
Kinematic Analysis of Lower Limb Joint Asymmetry During Gait in People with Multiple Sclerosis

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
1.1. Characterization of Gait Asymmetry in PwMS: Methods Based on Discrete Values
1.2. Waveform-Based Methods to Assess Interlimb Symmetry During Gait
2. Materials and Methods
2.1. Participants
- Low-mild disability (EDSS ≤ 3.5, n = 59)
- Moderate-severe disability (EDSS > 3.5, n = 42)
2.2. Spatio-Temporal and Kinematic Data Collection and Processing
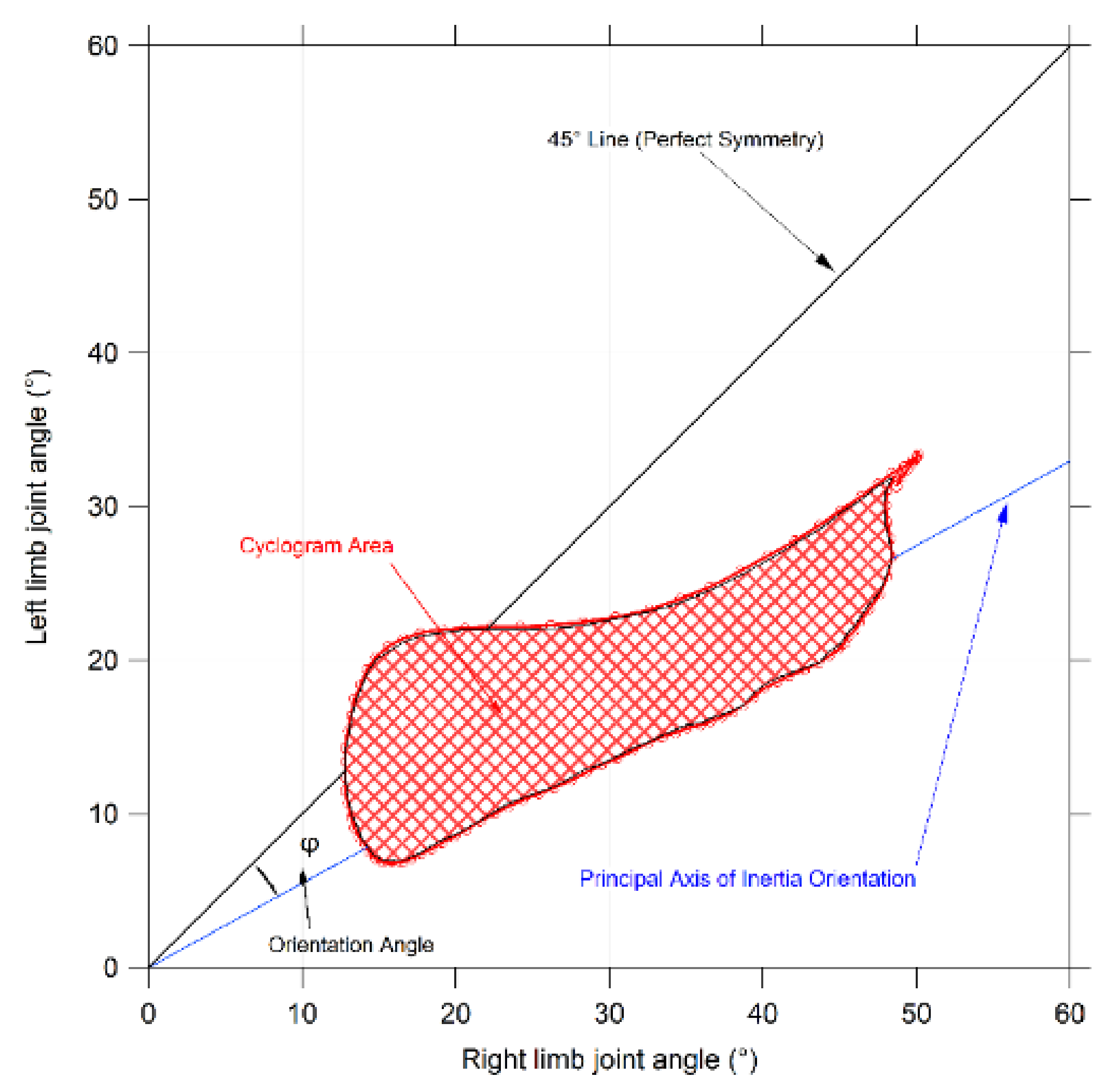
