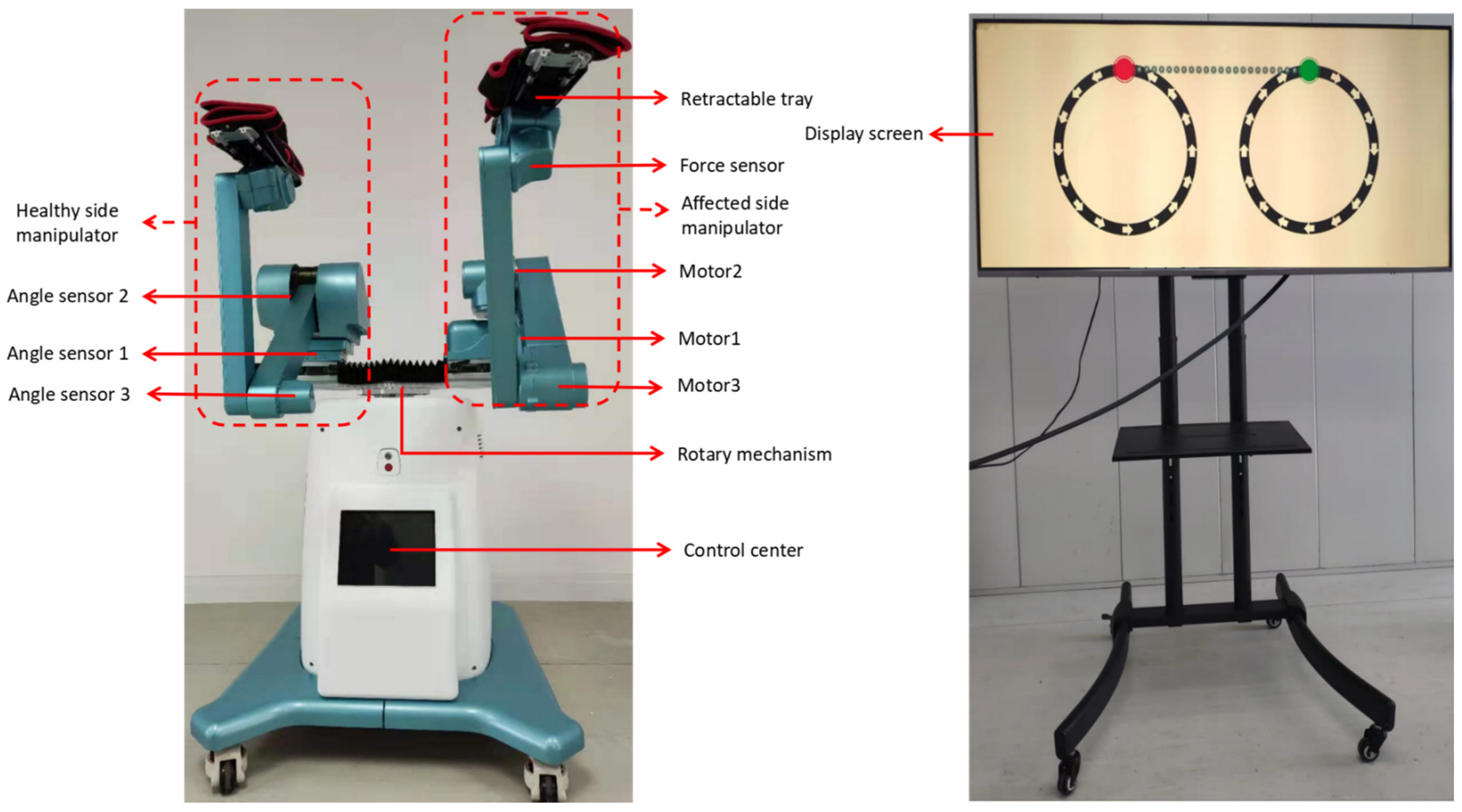
In this study, a self-designed end-effector bilateral mirror upper limb rehabilitation robot device was used. The rehabilitation robot has two mechanical arms, one is a mechanical structure, and the internal spring is helpful for the flexible movement of the mechanical arm, which interacts with the volunteer’s PFL; the other side of the robot arm contains three motors to drive the volunteer’s PIL movement, which interacts with the volunteer’s PIL to help patients achieve spatial rehabilitation tasks (
Figure 4). During the experiment, volunteers sat directly opposite the rehabilitation robot. The virtual environment used in the experiment (
Figure 5) was developed by Unity. The volunteer’s right arm mimicked the PIL and their left arm mimicked the PFL.
