1. Introduction
Symmetry is defined as the mirror-image mathematical and geometrical identity between the right and left halves. Such mathematical and geometric symmetry is rare in living organisms. Facial symmetry refers to the harmonized balance and agreement between the right and left facial halves of the face in terms of size, shape, and arrangement. Facial asymmetry is considered a major factor in the perception of beauty and attractiveness. Asymmetries close to the midline are significantly less attractive than those affecting the lateral aspect of the face, indicating that the visual impact of symmetry on the perception of beauty increases considerably when approaching the facial midline [
1]. However, Swaddle and Cuthill indicated that totally symmetric faces are less attractive because of the reduction in natural directional asymmetries and unemotional appearance [
2]. Kowner indicated that a low degree of facial asymmetry in normal individuals does not affect their attractiveness rating [
3]. Thus, facial symmetry is an essential but not the only element affecting the perception of facial beauty. Overall, facial harmony with an appropriate facial proportion and satisfactory midline facial symmetry are vital factors with respect to attractiveness.
Facial asymmetry can result from congenital craniofacial anomalies, such as hemifacial microsomia, or acquired dentofacial deformities caused by facial development, trauma, and disease. Facial asymmetry can also result from abnormalities in the facial skeleton, muscles, and function. A differential diagnosis of these origins is essential for adequate correction [
4].
Orthodontists’ role in correcting facial asymmetry begins from the diagnosis of the condition and the identification of patients’ expectations. The selection of treatment modalities—orthodontic treatment alone or surgical orthodontics—depends on the severity of skeletal deviation and awareness and concerns regarding facial asymmetry. Before treatment initiation, orthodontists appropriately diagnose the condition and identify whether facial asymmetry is caused by skeletal, muscular, or functional abnormalities. In some borderline cases, skeletal asymmetry might be masked by dental crowding or spacing, sagittal jaw discrepancy, transverse dental compensation, or tilted head posture. Facial asymmetry can be revealed once the main problem is corrected. The aim of this clinical review is to provide information on surgical indications for facial asymmetry, optimal treatment goals, presurgical orthodontic preparation, the surgery-first approach, three-dimensional (3D) surgical simulation, postsurgical orthodontic finishing, and treatment outcome evaluation. Thus, a stepwise approach of meeting patients’ expectations and delineating clinical problems, as well as identifying optimal treatment solutions, are practical guides for correction of facial asymmetry.
2. Methods
2.1. Perception of Face and Dental Asymmetry
Most studies recommend diagnosis of facial asymmetry based on the amount of chin deviation 4 mm relative to the facial midline because most individuals, whether dental professionals or laymen, can notice a chin deviation of more than 4 mm [
5]. In terms of the three-dimensional (3D) dentoskeletal parameters correlated with the visual perception of facial asymmetry, a study identified that the midline parameter deviation, shape of the mandibular border, and the contour of menton morphology play major roles in the visual perception of postoperative asymmetry after Class III surgical correction [
6]. Meyer-Marcotty et al. reported that most individuals focus on the central part of the face and that significant midline asymmetry can be detected even by laymen [
7]. Lee et al. reported factors considered by orthodontists to subjectively identify patients with facial asymmetry requiring surgical treatment. Lip cant, chin deviation, and differences in body inclination and the gonial angle between the two sides of the lower jaw were identified as main factors affecting the decision to perform surgery [
8].
The level of the occlusal plane is a prerequisite for the success of all orthognathic surgical procedures [
9]. The occlusal plane cant in the frontal plane can be evaluated using posteroanterior (PA) cephalograms. Padwa et al. indicated that an occlusal cant of >4° can be recognized in more than 90% patients by both untrained and trained observers [
10]. Thus, apart from the extent of the deviation of the midline structure and bilateral contour difference, evaluation of the occlusal plane cant is crucial for deciding on surgical treatment for facial asymmetry. The occlusal plane and lip cant can be corrected through asymmetric maxillary posterior impaction or posterior impaction and extrusion on different sides. In a study by Lin et al., the occlusal plane and lip cant were observed to be undercorrected 1 year following asymmetric maxillary posterior impaction [
11].
In terms of intraoral parameters, asymmetric bilateral angle molar occlusion, dental midline deviation, and transverse discrepancy in posterior teeth can provide some information on the extent of skeletal asymmetry. Further analysis of facial asymmetry is required if patients present with the aforementioned intraoral malocclusion.
2.2. Subjective Clinical Evaluation of Dentofacial Asymmetry
Facial asymmetry can be evaluated by examining the soft tissue, dental manifestations, and the 3D facial skeleton. Complete initial dental records are required. Facial photos should contain frontal and bilateral profile views with reposed lip and smile postures. Intraoral photos and dental casts with a centric occlusion bite provide information on dental occlusion and arch coordination. The size, shape, and orientation of the overall cranium can be determined using PA and lateral cephalograms. Cone beam computed tomography (CBCT), which involves the use of a relatively low radiation dosage (0.1~0.3 µSv), is typically usually used for surgical simulation or diagnosis of complex dental and skeletal problems.
Table 1 lists the overall 3D evaluations of dentofacial deformities.
A dynamic assessment of the smile is essential. In a previous study, 41% of patients presented with a canted maxillary occlusal plane, which indicates vertical asymmetry [
12]. However, in another study, after the exclusion of patients with occlusal plane cants, 8.7% of patients were observed to have an asymmetric smile secondary to the canting of the upper lip [
13]. Differential diagnoses of hard tissue abnormalities, asymmetric perioral musculature, or imbalanced upper lip activity are required for the dynamic assessment of an asymmetric smile.
2.3. Surgical Orthodontic Management of Facial Asymmetry
2.3.1. Surgical Indication
Patients with facial asymmetry usually exhibit some vertical and sagittal discrepancies. Problems typically occur in two jaws rather than one jaw. Overall consideration of the expectations of patients and the limitations of orthodontic treatment and surgical management can lead to an optimal final decision regarding treatment. Indications for surgical correction are as follow.
- (1)
Asymmetric dentofacial deformities of skeletal Class II, III, or open bites that already require surgical correction;
- (2)
Visible mandibular deviation > 4 mm combined with asymmetric buccal occlusion and midline deviation that cannot be corrected by orthodontic treatment alone;
- (3)
A major occlusal plane cant > 4° with a vertical discrepancy or an asymmetric tooth that cannot be corrected by orthodontic treatment alone;
- (4)
Major asymmetric mandibular contour with maxillomandibular lateral shifting;
- (5)
Inability of previous orthodontic treatment alone to meet patients’ expectations regarding facial correction;
- (6)
Facial trauma and pathologic lesions of the mandible or condyles; and
- (7)
Congenital craniofacial anomalies associated with facial asymmetry.
