1. Introduction
Computed tomography (CT) is a widely used clinical examination because of its fast scan time and the advantages of its three-dimensional representation of the human body. Although CT has the potential to increase the radiation dose to the patient, the sensitivity and specificity among diagnostic images is very high, so CT scans for disease diagnosis in clinical examinations are increasing. Despite concerns about radiation risks in children, the need for pediatric CT examinations continues to grow. CT of the pediatric body, including in an emergency room and for patients with cancer, is an important type of imaging for children [
1]. Since children have a longer life expectancy and are more sensitive to radiation than adults, children are at risk of radiation-induced damage. Therefore, there is a need to minimize the dose received during CT examination in diagnostic radiology and pediatric CT. This is because children have a high risk of developing cancer compared with adults receiving equivalent doses. In France, there are pediatric diagnostic reference levels (DRLs) that are regularly updated by the Institute for Radiation Protection and Nuclear Safety (IRSN) and the French Society for Pediatric and Prenatal Imaging (SFFIPP) [
2]. This states that according to the principles of as low as reasonably achievable (ALARA), delivered doses should be evaluated regularly for comparison with DRL and should not be exceeded without justification.
With the development of technology, efforts have been made to reduce the radiation dose children are exposed to by pediatric CT scans. For the implementation of low-dose CT, the CT protocol includes automatic exposure control (AEC) [
3], tube current control, and tube voltage optimization [
4]. In addition, studies have considered the protocols for dose optimization in pediatric CT scans [
5]. CT protocol optimization is performed through changing imaging parameters. Although this method is simple, it has limitations in fundamentally reducing pediatric dose. Moreover, a low-dose implementation can be achieved through a hardware approach, such as using a photon-counting detector. When using a photon-counting detector, image data without any electronic noise can be obtained [
6]; furthermore, the energy discrimination function optimizes the signal summation according to energy to increase the signal-to-noise ratio (SNR) [
7]. However, photon-counting detectors have difficulties in X-ray imaging in which a large amount of radiation is emitted. Photon-counting detectors have phenomena of pulse pile-up and charge-sharing. Pile-up is when photons arrive too fast and some of the resulting electrical pulses overlap each other, resulting in count loss at high count rates. A small electrode is required to avoid pile-up, which causes energy dissipation due to secondary photons or charge diffusion. Therefore, the application of photon-counting detectors for rapid X-ray based inspection is still difficult.
Recently, software methods, such as iterative reconstruction (IR) and deep learning reconstruction (DLR), are being used to implement low-dose CT given the rapid development of computing power [
8]. Since DLR reconstructs an image using an artificial neural network trained through prior learning, it is helpful in distinguishing between image signal and noise. Therefore, DLR not only achieves high-quality images with a lower dose than FBP and IR but also achieves a reconstruction speed similar to those of FBP and IR. In particular, DLR has been applied to pediatric CT because it can maintain a high image quality regarding noise reduction, as well as high spatial resolution, even at low doses. Previous studies have included the effect of DLR on image noise, spatial resolution, and radiation dose. Yeoh et al. reported that DLR reduces noise in lumbar CT images [
9]. Greffier et al. investigated that DLR had higher spatial resolution improvements and better dose-reduction effects than IR [
10]. However, there have been no quantitative studies on the effect of tube voltage on pediatric CT images when using DLR.
Therefore, the purpose of this phantom study is to estimate how tube voltage affects the DLR image quality in abdominal pediatric CT. CT images were acquired using a phantom similar to the abdominal size of children and adults. Image quality was measured according to the tube voltage, image reconstruction method, and radiation dose. The image quality of the DLR image was compared with those of FBP and IR.
2. Materials and Methods
Filtered backprojection (FBP) acquires attenuation information of an object obtained by rotating an X-ray tube and a detector, and then backprojects it to obtain an axial image. FBP is very sensitive to noise because it does not consider Poisson distribution and photon number statistics. Therefore, FBP requires radiation dose increments to reduce image noise [
11]. Therefore, FBP requires an increased radiation dose to reduce the noise of CT images.
IR calculates image data that match the acquired projection data. Generally, IR reduces high-frequency noise, but performance of IR is limited in terms of reducing low-frequency noise, resulting in an unnatural image appearance. The IR is divided into hybrid IR and model-based IR (MBIR) according to the level of detail in the image-processing modeling. Hybrid IR minimizes data variability because it iteratively optimizes the physical model of system statistics in projection or image space. MBIR is more accurate and detailed than hybrid IR because it includes not only system statistics but also CT system optics. However, MBIR has a time-consumption problem [
12].