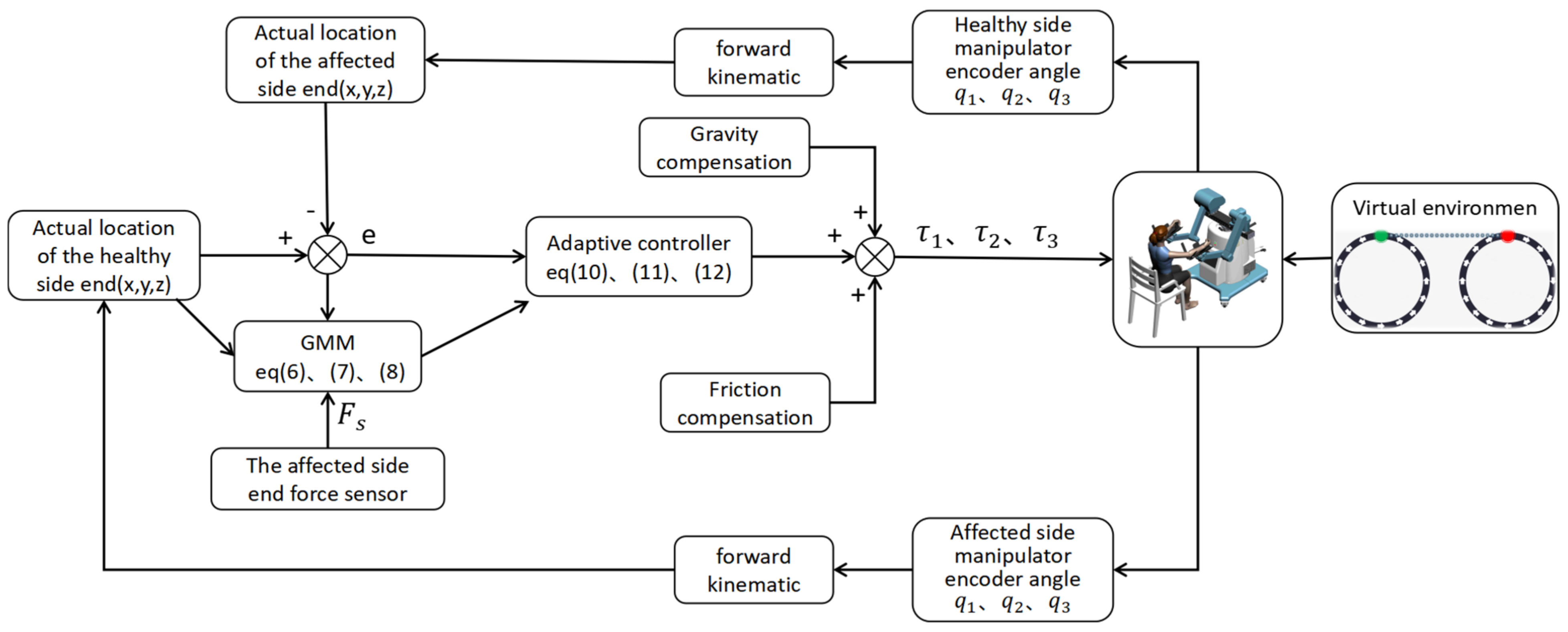
In order to verify the mechanism design and control strategy of the rehabilitation robot designed in this paper, the electrical system and human-computer interaction interface of the robot are also designed.
Figure 5 is the block diagram of the electrical system of the rehabilitation robot, which mainly includes the control center module, human-computer interaction module, data processing module, and data acquisition module.
