
Modulation of Asymmetry in Auditory Perception through a Bilateral Auditory Intervention

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Type
2.2. Subjects
2.3. Intervention
2.4. Auditory Intervention (Modified Bérard Method)
2.5. Absence of Auditory Intervention
2.6. Study Variables
2.7. Pure-Tone Audiometry (Air Conduction)
2.8. Goldberg Anxiety and Depression Scale (GADS)
2.9. Hamilton Anxiety Rating Scale (HAM-A)
2.10. Hamilton Depression Rating Scale (HAM-D)
2.11. Sociodemographic Variables
2.12. Statistical Analysis
2.13. Sample Characteristics
2.14. Audiogram Analysis
3. Results
3.1. Evaluation of Auditory Intervention on Hearing in Different Groups
3.1.1. Emotional Well-Being Group
Analysis of Hearing Thresholds in the Emotional Well-Being Group
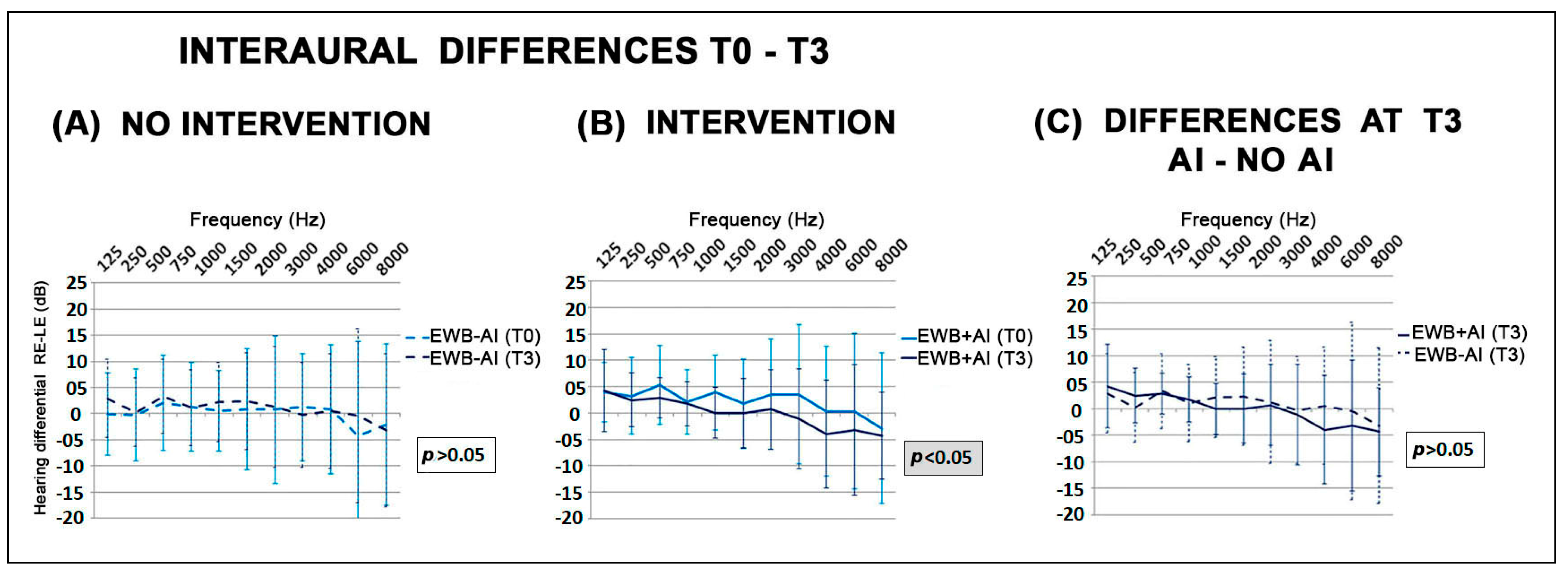
Comparison of Interaural Differences in the Emotional Well-Being Group
3.1.2. Anxiety Group
Analysis of Hearing Thresholds in the Anxiety Group
Comparison of Interaural Differences in the Anxiety Group
3.1.3. Mixed Group
Analysis of Hearing Thresholds in the Mixed Group
Comparison of Interaural Differences in the Mixed Group
3.2. Effect of Auditory Intervention in Each Ear and in Each Group
3.3. Comparison of Hearing Thresholds in Both Ears between the Emotional Well-Being Group without Auditory Intervention and the Anxiety and Mixed Groups with Auditory Intervention
3.4. Analysis of Auditory Patterns after Auditory Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Broca, P. Remarques sur le siège de la faculté du langage articulé, suivies d’une observation d’aphémie (perte de la parole). Bull. Mem. Soc. Anat. Paris 1861, 6, 330–357. [Google Scholar]
- Geschwind, N.; Levitsky, W. Human brain: Left-right asymmetries in temporal speech region. Science 1968, 161, 186–187. [Google Scholar] [CrossRef] [PubMed]
- Eberstaller, O. Das Stirnhirn; ein Beitrag zur Anatomie der Oberfläche des Grosshirns; Urban & Schwarzenberg: Munich, Germany, 1890. [Google Scholar]
- Ocklenburg, S.; Güntürkün, O. Hemispheric asymmetries: The comparative view. Front. Psychol. 2012, 3, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, E.; Roediger, D.; Kucukboyaci, N.E.; Carlson, C.; Devinsky, O.; Kuzniecky, R.; Halgren, E.; Thesen, T. Hemispheric asymmetries of cortical volume in the human brain. Cortex 2013, 49, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Frässle, S.; Paulus, F.M.; Krach, S.; Schweinberger, S.R.; Stephan, K.E.; Jansen, A. Mechanisms of hemispheric lateralization: Asymmetric interhemispheric recruitment in the face perception network. NeuroImage 2016, 124, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Kimura, D. Functional Asymmetry of the Brain in Dichotic Listening. Cortex 1967, 3, 163–178. [Google Scholar] [CrossRef]
- Hirnstein, M.; Westerhausen, R.; Korsnes, M.S.; Hugdahl, K. Sex differences in language asymmetry are age-dependent and small: A large-scale, consonant-vowel dichotic listening study with behavioral and fMRI data. Cortex 2013, 49, 1910–1921. [Google Scholar] [CrossRef]
- Hugdahl, K.; Løberg, E.-M.; Jørgensen, H.A.; Lundervold, A.; Lund, A.; Green, M.F.; Rund, B. Left hemisphere lateralisation of auditory hallucinations in schizophrenia: A dichotic listening study. Cogn. Neuropsychiatry 2008, 13, 166–179. [Google Scholar] [CrossRef]
