4. Discussion
Reshaping teeth and closing diastemas with direct resin composite has become a common practice in dentistry to achieve dental symmetry and improve esthetics [
2,
3]. This approach is particularly indicated when it involves restoring healthy teeth where there is a need to preserve as much dental structure as possible, namely enamel [
3].
The diagnostic evaluation of each case when carrying out direct anterior restorative treatments using composite resins is based on the evaluation of clinical crown dimensions, gingival display and architecture, tooth position, wear factors, occlusion, and anterior guidance [
4,
5,
11]. In addition, before initiating any restorative treatment, the periodontal tissues must be healthy and stable [
5], which was the case in both clinical cases described. Therefore, all these aspects should be considered while planning these cases to ensure predictable and long-lasting esthetic results [
11]. As for smile symmetry variables, even though the concept of esthetics is highly subjective, there are some aspects that the clinician should take into consideration, namely the smile arc, buccal corridors, and the existence or not of diastemas as well as of dental and gingival asymmetries [
12]. In both clinical cases, all these features were carefully evaluated in order to achieve the most symmetric smile possible, which was what both patients intended.
Obtaining a satisfactory and predictable esthetic and functional result is the main goal of restorative dental treatments. Specific tools, such as the diagnostic wax-up, may help improve the predictability of direct restorations. This technique consists of a dental diagnostic procedure in which planned restorations are developed in wax on a diagnostic cast to determine the necessary clinical procedures to achieve the desired clinical results [
13]. It may assist in estimating the amount of restorative space available and how to manage it, and it can also help evaluate the occlusal scheme [
13]. In addition, it can be used as a communication tool between the clinician and the patient and may help facilitate the acceptance and approval of the restorative treatment. From the diagnostic wax-up, it is possible to make a PVC matrix that will later serve as a guide throughout the restorative process, which was the case in the reported Case 1. The wax-up might also be a helpful tool when trying to restore smile symmetry, since the clinician may easily manage the available space in order to achieve perfect proportions and, therefore, smile symmetry [
9]. In Case 1, the authors found it much easier to achieve an esthetic final result as compared to Case 2, where freehand restorations of both central incisors were performed.
The composite resin type, adhesive systems, and the entire restorative technique can influence both the longevity of the restorations and the esthetic results, which is the main concern when restoring anterior teeth [
14]. Ceramic materials are an excellent option for anterior teeth rehabilitation [
15]. Even though this is a more expensive treatment option, it offers great advantages as it allows for a better, more durable, and more predictable esthetic outcome [
15]. However, composite resins have gained popularity as restorative materials, which is mainly due to the fact that they allow for maximum dental tissue conservation and possess excellent esthetic properties [
6]. They are also a good alternative to ceramics when there are financial and time limitations, are easy to substitute or repair, and if well-executed, they allow for excellent esthetic results [
7]. When working with dental composite materials, the main disadvantages relate to its color stability, possible resin chipping [
16], and it requires a trained and skilled professional in restorative dentistry to optimize the results [
1]. In fact, the failure behavior in anterior restorations is different from posterior restorations, presenting with less secondary caries and more restorations being replaced for other reasons such as chipping and color mismatch, which can many times be solved by repairing and polishing [
6,
16]. Therefore, regular maintenance appointments are mandatory, to correct any defects early or for a simple polishing procedure. Each material has its unique fabrication process, composition, and optical characteristics, which makes it predictable that the treatment outcome and longevity might differ according to the material used [
15].