The core function of the control center module is to run the control program, carry out TCP/IP communication with the human-computer interaction module and the data processing module, transmit the physical information needed, and carry out EtherCAT communication with the data acquisition module, accept and send operation instructions, and realize the coordinated control of the robot. The human-computer interaction module communicates with the control center, which is mainly used for doctors to set the rehabilitation parameters of patients, and displays the current position of the end of the robot on the main interface, using visual feedback to interact with patients. Through communication with the control center, the data acquisition module mainly collects signals from motor encoders, force sensors and angle sensors to identify the patient’s current position and motion intention, and read the rotation angle and angular velocity of motion. The data processing module communicates with the control center, mainly carries on the down-sampling processing to the collected physical signals, and then uses the GMM algorithm to process and transmit the necessary information to the control center.
Stretching exercises are usually part of rehabilitation exercises. For simplicity, this training task is designed to draw a circle in a two-dimensional cartesian plane with the starting coordinates of (0.4, 0, 0) m, the center coordinates of (0.5, 0, 0) m, and the radius of 0.1 m (
Figure 6). Studies have shown that slow training can improve the recovery of upper limb movement more than fast training, so the virtual mass parameter is set as M = 0 and the virtual damping coefficient is set as B = 0.
3.3. EMG Signals Are Used to Verify the Effectiveness of the GMM Algorithm
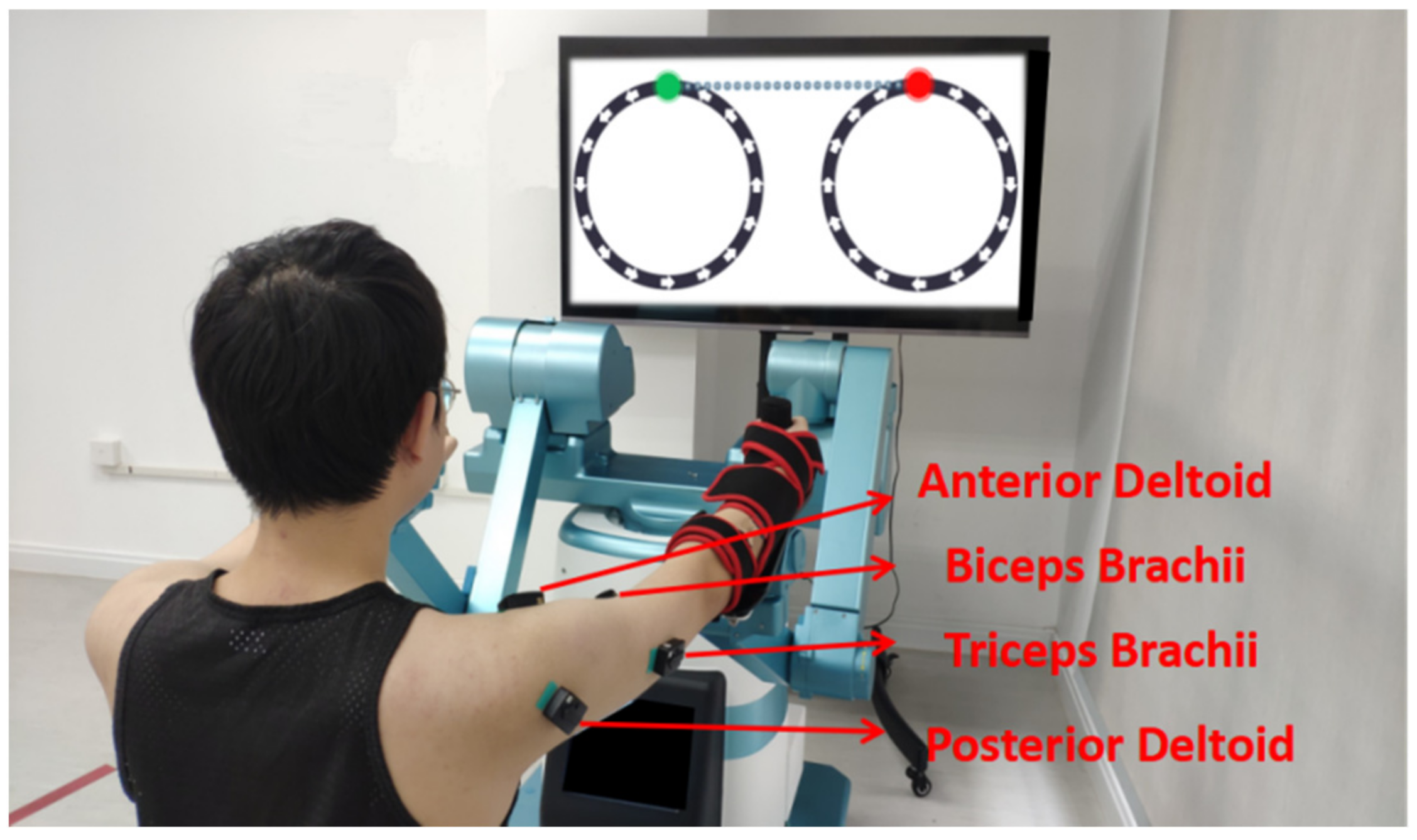
The experiment was carried out by a healthy volunteer aged 25 years and measured 175 cm tall. During the experiment, the volunteer sat opposite the rehabilitation robot and placed a screen in front of it to display the designed virtual environment, and visually induced the volunteer to do tasks (
Figure 7).
In the experiment, the DelsysTrigno device was used to collect EMG signals, and the sampling rate was 1927 Hz. The control period of the rehabilitation robot system was 1 ms. During the interaction between the volunteer and the rehabilitation robot, the position information and force sensor information of the affected side of the robot arm were collected, and the emG signals of the volunteer’s biceps brachii, triceps brachii, anterior deltoid and posterior deltoid muscles were collected at the corresponding time.