2.3.2. Treatment Goal of Orthognathic Intervention
Surgical orthodontics mainly involves the alignment of the maxilla and mandible and the treatment of dental occlusion, although overall facial symmetry might still present in the soft tissue and other facial organs, such as eyes and nose.
Skeletal alignment in the PA view relates to roll and transverse correction and involves the following steps [
14]:
- (1)
Leveling the maxillary occlusal plane to maintain it parallel to the orbital plane;
- (2)
Placing the maxillary dental midline such that it is correlated with the facial midline;
- (3)
Correcting the maxillary anterior dental axis and ensuring that it is parallel to the facial midline; and
- (4)
Placing the chin center along the facial midline.
Correction of the jaw, especially the bilateral mandibular contour symmetry, can be performed through 3D evaluation and simulation by implementing the following steps [
15]:
- (1)
Placing the maxilla in the center position relative to that of the cranial base;
- (2)
Placing the chin in the center and ensuring bilateral symmetric mandibular body alignment; and
- (3)
Adjusting the bilateral symmetric alignment of the gonial and ramus in their counterpart positions.
Vertical skeletal alignment related to the facial height and upper tooth is required under the following conditions:
- (1)
The static upper tooth relative to the upper lip is approximately 2 to 4.5 mm in women and 1 to 3 mm in men [
16];
- (2)
The upper teeth visible in the posed smile exhibit a full crown or 1 to 2 mm gum with a consonant smile arc [
17]; and
- (3)
The ratio of the upper-to-lower anterior facial height is approximately 0.90 in women and 0.82 in men [
18].
The sagittal position of the maxilla and mandible can be evaluated using McNamara’s cephalometric analysis. The A point and pogonion point to the nasion perpendicular (NP) line to the Frankfort horizontal (FH) plane can be readily applied for 3D analysis. The A point to the NP line is −0.53 ± 4.62 for women and −0.02 ± 4.21 for men; the pogonion to the NP line is −6.65 ± 9.55 for women and −2.49 ± 9.01 for men in the southern Chinese population [
19]. The inclination of the upper incisor, which can be evaluated using the sella-nasion to upper incisor angulation, is 108.68° ± 6.45° for women and 108.9° ± 5.52° for men [
20].
2.3.3. Presurgical Orthodontic Preparation
Manipulation of the initial dental model with trial surgical occlusion can provide information on how presurgical orthodontic treatment should be conducted. The goal of presurgical orthodontics is to remove dental interferences for anterior tooth contact with appropriate overbite and overjet, as well as to maintain lateral side shifting to the nondeviated side. For patients with severe crowding, dental extraction might be required for initial dental leveling before surgery. For patients with transverse dental arch incompatibility that cannot be corrected by orthodontic treatment alone, a 1 to 1.5 mm space should be prepared for an interdental cut of segmental osteotomies in the nonextraction arch. Six months are typically required for presurgical orthodontic leveling. Dental compensation for facial asymmetry is not necessarily corrected presurgically. The molar torque can be decompensated more efficiently after surgery.
Four weeks before surgery, presurgical records are obtained, including photographs, CBCT images, 3D facial scans, cephalometric radiographs, and digital dental models. By integrating all the 3D images of the soft tissue, skeleton, and dentition, a 3D composite craniofacial model is constructed for surgical simulation. Steps involved in 3D surgical simulation are as follow:
- (1)
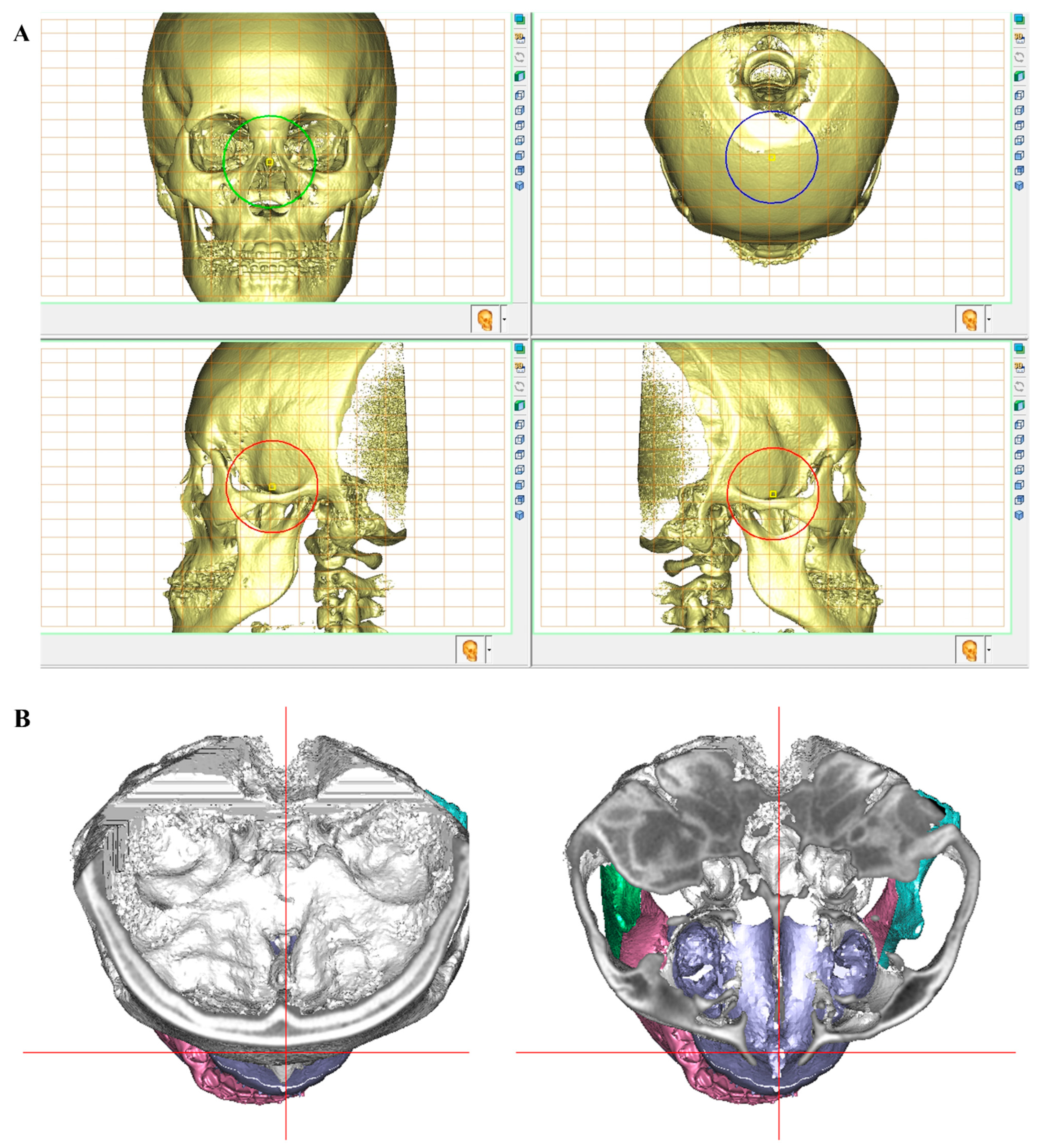
Orient the 3D composite craniofacial model to an appropriate head posture (
Figure 1). In the sagittal view, the FH plane is parallel to the floor. In the frontal view, the face is upright with an even eye level and a straight nose axis. If the eyes are not even or the nose is crooked, the head posture is further adjusted in the software according to a facial photograph or manipulated by doctors. In the axial view, the supraorbital and infraorbital contours should be symmetrically projected. The mid-sagittal plane (MSP) should also bisect the cranial base in the axial view.
