
Biomechanics of Ascending and Descending Stairs in a Patient with Transfemoral Amputation and Neural Sensory Feedback: A Case Report

 , , , ,
, , , ,  , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample of Respondents
2.2. Sample of Parameters
- STANCE_NSFB—ascending/descending stance phase in s;
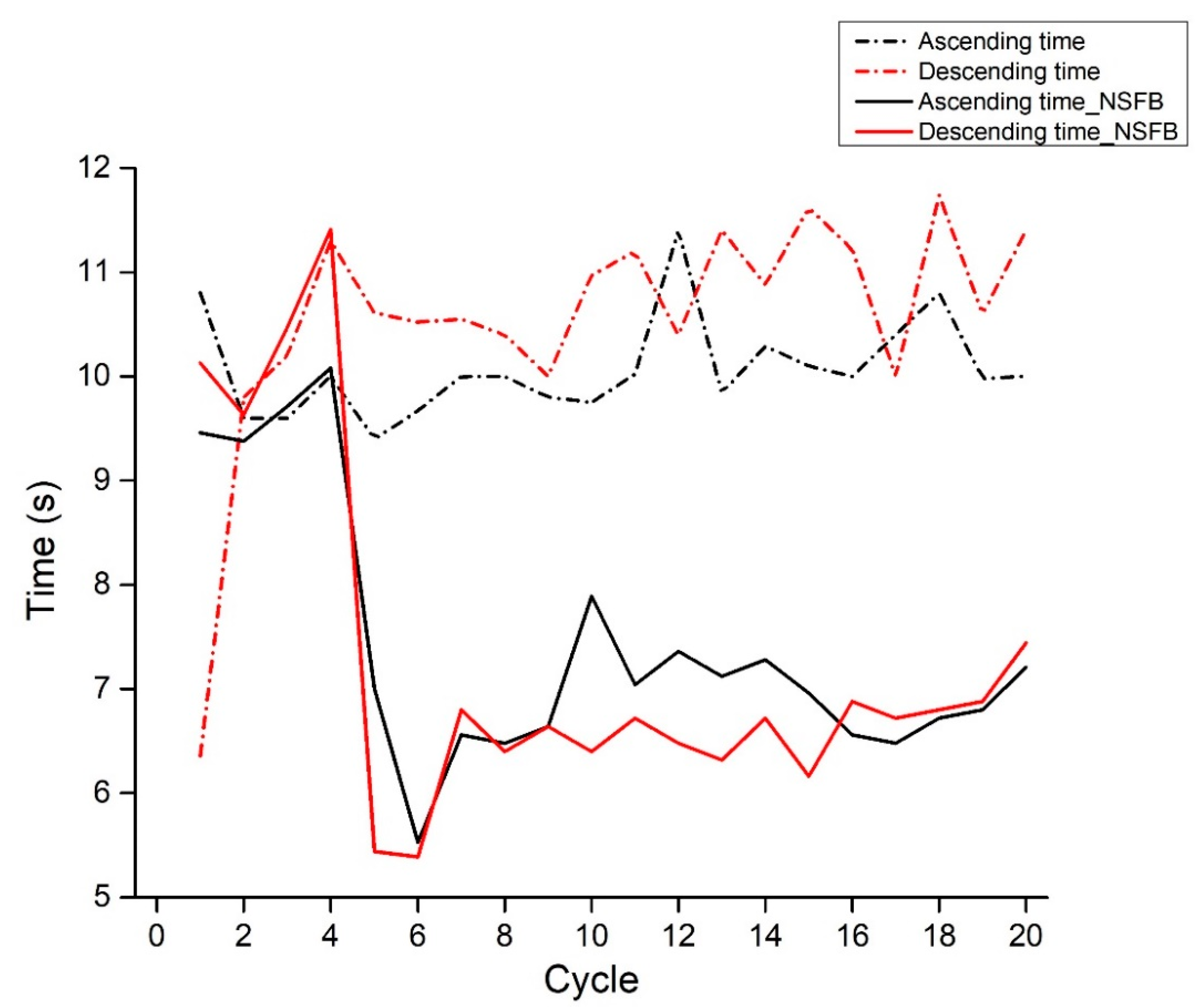
- TIME_NSFB—ascending/descending cycle in s;
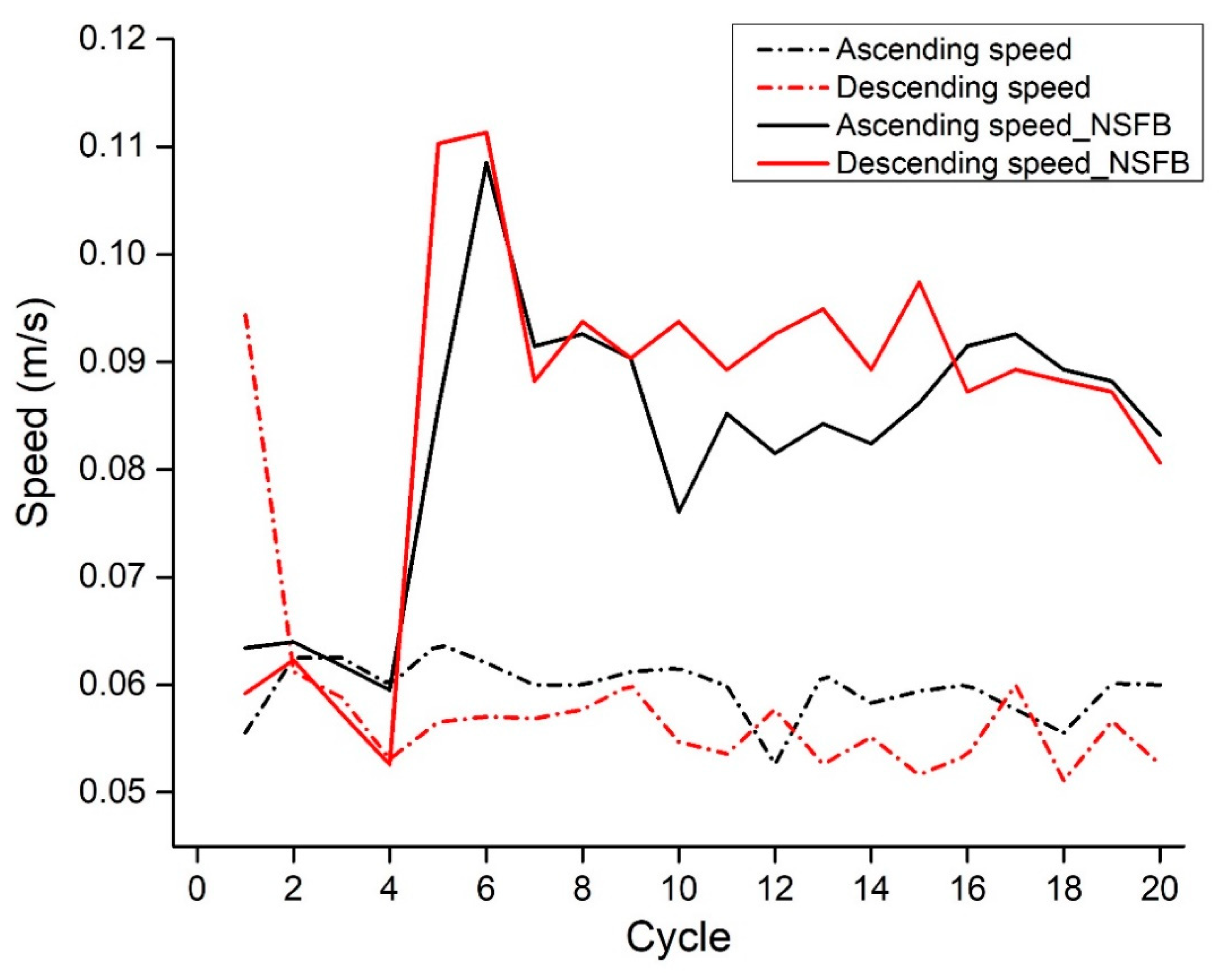
- SPEED_NSFB—ascending/descending speed in m/s.