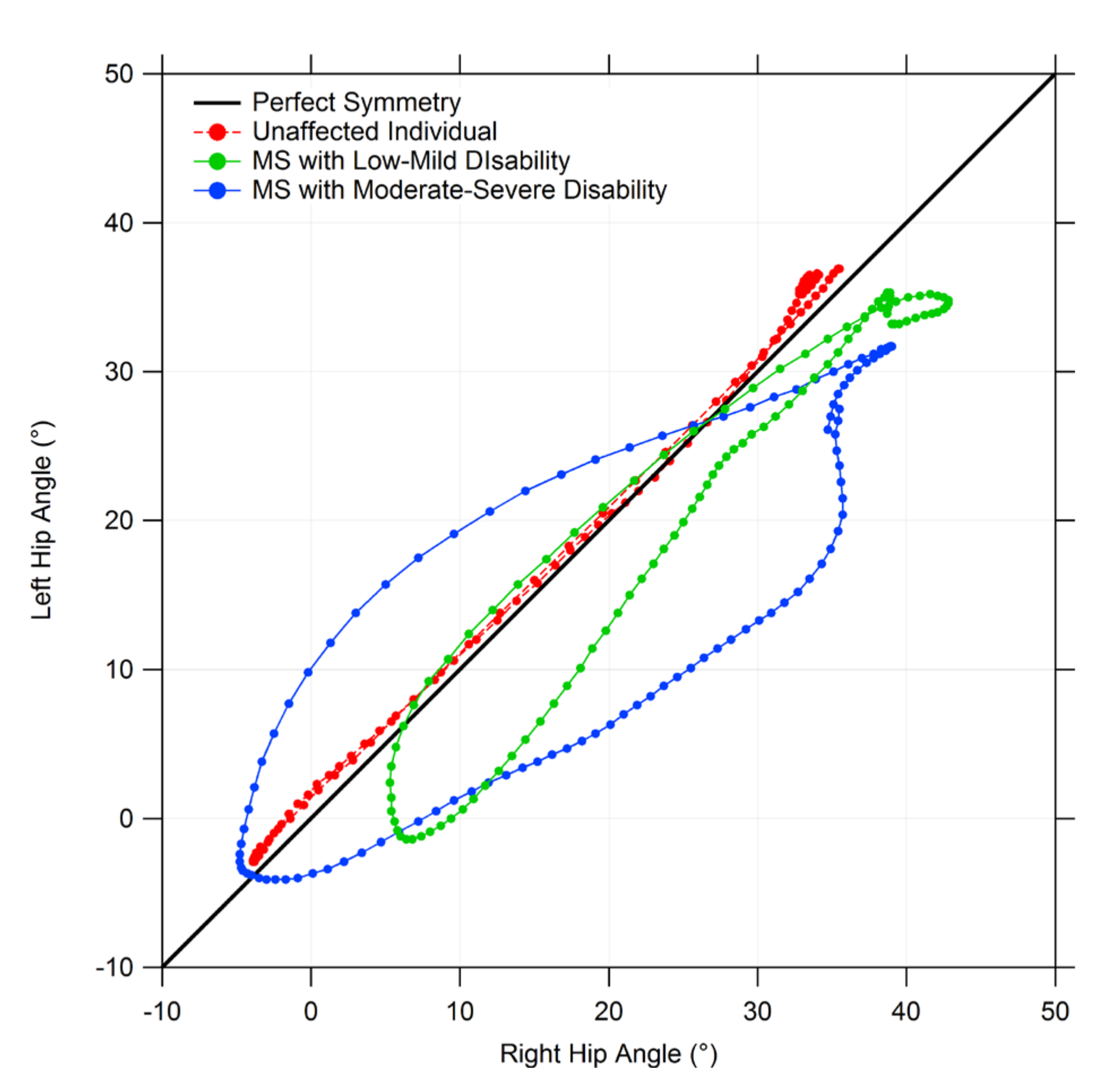
2.3. Gait Symmetry Quantification by Means of Cyclograms
- Cyclogram area (degrees2) represents the area of the closed curve obtained from each angle–angle diagram [42]. Since a perfectly symmetrical gait is achieved when both left and right joints are positioned at the same angle for a certain time of the gait cycle (i.e., all the cyclogram points stand on a 45° line in the diagram and thus the area is null), the interpretation of this parameter is quite straightforward; that is, the smaller the area, the more symmetrical the gait.