- Prete, G.; D’Anselmo, A.; Brancucci, A.; Tommasi, L. Evidence of a Right Ear Advantage in the absence of auditory targets. Sci. Rep. 2018, 8, 15569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sininger, Y.S.; Bhatara, A. Laterality of basic auditory perception. Laterality 2012, 17, 129–149. [Google Scholar] [CrossRef] [Green Version]
- Estalayo-Gutiérrez, B.; Álvarez-Pasquín, M.J.; Germain, F. Modulation of Auditory Perception Laterality under Anxiety and Depression Conditions. Symmetry 2022, 14, 24. [Google Scholar] [CrossRef]
- Brancucci, A.; Babiloni, C.; Rossini, P.M.; Romani, G.L. Right hemisphere specialization for intensity discrimination of musical and speech sounds. Neuropsychologia 2005, 43, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, H.; Stracke, H.; Draganova, R.; Pantev, C. Hemispheric asymmetry of auditory evoked fields elicited by spectral versus temporal stimulus change. Cereb. Cortex 2009, 19, 2290–2297. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, H.; Kakigi, R. Hemispheric asymmetry of auditory mismatch negativity elicited by spectral and temporal deviants: A magnetoencephalographic study. Brain Topogr. 2015, 28, 471–478. [Google Scholar] [CrossRef] [Green Version]
- Brancucci, A.; D’Anselmo, A.; Martello, F.; Tommasi, L. Left hemisphere specialization for duration discrimination of musical and speech sounds. Neuropsychologia 2008, 46, 2013–2019. [Google Scholar] [CrossRef]
- Gainotti, G. Emotional behavior and hemispheric side of the lesion. Cortex 1972, 8, 41–55. [Google Scholar] [CrossRef]
- Gainotti, G. Unconscious processing of emotions and the right hemisphere. Neuropsychologia 2012, 50, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Davidson, R.J.; Mednick, D.; Moss, E.; Saron, C.; Schaffer, C.E. Ratings of emotion in faces are influenced by the visual field to which stimuli are presented. Brain Cogn. 1987, 6, 403–411. [Google Scholar] [CrossRef]
- Baijal, S.; Srinivasan, N. Emotional and hemispheric asymmetries in shifts of attention: An ERP study. Cogn. Emot. 2011, 25, 280–294. [Google Scholar] [CrossRef]
- Wyczesany, M.; Capotosto, P.; Zappasodi, F.; Prete, G. Hemispheric asymmetries and emotions: Evidence from effective connectivity. Neuropsychologia 2018, 121, 98–105. [Google Scholar] [CrossRef]
- Gainotti, G. Emotions and the Right Hemisphere: Can New Data Clarify Old Models? Neurosci. Rev. J. Bringing Neurobiol. Neurol. Psychiatry 2019, 25, 258–270. [Google Scholar] [CrossRef]
- Contrera, K.J.; Betz, J.; Deal, J.A.; Choi, J.S.; Ayonayon, H.N.; Harris, T.; Helzner, E.; Martin, K.R.; Mehta, K.; Pratt, S.; et al. Association of Hearing Impairment and Emotional Vitality in Older Adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2016, 71, 400–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakagami, M.; Kitahara, T.; Okayasu, T.; Yamashita, A.; Hasukawa, A.; Ota, I.; Yamanaka, T. Negative prognostic factors for psychological conditions in patients with audiovestibular diseases. Auris Nasus Larynx 2016, 43, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Zhai, F.; Wang, J.; Zhang, Y.; Dai, C.-F. Quantitative Analysis of Psychiatric Disorders in Intractable Peripheral Vertiginous Patients: A Prospective Study. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2016, 37, 539–544. [Google Scholar] [CrossRef]