2.3. Description of NSFB in This Experiment
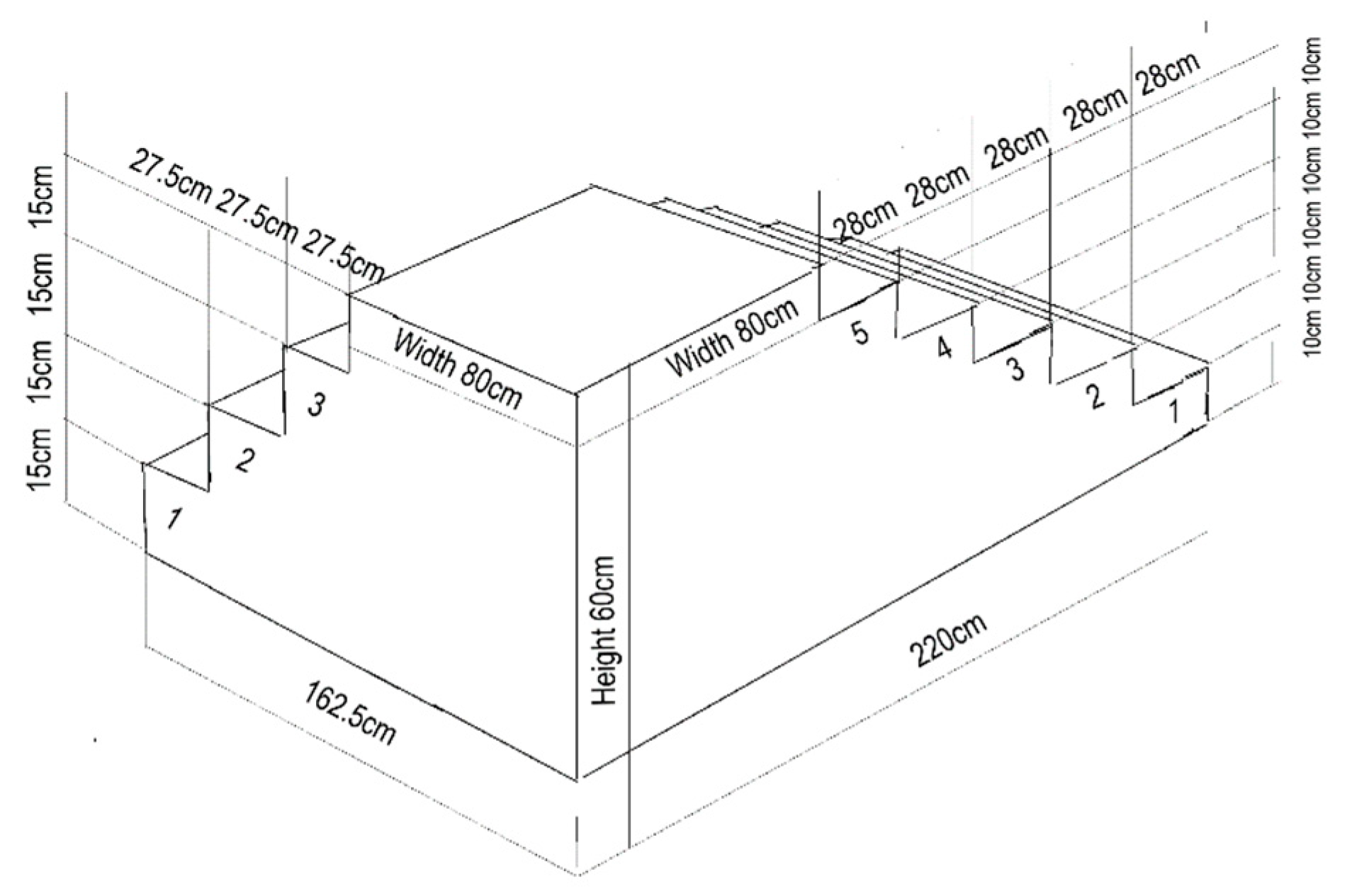
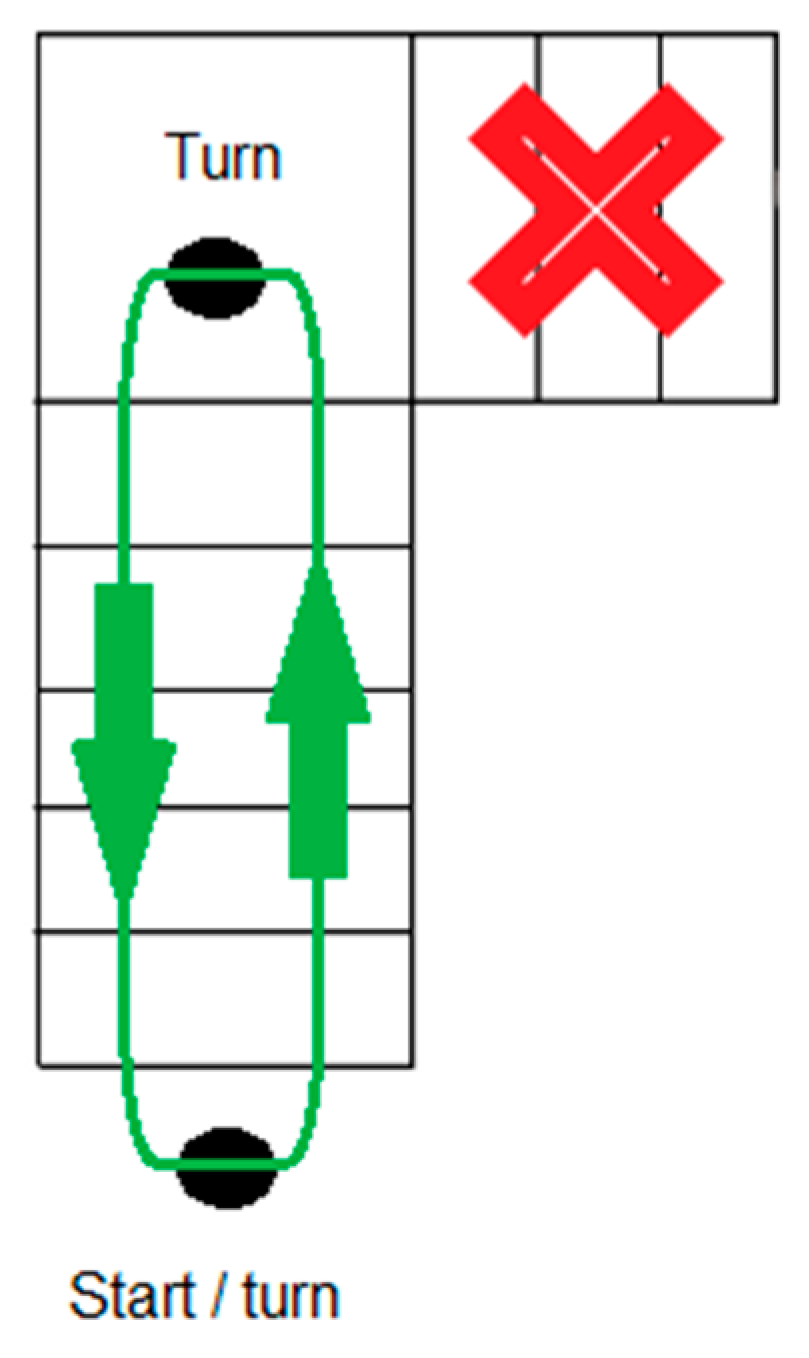
2.4. Testing Procedure and Instrumentation
2.5. Data Processing Method
- Signal acquisition: We imported into Kinovea software a recorded footage of 20 gait cycles from the camera and extracted relevant signals from the recorded motion using frame-by-frame analysis of the video.