- (2)
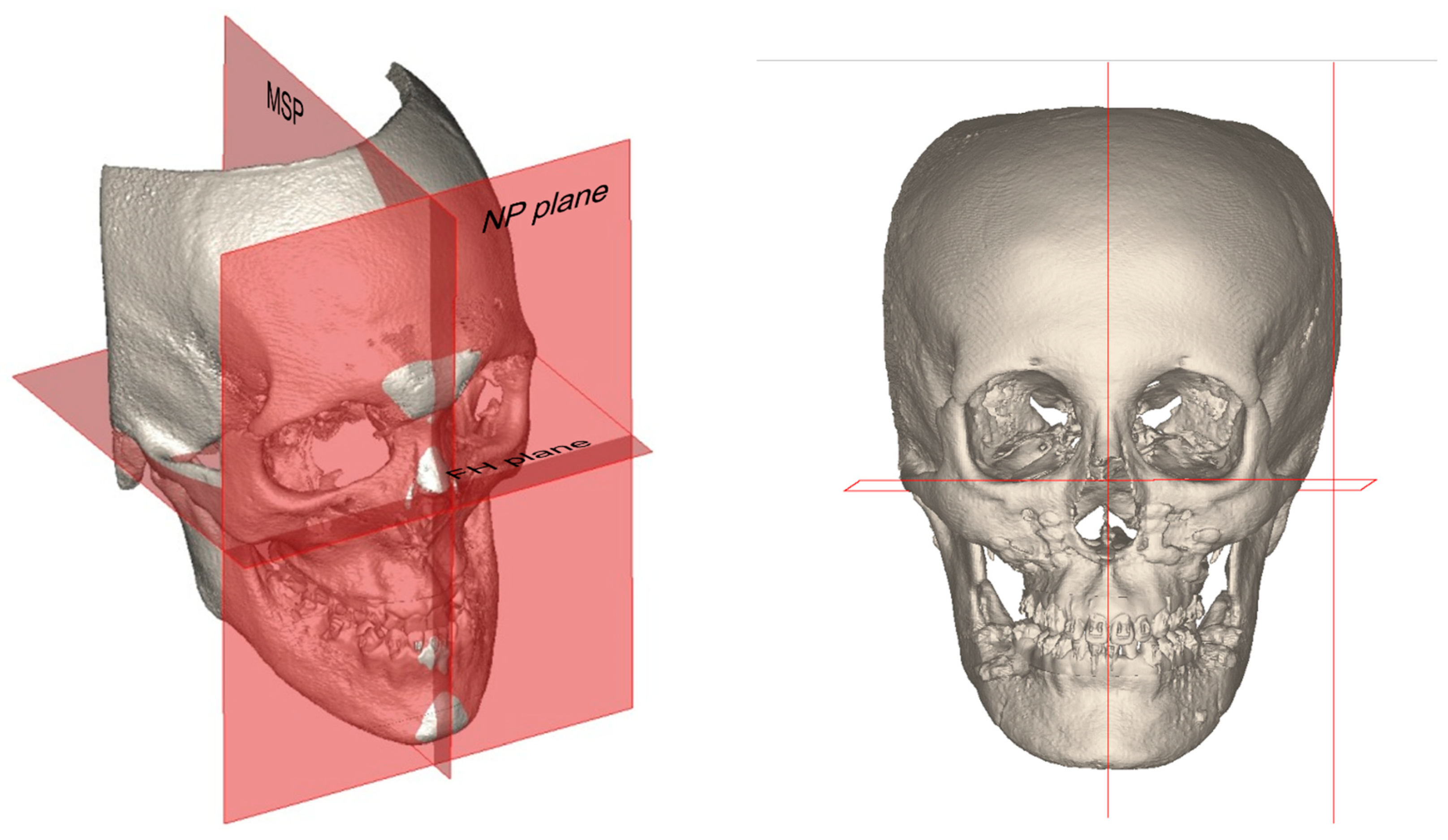
Determine all 3D landmarks, lines, and planes. Three reference planes are chosen for surgical simulation (
Figure 2). The FH plane is defined as connecting the bilateral orbitales and the middle point of the bilateral portions. The MSP is defined as the plane parallel to the patient’s true sagittal plane and passing through the nasion. The NP plane is defined as the plane passing through the nasion and perpendicular to the MSP. If the bilateral orbital level is not at an even height, the FH plane and MSP might not be perpendicular to one another.
