
Motor Skills Training Program Reinforces Crossing the Body’s Midline in Children with Developmental Coordination Disorder


Abstract
:1. Introduction
2. Methods
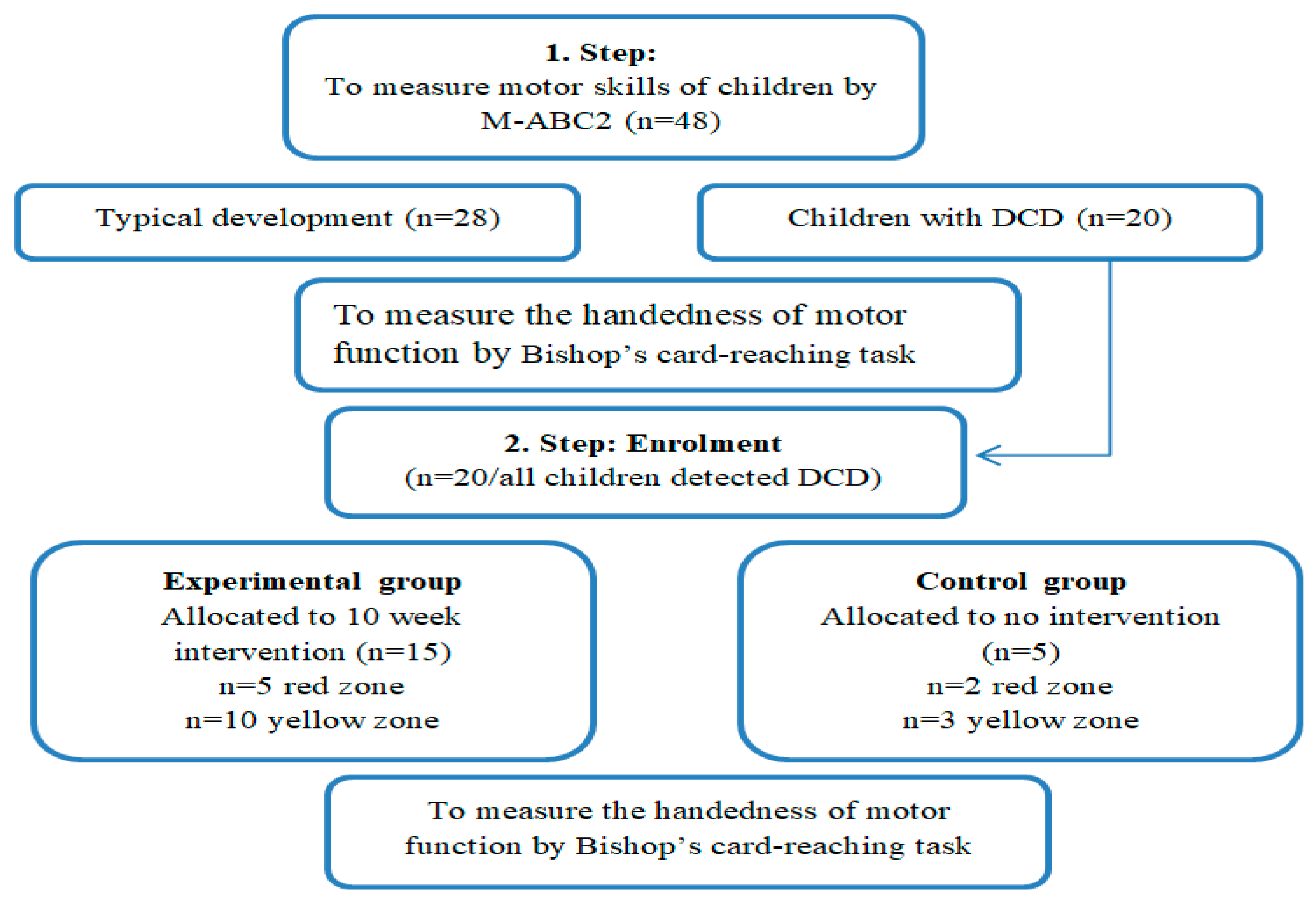
2.1. Study Design
2.2. Participants
2.3. Instruments
2.4. Procedures
2.5. Ethics
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ayers, A. Sensory Integration and Learning Disorders; Western Psychological Services: Los Angles, CA, USA, 1971. [Google Scholar]
- Schilder, P. The Image an Appearance of the Human Body; International University Press: New York, NY, USA, 1950. [Google Scholar]
- Stilwell, J.M. The development of manual midline crossing in 2- to 6-year-old children. Am. J. Occup. Ther. 1987, 41, 783–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.M. Performance difference between hands in children on the motor accuracy test-revised. Am. J. Occup. Ther. Off. Publ. Am. Occup. Ther. Assoc. 1983, 37, 96–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherick, I.; Greenman, G.; Legg, C. Some comments on the significance and development of midline behavior during infancy. Child Psychiatry Hum 1976, 6, 170–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goody, W.; Reinhold, M. Some aspects of human orientation in space: Sensation and movement. Brain 1952, 75, 472–509. [Google Scholar] [CrossRef] [PubMed]
- Serrien, D.J.; O’Regan, L. The development of motor planning strategies in children. Eur. J. Dev. Psychol. 2021, 18, 1–17. [Google Scholar] [CrossRef]
- Carlier, M.; Anne-Lise, D.; Lamard, C. Midline crossing: Developmental trend from 3 to 10 years of age in a preferential card-reaching task. Brain Cogn. 2006, 61, 255–261. [Google Scholar] [CrossRef]
- Cermak, S.A.; Quintero, E.J.; Cohen, P.M. Developmental age trends in crossing the body midline in normal children. Am. J. Occup. Ther. Off. Publ. Am. Occup. Ther. Assoc. 1980, 34, 313–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, S.J.; Young, M.N. Midline crossing movements: A teachable skill for developing children. In Proceedings of the AARE 2010 Conference Proceedings, Melbourne, VIC, Australia, 28 November–2 December 2010. [Google Scholar]
- Michell, D.; Wood, N. An investigation of midline crossing in three-year old children. Physiotherapy 1999, 85, 607–615. [Google Scholar] [CrossRef]
- Murata, N.M.; Tan, C.A. Collaborative teaching of motor skills for preschools with developmental delays. Early Child. Educ. 2009, 36, 483–489. [Google Scholar] [CrossRef]
- Begum Ali, J.; Charman, T.; Johnson, M.H.; Jones, E.J. Early motor differences in infants at elevated likelihood of autism spectrum disorder and/or attention deficit hyperactivity disorder. J. Autism Dev. Disord. 2020, 50, 4367–4384. [Google Scholar] [CrossRef] [Green Version]