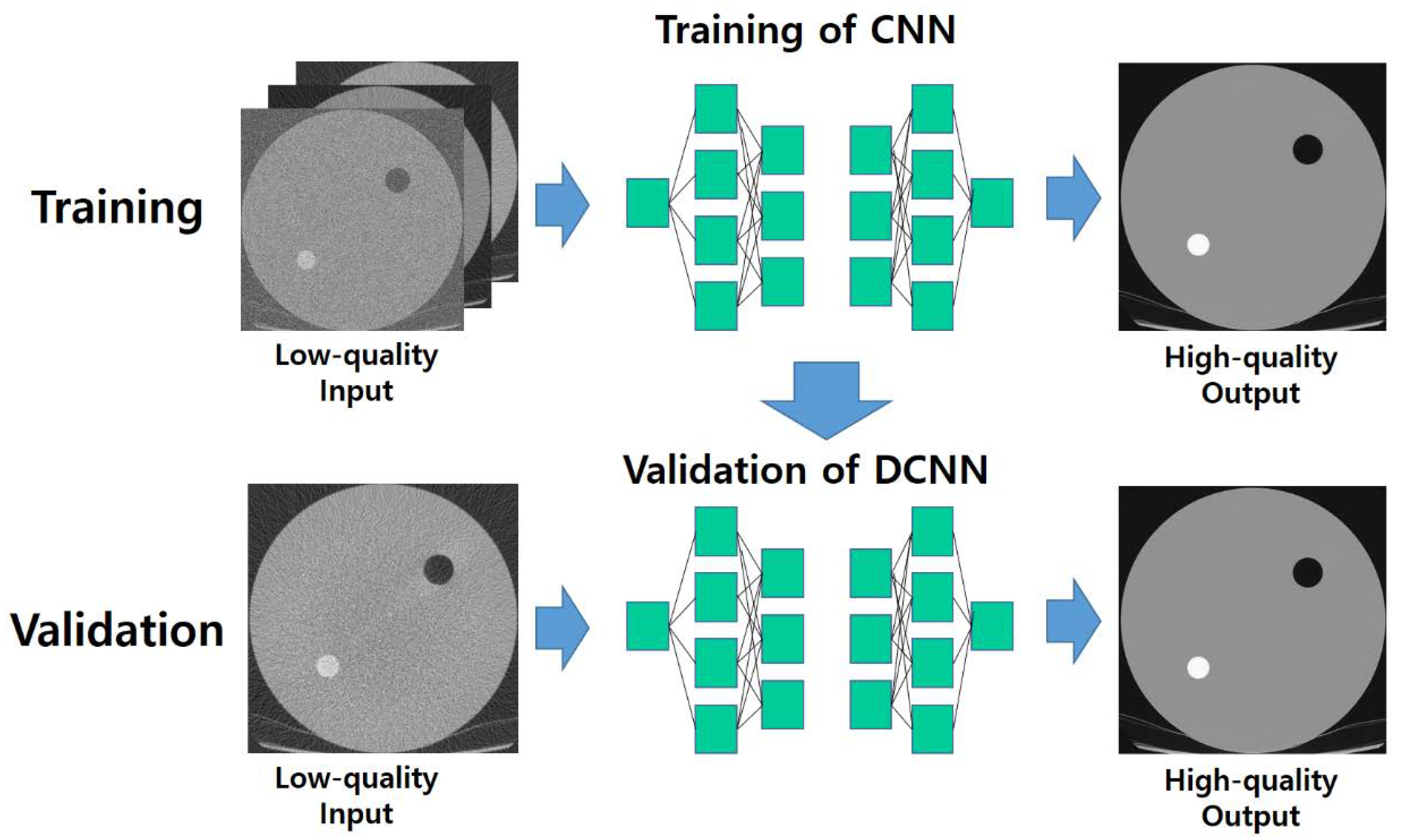
DLR reconstructions are trained to have image quality similar to MBIR images by extracting signals from low-dose hybrid IR images network kernels, as shown in
Figure 1. The network needs to compare the output image to a standard reference image in order to learn (i.e., adjust the weight of the neurons). To achieve this, the deep convolution neural network (DCNN) uses a mathematic loss function to determine the amount of error between the output and the reference data set. Standard reference images are acquired with high tube current and take into account system physics, statistical properties, and modeling of human anatomy. Using the error estimate between output of DCNN and the standard reference image, DCNN adjusts the weights of the neurons to reduce discrepancies with the error estimate through the network. This process is repeated until the network is optimized [
12].