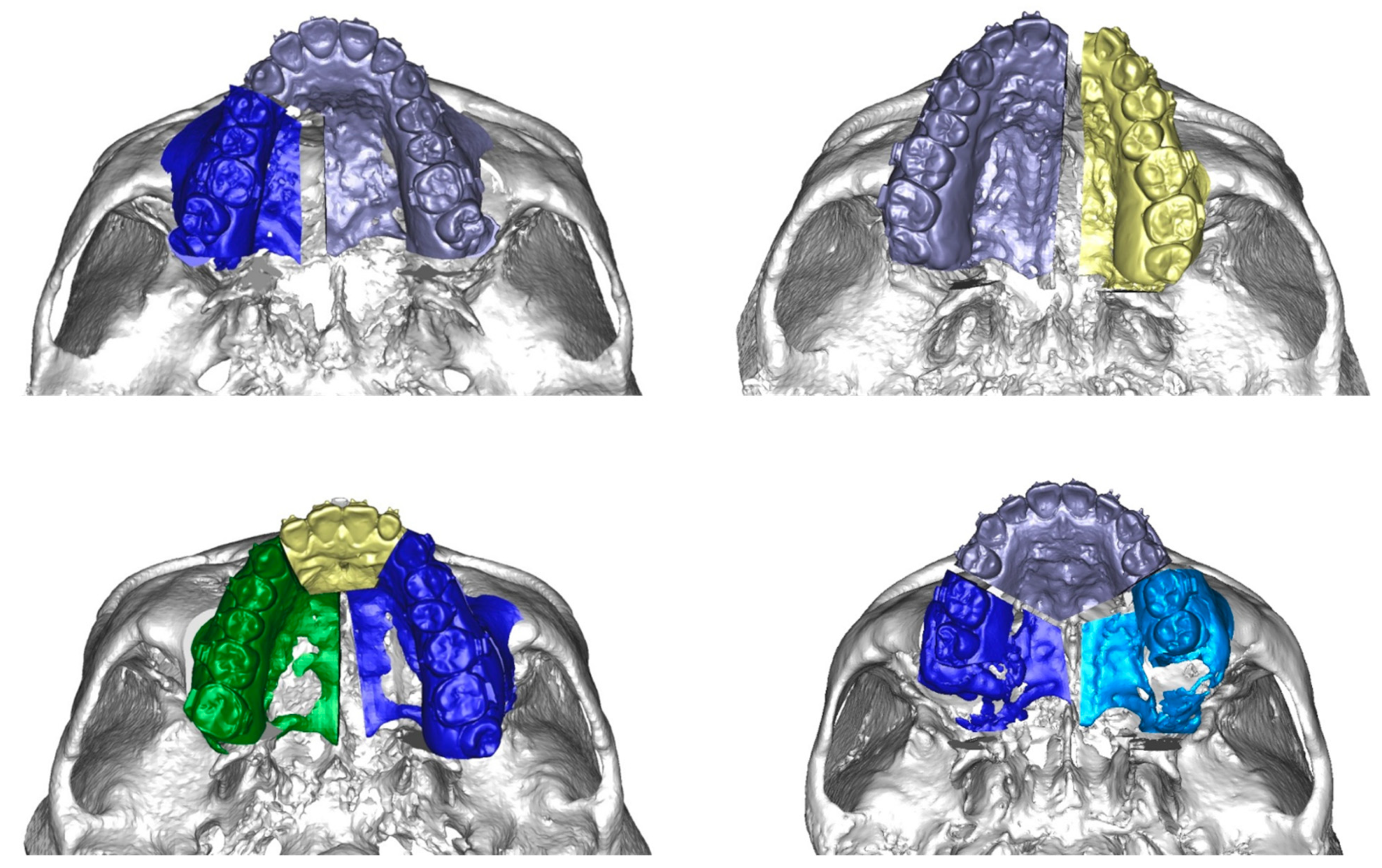
- (3)
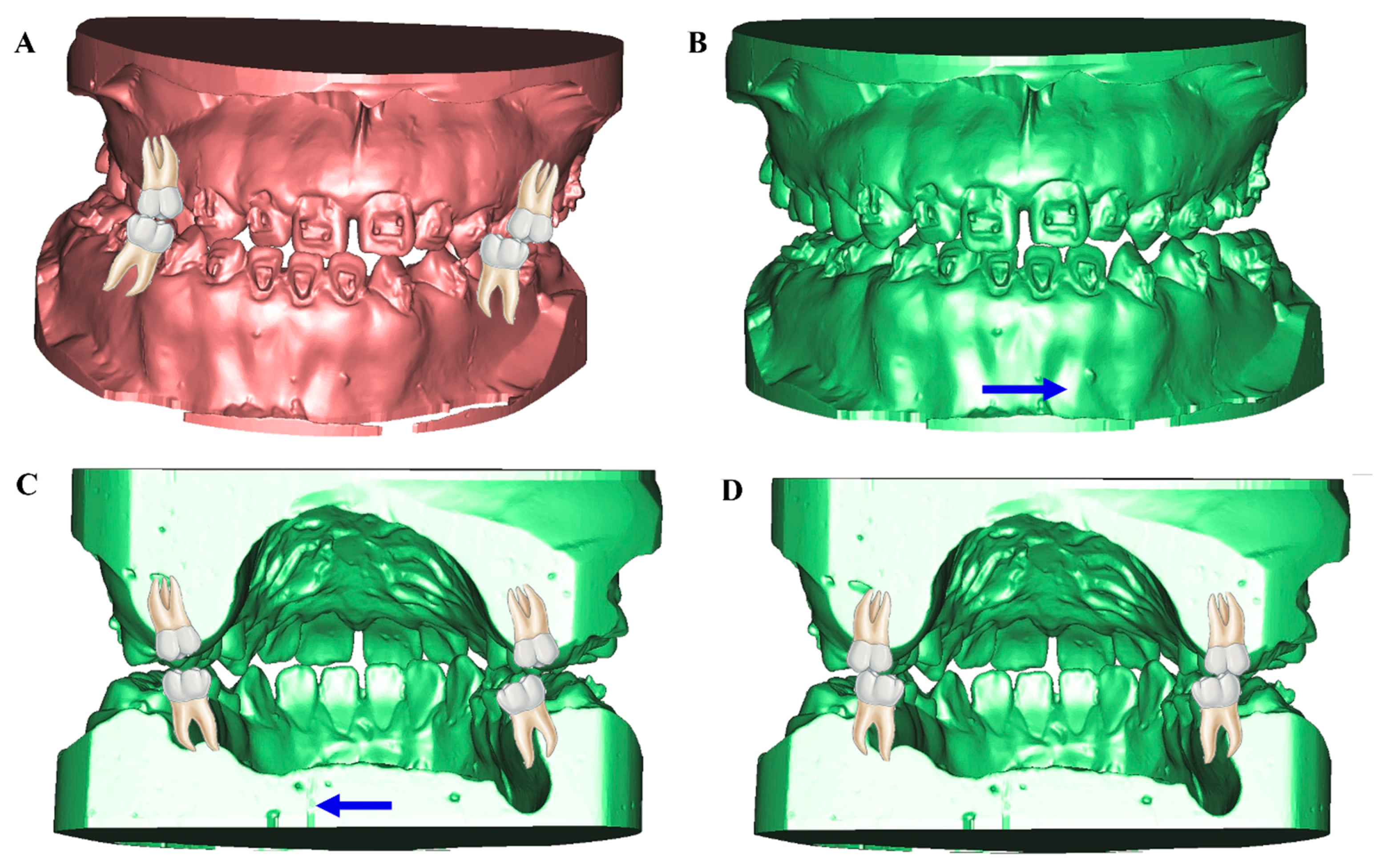
Perform osteotomies by using craniofacial models, such as LeFort I (with or without segmentation), bilateral sagittal split, and genioplasty. Surgery is performed for a treatable dental occlusion setup that links the osteotomized maxilla and mandible. The osteotomized maxilla and mandible with the set-up surgical occlusion form the maxilla–mandibular complex (MMC). Versatile maxillary segmental osteotomy can be performed to adjust the width and alignment of the maxillary dental arch, such as a midline split and three-piece adjustment for the bilateral arch or two-piece adjustment for the unilateral arch (
Figure 3).
