Straight Leg Raise Test: Influence of Lumbosant© and Assistant Examiner in Hip, Pelvis Tilt and Lumbar Lordosis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Testing Procedure
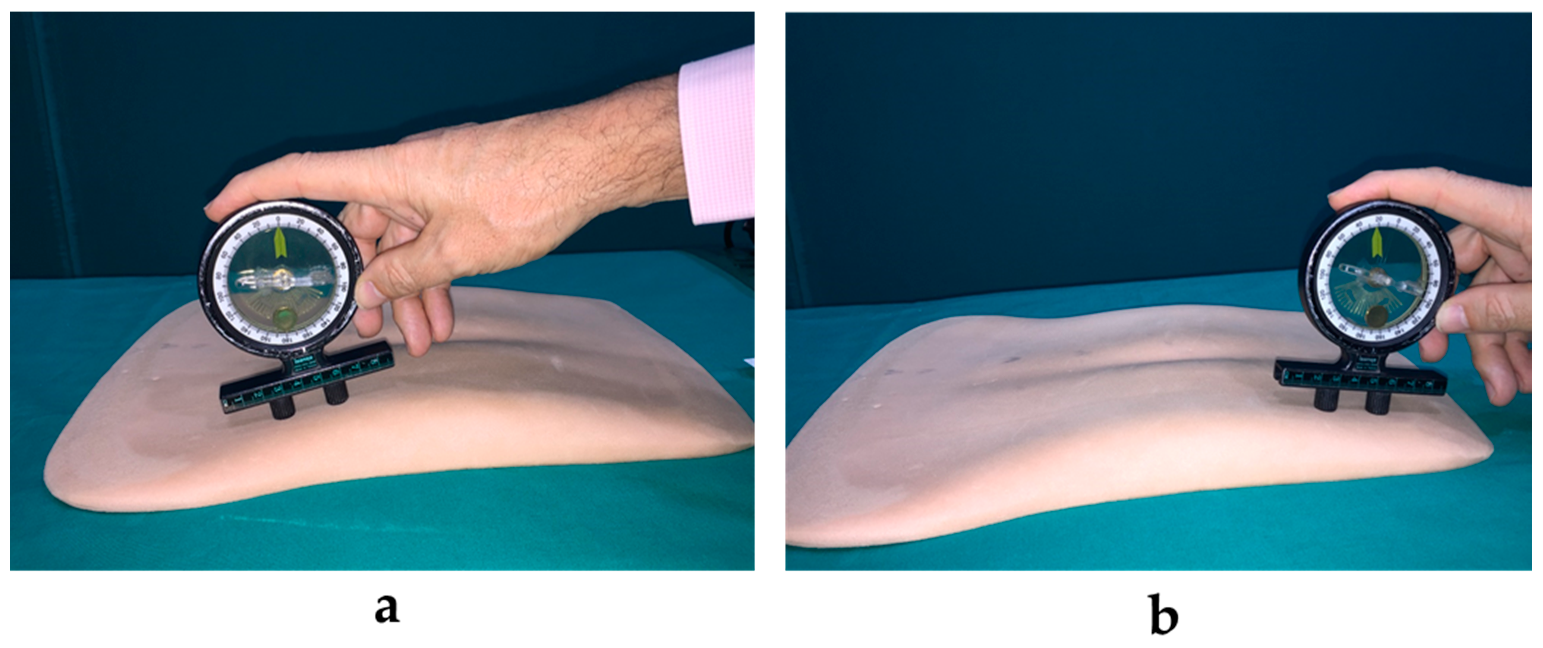