- Signal processing: Once the video was imported into Kinovea software, we performed signal processing. This included extracting specific points with markers from the video frames to track the ascending and descending of stairs. We used a combination of automatic and manual tracking tools to track the movement of selected body parts (foot, ankle joint, knee joint, hip joint, wrist joint, elbow joint, shoulder joint, head) throughout the video sequence and to calculate the position and speed of the tracked points over time. The entire process of both automatic and manual tracking was enabled by placing reflective markers on the specified anatomical landmarks of the participant’s body. After entering the appropriate scale and tracking, Kinovea software automatically calculated the values of the parameters of interest in our case study.
- Signal trimming: Where necessary, signals were trimmed to focus on specific segments of the motion. This trimming process helped us in isolating specific movements and time intervals for further analysis.
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Crane, H.; Boam, G.; Carradice, D.; Vanicek, N.; Twiddy, M.; Smith, G.E. Through-knee versus above-knee amputation for vascular and non-vascular major lower limb amputations. Cochrane Database Syst. Rev. 2021, 12, CD013839. [Google Scholar] [CrossRef]
- Harding, J.L.; Andes, L.J.; Rolka, D.B.; Imperatore, G.; Gregg, E.W.; Li, Y.; Albright, A. National and state-level trends in nontraumatic lower-extremity amputation among US medicare beneficiaries with diabetes, 2000–2017. Diabetes Care. 2020, 43, 2453–2459. [Google Scholar] [CrossRef] [PubMed]
- Mabarak, D.; Behzadi, F.; Yang, M.; Wozniak, A.; Patel, P.; Aulivola, B. Concomitant orthopedic injury is the strongest predictor of amputation in extremity vascular trauma. Ann. Vasc. Surg. 2023, 91, 161–167. [Google Scholar] [CrossRef]
- Meshkin, D.H.; Zolper, E.G.; Chang, K.; Bryant, M.; Bekeny, J.C.; Evans, K.K.; Attinger, C.E.; Fan, K.L. Long-term mortality after nontraumatic major lower extremity amputation: A systematic review and meta-analysis. J. Foot Ankle Surg. 2021, 60, 567–576. [Google Scholar] [CrossRef]
- Regalado-Solís, F.; Ziga-Martínez, A.; Olivares-Cruz, S.; Sierra-Juárez, M.Á.; Santillán-Aguayo, E.; Fabián-Mijangos, W.; Carbajal-Robles, V. Perioperative morbidity and mortality in patients with dysvascular amputations. Rev. Mex. Angiol. 2021, 49, 80–87. [Google Scholar] [CrossRef]
- Gailey, R.; Allen, K.; Castles, J.; Kucharik, J.; Roeder, M. Review of secondary physical conditions associated with lower-limb amputation and long-term prosthesis use. J. Rehabil. Res. Dev. 2008, 45, 15–29. [Google Scholar] [CrossRef]
- Burke, M.J.; Roman, V.; Wright, V. Bone and joint changes in lower limb amputees. Ann. Rheum. Dis. 1978, 37, 252–254. [Google Scholar] [CrossRef]
- Kulkarni, J.; Adams, J.; Thomas, E.; Silman, A. Association between amputation, arthritis and osteopenia in British male war veterans with major lower limb amputations. Clin. Rehabil. 1998, 12, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Pagan-Rosado, R.; Smith, B.J.; Smither, F.C.; Pingree, M.J.; D’Souza, R.S. Peripheral nerve stimulation for the treatment of phantom limb pain: A case series. Case Rep. Anesthesiol. 2023, 2023, 1558183. [Google Scholar] [CrossRef]