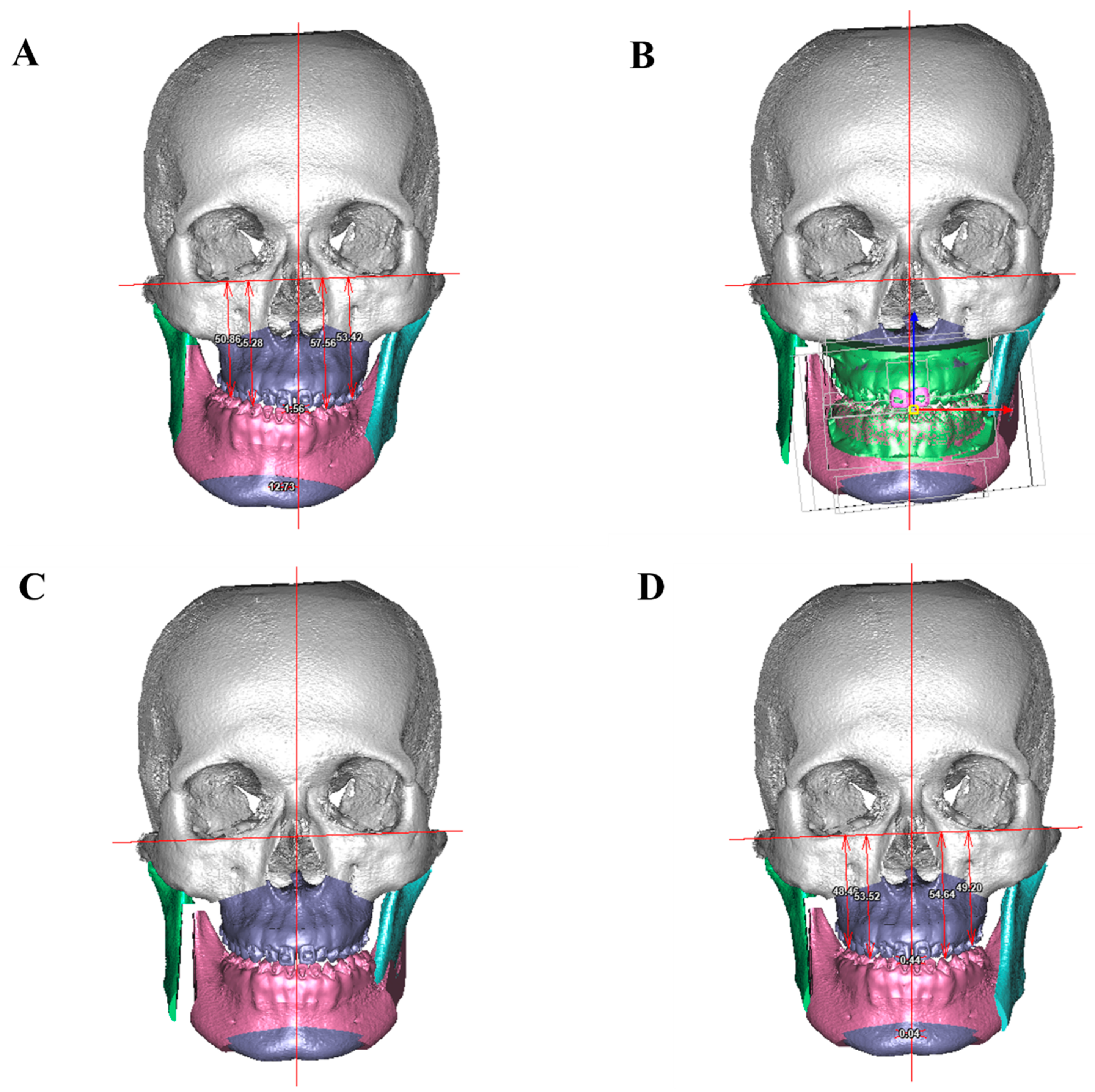
- (4)
Conduct surgical simulation by moving the MMC. The sequence starts with dental midline coordination with MSP, roll correction, yaw rotation, vertical movement, sagittal movement, and pitch correction. After moving the MMC, genioplasty and adaptation of the proximal segment are performed for chin projection and gonial/ramus contour symmetry (
Figure 4).
- (5)
Examine 3D facial morphing after surgical simulation of the jawbone. Check the proportion, harmonization, and symmetry in all planes. The final 3D images can be used for surgical stent fabrication with 3D printing. The sequence of surgery (maxilla first or mandible first) can be decided according to the status of the mandible opening during intermediate stent fabrication and the type of mandible movement (forward or backward) [
21].
2.3.4. Surgery-First Approach to Facial Asymmetry
Dental compensation for facial asymmetry usually involves molars with torque following the deviation of the jawbone [
22]. The molars might not be appropriately decompensated before surgery due to locking by the crossbite in an adaptational interdigitation. If no dental interference occurs during anterior dentition or lateral side shifting, most cases can be managed using the surgery-first approach (SFA).
The surgical occlusion setup should be based on the relationship of the basal bones with fair sagittal and transverse position instead of the maximum occlusal surface contact (
Figure 5). When the lower arch occludes the upper arch based on the relationship with the basal bone, the buccal overjet is smaller on the non-deviated side and larger on the deviated side. A setup with increased buccal overjet on the deviated side is necessary due to buccal inclination in the maxillary molars and lingual inclination in the mandibular molars in the compensation occlusion. By leaving some posterior open contact in surgical occlusion, the molars can be uprighted by using the occlusal space after surgery. A surgical occlusion setup with a posterior open bite of 3 to 4 mm can be extruded after surgery without impairing postsurgical stability in skeletal Class III deformities [
23]. A similar approach can be applied to set up upper and dental midline coordination by aligning the apical root portion instead of the incisal edge because tilted dental compensation usually occurs in facial asymmetry.
2.3.5. Postsurgical Orthodontic Finishing
In the first week after surgery, overall facial and occlusal evaluations and radiographic examination are performed to evaluate the symmetry and facial profile of the following factors with preoperative surgically simulated parameters:
Overall facial soft tissue swelling and localized infection;
Oral commissure leveling and chin and gonial contour symmetry;
General outcomes of facial proportion and profile;
Upper dental midline coordination with facial midline with appropriate tooth visibility;
Intraoral proper overbite, overjet, general arch coordination, and dental midline.
If maxillary three-piece adjustment with expansion is performed, the surgical stent needs to be retained in the maxillary arch for 4 weeks to ensure transverse maxillary arch stability. Light intermaxillary elastics are applied to guide occlusion if dental deviation occurs.
One month after surgery, radiographic examination is performed to examine bone healing and initial changes. Open-mouth rehabilitation is performed to gradually restore oral function [
24,
25]. The two-dimensional and 3D photos are obtained to document facial changes.