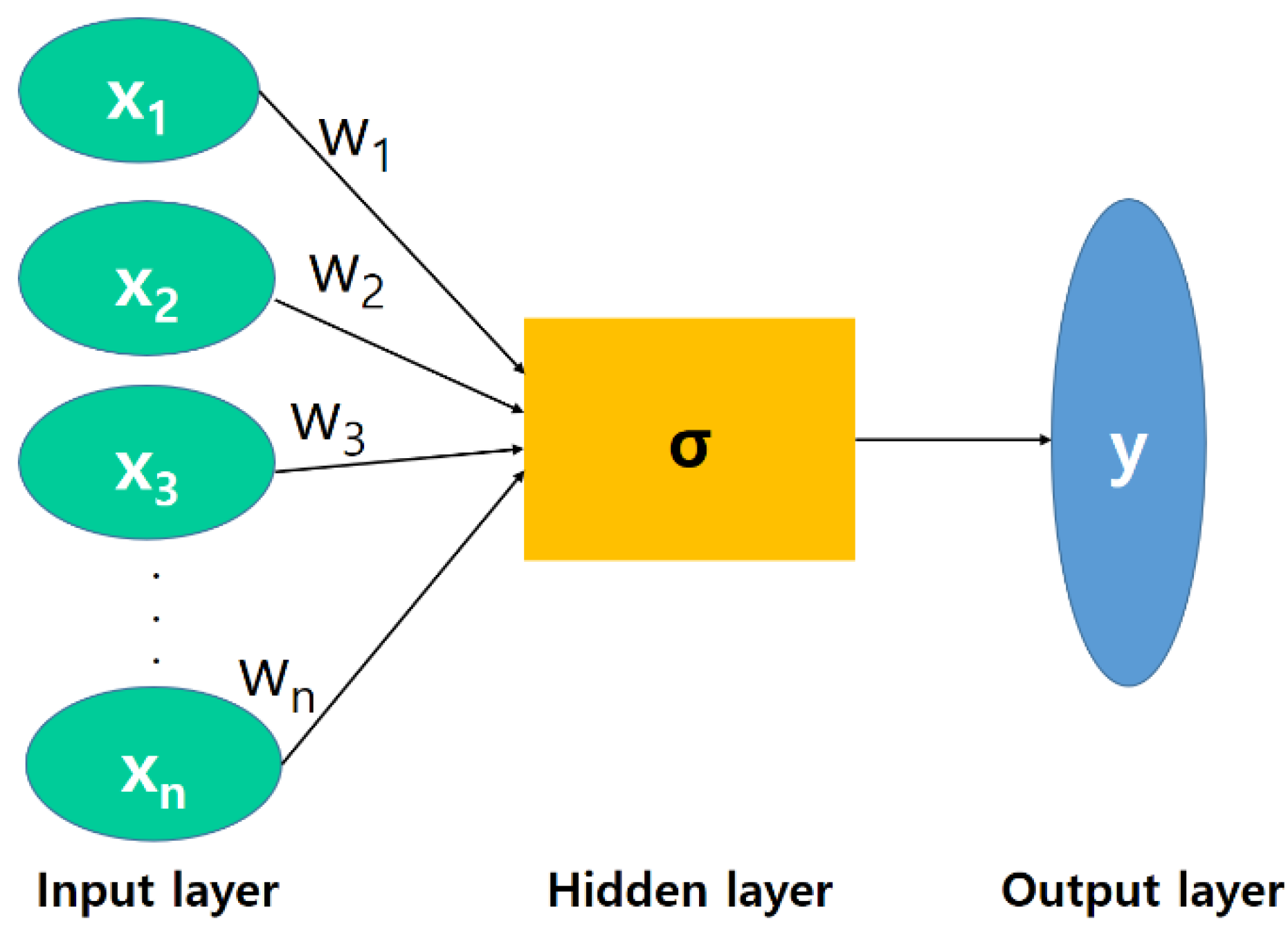
Figure 2 shows the basic structure of a neuron. Neurons adjust the weights of relevant features as they learn. The activation function (sigma) measures the strength of a neuron’s response. A data set, including a training set, a validation set, and a test set, is required to train and evaluate a neural network model for deep learning. Each model was trained and evaluated accordingly. Training and learning refer to fitting parameters, such as weights of connections between neurons in a neural network model. Typically, different epochs of training are attempted on different models using a training set. Here, different models mean a slight change in the hidden layer or hyperparameter. The fitted model was used to predict the feedback for a set of observations in the validation set. A validation set is a dataset that monitors model performance during training and validates an already trained model through fine-tuning parameters. A training set is a dataset used to evaluate the performance of a trained and validated model.