- Bruinsma, J.; Carloni, R. Imu-based deep neural networks: Prediction of locomotor and transition intentions of an osseointegrated transfemoral amputee. IEEE Trans. Neural Syst. Rehabil. 2021, 29, 1079–1088. [Google Scholar] [CrossRef]
- Murray, R.; Mendez, J.; Gabert, L.; Fey, N.P.; Liu, H.; Lenzi, T. Ambulation mode classification of individuals with transfemoral amputation through a-mode sonomyography and convolutional neural networks. Sensors. 2022, 22, 9350. [Google Scholar] [CrossRef] [PubMed]
- Parri, A.; Martini, E.; Geeroms, J.; Flynn, L.; Pasquini, G.; Crea, S.; Molino Lova, R.; Lefeber, D.; Kamnik, R.; Munih, M.; et al. Whole body awareness for controlling a robotic transfemoral prosthesis. Front. Neurorobot. 2017, 11, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarvis, H.L.; Bennett, A.N.; Twiste, M.; Phillip, R.D.; Etherington, J.; Baker, R. Temporal spatial and metabolic measures of walking in highly functional individuals with lower limb amputations. Arch. Phys. Med. Rehabil. 2017, 98, 1389–1399. [Google Scholar] [CrossRef] [Green Version]
- Hagberg, K.; Haggstrom, E.E.; Branemark, R. Physiological cost index (PCI) and walking performance in individuals with transfemoral prostheses compared to healthy controls. Disabil. Rehabil. 2007, 29, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Wentink, E.C.; Prinsen, E.C.; Rietman, J.S.; Veltink, P.H. Comparison of muscle activity patterns of transfemoral amputees and control subjects during walkin. J. Neuroeng. Rehabil. 2013, 10, 87–98. [Google Scholar] [CrossRef] [Green Version]
- Highsmith, M.J.; Andrews, C.R.; Millman, C.; Fuller, A.; Kahle, J.T.; Klenow, T.D.; Lewis, K.L.; Bradley, R.C.; Orriola, J.J. Gait training interventions for lower extremity amputees: A systematic literature review. Technol. Innov. 2016, 18, 99–113. [Google Scholar] [CrossRef] [Green Version]
- Boonstra, A.M.; Schrama, J.; Fidler, V.; Eisma, W.H. The gait of unilateral transfemoral amputees. Scand. J. Rehabil. 1994, 26, 217–223. [Google Scholar] [CrossRef]
- Kowal, M.; Winiarski, S.; Gieysztor, E.; Kołcz, A.; Dumas, I.; Paprocka-Borowicz, M. Symmetry function: The differences between active and non-active above-the-knee amputees. Sensors 2022, 22, 5933. [Google Scholar] [CrossRef]
- Kaufman, K.R.; Frittoli, S.; Frigo, C.A. Gait asymmetry of transfemoral amputees using mechanical and microprocessor-controlled prosthetic knees. Clin. Biomech. 2012, 27, 460–465. [Google Scholar] [CrossRef] [Green Version]
- Tura, A.; Rocchi, L.; Raggi, M.; Cutti, A.; Chiari, L. Recommended number of strides for automatic assessment of gait symmetry and regularity in above-knee amputees by means of accelerometry and autocorrelation analysis. J. Neuroeng. Rehabil. 2012, 9, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Tura, A.; Raggi, M.; Rocchi, L.; Cutti, A.G.; Chiari, L. Gait symmetry and regularity in transfemoral amputees assessed by trunk accelerations. J. Neuroeng. Rehabil. 2010, 7, 4–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pather, S.; Sondergeld, P.; Epari, D.; Pearcy, M.J.; Frossard, L.A. A Synthesis of the Range of Loads Applied on the Residuum of Individuals with Transfemoral Amputation Fitted with Bone-Anchored Prostheses. In Proceedings of the ISPO World Congress, Cape Town, South Africa, 8–11 May 2017; (Unpublished). Available online: http://eprints.qut.edu.au/104643/ (accessed on 18 February 2023).