Active orthodontic treatment is performed after an acceptable range of mouth opening is achieved, including leveling to the distal molars, proper overbite and overjet, transverse coordination, solid interdigitation to the Class I canine, and molar relationship. Torque enhancement is more efficient after the correction of skeletal asymmetry, especially in the SFA (
Figure 6). On the deviated side, the previous surgical occlusion setup with increased buccal overjet can be solved by lingual crown torque in the upper molars and buccal crown torque in the lower molars. On the non-deviated side, the upper molar should have buccal crown torque, and the lower molar should have lingual crown torque. After the molar torques are appropriately managed, the dental midline can be readily corrected with short-term intermaxillary elastics.
A fixed retainer can be used for stable anterior alignment. Removable retainers (Hawley or wraparound) can be used to maintain transverse arch stability.
2.3.6. Treatment Outcome Evaluation
Soft tissue: The level of oral commissure, position of chin center relative to the face, facial contour, and symmetric bilateral tooth visibility and upper midline coordination during smile are evaluated.
Skeletal: Initial outcomes can be examined through CBCT and radiography. The accuracy of treatment can be detected through the superimposition of the short-term CBCT and 3D simulation plan [
26]. Long-term stability can be determined through the registration of CBCT within 1 week and at the time of orthodontic bracket removal.
Dental occlusion and alignment: Solid occlusal contact with the molar teeth, normal overbite and overjet, proper molar toque, and Class I buccal interdigitation with transverse stability are examined.
3. Discussion
3.1. Determination of Facial Midline in Facial Asymmetry
Facial asymmetry is a complex 3D deformity that manifests itself as size, morphology, and directional deviation of bilateral facial structures. The MSP is commonly used as a reference plane to compare and measure the difference of both sides of the face. Huang et al. proposed the use of soft tissue nasion that bisects the line connecting the bilateral exocanthion to analyze the facial asymmetric index [
27]. If possible, the MSP should be determined to link the facial soft tissue and skeletal structure for accurate and feasible clinical evaluation [
28]. Zheng et al. compared the closeness of two skeletal MSPs with soft tissue facial midline evaluation and indicated that the discrepancy between soft- and hard-tissue MSP in the orbital margin plane group was smaller than that in the skull base group [
29]. The orbits could be used as reference for midline determination. Dobai et al. used a landmark-based MSP by connecting the nasion–ANS (anterior nasal spine)–PNS (posterior nasal spline) to analyze facial asymmetry and asymmetry [
30]. It is clear and simple to identify the MSP. However, the maxilla could exhibit compensatory deviation toward the side of chin deviation. The MSP could underestimate the facial asymmetry caused by the deviation of ANS and PNS.
In our method, the MSP is defined as the plane parallel to the patient’s true sagittal plane (based on adjusted head orientation) and passing through the nasion. For patients with fair upper facial symmetry and level orbital rims, the MSP and the FH plane could be perpendicular to one another. For patients with uneven orbital height, if the MSP is determined by connecting the nasion perpendicular to the FH plane, it could not represent the true midline for facial analysis. Furthermore, doubly check two elements before conducting 3D surgical simulation: whether the MSP could bisect the anterior cranium base for patients with normal cranial form and whether the clinical upper dental midline deviation to the facial midline is similar to the computerized constructed MSP.
Landmark identification errors and improper head orientation could cause problems in MSP identification. The advanced application of an optimization algorithm [
31] or neural network deep learning [
32] could generate a more reliable MSP. Jajoo et al. developed a landmark-based algorithm to automatically calculate the MSP by detecting the least asymmetric regions of the face and computing the MSP [
31], which could represent the future trend toward a more subjective determination of facial MSP.
3.2. Surgery-First or Orthodontic-First Approach
Dental compensation occurs in most dentofacial deformities, including facial asymmetry. An appropriate surgical dental occlusion setup is required if the surgical movement is guided by dental occlusion alone, usually in one-jaw surgery. The “orthodontic-first” concept emphasizes the removal of all the dental compensation, interocclusal interference, and dental arch coordination prior to surgery [
33]. The orthodontic-first approach has been standard procedure for surgical orthodontic treatment (i.e., presurgical orthodontic phase, surgical phase, and postsurgical orthodontic finish) since the 1970s. The presurgical orthodontic phase is complicated and time-consuming. The development and application of 3D medical images and surgical simulation ensures an efficient and predictable two-jaw orthognathic surgery [
34]. Advances in osteotomy techniques and rigid internal fixation ensure a reliable and relative stable surgical outcome. In addition, postsurgical orthodontic treatment can be twofold accelerated by taking advantage of healing tissue reactions, called the “reginal accelerated phenomenon” [
35]. Thus, the paradigm shifted from an orthodontic-first approach to SFA [
36].
Most studies related to SFA involve skeletal Class III malocclusion. Few related studies have focused on issues associated with facial asymmetry [
37,
38]. Choi compared the SFA and traditional approach in cases that were classified as horizontal and vertical asymmetry and indicated a similar degree of asymmetry correction and skeletal stability in both methods [
37]. Similar treatment outcomes and stability of the surgery-first and orthodontic-first approach were reported by the same team by using artificial-intelligence-based cephalometric analysis [
38]. Most concerns related to facial asymmetry correction involve transverse discrepancy and dental interference caused by dental compensation. Surgical modification by maxillary segmental osteotomy, proper surgical occlusal setup, and two-jaw 3D correction could solve the major problems. Presurgical dental alignment might still be required if there are problems in determining the amount of dental midline deviation and discrepancy.
3.3. Improving Treatment Outcomes in Facial Asymmetry
Overall, comprehensive outside-to-inside and static-to-dynamic evaluations are necessary. Patients requiring optimal presurgical orthodontic treatment with the SFA should be identified to improve treatment efficacy. Multipiece osteotomies can be performed to improve arch incompatibility, close dental spaces, and partially correct the torque in molars.
A 3D-printed intermediate stent should be used to guide the sequence of two-jaw surgeries. Some surgical indicators can be integrated into the intermediate stent [
39]. The final stent should be appropriately designed by an orthodontist by considering problems related to postsurgical orthodontic finishing.
The relapse rate of skeletal Class III occlusion is 11% [
40]. Thus, slight overcorrection might be required to achieve a long-term favorable outcome for facial asymmetry correction.
The techniques of surgeons should be well-documented and recorded. Periodic feedback to surgeons regarding surgical accuracy and postoperative problems can help to improve overall surgical outcomes and stability.
Orthognathic surgery is performed only for correction of the lower face. Some of the upper face and cranial base deviations, mismatched vertical eye levels, and crooked noses can pose problems in facial midline identification. Any unusual condition occurring after a 3D simulation should be reported to patients and surgeons; this can help them determine the limitations of surgery in terms of residual facial asymmetry. Types of mandibular asymmetry regarding the ramus discrepancy should be addressed, as they can result in different surgical outcomes with respect to mandibular contour symmetry [
41]. Some cosmetic enhancement, such as autologous fat tissue transfer [
42], bone contouring, or revision surgery, can be performed to achieve improved symmetric outcomes.