- Groen, M.A.; Yasin, I.; Laws, G.; Barry, J.G.; Bishop, D.V. Weak hand preference in children with Down syndrome is associated with language deficits. Dev. Psychobiol. J. Int. Soc. Dev. Psychobiol. 2008, 50, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.L.; Bishop, D.V. A reaching test reveals weak hand preference in specific language impairment and developmental co-ordination disorder. Laterality 1998, 3, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Smits-Engelsman, B.C.; Bloem-van der Wel, H.E.; Duysens, J. Children with Developmental Coordination Disorder respond similarly to age-matched controls in both speed and accuracy if goal-directed movements are made across the midline. Child Care Health Dev. 2006, 32, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Zoia, S.; Blason, L.; D’Ottavio, G.; Bulgheroni, M.; Pezzetta, E.; Skabar, A.; Castiello, U. Evidence of early development of action planning in the human foetus: A kinematic study. Experimental brain research. Experimentelle Hirnforschung. Expérimentation Cérébrale 2007, 176, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Goez, H.; Zelnik, N. Handedness in Patients with Developmental Coordination Disorder. J. Child Neurol. 2008, 23, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Freitas, C.; Vasconcelos, O.; Botelho, V. Handedness and developmental coordination disorder in Portuguese children: Study with the M-ABC test. Laterality Asymmetries Body Brain Cogn. 2014, 6, 655–676. [Google Scholar] [CrossRef]
- Biancotto, M.; Skabar, A.; Bulgheroni, M.; Carrozzi, M.; Zoia, S. Neuromotor deficits in developmental coordination disorder: Evidence from a reach-to-grasp task. Res. Dev. Disabil. 2011, 32, 1293–1300. [Google Scholar] [CrossRef]
- Saidmamatov, O.; Raximov, Q.; Rodrigues, P.; Vasconcelos, O. A Ten-Week Motor Skills Training Program Increases Motor Competence in Children with Developmental Coordination Disorder. Children 2021, 8, 1147. [Google Scholar] [CrossRef]
- Coryell, J.F.; Michel, G.F. How Supine Postural Preferences of Infants can contribute toward the development of handedness. Infant Behav. 1978, 1, 245–257. [Google Scholar] [CrossRef]
- Nudo, R.J.; Milliken, G.W.; Jenkins, W.M.; Merzenich, M.M. Usedependent alterations of movement representations in primary motor cortex of adult squirrel monkeys. J. Neurosci. 1996, 16, 785–807. [Google Scholar] [CrossRef] [Green Version]
- Provins, K.A. Handedness and speech: A critical reappraisal of the role of genetic and environmental factors in the cerebral lateralization of function. Psychol. Rev. 1997, 104, 554–571. [Google Scholar] [CrossRef] [PubMed]
- Corbetta, D.; Thelen, E. Behavioral fluctuations and the development of manual asymmetries in infancy: Contributions of the dynamic systems approach. Handb. Neuropsychol. 2002, 8, 311–330. [Google Scholar]
- American Psychiatric Association. DSM-5 Task Force, 5th ed.; American Psychiatric Publishing, Inc.: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Henderson, S.E.; Sugden, D.A.; Barnett, A.L. Movement Assessment Battery for Children-2; Harcourt Assessment: London, UK, 2007. [Google Scholar]
- Lander, N.; Morgan, P.J.; Salmon, J.; Barnett, L.M. Teachers’ Perceptions of a Fundamental Movement Skill (FMS) Assessment Battery in a School Setting. Meas. Phys. Educ. Exerc. Sci. 2016, 20, 50–62. [Google Scholar] [CrossRef] [Green Version]