Dental composite materials have extensively evolved throughout the years, progressively improving their mechanical and optical properties [
17]. Both nanohybrid and nanofilled composites are highly clinically successful and popular composites, since they combine good mechanical properties, such as clinical wear resistance, and allow excellent esthetic results since they are highly polishable and enable a smooth and lustrous surface [
17,
18]. The composite resin systems used in Case 1 and Case 2 are nanofilled and nanohybrid composites, respectively. They present similar characteristics, and the authors believe that the choice of these restorative materials positively influenced the final esthetic outcome. The main difference when using nanohybrid or nanofilled composites is regarding the polishing step, since there is evidence that nanofilled composites may show better polishability than hybrid composites [
18]. However, in this case, the authors found this difference imperceptible in the final results. As for optical characteristics, it is known that composite optical features are different from those of the natural teeth, as teeth color results from the interaction between light with tooth tissues (enamel, dentin, and pulp) [
19]. The optical properties (translucency, opalescence, and fluorescence) and thickness of these tissues determine the final tooth color [
19]. In order to try to mimic teeth’s layered structure, two optically different restorative materials are usually the materials of choice. Generally, composite resins used for dentin restoration are less translucent and highly chromatic, whereas enamel composites are highly translucent and less chromatic [
19]. By using restorative layering techniques using dentin and enamel composites, a more realistic final color can be achieved. However, since the optical properties of composite resins are not identical to the optical properties of the tooth tissues, it is not always advisable to place the enamel or dentin layers with the corresponding thickness to that of the natural structures [
19]. For example, when placing the enamel layer with the same thickness as the natural enamel, the final restoration may result in a grayish appearance. One of the optical characteristics that may justify this is the refractive index (RI), which is usually lower in composites [
19]. This means that using composite resins with a higher RI could result in better optical integration, with the possibility of using the same thickness as natural enamel [
19]. The composite system used in Case 2, ENA HRi
® (Micerium S.p.A., Genova, Italy), is an example of a high RI system (RI = 1.62) [
19], which allowed the authors to use composite layers with a thickness closer to that of natural enamel without losing value. Since Case 2 was a more demanding case in terms of color matching as teeth had a higher value and little available space on tooth 11 for the restorative procedures, the authors decided to use this composite system to restore these teeth without taking the risk of losing value.
Along with improvements in their physicochemical properties, recent composites allow good esthetic results with relatively simple application and layering techniques, including the use of dentin- and enamel-like composites as well as effect materials [
1]. There are two possible ways of performing the incremental application of composite resins: the centrifugal technique, which requires one or two oblique positioned layers of dentin shades, followed by an enamel layer as a final coat, or the buccolingual technique, first described by Didier Dietschi [
8], which was the one used in both clinical cases reported in this study. This technique advocates using a silicon index made from a previously planned wax-up to facilitate the initial reshaping of the teeth [