Patients’ expectations should be determined before treatment to decide on the optimal treatment modality. Carefully understanding patients’ needs and obtaining feedback from patients after surgery can help surgeons and orthodontists improve the care and outcome of patients requiring facial asymmetry correction.
4. Conclusions
The diagnosis of facial and dental symmetry requires the careful detection of problems through the evaluation of the 3D skeleton. On the basis of patients’ expectations regarding treatment outcomes, surgeons can select optimal treatment modalities to correct soft tissue and skeletal abnormalities and dental occlusion. In a surgical occlusal setup, aligning the maxillary–mandibular basal bone relationship instead of the occlusal contact can facilitate more complete correction because transverse dental compensation might mask the amount of overall correction. Moreover, the torque in molar transverse compensation can be corrected more efficiently after surgery. Multiple segmental osteotomies can be performed to alter the arch form and improve transverse dental compatibility and occlusion. A 3D surgical simulation is required to provide a forecast of treatment outcomes and treatment limitations.
Author Contributions
Conceptualization, E.W.-C.K., C.S.H.; methodology, E.W.-C.K., C.S.H.; validation, C.S.H., C.-H.L., Y.-R.C.; investigation, E.W.-C.K., C.-H.L.; resources, C.S.H., Y.-R.C.; writing—original, E.W.-C.K.; draft preparation, E.W.-C.K., C.S.H., C.-H.L., Y.-R.C.; visualization, E.W.-C.K.; supervision, C.-H.L., Y.-R.C.; funding acquisition, E.W.-C.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This review was approved by the Institutional Review Board and Medical Ethics Committee at Chang Gung Memorial Hospital (IRB no. 202201004B0).
Informed Consent Statement
The IRB approves the waiver of the participants’ consent because it is expedited review according to case research or cases treated or diagnosed by clinical routines.
Data Availability Statement
Not applicable.
Acknowledgments
We acknowledge the support of the Craniofacial Research Center, Chang Gung Memorial Hospital, Linkou, Taiwan.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Springer, I.N.; Wannicke, B.; Warnke, P.H.; Zernial, O.; Wiltfang, J.; Russo, P.A.; Terheyden, H.; Reinhardt, A.; Wolfart, S. Facial attractiveness: Visual impact of symmetry increases significantly toward the midline. Ann. Plast. Surg. 2007, 59, 156–162. [Google Scholar] [PubMed]
- Swaddle, J.P.; Cuthill, I.C. Asymmetry and human facial attractiveness: Symmetry may not always be beautiful. Proc. R. Soc. B Boil. Sci. 1995, 261, 111–116. [Google Scholar]
- Kowner, R. Facial asymmetry and attractiveness judgment in developmental perspective. J. Exp. Psychol. Hum. Percept. Perform. 1996, 22, 662–675. [Google Scholar]
- Cheong, Y.W.; Lo, L.J. Facail asymmetry: Etiology, evaluation and management. Chang Gung Med. J. 2011, 34, 341–351. [Google Scholar] [PubMed]
- van Keulen, C.; Marten, G.; Dermaut, L. Unilateral posterior crossbite and chin deviation: Is there a correlation? Eur. J. Orthod. 2004, 26, 283–288. [Google Scholar]
- Lin, C.-W.; Wang, Y.-C.; Chen, Y.-H.; Ko, E.-C. Dentoskeletal parameters related to visual perception of facial asymmetry in patients with skeletal class III malocclusion after orthognathic surgery. Int. J. Oral Maxillofac. Surg. 2018, 47, 48–56. [Google Scholar]
- Meyer-Marcotty, P.; Stellzig-Eisenhauer, A.; Bareis, U.; Hartmann, J.; Kochel, J. Three-dimensional perception of facial asymmetry. Eur. J. Orthod. 2011, 33, 647–653. [Google Scholar] [CrossRef]
- Lee, M.-S.; Chung, D.H.; Lee, J.-W.; Cha, K.-S. Assessing soft-tissue characteristics of facial asymmetry with photographs. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 23–31. [Google Scholar]
- Polley, J.W.; Figueroa, A.; Cohen, M. Leveling of the occlusal plane during model surgery. J. Craniofac. Surg. 1993, 4, 266–267. [Google Scholar]
- Padwa, B.L.; O Kaiser, M.; Kaban, L.B. Occlusal cant in the frontal plane as a reflection of facial asymmetry. J. Oral Maxillofac. Surg. 1997, 55, 811–816. [Google Scholar]
- Lin, C.-L.; Chen, Y.-A.; Yao, C.-F.; Chang, C.-S.; Liao, Y.-F.; Chen, Y.-R. Comparative stability and outcomes of two surgical approaches for correction of class III asymmetry with lip or occlusal cant. Clin. Oral Investig. 2021, 25, 5449–5462. [Google Scholar] [CrossRef] [PubMed]
- Severt, T.R.; Proffit, W.R. The prevalence of facial asymmetry in the dentofacial deformities population at the University of North Carolina. Int. J. Adult Orthod. Orthognath. Surg. 1997, 12, 171–176. [Google Scholar]
- Benson, K.J.; Laskin, D.M. Upper lip asymmetry in adult during smiling. J. Oral Maxillofac. Surg. 2001, 59, 396–398. [Google Scholar] [CrossRef]
- Ko, E.W.-C.; Huang, C.S.; Chen, Y.R. Characteristics and Corrective Outcome of Face Asymmetry by Orthognathic Surgery. J. Oral Maxillofac. Surg. 2009, 67, 2201–2209. [Google Scholar] [CrossRef] [PubMed]
- Udomlarptham, N.; Lin, C.H.; Wang, Y.C.; Ko, E.W.C. Does 2D vs 3D Surgical Simulation Produce Better Surgical Outcomes Among Patients with Class III Facial Asymmetry? Int. J. Oral Maxillofac. Surg. 2018, 47, 1022–1031. [Google Scholar] [CrossRef] [PubMed]
- Seixas, M.R.; Costa-Pinto, R.A.; de Araújo, T.M. Checklist of esthetic features to consider in diagnosing and treating excessive gingival display (gummy smile). Dental Press J. Orthod. 2011, 16, 131–157. [Google Scholar] [CrossRef]
- Sarver, D.M. The importance of incisor positioning in the esthetic smile: The smile arc. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 98–111. [Google Scholar] [CrossRef]