- Cyclogram orientation (degrees): this feature is identified by the absolute value of angle ϕ formed by the 45° line, which corresponds to perfect interlimb symmetry and the orientation of the principal axis of inertia, which corresponds to the minimum moment of inertia of the cyclogram [41,43]. The latter was calculated as the direction of the eigenvector of the matrix of inertia of the cyclogram points distribution in the x-y (i.e., left joint angle–right joint angle) reference system. Smaller values of this angle indicate higher interlimb symmetry.
- Trend Symmetry: this dimensionless parameter quantifies the similarity between two waveforms (in our case time-normalized right leg and left leg angular trend across the gait cycles for each joint of interest) using an eigenvector analysis (see [44] for details of the mathematical procedure). In particular, it is obtained by dividing the variability about the eigenvector to the variability along the eigenvector, and it is not influenced by the presence of a shift or by magnitude differences in two waveforms. Even in this case, the interpretation of this parameter is quite simple; a 0 value indicates perfect symmetry, and asymmetry increases as the Trend Symmetry value increases.
2.4. Statistical Analysis
3. Results
3.1. Spatio-Temporal Parameters of Gait
3.2. Gait Symmetry Indexes
3.3. Relationship between Symmetry Indexes and Spatio-Temporal Parameters of Gait
4. Discussion
4.1. General Considerations
4.2. Relationship between Interlimb Asymmetry, Spatio-Temporal Parameters of Gait and Disability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Compston, A.; Coles, A. Multiple sclerosis. Lancet 2008, 372, 1502–1517. [Google Scholar] [CrossRef]
- Koch-Henriksen, N.; Sørensen, P.S. The changing demographic pattern of multiple sclerosis epidemiology. Lancet Neurol. 2010, 9, 520–532. [Google Scholar] [CrossRef]
- Thompson, A.J.; Baranzini, S.E.; Geurts, J.; Hemmer, B.; Ciccarelli, O. Multiple sclerosis. Lancet 2018, 91, 1622–1636. [Google Scholar] [CrossRef]
- Cameron, M.H.; Lord, S. Postural control in multiple sclerosis: Implications for fall prevention. Curr. Neurol. Neurosci. Rep. 2010, 10, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Comber, L.; Galvin, R.; Coote, S. Gait deficits in people with multiple sclerosis: A systematic review and meta-analysis. Gait Posture 2017, 51, 25–35. [Google Scholar] [CrossRef]
- Lamers, I.; Feys, P. Assessing upper limb function in multiple sclerosis. Mult. Scler. 2014, 20, 775–784. [Google Scholar] [CrossRef]
- Buzaid, A.; Dodge, M.P.; Handmacher, L.; Kiltz, P.J. Activities of daily living: Evaluation and treatment in persons with multiple sclerosis. Phys. Med. Rehabil Clin. N. Am. 2013, 24, 629–638. [Google Scholar] [CrossRef]
- Institute of Medicine. Multiple Sclerosis: Current Status and Strategies for the Future; The National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Rudroff, T.; Proessl, F. Effects of Muscle Function and Limb Loading Asymmetries on Gait and Balance in People with Multiple Sclerosis. Front. Physiol. 2018, 9, 531. [Google Scholar] [CrossRef]
- Flachenecker, P.; Henze, T.; Zettl, U.K. Spasticity in patients with multiple sclerosis: Clinical characteristics, treatment and quality of life. Acta Neurol. Scand. 2014, 129, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Chung, L.H.; Remelius, J.G.; van Emmerik, R.E.; Kent-Braun, J.A. Leg power asymmetry and postural control in women with multiple sclerosis. Med. Sci. Sports Exerc. 2008, 40, 1717–1724. [Google Scholar] [CrossRef]