20]. The first layer of enamel is directly placed on the silicon index (to construct the palatal shell) followed by layers of dentin and/or different effect materials, which provides an optimal esthetic result, with a natural translucency and opalescence effect [
20]. In Case 1 and 2, the combination of the incremental buccolingual technique with the use of recent composite materials allowed the creation of a natural and esthetic result in both cases, imperceptibly matching the remaining tooth structure.
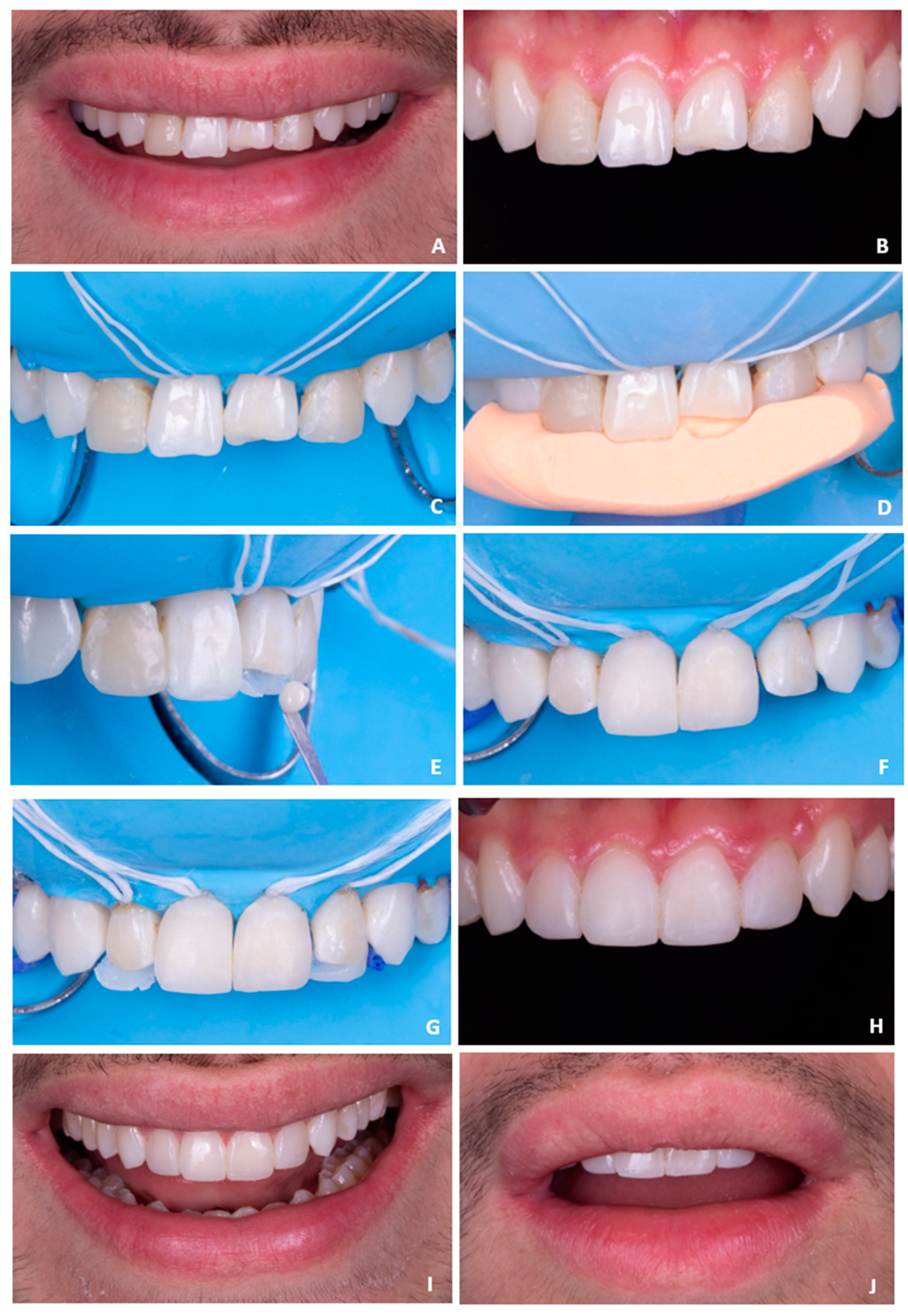
Accurate opposing and proximal contacts should also be correctly established when performing direct restorations. There are several ways of reshaping the proximal areas in anterior teeth. In Case 1, the authors used the Unica Anterior matrix (Unica Anterior, Polydentia, Mezzovico-Vira, Switzerland) to reshape the lateral incisors’ proximal areas. This particular matrix can be very helpful in more demanding cases, where perfect symmetry is the ultimate goal in anterior teeth. It is a pre-contoured metal matrix that can be easily adapted around the tooth, adjusting perfectly in the cervical area and allowing for the simultaneous shaping of both proximal areas. To the author’s knowledge, this is the first published clinical case using the Unica Anterior matrix system. Regarding diastema closure, it should be taken into consideration that the esthetic perception of the midline diastema varies according to culture, ethnic background, and socioeconomic and age groups [
21]. For example, in Africans, the maxillary midline diastema is perceived as an attractive dental feature and as a sign of beauty, whereas in Caucasians, this is rarely the case, and so, these varying concepts may influence the clinical decision on how to manage the presence of midline diastemas [
21]. In this case, the patient was unsatisfied with the presence of the diastema and aimed for its resolution. As for Case 2, the proximal areas were shaped using acetate matrices, which also allow a good proximal contour; however, it is more challenging to easily accomplish symmetry when comparing to the Unica Anterior matrix, for example. As for opposing contacts, these are as important as proximal contacts, and a careful evaluation should be previously carried out to avoid restorations fracture and interference with occlusal guides. In Case 1, the patient mentioned that tooth 21 was unsuccessfully restored several times before, as it fractured shortly after it was repaired. A carefully performed occlusal analysis suggested that anterior guidance was supported mainly on this tooth, justifying the recurrent fractures of the restoration. This highlights the need for a carefully planned case and the importance of analyzing all aspects involving extensive rehabilitations. In both clinical cases, the fractured central incisors (tooth 21 in both cases) were also a major complaint from both patients, which is understandable since the presence of maxillary incisor asymmetries strongly influences the perception of smile esthetics [
12]. For example, central incisors rarely show asymmetries in one of the three dimensions (length, width, or thickness) bigger than 0.2 to 0.3 mm [
9]. In addition, in a study conducted by Ribeiro et al. [
12], the authors concluded that the closer to the midline, the greater the need for symmetry, while pleasant asymmetric irregularities, distant from the midline, are acceptable. The authors also concluded that other facial components such as eyes, nose, and hair do not significantly influence the assessment of smile esthetics. All of these clinical features were taken into consideration in both cases, and a careful evaluation was performed in order to achieve smile symmetry.