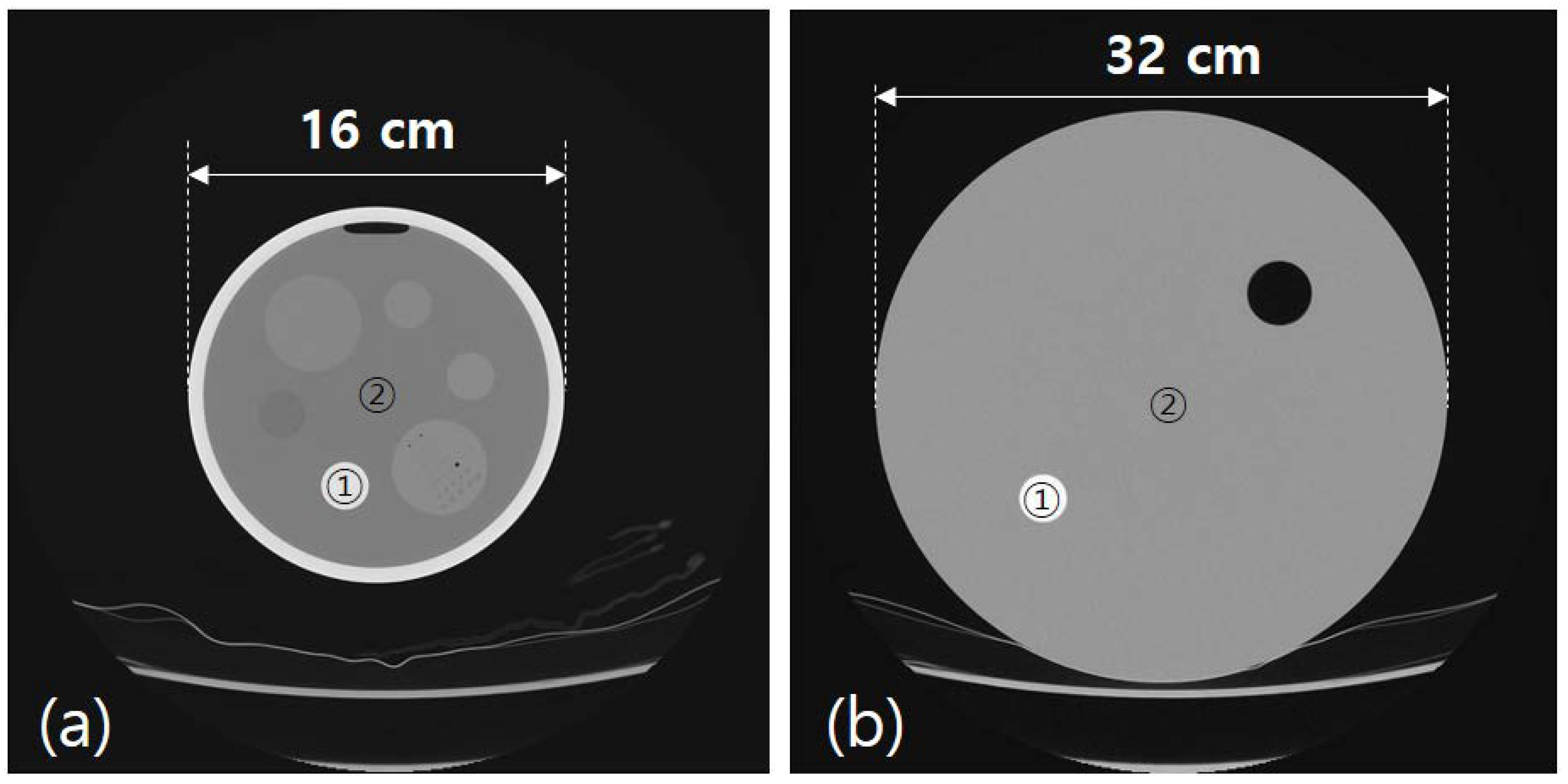
The pediatric and adult abdominal phantom images were obtained using CT (Aquilion ONE GENESIS, Canon medical systems, Japan). CT is a commercial product, and it has built-in software capable of reconstructing FBP, IR, and DLR with acquired projection images. The reconstruction speeds (in seconds) of FBP, IR, and DLR of the CT device used in this study are 15 s, 21 s, and 50 s, respectively, based on 1000 image slices. The CT had a 320 row × 0.5 mm detector element width. The phantom was exposed to X-rays in the form of a fan beam. The geometry of the detector facing the X-ray is symmetrical. The diameter of the phantom was 16 and 32 cm for children and adults body sizes, respectively, as shown in
Figure 3.
Table 1 shows the CT imaging conditions used in this study. The phantom was scanned with tube voltages at 80, 100, and 120 kV, and the radiation dose for each tube voltage was set to 0.5, 1.0, 2.0, 5.0, and 10.0, with mGy as CTDIvol. CTDIvol for the abdomen of children and adults was selected within a range not exceeding the diagnostic reference level (DRL) [
13]. According to the DRL, the CTDIvols for children and adults are 20 and 25 mGy, respectively. For all CT images, the image matrix was 512 × 512, and the slice thickness was 1 mm. The CT images were reconstructed with FBP, IR, and DLR.
Quantitative analysis of pediatric and adult phantom images was performed. We analyzed the contrast-to-noise ratio (CNR), which is the ratio of the estimated contrast and noise. The CNR is expressed as shown in Equation (1):
where S
s and S
b are pixel intensity for the signal and background material, respectively, in the region of interest (ROI). σ
s and σ
b are the standard deviation (SD) for the signal and background material, respectively, in the ROI. In the pediatric and adult phantoms shown in
Figure 2a,b, respectively, ① and ② denote the signal and background, respectively. CNR was calculated by substituting the mean value and SD value of the pixels of ① and ② into Equation (1).
4. Discussion
The need to maintain health is increasing, and the average lifespan of people is extending with the development of medical technology. The number of examinations using CT for the early diagnosis of disease has increased, and the radiation dose for patients has also increased significantly. Accordingly, CT scans for children are increasing, and children are more sensitive to radiation than adults, so it is necessary to reduce overexposure to children during CT scans. Prior to the early 2000s, there was little distinction between pediatric and adult patients, so radiation dose control and image quality control during CT scans were poor. CT acquisition skills during this period were rarely adjusted for body size. Early recommendations for radiation dose reduction emerged, from which interest in pediatric doses expanded worldwide [
15]. Advances in radiation awareness have come through education, hardware and software development, and available radiation dose indices. These advances stemmed from a collective desire among facilities, countries, and CT manufacturers to improve health care for all patients, especially pediatric patients undergoing CT [
15]. Therefore, this work studied the possibility of a dose reduction for a pediatric CT scan according to the tube voltage, CTDIvol, and reconstruction method. According to the results, DLR showed better results than FBP and IR in terms of CNR improvement and noise reduction.