- Larson, R.D.; McCully, K.K.; Larson, D.J.; Pryor, W.M.; White, L.J. Bilateral differences in lower-limb performance in individuals with multiple sclerosis. J. Rehabil. Res. Dev. 2013, 50, 215–222. [Google Scholar] [CrossRef]
- Proessl, F.; Ketelhut, N.B.; Rudroff, T. No association of leg strength asymmetry with walking ability, fatigability, and fatigue in multiple sclerosis. Int. J. Rehabil. Res. 2018, 41, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Farrell III, J.W.; Motl, R.W.; Learmonth, Y.C.; Pilutti, L.A. Persons with Multiple Sclerosis Exhibit Strength Asymmetries in both Upper and Lower Extremities. Physiotherapy 2020, 25, S0031-9406(20)30392-8. [Google Scholar] [CrossRef] [PubMed]
- Workman, C.D.; Fietsam, A.C.; Rudroff, T. Associations of lower limb joint asymmetry with fatigue and disability in people with multiple sclerosis. Clin. Biomech. 2020, 75, 104989. [Google Scholar] [CrossRef] [PubMed]
- Daunoraviciene, K.; Ziziene, J.; Ovcinikova, A.; Kizlaitiene, R.; Griskevicius, J. Quantitative body symmetry assessment during neurological examination. Technol. Health Care 2020, 28, 573–584. [Google Scholar] [CrossRef]
- Filli, L.; Sutter, T.; Easthope, C.S.; Killeen, T.; Meyer, C.; Reuter, K.; Lörincz, L.; Bolliger, M.; Weller, M.; Curt, A.; et al. Profiling walking dysfunction in multiple sclerosis: Characterisation, classification and progression over time. Sci. Rep. 2018, 8, 4984. [Google Scholar] [CrossRef] [PubMed]
- Cofré-Lizama, L.E.; Khan, F.; Lee, P.V. The use of laboratory gait analysis for understanding gait deterioration in people with multiple sclerosis. Mult. Scler. 2016, 22, 1768–1776. [Google Scholar] [CrossRef]
- Robinson, R.O.; Herzog, W.; Nigg, B.M. Use of force platform variables to quantify the effects of chiropractic manipulation on gait symmetry. J. Manip. Physiol. Ther. 1987, 10, 172–176. [Google Scholar]
- Viteckova, S.; Kutilek, P.; Svoboda, Z.; Krupicka, R.; Kauler, J.; Szabo, Z. Gait symmetry measures: A review of current and prospective methods. Biomed. Signal Proces. 2018, 42, 89–100. [Google Scholar] [CrossRef]
- Dujmovic, I.; Radovanovic, S.; Martinovic, V.; Dackovic, J.; Maric, G.; Mesaros, S.; Pekmezovic, T.; Kostic, V.; Drulovic, J. Gait pattern in patients with different multiple sclerosis phenotypes. Mult. Scler. Relat. Disord. 2017, 13, 13–20. [Google Scholar] [CrossRef]
- Moraes, A.G.; Neri, S.G.R.; Motl, R.W.; Tauil, C.B.; Glehn, F.V.; Corrêa, É.C.; de David, A.C. Effect of hippotherapy on walking performance and gait parameters in people with multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 43, 102203. [Google Scholar] [CrossRef]
- Liao, F.; Wang, J.; He, P. Multi-resolution entropy analysis of gait symmetry in neurological degenerative diseases and amyotrophic lateral sclerosis. Med. Eng. Phys. 2008, 30, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.-B.; Zheng, Y.-P.; Guo, J.-Y.; Chen, X. Cross-fuzzy entropy: A new method to test pattern synchrony of bivariate time series. Inf. Sci. 2010, 180, 1715–1724. [Google Scholar] [CrossRef]
- Kutilek, P.; Viteckova, S.; Svoboda, Z.; Socha, V.; Smrcka, P. Kinematic quantification of gait asymmetry based on characteristics of angle-angle diagrams. Acta Polytechnica Hungarica 2014, 11, 25–38. [Google Scholar]
- Viteckova, S.; Kutilek, P.; Krupicka, R.; Adamova, B.; Szabo, Z.; de Brito, A.C.D.M.; Kopecka, J. Evaluation of movement of patients with Parkinson’s disease using wearable MoCap system and bilateral cyclograms. In Proceeding of the International Conference on Applied Electronics, Plisen, Chech Republic, 5–6 September 2017; University of West Bohami: Plisen, Chech Republic, 2017; pp. 269–272. [Google Scholar] [CrossRef]