This experiment asked the volunteer to achieve the two different states in the two groups of experiments. In the first group of experiments, the volunteer was asked to simulate the state of a healthy person to interact with the robot; in the second group of experiments, the volunteer was asked to simulate the state of a patient to interact with the robot. The initial position was set in the distal circle, as shown in
Figure 6. The volunteer adjusted their state according to the terminal real-time trajectory displayed on the screen, and the speed should not be too fast. Each group of experiments carried out five circle drawing tasks. When the GMM algorithm is used for classification, the size of data will affect the processing speed, so the sampling rate in the system is reduced to 20 Hz to improve the processing efficiency.
As the time for the volunteer to complete the task could not be guaranteed during the experiment, there was no periodic correspondence between the EMG signals of the two states in
Figure 8. As can be seen from
Figure 8, the EMG signal values of the simulated patient are generally higher than that of the healthy subject, which is due to the presence of the volunteer’s simulated muscle tension. The anterior deltoid and the posterior deltoid muscles in the two states of the volunteer are the same under the overall trend, so only the analysis of the biceps brachii and the triceps brachii occurred.
Figure 8 showed that the exercise cycle was about 11–12 s. As can be seen from the EMG signals of biceps brachii and triceps brachii, the EMG signals gradually increased during 0~6 s at each cycle, corresponding to the blue area in the upper half of the circle (y > 0). In
Figure 9 and
Figure 10, the volunteer actively contracts his arm, at this time the EMG signal of the biceps brachii is higher in the healthy subject than in the patient, and those of the triceps brachii is lower in the healthy subject than in the patient. In 6~12 s of each cycle, the EMG signal of the healthy subject showed no obvious increase in the biceps brachii, but an obvious increase in the triceps brachii, corresponding to the blue area in the lower half-circle (y < 0) of
Figure 9, however, the EMG signal of the patient showed that the EMG signal of the biceps brachii is further increased and that of the triceps brachii decreased, corresponding to the red area in
Figure 10 in the lower half of the circle (y < 0). At this time, the EMG signal of the biceps brachii is lower in the healthy subject than in the patient, and those of the triceps brachii is also lower in the healthy subject than in the patient.