2.2.1. Testing Measurement
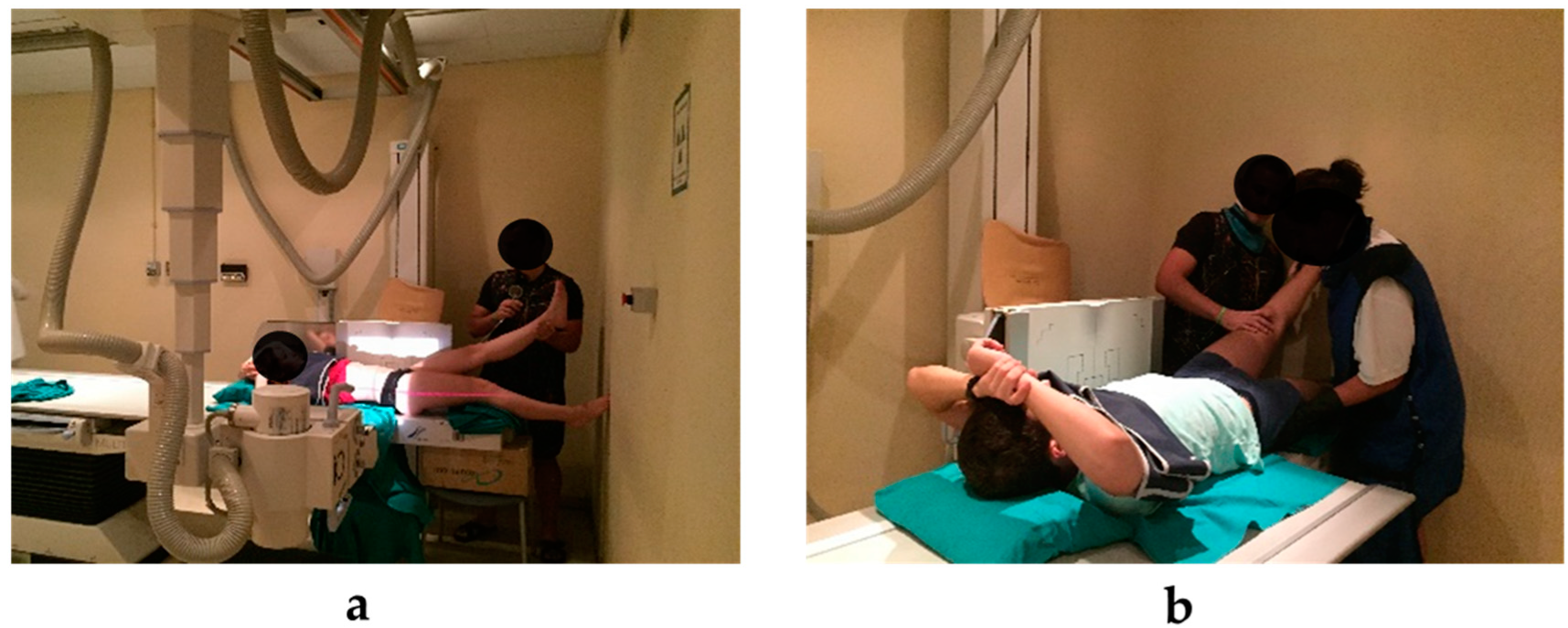
2.2.2. Radiographs. Image Acquisition
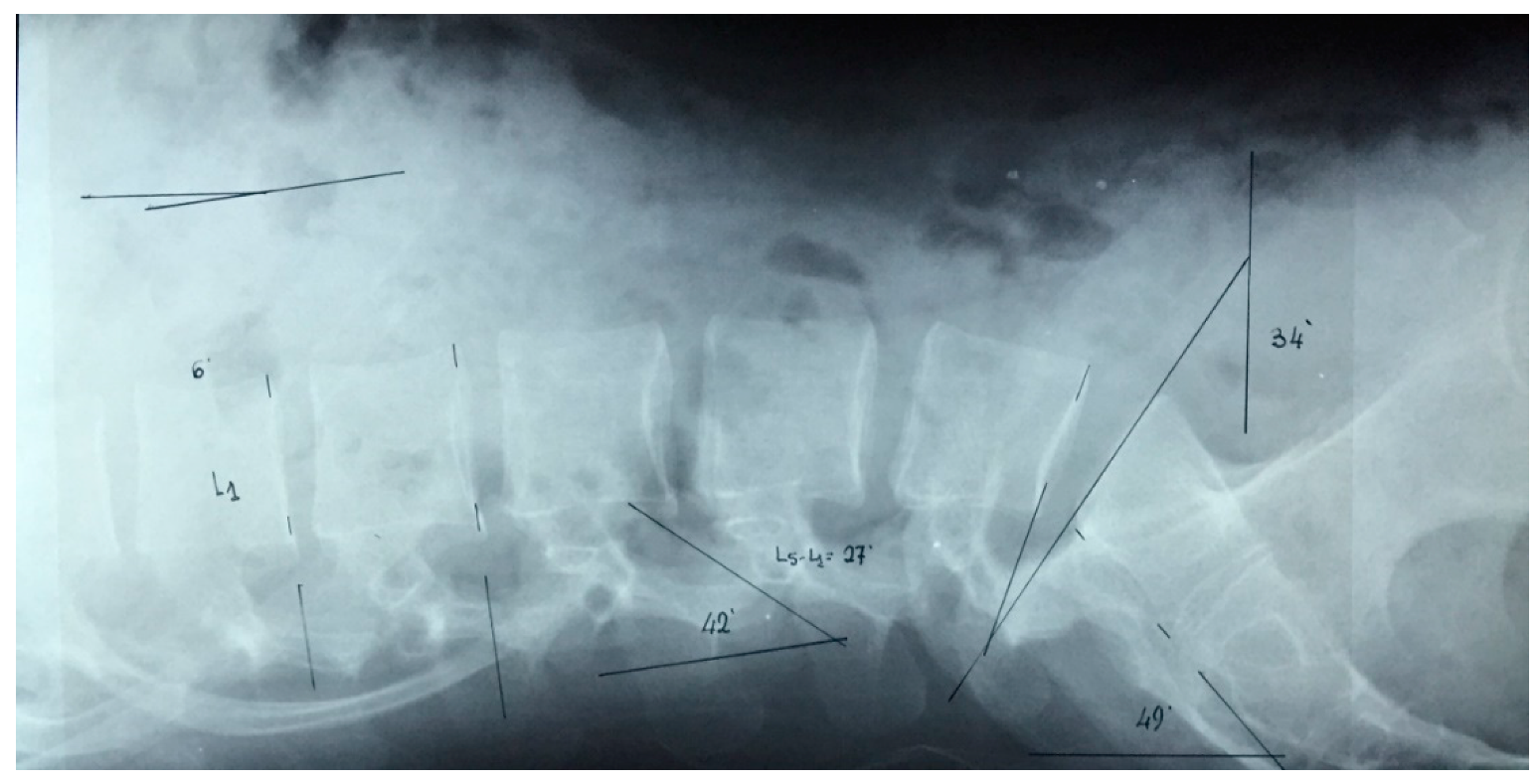
2.2.3. Radiographic Measurement
- ▪
- The pelvic tilt (angle S1): the angle between the vertical and the line connecting the midpoint of the upper plate of S1.
- ▪
- Lumbar lordosis: the angle between the superior sacral plate and the more backward tilted vertebral plate (using the method described by Cobb).