In esthetic dentistry, even if clinicians use the best restorative materials and layering techniques, the color-matching process is still one of the most challenging steps in direct anterior restorations [
22]. The determination of dental color can be done visually, or employing instruments, such as the spectrophotometer, which allows a more objective evaluation [
22]. However, even when using a more objective measuring tool, the color of identical shade designated esthetic restorative materials is usually not consistent among different brands of materials [
23]. Therefore, the use of customized and individualized shade guides, layered in different colors and thicknesses, made from the same material as the future restoration is preferable [
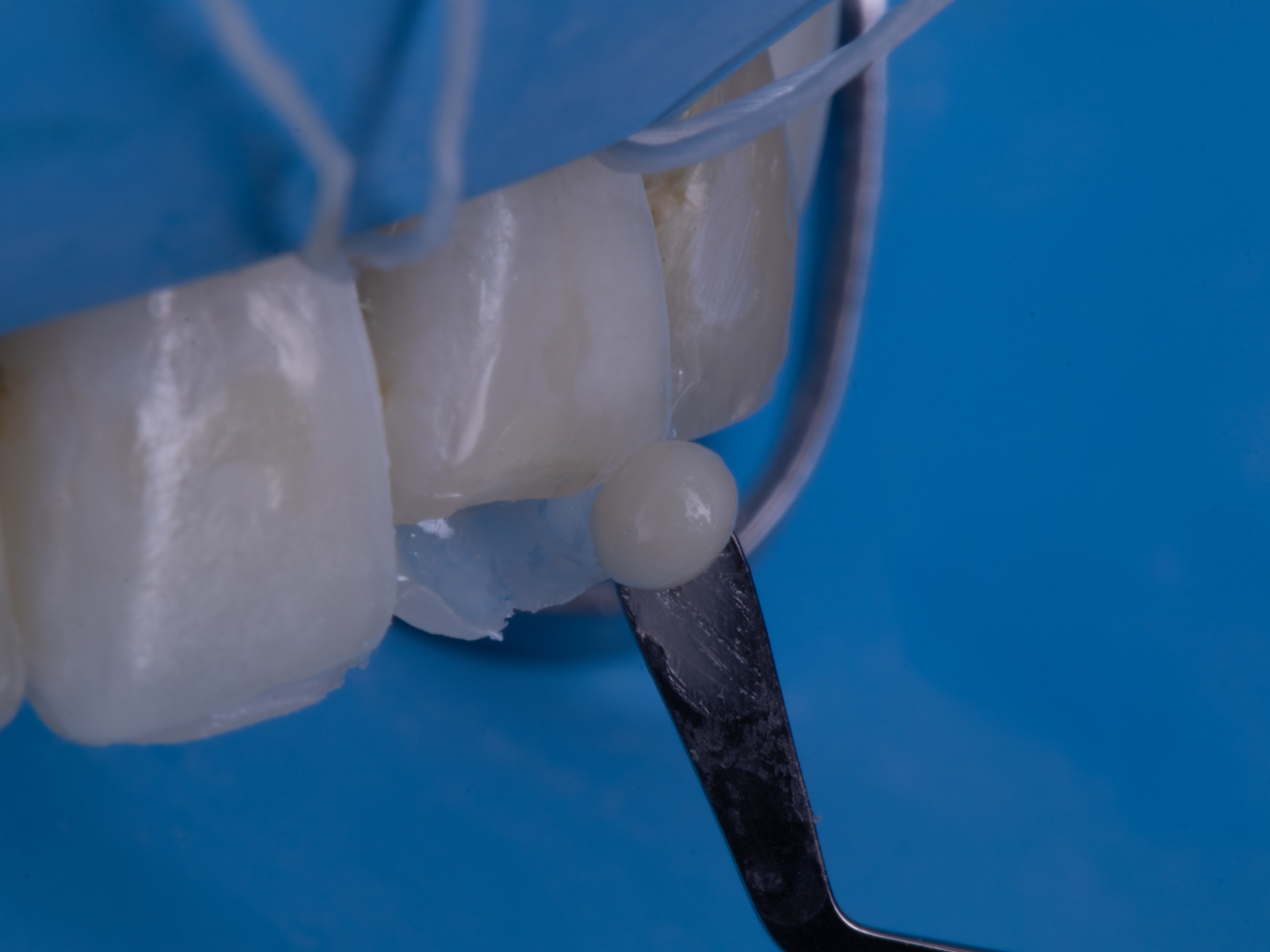
22]. Alternatively, the “button try” technique can also be an excellent option. It consists of placing small amounts of different shades of the resin composite that will be used in the restorative process on the vestibular surface of the tooth to be restored and then, after photopolymerization, the clinician may carefully observe the different shades and choose the best match between the composite and the natural tooth [
22]. Furthermore, it involves analyzing each dental area (cervical, medium, and incisal third) to accurately choose the best color for every specific area [
22]. This technique was the one used in Case 1 and 2 for the authors to achieve the best possible color match in both situations.