- Lander, N.; Morgan, P.J.; Salmon, J.; Logan, S.W.; Barnett, L.M. The reliability and validity of an authentic motor skill assessment tool for early adolescent girls in an Australian school setting. J. Sci. Med. Sport 2017, 20, 590–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, M.O.; Kastner, J.; Petermann, F.; Bös, K. Factorial validity of the Movement Assessment Battery for Children-2 (age band 2). Res. Dev. Disabil. 2011, 32, 674–680. [Google Scholar] [CrossRef] [Green Version]
- Kita, Y.; Suzuki, K.; Hirata, S.; Sakihara, K.; Inagaki, M.; Nakai, A. Applicability of the Movement Assessment Battery for Children-Second Edition to Japanese children: A study of the Age Band 2. Brain Dev. 2016, 38, 706–713. [Google Scholar] [CrossRef]
- Ellinoudis, T.; Evaggelinou, C.; Kourtessis, T.; Konstantinidou, Z.; Venetsanou, F.; Kambas, A. Reliability and validity of age band 1 of the Movement Assessment Battery for Children--second edition. Res. Dev. Disabil. 2011, 32, 1046–1051. [Google Scholar] [CrossRef]
- Jaikaew, R.; Satiansukpong, N. Movement Assessment Battery for Children-(MABC2): Cross-Cultural Validity, Content Validity, and Interrater Reliability in Thai Children. Occup. Ther. Int. 2019, 2019, 4086594. [Google Scholar] [CrossRef] [Green Version]
- Bishop, D.V.M.; Ross, V.; Daniels, M.S.; Bright, P. The measurement of hand preference. A validation study comparing three groups of right-handers. Br. J. Psychol. 1996, 87, 269–285. [Google Scholar] [CrossRef]
- Doyen, A.-L.; Carlier, M. Measuring Handedness: A validation study of the Bishop’s Card-reaching test. Laterality 2002, 7, 115–130. [Google Scholar] [CrossRef]
- Saidmamatov, O.A.; Nascimento, M.M.; Cerqueira, J.C.; Rodriguez, P.; Vasconcelos, O. Motor skill training programs for children with developmental coordination disorder: Does gender matter? Neuropsychiatr. L’enfance L’adolescence 2022, in press. [Google Scholar] [CrossRef]
- Howell, D.C. Statistical Methods for Psychology, 4th ed.; Wadsworth Publishing: Belmont, CA, USA, 1997. [Google Scholar]
- Cohen, J. Eta-squared and partial eta-squared in fixed factor ANOVA design. Educ. Psychol. Meas. 1973, 33, 107–112. [Google Scholar] [CrossRef]
- Bryden, P.J.; Pryde, K.M.; Roy, E.A. A performance measure of the degree of hand preference. Brain Cogn. 2000, 44, 402–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Regan, L.; Serrien, D. Individual Differences and Hemispheric Asymmetries for Language and Spatial Attention. Front. Hum. Neurosci. 2018, 12, 380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyen, A.; Dufour, T.; Caroff, X.; Cherfouh, A.; Carlier, M. Hand preference and hand performance: Cross sectional developmental trends and family resemblance in degree of laterality. Laterality 2008, 13, 179–197. [Google Scholar] [CrossRef]
- Bishop, D.V.; Adams, C. A prospective study of the relationship between specific language impairment, phonological disorders and reading retardation. J. Child Psychol. Psychiatry Allied Discip. 1990, 31, 1027–1050. [Google Scholar] [CrossRef]