- Mohamed, S.; Khan, I.; Iliodromiti, S.; Gaggini, M.; Kontorinis, G. Ménière’s Disease and Underlying Medical and Mental Conditions: Towards Factors Contributing to the Disease. ORL J. Oto-Rhino-Laryngol. Its Relat. Spec. 2016, 78, 144–150. [Google Scholar] [CrossRef]
- Kim, S.Y.; Jeon, Y.J.; Lee, J.-Y.; Kim, Y.H. Characteristics of tinnitus in adolescents and association with psychoemotional factors. Laryngoscope 2017, 127, 2113–2119. [Google Scholar] [CrossRef]
- Wiegner, L.; Hange, D.; Björkelund, C.; Ahlborg, G. Prevalence of perceived stress and associations to symptoms of exhaustion, depression and anxiety in a working age population seeking primary care--an observational study. BMC Fam. Pract. 2015, 16, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Kovel, C.G.F.; Aftanas, L.; Aleman, A.; Alexander-Bloch, A.F.; Baune, B.T.; Brack, I.; Bülow, R.; Busatto Filho, G.; Carballedo, A.; Connolly, C.G.; et al. No Alterations of Brain Structural Asymmetry in Major Depressive Disorder: An ENIGMA Consortium Analysis. Am. J. Psychiatry 2019, 176, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Hirakawa, N.; Hirano, Y.; Nakamura, I.; Hirano, S.; Sato, J.; Oribe, N.; Ueno, T.; Kanba, S.; Onitsuka, T. Right hemisphere pitch-mismatch negativity reduction in patients with major depression: An MEG study. J. Affect. Disord. 2017, 215, 225–229. [Google Scholar] [CrossRef]
- Bruder, G.E.; Stewart, J.W.; McGrath, P.J. Right brain, left brain in depressive disorders: Clinical and theoretical implications of behavioral, electrophysiological and neuroimaging findings. Neurosci. Biobehav. Rev. 2017, 78, 178–191. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Xu, H.; Lu, S. Neural Basis of Depression Related to a Dominant Right Hemisphere: A Resting-State fMRI Study. Behav. Neurol. 2018, 2018, 5024520. [Google Scholar] [CrossRef]
- Bruder, G.E.; Alvarenga, J.; Abraham, K.; Skipper, J.; Warner, V.; Voyer, D.; Peterson, B.S.; Weissman, M.M. Brain laterality, depression and anxiety disorders: New findings for emotional and verbal dichotic listening in individuals at risk for depression. Laterality 2016, 21, 525–548. [Google Scholar] [CrossRef]
- Jung, Y.-H.; Shin, J.E.; Lee, Y.I.; Jang, J.H.; Jo, H.J.; Choi, S.-H. Altered Amygdala Resting-State Functional Connectivity and Hemispheric Asymmetry in Patients With Social Anxiety Disorder. Front. Psychiatry 2018, 9, 164. [Google Scholar] [CrossRef]
- Peng, X.; Lau, W.K.W.; Wang, C.; Ning, L.; Zhang, R. Impaired left amygdala resting state functional connectivity in subthreshold depression individuals. Sci. Rep. 2020, 10, 17207. [Google Scholar] [CrossRef] [PubMed]
- Zatorre, R.J.; Chen, J.L.; Penhune, V.B. When the brain plays music: Auditory-motor interactions in music perception and production. Nat. Rev. Neurosci. 2007, 8, 547–558. [Google Scholar] [CrossRef]
- Koelsch, S. Brain correlates of music-evoked emotions. Nat. Rev. Neurosci. 2014, 15, 170–180. [Google Scholar] [CrossRef]
- Särkämö, T.; Tervaniemi, M.; Huotilainen, M. Music perception and cognition: Development, neural basis, and rehabilitative use of music. Wiley Interdiscip. Rev. Cogn. Sci. 2013, 4, 441–451. [Google Scholar] [CrossRef]