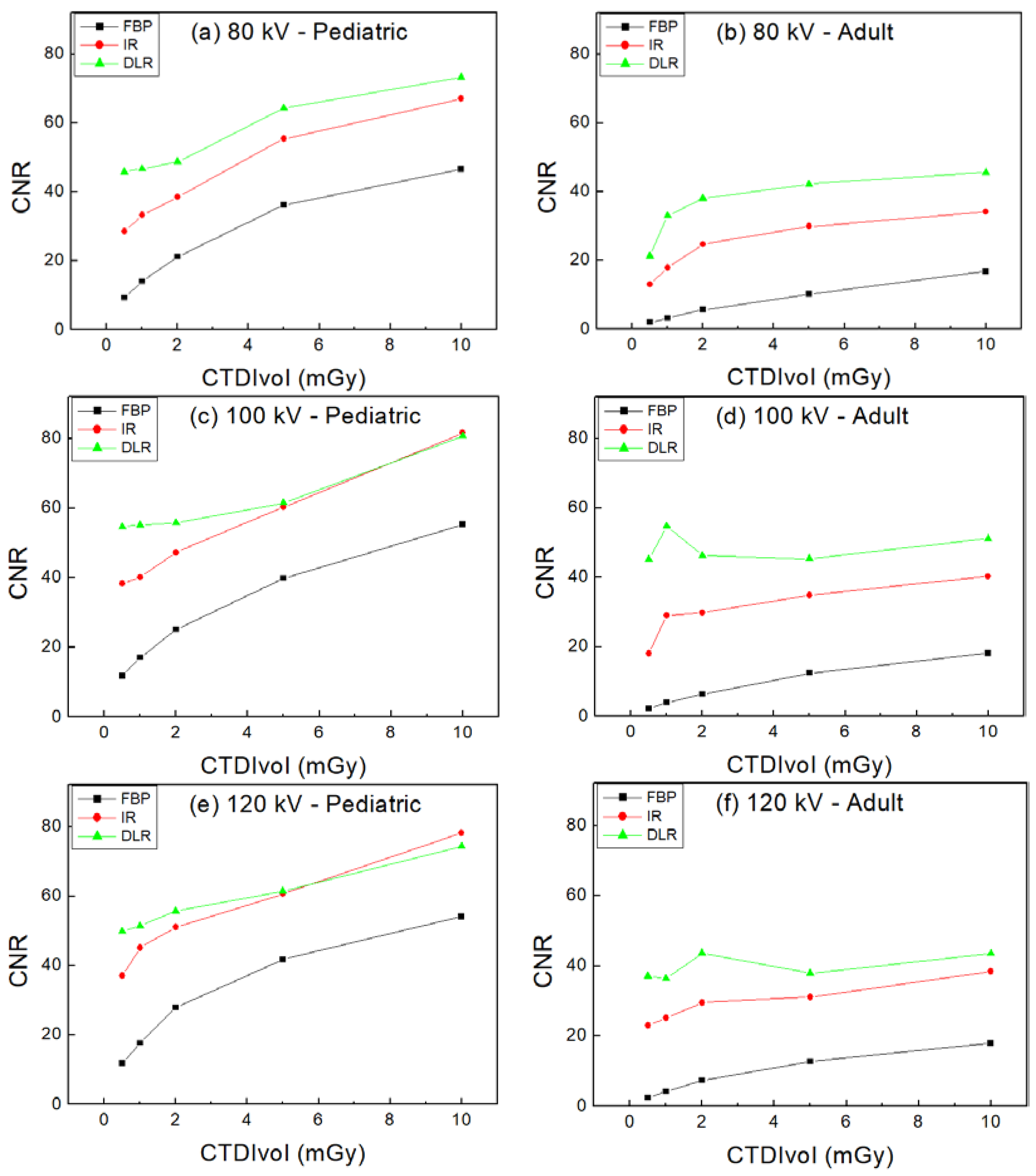
Regarding the effect of tube voltage, FBP generally increased the CNR of adult and pediatric images as the tube voltage increased. DLR showed the highest CNR in both adult and pediatric images at 100 kV. Usually, among the imaging parameters for CT imaging, a tube voltage of 120 kV is used. Since a radiation dose is approximately proportional to the square of the tube voltage, it is possible to reduce the radiation dose by using a low tube voltage. However, it has been reported that a low tube voltage of 80 kV causes the beam hardening of dense materials such as the intravascular contrast agents during CT imaging, resulting in significant image quality degradation [
16]. In our results, the 80 kV image resulted in CNR reduction and noise increase compared with the 100 and 120 kV images. On the other hand, 100 kV has a high attenuation difference between materials than 120 kV, resulting in increased image contrast. A study by Gill et al. found that the vessel-enhancing effect was higher at 100 kV than at 120 kV [
17]. The results of this study also demonstrated the CNR improvement of bone- and soft-tissue-equivalent materials at 100 kV, and CNR improvement is expected even in materials with a higher linear attenuation coefficient than bone, such as iodine contrast agents.