Regarding field isolation, the use of a rubber dam is still the gold standard in all dental restorative treatments, since it allows for the ideal conditions for an adhesive approach without any kind of contamination [
1]. It also helps to achieve good gingival retraction, providing better access to the cervical area and permitting, when necessary, composite addition in areas previously occupied by gingival tissue and avoiding the undesirable black triangles [
16]. In both clinical cases (1 and 2), a rubber dam isolation was performed even though, in Case 1, the split dam technique was preferred to allow the correct use of the Unica Anterior matrix since, as previously stated, this matrix needs to be adapted around the tooth, with a perfect fit in the cervical area. To achieve this perfect fit and avoid compromising the correct placement of the composite, the authors chose to use this modified rubber dam isolation technique. Importantly, even though the use of a rubber dam is crucial, its use makes the teeth drier, and it is not possible to accurately evaluate the final esthetic result, since teeth need time to rehydrate. The air that replaces the organic fluids when teeth become drier has a lower refractive index (RI air ≈ 1 < RI organic fluids = 1.33), and the color difference between the natural teeth (RI hydroxyapatite = 1.62) and the restorations becomes more obvious [
24]. That is why the final result should be evaluated at a second appointment. Since patients should schedule this second session to fully evaluate the final integration of the restorations with the natural teeth, the clinician may also use this session to execute the finishing and polishing procedures with more accuracy. Since some direct rehabilitations, such as Cases 1 and 2, are extensive and esthetically challenging, they might benefit from a second appointment to look for aspects that can be improved and that can easily go unnoticed at the time of the restoration since, sometimes, it is a very long and tiring session, and small details might be overlooked. This was the case for both clinical cases, where the finishing and polishing procedures were only performed in a follow-up session. Finishing is related to the contouring, shaping, and smoothing of the restorations to restore anatomical contours and remove any excess material. After finishing, polishing is performed to achieve a surface with high luster and enamel-like texture [
25]. These are important steps in the restorative protocol not only for esthetic reasons but also because the lack of surface smoothness can easily lead to staining, plaque accumulation, gingival irritation, recurrent caries, and tactile perception by the patient [
25]. The main goal is to achieve the smoothest possible surface, since a surface roughness greater than 0.2 μm can not only be perceived by patients, but it is the value below which no further reduction in bacterial accumulation could be expected [
18].
Even though both patients were very pleased with the final results, there were some details that could have been improved. In Case 1, the final smile symmetry might have been further improved, for example, by extending the restorative procedures to both canines and even by considering periodontal surgery on tooth 13 to cover up the gingival recession. However, these features did not oppose a problem to the patients’ notion of an ideal smile, as the main complaint was only focused on central and lateral incisors. Another possible improvement would be the substitution of the conventional diagnostic wax-up (performed by the authors) made for Case 1 for a digital wax-up, as it would be much easier to get a perfect symmetry when comparing to the use of a conventional wax-up. However, a digital wax-up requires additional costs when comparing to the alternative. Finally, Case 2 would probably have benefited from a diagnostic wax-up as was performed for Case 1. It would have made the treatment easier and more predictable. However, since the patient had time limitations, it was not possible to perform it.


 ,
, 
{kind=link}
{kind=link}
{kind=link}