- Farina, D.; Vujaklija, I.; Brånemark, R.; Bull, A.M.; Dietl, H.; Graimann, B.; Hargrove, L.J.; Hoffmann, K.-P.; Huang, H.; Ingvarsson, T.; et al. Toward higher-performance bionic limbs for wider clinical use. Nat. Biomed. Eng. 2023, 7, 473–485. [Google Scholar] [CrossRef]
- Raspopovic, S. Advancing limb neural prostheses. Science 2020, 370, 290–291. [Google Scholar] [CrossRef]
- Petrini, F.M.; Bumbasirevic, M.; Valle, G.; Ilic, V.; Mijovic, P.; Cvancara, P.; Barberi, F.; Katić, N.; Bortolotti, D.; Andreu, D.; et al. Sensory feedback restoration in leg amputees improves walking speed, metabolic cost and phantom pain. Nat. Med. 2019, 25, 1356–1363. [Google Scholar] [CrossRef] [Green Version]
- Rossignol, S.; Dubuc, R.; Gossard, J.-P. Dynamic sensorimotor interactions in locomotion. Physiol. Rev. 2006, 86, 89–154. [Google Scholar] [CrossRef] [PubMed]
- Valle, G.; Saliji, A.; Fogle, E.; Cimolato, A.; Petrini, F.M.; Raspopovic, S. Mechanisms of neuro-robotic prosthesis operation in leg amputees. Sci. Adv. 2021, 7, eabd8354. [Google Scholar] [CrossRef]
- Hickox, L. Exploration of the Validity of the Two-Dimensional Sagittal Plane Standing Long Jump Model. Master’s Thesis, Grand Valley State University, Padnos College of Engineering and Computing, Allendale, MI, USA, 2014. Available online: https://scholarworks.gvsu.edu/cgi/viewcontent.cgi?article=1721&context=theses (accessed on 18 February 2023).
- Puig-Diví, A.; Escalona-Marfil, C.; Padullés-Riu, J.M.; Busquets, A.; Padullés-Chando, X.; Marcos-Ruiz, D. Validity and reliability of the Kinovea program in obtaining angles and distances using coordinates in 4 perspectives. PLoS ONE. 2019, 14, e0216448. [Google Scholar] [CrossRef] [PubMed]
- Pueo, B.; Penichet-Tomas, A.; Jimenez-Olmedo, J.M. Validity, reliability and usefulness of smartphone and Kinovea motion analysis software for direct measurement of vertical jump height. Physiol. Behav. 2020, 227, 113144. [Google Scholar] [CrossRef]
- Pallant, J. SPSS Survival Manual: A Step by Step Guide to Data Analysis Using SPSS, 7th ed.; Routledge: London, UK, 2020. [Google Scholar]
- Raspopovic, S.; Petrini, F.M. The Prosthetic Leg Speaks to the Brain through a Wireless Link with the Nerves in the Upper Leg of Subjects. IEE.org. 2019. Available online: https://brain.ieee.org/newsletter/2019-issue-3/the-prosthetic-leg-speaks-to-the-brain-through-a-wireless-link-with-the-nerves-in-the-upper-leg-of-subjects/ (accessed on 10 March 2023).
- Hood, S.; Creveling, S.; Gabert, L.; Tran, M.; Lenzi, T. Powered knee and ankle prostheses enable natural ambulation on level ground and stairs for individuals with bilateral above-knee amputation: A case study. Sci. Rep. 2022, 12, 15465. [Google Scholar] [CrossRef]
- Preatoni, G.; Valle, G.; Petrini, F.M.; Raspopovic, S. Lightening the perceived prosthesis weight with neural embodiment promoted by sensory feedback. Curr. Biol. 2021, 31, 1065–1071. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Ascending Stairs | Descending Stairs | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Healthy leg | N | NSFB | Mean | SD | SE | Mean | SD | SE | |