- Pilkar, R.; Ramanujam, A.; Chervin, K.; Forrest, G.; Nolan, K.J. Cyclogram based Joint Symmetry Assessment after Utilization of a Foot Drop Stimulator during Post Stroke Hemiplegic Gait. J. Biomech. Eng. 2018. [Google Scholar] [CrossRef] [PubMed]
- Sung, P.S.; Danial, P. A Kinematic Symmetry Index of Gait Patterns Between Older Adults with and Without Low Back Pain. Spine 2017, 42, E1350–E1356. [Google Scholar] [CrossRef]
- Farkas, G.J.; Schlink, B.R.; Fogg, L.F.; Foucher, K.C.; Wimmer, M.A.; Shakoor, N. Gait asymmetries in unilateral symptomatic hip osteoarthritis and their association with radiographic severity and pain. Hip. Int. 2019, 29, 209–214. [Google Scholar] [CrossRef]
- Bai, X.; Ewins, D.; Crocombe, A.D.; Xu, W. Kinematic and biomimetic assessment of a hydraulic ankle/foot in level ground and camber walking. PLoS ONE 2017, 12, e0180836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grieve, D.W. Gait patterns and the speed of walking. Biomed. Eng. 1968, 3, 119–122. [Google Scholar]
- Crenshaw, S.J.; Richards, J.G.; Miller, C.M. Gait Symmetry in Subjects with Multiple Sclerosis. Med. Sci. Sports Exerc. 2006, 38, S1. [Google Scholar] [CrossRef]
- Polman, C.H.; Reingold, S.C.; Edan, G.; Filippi, M.; Hartung, H.P.; Kappos, L.; Lublin, F.D.; Metz, L.M.; McFarland, H.F. Diagnostic criteria for multiple sclerosis: 2005 revisions to the McDonald criteria. Ann. Neurol. 2005, 58, 840–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [Green Version]
- Pau, M.; Coghe, G.; Atzeni, C.; Corona, F.; Pilloni, G.; Marrosu, M.G.; Cocco, E.; Galli, M. Novel characterization of gait impairments in people with multiple sclerosis by means of the gait profile score. J. Neurol. Sci. 2014, 345, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Pau, M.; Coghe, G.; Corona, F.; Marrosu, M.G.; Cocco, E. Effect of spasticity on kinematics of gait and muscular activation in people with Multiple Sclerosis. J. Neurol. Sci. 2015, 358, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Pau, M.; Corona, F.; Coghe, G.; Marrosu, M.G.; Cocco, E. Quantitative assessment of the effects of 6 months of adapted physical activity on gait in people with multiple sclerosis: A randomized controlled trial. Disabil. Rehabil. 2017, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wells, R.P. The kinematics and energy variations of swing-through crutch gait. J. Biomech. 1979, 12, 579–585. [Google Scholar] [CrossRef]
- Crosbie, J. Kinematics of walking frame ambulation. Clin. Biomech. 1993, 8, 31–36. [Google Scholar] [CrossRef]
- Davis, R.B.; Õunpuu, S.; Tyburski, D. A gait analysis data collection and reduction technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Goswami, A. Kinematic quantification of gait symmetry based on bilateral cyclograms. In Proceedings of the International Society of Biomechanics XIXth Congress, Dunedin, New Zealand, 6–11 July 2003. [Google Scholar]
- Hershler, C.; Milner, M. Angle-angle diagrams in the assessment of locomotion. Am. J. Phys. Med. 1980, 59, 109–125. [Google Scholar]
- Goswami, A. A new gait parameterization technique by means of cyclogram moments: Application to human slope walking. Gait Posture 1998, 8, 15–36. [Google Scholar] [CrossRef]
- Crenshaw, S.J.; Richards, J.G. A method for analyzing joint symmetry and normalcy, with an application to analyzing gait. Gait Posture 2006, 24, 515–521. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, MI, USA, 1998. [Google Scholar]