To analyze the reasons for the above phenomena, when the volunteer completes the task of drawing a circle, the arms contracting (y > 0) relies mainly on the biceps brachii. Therefore, the biceps brachii of the healthy subject will actively contract and activate, and the patient’s biceps brachii—because of their upper limb muscle paralysis—cannot activate; the triceps brachii was forced to stretch, and hence, in each cycle of 0~6 s the EMG signal of the biceps brachii is higher in the healthy subject than in the patient, and those of the triceps brachii are lower in the healthy subject than in the patient. Arm extension (y < 0) relies mainly on the triceps brachii, and therefore the triceps brachii of the healthy subject will actively contract and activate, while the patient cannot activate the triceps brachii. Furthermore, the biceps brachii was forced to stretch, and hence, in each cycle of 6~12 s, the EMG signal of the biceps brachii is lower in the healthy subject than in the patient. Additionally, the triceps brachii muscle signal increased in the healthy subject, while the triceps brachii muscle signal directly decreased in the patient. The experiment showed that the patient simulated by the volunteer was actively completing the task in the blue area, while in the red area, due to the presence of muscle tension, passively completing the task would increase the muscle tension of the biceps brachii, thus hindering the completion of the rehabilitation task. The effectiveness of the GMM classification was verified by comparing the EMG and GMM classification of tasks completed by the volunteer in this experiment.
3.4. AAN Control Strategy Experiment
In the design of the controller, after the subjects’ first task, the GMM algorithm can identify areas where the subjects need and do not need assistance. When the subjects started the second task, the controller will judge the area where the subjects are currently located and only provide necessary assistance according to the AAN strategy. After the subjects’ second task, the GMM algorithm would continue to identify the state of the subjects completing the task. In order to verify the effectiveness of the designed controller, the online experiment was completed by a healthy volunteer aged 24 years and measured 172 cm tall. During the experiment, the volunteer was asked to simulate a patient interaction with the robot (drawing a circle task).
Table 2 shows the subject in the active and passive rehabilitation area of each task period, and corresponds to the error of the mean value and mean assistance force. Although the mean error of the active rehabilitation area is larger than the mean error of the passive rehabilitation area, the mean of the active rehabilitation area assistance force is much smaller than the mean of the passive rehabilitation area assistance force.
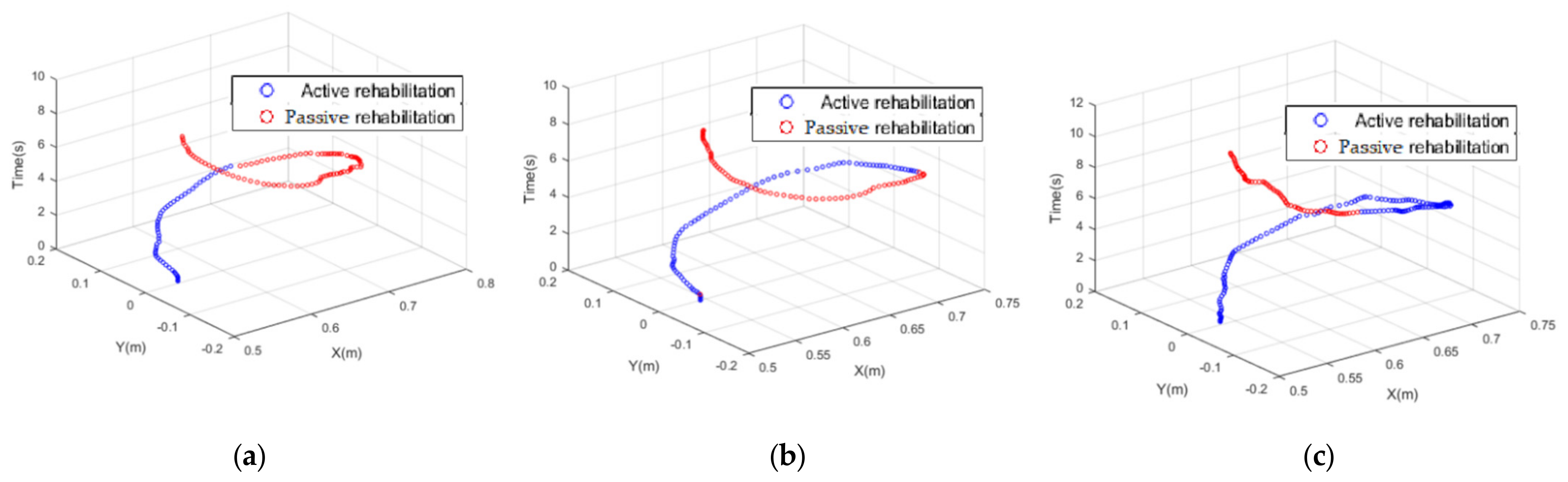
Figure 11 shows GMM classifies the task completion status of volunteer.