A study on contrast enhancement using DLR CT was also conducted. Ye et al. improved the accuracy and efficiency of chest intravenous contrast enhancement using a convolutional neural network (CNN) in CT scans [
18]. Our future study will include not only contrast enhancement but also studies on various tissue-equivalent-materials detection models.
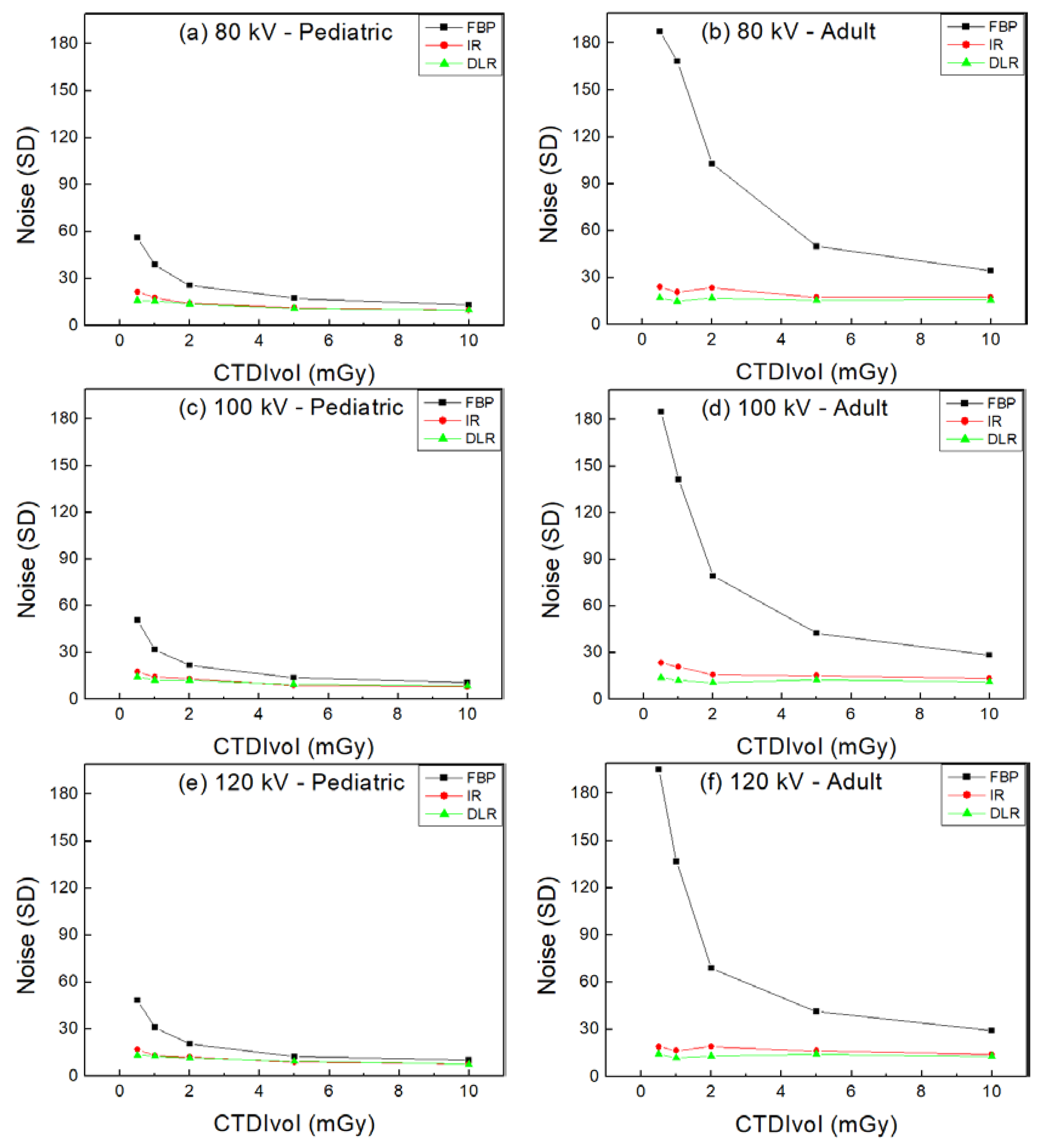
For noise evaluation, DLR generally showed a better reduction in noise than FBP and IR. Exceptionally, in pediatric images, when the tube voltages were 100 and 120 kV and the CTDIvols increased, the noise level of IR was almost similar to that of DLR. As the radiation dose increased, IR reduced noise more than DLR. This is because at a high radiation dose, IR has less noise in the high-frequency region [
19].