- Lord, S.; Galna, B.; Rochester, L. Moving forward on gait measurement: Toward a more refined approach. Mov. Disord. 2013, 28, 1534–1543. [Google Scholar] [CrossRef] [PubMed]
- Cofré Lizama, L.E.; Bastani, A.; van der Walt, A.; Kilpatrick, T.; Khan, F.; Galea, M.P. Increased ankle muscle coactivation in the early stages of multiple sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2020, 11, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalron, A. Association between perceived fatigue and gait parameters measured by an instrumented treadmill in people with multiple sclerosis: A cross-sectional study. J. Neuroeng. Rehabil. 2015, 12, 34. [Google Scholar] [CrossRef] [Green Version]
- Escudero-Uribe, S.; Hochsprung, A.; Izquierdo-Ayuso, G. Gait pattern changes after six-minute walk test in persons with multiple sclerosis. Physiother. Res. Int. 2019, 24, e1741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shema-Shiratzky, S.; Gazit, E.; Sun, R.; Regev, K.; Karni, A.; Sosnoff, J.J.; Herman, T.; Mirelman, A.; Hausdorff, J.M. Deterioration of specific aspects of gait during the instrumented 6-min walk test among people with multiple sclerosis. J. Neurol. 2019, 266, 3022–3030. [Google Scholar] [CrossRef]
- Taborri, J.; Studer, V.; Grossi, P.; Brambilla, L.; Patanè, F.; Ferrò, M.T.; Mantegazza, R.; Rossi, S. Reliability and Repeatability Analysis of Indices to Measure Gait Deterioration in MS Patients during Prolonged Walking. Sensors 2020, 20, 5063. [Google Scholar] [CrossRef]
- Richmond, S.B.; Swanson, C.W.; Peterson, D.S.; Fling, B.W. A temporal analysis of bilateral gait coordination in people with multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 45, 102445. [Google Scholar] [CrossRef]
- Von Meyenburg, J.; Wilm, B.J.; Weck, A.; Petersen, J.; Gallus, E.; Mathys, J.; Schaetzle, E.; Schubert, M.; Boesiger, P.; von Meyenburg, K.; et al. Spinal cord diffusion-tensor imaging and motor-evoked potentials in multiple sclerosis patients: Microstructural and functional asymmetry. Radiology 2013, 267, 869–879. [Google Scholar] [CrossRef]
- Ramari, C.; Hvid, L.G.; David, A.C.; Dalgas, U. The importance of lower-extremity muscle strength for lower-limb functional capacity in multiple sclerosis: Systematic review. Ann. Phys. Rehabil. Med. 2020, 63, 123–137. [Google Scholar] [CrossRef]
- Plotnik, M.; Giladi, N.; Hausdorff, J.M. A new measure for quantifying the bilateral coordination of human gait: Effects of aging and Parkinson’s disease. Exp. Brain Res. 2007, 181, 561–570. [Google Scholar] [CrossRef]
- Plotnik, M.; Wagner, J.M.; Adusumilli, G.; Gottlieb, A.; Naismith, R.T. Gait asymmetry, and bilateral coordination of gait during a six-minute walk test in persons with multiple sclerosis. Sci. Rep. 2020, 10, 12382. [Google Scholar] [CrossRef] [PubMed]
- Pau, M.; Corona, F.; Pilloni, G.; Porta, M.; Coghe, G.; Cocco, E. Do gait patterns differ in men and women with multiple sclerosis? Mult. Scler. Relat. Disord. 2017, 18, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Farrell, J.W., III; Merkas, J.; Pilutti, L.A. The Effect of Exercise Training on Gait, Balance, and Physical Fitness Asymmetries in Persons with Chronic Neurological Conditions: A Systematic Review of Randomized Controlled Trials. Front. Physiol. 2020, 11, 585765. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Healthy Controls | All MS | MS Low-Mild Disability (EDSS ≤3.5) | MS Moderate-Severe Disability (EDSS >3.5) | |
|---|---|---|---|---|
| Participants (M, F) | 81 (44F, 37M) | 101 (55F, 46M) | 59 (33F, 26M) | 42 (22F, 20M) |
| Age (years) | 48.9 (15.2) | 46.3 (10.4) | 44.2 (10.3) | 49.3 (9.7) |