| STANCE (s) | 20 | With | 3.783 | 0.398 | 0.089 | 3.686 | 0.288 | 0.064 | |
| Without | 4.140 | 0.316 | 0.070 | 3.886 | 0.275 | 0.061 | |||
| Prosthetic leg | With | 2.990 | 0.288 | 0.060 | 2.988 | 0.260 | 0.058 | ||
| Without | 3.086 | 0.360 | 0.080 | 3.413 | 0.301 | 0.067 | |||
| Condition | Ascending Stairs | Descending Stairs | ||||||
|---|---|---|---|---|---|---|---|---|
| TIME (s) | N | NSFB | Mean | SD | SE | Mean | SD | SE |
| 20 | With | 7.413 | 1.246 | 0.278 | 7.291 | 1.691 | 0.378 | |
| Without | 10.072 | 0.476 | 0.106 | 10.558 | 1.138 | 0.254 | ||
| SPEED (m/s) | With | 0.082 | 0.012 | 0.002 | 0.085 | 0.016 | 0.003 | |
| Without | 0.059 | 0.002 | 0.000 | 0.057 | 0.009 | 0.002 | ||
| Pair | STANCE (s) | Mean | SD | t-Test | df | Sig. (2-Tailed) |
|---|---|---|---|---|---|---|
| 1 | A_STANCEH | 4.140 | 0.316 | 14.635 | 19 | 0.000 |
| A_STANCEP | 3.086 | 0.361 | ||||
| 2 | A_STANCEH_NSFB | 3.783 | 0.399 | 3.373 | 19 | 0.003 |
| A_STANCEP_NSFB | 3.346 | 0.402 | ||||
| 3 | A_STANCEH | 4.140 | 0.316 | 4.678 | 19 | 0.000 |
| A_STANCEH_FB | 3.783 | 0.399 | ||||
| 4 | A_STANCEP | 3.086 | 0.361 | −2.919 | 19 | 0.009 |
| A_STANCEP_FB | 3.346 | 0.402 | ||||
| 5 | D_STANCEH | 3.886 | 0.275 | 4.900 | 19 | 0.000 |
| D_STANCEP | 3.413 | 0.302 | ||||
| 6 | D_STANCEH_NSFB | 3.686 | 0.288 | 8.252 | 19 | 0.000 |
| D_STANCEP_NSFB | 2.988 | 0.261 | ||||
| 7 | D_STANCEH | 3.886 | 0.275 | 3.734 | 19 | 0.001 |
| D_STANCEH_NSFB | 3.686 | 0.288 | ||||
| 8 | D_STANCEP | 3.413 | 0.302 | 8.799 | 19 | 0.000 |
| D_STANCEP_NSFB | 2.988 | 0.261 |
| Pair | TIME (s) | Mean | SD | t-Test | df | Sig. (2-Tailed) |
|---|---|---|---|---|---|---|
| 1 | A_TIME | 10.072 | 0.476 | 8.860 | 19 | 0.000 |
| A_TIME_NSFB | 7.413 | 1.246 | ||||
| 2 | D_TIME | 10.558 | 1.138 | 6.128 | 19 | 0.000 |
| D_TIME_NSFB | 7.291 | 1.691 |
| Pair | SPEED (m/s) | Mean | SD | t-Test | df | Sig. (2-Tailed) |
|---|---|---|---|---|---|---|
| 1 | A_SPEED | 0.060 | 0.003 | −8.203 | 19 | 0.000 |
| A_SPEED_NSFB | 0.083 | 0.012 | ||||
| 2 | D_SPEED | 0.058 | 0.009 | −5.843 | 19 | 0.000 |
| D_SPEED_NSFB | 0.086 | 0.016 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bubanj, S.; Radenković, M.; Stanković, D.; Petković, E.; Lilić, A.; Bojić, I.; Aksović, N.; Dobrescu, T.; Bjelica, B.; Ćuk, I.; et al. Biomechanics of Ascending and Descending Stairs in a Patient with Transfemoral Amputation and Neural Sensory Feedback: A Case Report. Symmetry 2023, 15, 1443. https://doi.org/10.3390/sym15071443
Bubanj S, Radenković M, Stanković D, Petković E, Lilić A, Bojić I, Aksović N, Dobrescu T, Bjelica B, Ćuk I, et al. Biomechanics of Ascending and Descending Stairs in a Patient with Transfemoral Amputation and Neural Sensory Feedback: A Case Report. Symmetry. 2023; 15(7):1443. https://doi.org/10.3390/sym15071443
Chicago/Turabian StyleBubanj, Saša, Marko Radenković, Dušan Stanković, Emilija Petković, Ana Lilić, Ivana Bojić, Nikola Aksović, Tatiana Dobrescu, Bojan Bjelica, Ivan Ćuk, and et al. 2023. "Biomechanics of Ascending and Descending Stairs in a Patient with Transfemoral Amputation and Neural Sensory Feedback: A Case Report" Symmetry 15, no. 7: 1443. https://doi.org/10.3390/sym15071443