In this study, the CTDIvol ranged from 0.5 to 10 mGy. Eray Atlı et al. reported that the CTDIvol of an abdominal CT varies from 8.6 to 25 mGy [
20]. In South Korea, a CTDIvol of about 8.2 to 9.4 mGy is used for abdominal CT scans [
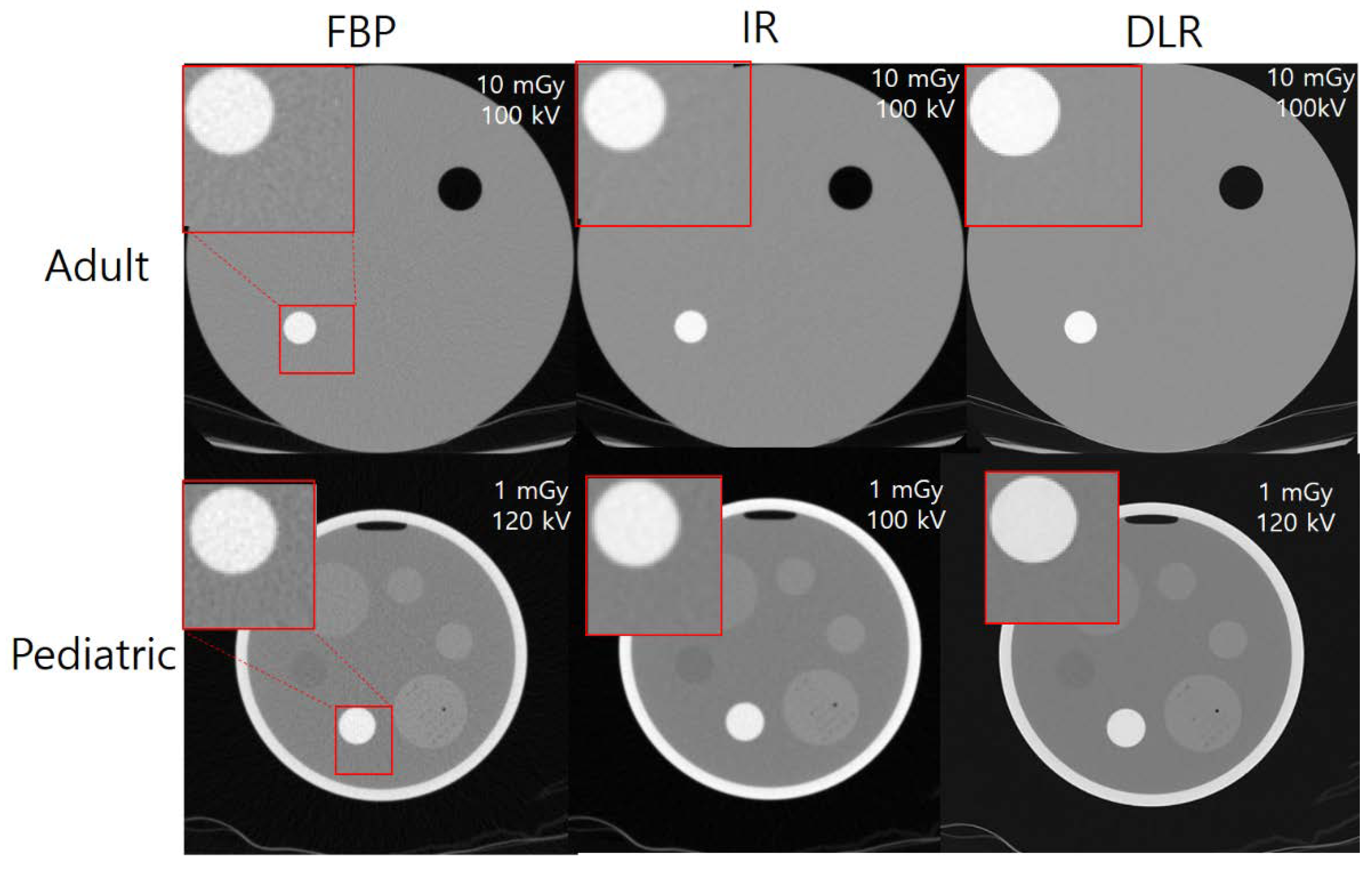
14]. Therefore, the CTDIvol range was set based on the abdominal CTDIvol, which is commonly used around the world and in South Korea for DRL. Overall, DLR provided a higher image quality at the same CTDIvol compared with FBP and IR. In this study, the standard protocol for an adult abdominal CT was a tube voltage of 120 kV, a CTDIvol of 10 mGy, and the reconstruction of FBP, and the measured CNR under these conditions was 17.99. The maximum CNR for DLR in the adult images was 51.16 at 100 kV and 10 mGy, and the CNR increased by 184.38% compared with the reference imaging conditions. In pediatric imaging, the maximum CNR for DLR was 80.67, a 348.42% CNR improvement over the reference imaging condition. The image quality of DLR increased in both the adult and pediatric images, which can be expected to reduce the radiation dose of DLR. This is because DLR distinguishes the noise from a CT image and enhances the signal, so that an improvement of image quality can be obtained by suppressing noise while enhancing the signal.