- Maskey, S.; Shrestha, R. Cephalometric approach to vertical facial height. Orthdontic J. Nepal 2019, 9, 54–58. [Google Scholar] [CrossRef]
- Wong, R.; Chau, A.; Hägg, U. 3D CBCT McNamara’s cephalometric analysis in an adult southern Chinese population. Int. J. Oral Maxillofac. Surg. 2011, 40, 920–925. [Google Scholar] [CrossRef]
- Chan, Y.L.; Cheng, J.H.C.; Chen, P.H.; Chen, D.D.S. Is the ANB Norm in TAO Board Examination Appropriate? Meta-analysis of Taiwanese Cephalometric Norms. Taiwan. J. Orthod. 2021, 33, 149–155. [Google Scholar]
- Borikanphanitphaisan, T.; Lin, C.H.; Chen, Y.A.; Ko, E.W.C. Analysis of Jawbone Positioning Accuracy by the Guide of Intermediate Splint in Maxilla-first or Mandible-first Approach. Plast. Reconstr. Surg. 2021, 147, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Hong, M.; Park, H.-S. Analysis of dental compensation in patients with facial asymmetry using cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Insawak, R.; Lin, C.-H.; Chen, Y.-A.; Ko, E.W.-C. Comparison of 3-dimensional postoperative dental movement in Class III surgical correction with and without presurgical orthodontic treatment. Biomed. J. 2021, 44 (Suppl. 2), S282–S295. [Google Scholar] [CrossRef] [PubMed]
- Teng, T.T.Y.; Ko, E.W.C.; Huang, C.S.; Chen, Y.R. Effect of early physiotherapy on the recovery of mandibular function after orthognathic surgery for Class III correction: Part I—Jaw-motion analysis. J. Cranio-Maxillofac. Surg. 2015, 43, 131–137. [Google Scholar] [CrossRef]
- Ko, E.W.C.; Teng, T.T.Y.; Huang, C.S.; Chen, Y.R. Effect of early physiotherapy on the recovery of mandibular function after orthognathic surgery for Class III correction: Part II—Electromyography activity of masticatory muscles. J. Cranio-Maxillofac. Surg. 2015, 43, 138–143. [Google Scholar] [CrossRef]
- Ko, E.W.C.; Lin, C.H.; Chen, Y.A.; Chen, Y.R. Enhance surgical outcomes in patients with skeletal class III facial asymmetry by 3D surgical simulation. J. Oral Maxillofac. Surg. 2018, 76, 1073–1083. [Google Scholar] [CrossRef]
- Huang, C.S.; Liu, X.Q.; Chen, Y.R. Facial asymmetry index in normal young adults. Orthod. Craniofacial Res. 2013, 16, 97–104. [Google Scholar] [CrossRef]
- Huang, C.; Chen, Y.-R. Orthodontic principles and guidelines for the surgery-first approach to orthognathic surgery. Int. J. Oral Maxillofac. Surg. 2015, 44, 1457–1462. [Google Scholar] [CrossRef]
- Zheng, X.; Wang, L.; Zhang, B.; Bai, X.; Qin, K.; Tian, Y.; Zhao, R.; Liu, S.; Wang, J.; Zhao, Z. Accuracy of two midsagittal planes in three-dimensional analysis and their measurement in patients with skeletal mandibular deviation: A comparative study. Br. J. Oral Maxillofac. Surg. 2018, 56, 600–606. [Google Scholar] [CrossRef]
- Dobai, A.; Markella, Z.; Vízkelety, T.; Fouquet, C.; Rosta, A.; Barabás, J. Landmark-based midsagittal plane analysis in patients with facial symmetry and asymmetry based on CBCT analysis tomography. J. Orofac. Orthop. 2018, 79, 371–379. [Google Scholar] [CrossRef]
- Jajoo, A.; Nicol, M.; Gateno, J.; Chen, K.C.; Tang, Z.; Chowdhury, T.; Li, J.; Shen, S.G.; Xia, J.J. Calculating the midsagittal plane for symmetrical bilateral shapes: Application to clinical facial surgical planning. arXiv 2018, arXiv:1803.05853. [Google Scholar]
- Zhu, Y.J.; Xu, Q.; Zhao, Y.J.; Zhang, L.; Fu, Z.W.; Wen, A.N.; Gao, Z.X.; Zhang, J.; Fu, X.L.; Wang, Y. Deep learning-assisted construction of three-dimensional facial midsagittal plane. J. Peking Univ. 2022, 54, 134–139. [Google Scholar]
- Worms, F.W.; Isaacson, R.J.; Speidel, T.M. Surgical orthodontic treatment planning: Profile analysis and mandibular surgery. Angle Orthod. 1976, 46, 1–25. [Google Scholar] [PubMed]
- Huang, C.; Hsu, S.-P.; Chen, Y.-R. Systematic review of the surgery-first approach in orthognathic surgery. Biomed. J. 2014, 37, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Verna, C. Regional Acceleratory Phenomenon. Front. Oral Biol. 2016, 18, 28–35. [Google Scholar] [PubMed]
- Assael, L.A. The Biggest Movement: Orthognathic Surgery Undergoes Another Paradigm Shift. J. Oral Maxillofac. Surg. 2008, 66, 419–420. [Google Scholar] [CrossRef]
- Choi, J.W.; Park, H.; Kwon, S.-M.; Lee, J.Y. Surgery-first orthognathic approach for the correction of facial asymmetry. J. Cranio-Maxillofac. Surg. 2021, 49, 435–442. [Google Scholar] [CrossRef]
- Choi, J.W.; Park, H.; Kim, B.I.-H.; Kim, N.; Kwon, S.-M.; Lee, J.Y. Surgery-First Orthognathic Approach to Correct Facial Asymmetry: Artificial Intelligence–Based Cephalometric Analysis. Plast. Reconstr. Surg. 2022, 149, 496e–499e. [Google Scholar] [CrossRef]
- Chang, H.W.; Lin, H.H.; Chortrakarnkij, P.; Kim, S.G.; Lo, L.J. Intraoperative navigation for single-splint two-jaw orthognathic surgery: From model to actual surgery. J. Cranio-Maxillofac. Surg. 2015, 43, 1110–1126. [Google Scholar] [CrossRef]
- Ko, E.W.-C.; Lin, S.C.; Chen, Y.R.; Huang, C.S. Skeletal and Dental Variables Related to the Stability of Orthognathic Surgery in Skeletal Class III Malocclusion with a Surgery-First Approach. J. Oral Maxillofac. Surg. 2013, 71, e215–e223. [Google Scholar] [CrossRef]
- Liu, L.-C.; Chen, Y.-A.; Chen, R.-F.; Yao, C.-F.; Liao, Y.-F.; Chen, Y.-R. Type of mandibular asymmetry affects changes and outcomes of bimaxillary surgery for class III asymmetry. Clin. Oral Investig. 2021, 26, 1077–1088. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-C.; Wallace, C.G.; Pai, B.C.-J.; Chen, H.-L.; Lee, Y.-T.; Hsiao, Y.-C.; Chang, C.-S.; Liao, Y.-F.; Chen, P.K.-T.; Chen, Y.-R. Orthognathic Surgery with Simultaneous Autologous Fat Transfer for Correction of Facial Asymmetry. Plast. Reconstr. Surg. 2017, 139, 693–700. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}