- Verfaellie, M.; Bowers, D.; Heilman, K.M. Attentional factors in the occurrence of stimulus-response compatibility effects. Neuropsychologia 1988, 28, 435–444. [Google Scholar] [CrossRef]
- Verfaellie, M.; Heilman, K. Hemispheric asymmetries in attentional control: Implications for hand preference in sensorimotor tasks. Brain Cogn. 1990, 14, 70–80. [Google Scholar] [CrossRef]
- Gabbard, C.; Rabb, C. What determines choice of limb for unimanual reaching movements? J. Gen. Psychol. 2000, 127, 178–184. [Google Scholar] [CrossRef]
- Vasconcelos, O.; Rodrigues, P.; Barreiros, J.; Jacobsohn, L. Laterality, developmental coordination disorders and posture. In Estudos em Desenvolvimento Motor da Criança II; Rodrigues, L.P., Saraiva, L., Barreiros, J., Vasconcelos, O., Eds.; Escola Superior de Educação, Instituto Politécnico de Viana do Castelo: Viana do Castelo, Portugal, 2009; pp. 19–26. ISBN 978-989-95980-3-4. [Google Scholar]
- Liederman, J. Mechanisms underlying instability in the development of hand preference. In Manual Specialization and the Developing Brain; Young, G., Segalworitz, S.J., Carter, C.M., Trehub, S.E., Eds.; Academic Press: New York, NY, USA, 1983; pp. 82–85. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Group | EG | CG | TD | |||
|---|---|---|---|---|---|---|
| N | 15 | 5 | 28 | |||
| Position | Mean | SD | Mean | SD | Mean | SD |
| 1 | 0.67 | 1.18 | 0.80 | 1.10 | 0.32 | 0.82 |
| 2 | 0.47 | 1.10 | 0.00 | 0.00 | 0.39 | 1.00 |
| 3 | 1.27 | 1.49 | 0.40 | 0.89 | 0.50 | 1.04 |
| 4 | 1.87 | 1.25 | 1.89 | 0.70 | 2.71 | 0.54 |
| 5 | 2.87 | 0.52 | 3.00 | 0.00 | 2.93 | 0.38 |
| 6 | 3.00 | 0.00 | 3.00 | 0.00 | 2.93 | 0.40 |
| 7 | 3.00 | 0.00 | 3.00 | 0.00 | 2.93 | 0.40 |
| Group | EG | CG | TD | |||
|---|---|---|---|---|---|---|
| N | 15 | 5 | 28 | |||
| Position | Mean | SD | Mean | SD | Mean | SD |
| 1 | 0.00 | 0.00 | 1.00 | 1.40 | 0.32 | 0.82 |
| 2 | 0.00 | 0.00 | 0.00 | 0.00 | 0.39 | 0.99 |
| 3 | 0.20 | 0.77 | 0.40 | 0.89 | 0.50 | 1.04 |
| 4 | 2.20 | 1.08 | 3.00 | 0.00 | 2.71 | 0.53 |
| 5 | 3.00 | 0.00 | 3.00 | 0.00 | 2.93 | 0.38 |
| 6 | 3.00 | 0.00 | 3.00 | 0.00 | 2.93 | 0.38 |
| 7 | 3.00 | 0.00 | 3.00 | 0.00 | 2.93 | 0.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saidmamatov, O.; Rodrigues, P.; Vasconcelos, O. Motor Skills Training Program Reinforces Crossing the Body’s Midline in Children with Developmental Coordination Disorder. Symmetry 2022, 14, 1259. https://doi.org/10.3390/sym14061259
Saidmamatov O, Rodrigues P, Vasconcelos O. Motor Skills Training Program Reinforces Crossing the Body’s Midline in Children with Developmental Coordination Disorder. Symmetry. 2022; 14(6):1259. https://doi.org/10.3390/sym14061259
Chicago/Turabian StyleSaidmamatov, Orifjon, Paula Rodrigues, and Olga Vasconcelos. 2022. "Motor Skills Training Program Reinforces Crossing the Body’s Midline in Children with Developmental Coordination Disorder" Symmetry 14, no. 6: 1259. https://doi.org/10.3390/sym14061259