| Body Mass (kg) | 65.2 (11.4) | 64.7 (12.0) | 66.1 (12.5) | 62.8 (11.1) |
| Height (cm) | 167.2 (9.1) | 166.3 (9.3) | 166.7 (9.6) | 165.8 (9.0) |
| EDSS Score | – | 3.5 (1.7) | 2.4 (1.0) | 5.2 (1.0) |
| Healthy Controls | All MS | MS Low-Mild Disability (EDSS ≤3.5) | MS Moderate-Severe Disability (EDSS >3.5) | |
|---|---|---|---|---|
| Gait Speed (m/s) | 1.23 (0.19) | 0.85 (0.34) a | 1.00 (0.31) a | 0.65 (0.27) a,b |
| Stride Length (m) | 1.29 (0.13) | 1.02 (0.25) a | 1.09 (0.22) a | 0.92 (0.24) a,b |
| Cadence (steps/min) | 113.07 (10.34) | 96.49 (20.26) a | 104.48 (17.06) a | 85.26 (19.17) a,b |
| Step Width (m) | 0.20 (0.03) | 0.22 (0.04) a | 0.21 (0.03) | 0.23 (0.04) a |
| Stance Phase | 59.09 (2.80) | 63.63 (4.82) a | 62.51 (4.03) a | 65.22 (5.41) a,b |
| Swing Phase | 40.45 (1.76) | 35.78 (4.78) a | 37.22 (4.01) a | 33.75 (5.08) a,b |
| Double Support | 19.86 (3.60) | 29.38 (10.72) a | 25.58 (8.24) a | 34.7 (11.60) a,b |
| Cyclogram Parameter | Healthy Controls | All MS | MS Low-Mild Disability (EDSS ≤ 3.5) | MS Moderate-Severe Disability (EDSS >3.5) | |
|---|---|---|---|---|---|
| Area | Hip | 108.17 (98.54) | 195.52 (190.40) a | 144.16 (163.77) | 267.68 (203.34) a,b |
| Orientation ϕ | 1.58 (1.34) | 5.09 (7.06) a | 2.28 (2.64) | 9.05 (9.18) a,b | |
| Trend Symmetry | 0.26 (0.43) | 1.74 (2.97) a | 0.66 (0.98) | 3.27 (4.02) a,b | |
| Area | Knee | 270.60 (192.50) | 311.18 (269.64) | 262.71 (259.20) | 379.28 (272.33) |
| Orientation ϕ | 1.51 (1.57) | 6.99 (9.60) a | 2.22 (2.46) | 13.71 (11.71) a,b | |
| Trend Symmetry | 0.48 (0.41) | 4.19 (6.89) a | 1.26 (2.01) | 8.29 (8.98) a,b | |
| Area | Ankle | 76.45 (62.25) | 91.07 (82.40) | 74.50 (68.90) | 114.33 (94.33) |
| Orientation ϕ | 3.05 (2.80) | 6.45 (6.48) a | 4.88 (5.38) a | 8.65 (7.28) a,b | |
| Trend Symmetry | 1.51 (1.58) | 8.46 (10.00) a | 5.40 (9.70) a | 12.77 (8.84) a,b |
| EDSS Score | Speed | Stride Length | Cadence | Step width | Double Support | ||
|---|---|---|---|---|---|---|---|
| Area | Hip | 0.433 ** | −0.268 ** | −0.245 * | −0.240 * | 0.147 | 0.321 ** |
| Orientation ϕ | 0.509 ** | −0.511 ** | −0.475 ** | −0.403 ** | 0.262 ** | 0.426 ** | |
| Trend Symmetry | 0.619 ** | −0.581 ** | −0.519 ** | −0.493 ** | 0.349 ** | 0.568 ** | |
| Area | Knee | 0.314 ** | −0.225 * | −0.322 ** | −0.093 | 0.318 ** | 0.228 * |
| Orientation ϕ | 0.644 ** | −0.590 ** | −0.486 ** | −0.517 ** | 0.473 ** | 0.524 ** | |
| Trend Symmetry | 0.687 ** | −0.634 ** | −0.546 ** | −0.547 ** | 0.419 ** | 0.532 ** | |
| Area | Ankle | 0.223 * | −0.136 | −0.046 | −0.114 | 0.124 | 0.100 |
| Orientation ϕ | 0.391 ** | −0.439 ** | −0.354 ** | −0.464 ** | 0.281 ** | 0.376 ** | |
| Trend Symmetry | 0.636 ** | −0.627 ** | −0.512 ** | −0.573 ** | 0.465 ** | 0.509 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pau, M.; Leban, B.; Deidda, M.; Putzolu, F.; Porta, M.; Coghe, G.; Cocco, E. Kinematic Analysis of Lower Limb Joint Asymmetry During Gait in People with Multiple Sclerosis. Symmetry 2021, 13, 598. https://doi.org/10.3390/sym13040598
Pau M, Leban B, Deidda M, Putzolu F, Porta M, Coghe G, Cocco E. Kinematic Analysis of Lower Limb Joint Asymmetry During Gait in People with Multiple Sclerosis. Symmetry. 2021; 13(4):598. https://doi.org/10.3390/sym13040598
Chicago/Turabian StylePau, Massimiliano, Bruno Leban, Michela Deidda, Federica Putzolu, Micaela Porta, Giancarlo Coghe, and Eleonora Cocco. 2021. "Kinematic Analysis of Lower Limb Joint Asymmetry During Gait in People with Multiple Sclerosis" Symmetry 13, no. 4: 598. https://doi.org/10.3390/sym13040598