- Alluri, V.; Toiviainen, P.; Jääskeläinen, I.P.; Glerean, E.; Sams, M.; Brattico, E. Large-scale brain networks emerge from dynamic processing of musical timbre, key and rhythm. NeuroImage 2012, 59, 3677–3689. [Google Scholar] [CrossRef] [PubMed]
- Wan, C.Y.; Schlaug, G. Music making as a tool for promoting brain plasticity across the life span. Neurosci. Rev. J. Bringing Neurobiol. Neurol. Psychiatry 2010, 16, 566–577. [Google Scholar] [CrossRef] [Green Version]
- Schlaug, G. Musicians and music making as a model for the study of brain plasticity. Prog. Brain Res. 2015, 217, 37–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaquero, L.; Hartmann, K.; Ripollés, P.; Rojo, N.; Sierpowska, J.; François, C.; Càmara, E.; van Vugt, F.T.; Mohammadi, B.; Samii, A.; et al. Structural neuroplasticity in expert pianists depends on the age of musical training onset. NeuroImage 2016, 126, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Soria-Urios, G.; Duque, P.; García-Moreno, J.M. Música y cerebro: Fundamentos neurocientíficos y trastornos musicales. Rev. Neurol. 2011, 52, 45–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, G.-Y.; Yang, M.; Liu, B.; Huang, Z.-C.; Li, J.; Chen, J.-Y.; Chen, H.; Zhang, P.P.; Liu, L.J.; Wang, J.; et al. Changes of the directional brain networks related with brain plasticity in patients with long-term unilateral sensorineural hearing loss. Neuroscience 2016, 313, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Shiell, M.M.; Champoux, F.; Zatorre, R.J. The Right Hemisphere Planum Temporale Supports Enhanced Visual Motion Detection Ability in Deaf People: Evidence from Cortical Thickness. Neural Plast. 2016, 2016, 7217630. [Google Scholar] [CrossRef] [Green Version]
- Shi, B.; Yang, L.-Z.; Liu, Y.; Zhao, S.-L.; Wang, Y.; Gu, F.; Yang, Z.; Zhou, Y.; Zhang, P.; Zhang, X. Early-onset hearing loss reorganizes the visual and auditory network in children without cochlear implantation. Neuroreport 2016, 27, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Mowery, T.M.; Kotak, V.C.; Sanes, D.H. The onset of visual experience gates auditory cortex critical periods. Nat. Commun. 2016, 7, 10416. [Google Scholar] [CrossRef] [Green Version]
- Heggdal, P.O.L.; Brännström, J.; Aarstad, H.J.; Vassbotn, F.S.; Specht, K. Functional-structural reorganisation of the neuronal network for auditory perception in subjects with unilateral hearing loss: Review of neuroimaging studies. Hear. Res. 2016, 332, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Harrison Bush, A.L.; Lister, J.J.; Lin, F.R.; Betz, J.; Edwards, J.D. Peripheral Hearing and Cognition: Evidence From the Staying Keen in Later Life (SKILL) Study. Ear Hear. 2015, 36, 395–407. [Google Scholar] [CrossRef] [Green Version]
- Voller, J.; Potužáková, B.; Šimeček, V.; Vožeh, F. The role of whiskers in compensation of visual deficit in a mouse model of retinal degeneration. Neurosci. Lett. 2014, 558, 149–153. [Google Scholar] [CrossRef]
- Puschmann, S.; Sandmann, P.; Bendixen, A.; Thiel, C.M. Age-related hearing loss increases cross-modal distractibility. Hear. Res. 2014, 316, 28–36. [Google Scholar] [CrossRef]
- Salimpoor, V.N.; Benovoy, M.; Larcher, K.; Dagher, A.; Zatorre, R.J. Anatomically distinct dopamine release during anticipation and experience of peak emotion to music. Nat. Neurosci. 2011, 14, 257–262. [Google Scholar] [CrossRef]