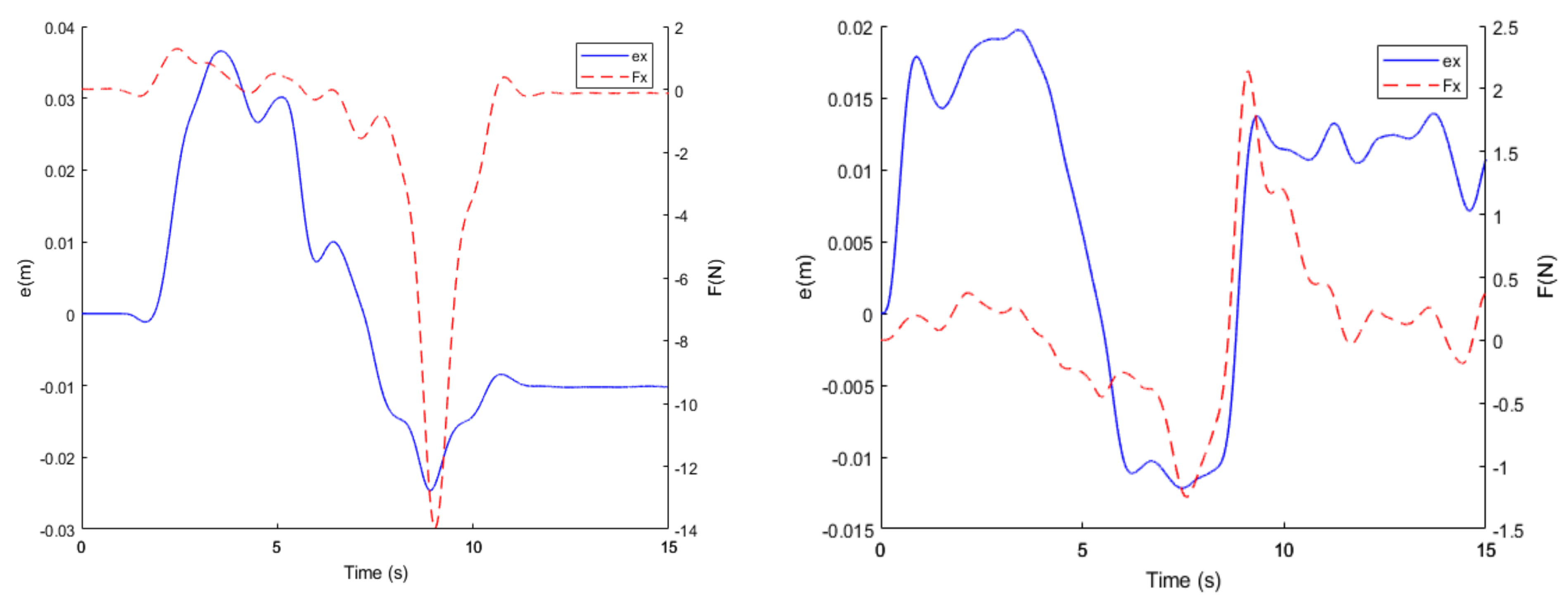
Figure 12 shows one period in which the subject completed the task, at 2–5 s. The GMM algorithm identifies the area where the subject is in active rehabilitation (the blue area in
Figure 11), so within this area, even though there is a large error between the two sides of the subject (0.04 m > |ex| > 0.03 m, 0.02 m > |ey| > 0.015 m), and the controller does not provide much assistance force (0 N < |Fx| < 2 N, 0 N < |Fy| < 0.5 N), only when the end of the subject is in the passive rehabilitation area (the red area in
Figure 11) will the controller be designed according to the error generated between the two sides of the subject (0.02 m < |ex| < 0.03 m, 0.01 m < |ey| < 0.015 m). This provides suitable assistance force (15 N < |Fx| < 10 N, 2.5 N < |Fy| < 1 N) to help the subject to complete the task.