The relationship between image quality and object size was discovered by Siegel et al. [
21]. The results reported a decrease in noise and an increase in image contrast as the object size decreased. Since children have a smaller body size than adults, image quality can be improved at the same dose. Accordingly, a dose-reduction effect can be expected for children compared with adults at the same image quality.
Our study confirmed the potential of DLR to improve CT image quality and reduce radiation doses in children. Pediatric CT imaging with reconstruction methods such as FBP and IR may have limitations. In particular, compared with adults, children may obtain an excessive dose under the same imaging conditions. DLR-based pediatric imaging can produce excellent images due to noise reduction, contrast enhancement, and dose reduction. This would be a non-invasive imaging tool capable of safely diagnosing lesions in pediatric patients. Based on this, it will be able to play an important role in enabling the identification of pediatric diseases through artificial intelligence in the future.
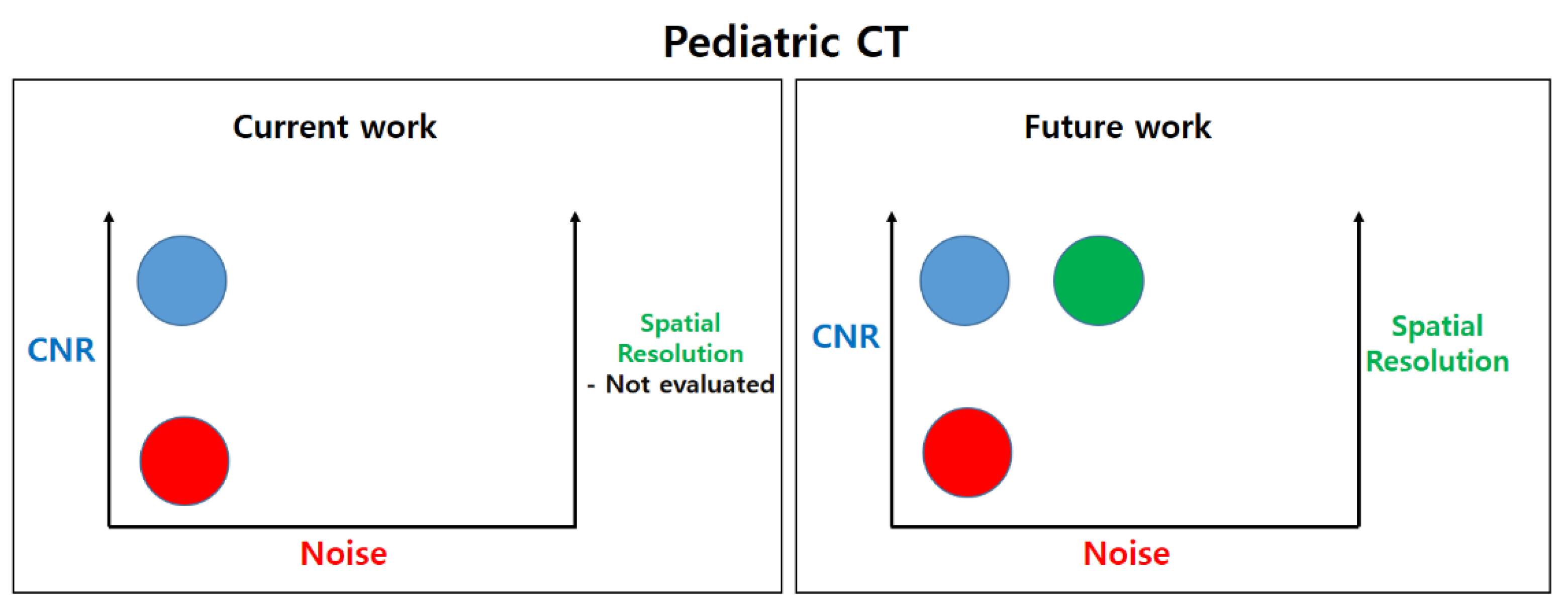
The architecture and hyperparameters of the DLR in this study used the CT manufacturer’s unique reconstruction method. In future work, we will develop a deep learning model for low-dose and high-definition CT (including spatial resolution) and conduct an optimization of the neural network, as shown in
Figure 7.
5. Conclusions
In the same reconstruction method, tube voltage, and radiation dose, the image quality of children was higher than that of adults. In pediatric abdominal CT scans, DLR generally showed higher image quality than FBP and IR at the same tube voltage and radiation dose. As for the effect of tube voltage, FBP and IR tended to increase image quality at 120 kV, but DLR increased image quality in children at 100 kV. According to the results, in pediatric CT, DLR is expected to not only reduce radiation dose to children more than FBP and IR, but also improve image quality. In addition, the tube voltage of 100 kV DLR can provide additional help in improving the image quality of DLR images in children. Therefore, DLR and 100 kV are expected to be applied for safe pediatric clinical image acquisition.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}