- Okada, K.; Kurita, A.; Takase, B.; Otsuka, T.; Kodani, E.; Kusama, Y.; Atarashi, H.; Mizuno, K. Effects of music therapy on autonomic nervous system activity, incidence of heart failure events, and plasma cytokine and catecholamine levels in elderly patients with cerebrovascular disease and dementia. Int. Heart J. 2009, 50, 95–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradt, J.; Dileo, C.; Potvin, N. Music for stress and anxiety reduction in coronary heart disease patients. Cochrane Database Syst. Rev. 2013, 12, CD006577. [Google Scholar] [CrossRef]
- Radley, J.; Morilak, D.; Viau, V.; Campeau, S. Chronic stress and brain plasticity: Mechanisms underlying adaptive and maladaptive changes and implications for stress-related CNS disorders. Neurosci. Biobehav. Rev. 2015, 58, 79–91. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, U. The effect of music intervention in stress response to cardiac surgery in a randomized clinical trial. Heart Lung J. Crit. Care 2009, 38, 201–207. [Google Scholar] [CrossRef]
- Särkämö, T.; Pihko, E.; Laitinen, S.; Forsblom, A.; Soinila, S.; Mikkonen, M.; Autti, T.; Silvennoinen, H.M.; Erkkilä, J.; Laine, M.; et al. Music and speech listening enhance the recovery of early sensory processing after stroke. J. Cogn. Neurosci. 2010, 22, 2716–2727. [Google Scholar] [CrossRef]
- Altenmüller, E.; Marco-Pallares, J.; Münte, T.F.; Schneider, S. Neural reorganization underlies improvement in stroke-induced motor dysfunction by music-supported therapy. Ann. N. Y. Acad. Sci. 2009, 1169, 395–405. [Google Scholar] [CrossRef]
- Amengual, J.L.; Rojo, N.; Veciana de Las Heras, M.; Marco-Pallarés, J.; Grau-Sánchez, J.; Schneider, S.; Vaquero, L.; Juncadella, M.; Montero, J.; Mohammadi, B.; et al. Sensorimotor plasticity after music-supported therapy in chronic stroke patients revealed by transcranial magnetic stimulation. PLoS ONE 2013, 8, e61883. [Google Scholar] [CrossRef]
- Bérard, G.; Brockett, S. Hearing Equals Behavior: Updated and Expanded; eBooks2go: Schaumburg, IL, USA, 2014. [Google Scholar]
- Goldberg, D.; Bridges, K.; Duncan-Jones, P.; Grayson, D. Detecting anxiety and depression in general medical settings. BMJ 1988, 297, 897–899. [Google Scholar] [CrossRef] [Green Version]
- Montón, C.; Pérez Echeverría, M.J.; Campos, R.; García Campayo, J.; Lobo, A. Escalas de ansiedad y depresión de Goldberg: Una guía de entrevista eficaz para la detección del malestar psíquico. Aten. Primaria Soc. Esp. Med. Fam. Comunitaria 1993, 12, 345–349. [Google Scholar]
- Carrobles, J.; Costa, M.; Del Ser, T.; Bartolomé, P. La práctica de la Terapia de Conducta; Promolibro: Valencia, Spain, 1986. [Google Scholar]
- Ramos-Brieva, J.A.; Cordero Villafáfila, A. Validación de la versión castellana de la escala de Hamilton para la depresión. Actas Luso-Esp. Neurol. Psiquiatr. Cienc. Afines 1986, 14, 324–334. [Google Scholar] [PubMed]
- Todd, W.V.; Douglas, J.G. Cerebral Cortex. Noltes Hum. Brain, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 541–578. [Google Scholar]
- Winer, J.A. Decoding the auditory corticofugal systems. Hear. Res. 2006, 212, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Straka, M.M.; Hughes, R.; Lee, P.; Lim, H.H. Descending and tonotopic projection patterns from the auditory cortex to the inferior colliculus. Neuroscience 2015, 300, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Papesh, M.A.; Hurley, L.M. Modulation of auditory brainstem responses by serotonin and specific serotonin receptors. Hear. Res. 2016, 332, 121–136. [Google Scholar] [CrossRef] [PubMed]