Figure 13 shows the different classification states that GMM can achieve according to the degree of active task completion of the subject, which further proves that the GMM algorithm can identify subjects simulating different muscle tension and provide corresponding assistance.
3.5. Security Verification
During the interaction between the patients and the rehabilitation robot, when PIL switches from the active rehabilitation position to the passive rehabilitation position, the sudden change of K value will lead to the mutation of the assistance force, which is not safe for the patients. Therefore, according to the transition function designed by Equation (12). The experiment was completed by a healthy volunteer aged 26 years and 178 cm in height. During the experiment, the volunteer was asked to simulate a patient interaction with the robot (drawing a circle task). During the movement of the experiment,
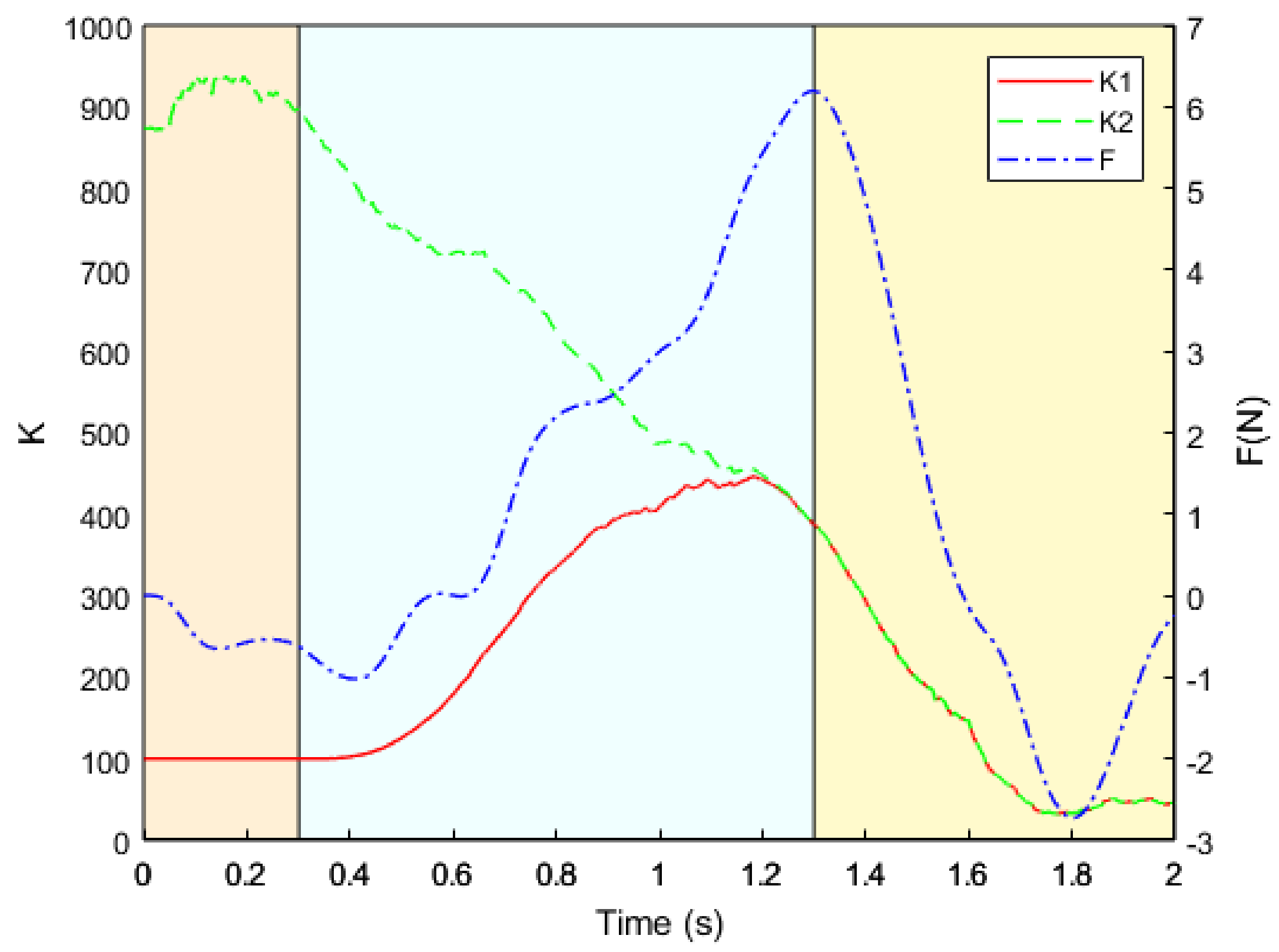
Figure 14 shows the change of K value when the active rehabilitation position is switched to the passive rehabilitation position.