- Felix, R.A.; Elde, C.J.; Nevue, A.A.; Portfors, C.V. Serotonin modulates response properties of neurons in the dorsal cochlear nucleus of the mouse. Hear. Res. 2017, 344, 13–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maison, S.F.; Liu, X.-P.; Vetter, D.E.; Eatock, R.A.; Nathanson, N.M.; Wess, J.; Liberman, M.C. Muscarinic signaling in the cochlea: Presynaptic and postsynaptic effects on efferent feedback and afferent excitability. J. Neurosci. Off. J. Soc. Neurosci. 2010, 30, 6751–6762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schofield, B.R.; Motts, S.D.; Mellott, J.G. Cholinergic cells of the pontomesencephalic tegmentum: Connections with auditory structures from cochlear nucleus to cortex. Hear. Res. 2011, 279, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Khalfa, S.; Collet, L. Functional asymmetry of medial olivocochlear system in humans. Towards a peripheral auditory lateralization. Neuroreport 1996, 7, 993–996. [Google Scholar] [CrossRef] [PubMed]
- Philibert, B.; Veuillet, E.; Collet, L. Functional asymmetries of crossed and uncrossed medial olivocochlear efferent pathways in humans. Neurosci. Lett. 1998, 253, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Maison, S.F.; Le, M.; Larsen, E.; Lee, S.-K.; Rosowski, J.J.; Thomas, S.A.; Liberman, M.C. Mice lacking adrenergic signaling have normal cochlear responses and normal resistance to acoustic injury but enhanced susceptibility to middle-ear infection. J. Assoc. Res. Otolaryngol. JARO 2010, 11, 449–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevue, A.A.; Felix, R.A.; Portfors, C.V. Dopaminergic projections of the subparafascicular thalamic nucleus to the auditory brainstem. Hear. Res. 2016, 341, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, W.; Suga, N. Histaminergic modulation of nonspecific plasticity of the auditory system and differential gating. J. Neurophysiol. 2013, 109, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Sadock, V.A.; Sadock, B.J.; Ruiz, P. Anxiety Disorders. In Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry, 11th ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2015; pp. e19290–e19567. [Google Scholar]
- Sadock, V.A.; Sadock, B.J.; Ruiz, P. Mood Disorders. In Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry, 11th ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2015; pp. e17600–e19258. [Google Scholar]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Estalayo-Gutiérrez, B.; Álvarez-Pasquín, M.J.; Germain, F. Modulation of Asymmetry in Auditory Perception through a Bilateral Auditory Intervention. Symmetry 2022, 14, 2490. https://doi.org/10.3390/sym14122490
Estalayo-Gutiérrez B, Álvarez-Pasquín MJ, Germain F. Modulation of Asymmetry in Auditory Perception through a Bilateral Auditory Intervention. Symmetry. 2022; 14(12):2490. https://doi.org/10.3390/sym14122490
Chicago/Turabian StyleEstalayo-Gutiérrez, Beatriz, María José Álvarez-Pasquín, and Francisco Germain. 2022. "Modulation of Asymmetry in Auditory Perception through a Bilateral Auditory Intervention" Symmetry 14, no. 12: 2490. https://doi.org/10.3390/sym14122490