In
Figure 14, the red line K1 represents the real-time K value, the green line K2 represents the calculated K value, and the blue line F represents the change in the real-time assistance force. As can be seen from
Figure 14, at about 0.3 s, the real-time K1 value begins to transition from the initial value of the active rehabilitation position to the K2 value calculated from the passive rehabilitation position, and one second later, the actual K1 value transitions to the calculated K2 value, at which point K1 = K2. It can be seen from this experiment that the designed transition function ensures the safety of the system and prevents the sudden change of K value from causing a surge in assistance force, which leads to risk with subjects.
4. Discussion
The AAN strategy is a relatively common assistance strategy in rehabilitation treatment. Nonetheless, the traditional AAN only succeeds in identifying whether the patients are currently able to complete the task [
8,
9]. The identification of the remaining ability of patients is more complex [
5,
7,
10], without further identifying whether the patients are in a state of needing assistance when completing the task, which has great limitations. Nonetheless, because of the advantages of the GMM algorithm in data modeling [
15], and how GMM has been successfully applied in robot demonstration learning [
16,
17,
18], this paper proposes an AAN control strategy based on GMM in order to solve the problem of whether patients need assistance when completing tasks. Firstly, a new end-effector bilateral mirror upper limb rehabilitation robot was designed for patients with upper limb motor dysfunction, differentiating it from other upper limb rehabilitation robots [
18,
21] that can only be provided by the virtual environment, which cannot accurately express the real intention of the patient. Furthermore, with the upper limb rehabilitation robot proposed in this paper, patients could use the robot PFL to provide rehabilitation trajectory for PIL. Secondly, a new rehabilitation robot is a proposed AAN control strategy. Different from the traditional AAN control strategy, which only identifies whether the patients can complete the task at present [
8,
9], the recognition means the remaining ability of the patient is relatively complex [
5,
7,
10]. In this paper, the GMM algorithm was used to classify the physical information of patients when they completed the task, and the results enabled us to guide the adaptive change of robot assistance force according to the degree of the patient’s participation; its advantage is that it can provide patients with as much assistance-as-needed (AAN). Finally, in order to induce the patient to recover, we designed a circular motion trajectory for the patients in the virtual environment. During the task, the AAN strategy can only provide the patients with assistance when necessary and according to the active participation degree that the patients can provide, allowing the patients to complete the task autonomously.
Compared with traditional rehabilitation robot assistance strategies, the proposed AAN control strategy for the bilateral upper limb mirror rehabilitation robot has the following advantages: The movement trajectory of PFL can more accurately reflect the patient’s movement intention; the AAN control strategy designed, based on GMM, can determine the areas that patients need assistance according to the degree of active participation of the patients; and although the rehabilitation robot designed in this paper can carry out rehabilitation training in three-dimensional space, this paper restricts the trajectory to a plane for subjects to better feel the assistance force. However, the controller proposed in this paper does not depend on the design of the training trajectory, and its performance has no influence on any spatial trajectory.


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}