- ▪
- Vertebral wedge angle: The wedge angle is defined as the angle formed between the two lines drawn parallel to the superior and inferior endplates of the vertebra
2.3. Sample Size Calculation
2.4. Statistical analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Whitehead, C.; Hillman, S.; Richardson, A. The Effect of Simulated Hamstring Shortening on Gait in Normal Subjects. Gait Posture 2007, 26, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Laird, R.; Gilbert, J.; Kent, P.; Keating, J. Comparing Lumbo-Pelvic Kinematics in People with and without Back Pain: A Systematic Review and Meta-Analysis. BMC Musculoskelet. Disord. 2014, 15, 229. [Google Scholar] [CrossRef]
- Reis, F.; Macedo, A. Influence of Hamstring Tightness in Pelvic, Lumbar and Trunk Range of Motion in Low Back Pain and Asymptomatic Volunteers during Forward Bending. Asian Spine J. 2015, 9, 535–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zawadka, M.; Skublewska-Paszkowska, M.; Gawda, P.; Lukasik, E.; Smolka, J.; Jablonski, M. What Factors Can Affect Lumbopelvic Flexion-Extension Motion in the Sagittal Plane? A Literature Review. Hum. Mov. Sci. 2018, 58, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Sainz de Baranda, P.; Cejudo, A.; Moreno-Alcaraz, V.; Martinez-Romero, M.; Aparicio-Sarmiento, A.; Santonja, F. Sagittal Spinal Morphotype Assessment in 8 to 15 Years Old Inline Hockey Players. PeerJ 2020, 8, e8229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bado, J.; Barros, P.; Ruiggero, A.; Navillat, M. Análisis Estadístico de La Frecuencia Del “Síndrome de Retracción de Los Isquiotibiales” Estudiado En Colectividades Infantiles Sanas y Su Relación Con El Dorso. An. Fac. Med. Montev. 1964, 49, 328–337. [Google Scholar] [PubMed]
- Santonja, F.; Collazo-Diéguez, M.; Martínez-Romero, M.; Rodríguez-Ferrán, O.; Aparicio-Sarmiento, A.; Cejudo, A.; Andújar, P.; Sainz De Baranda, P. Classification System of the Sagittal Integral Morphotype in Children from the ISQUIOS Programme (Spain). Int. J. Environ. Res. Public Health 2020, 17, 2467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somhegyi, A.; Ratko, I. Hamstring Tightness and Scheuemann’s Disease. Am. J. Phys. Med. Rehabil. 1993, 72, 44. [Google Scholar] [CrossRef]
- Santonja, F.; Ferrer, V.; Martínez, I. Exploración Clínica Del Síndrome de Isquiosurales Cortos. Selección 1995, 4, 81–91. [Google Scholar]
- Ferrer, V. Repercusiones de La Cortedad Isquiosural Sobre La Pelvis y El Raquis Lumbar. Ph.D. Thesis, Universidad de Murcia, Murcia, Spain, September 1998. [Google Scholar]
- Mistry, G.; Vyas, N.; Sheth, M. Comparison of Hamstrings Flexibility in Subjects with Chronic Low Back Pain versus Normal Individuals. J. Clin. Exp. Res. 2014, 2, 85–88. [Google Scholar] [CrossRef] [Green Version]
- Reiman, M.; Weisbach, P.; Glynn, P. The Hip’s Influence on Low Back Pain: A Distal Link to a Proximal Problem. J. Sport Rehabil. 2009, 18, 24–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sainz de Baranda, P.; Cejudo, A.; Martínez-Romero, M.; Aparicio-Sarmiento, A.; Rodríguez-Ferrán, O.; Collazo-Diéguez, M.; Hurtado-Avilés, J.; Andújar, P.; Santonja, F. Sitting Posture, Sagittal Spinal Curvatures and Back Pain in 8 to 12-Year-Old Children from the Region of Murcia (Spain): ISQUIOS Programme. Int. J. Environ. Res. Public Heal. Artic. 2020, 17, 2578. [Google Scholar] [CrossRef] [Green Version]
- Sadler, S.; Spink, M.; Ho, A.; De Jonge, X.; Chuter, V. Restriction in Lateral Bending Range of Motion, Lumbar Lordosis, and Hamstring Flexibility Predicts the Development of Low Back Pain: A Systematic Review of Prospective Cohort Studies. BMC Musculoskelet. Disord. 2017, 18, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croisier, J.; Forthomme, B.; Namurois, M.; Vanderthommen, M.; Crielaard, J. Hamstring Muscle Strain Recurrence and Strength Performance Disorders. Am. J. Sports Med. 2002, 30, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Chumanov, E.; Schache, A.; Heiderscheit, B.; Thelen, D. Hamstrings Are Most Susceptible to Injury during the Late Swing Phase of Sprinting. Br. J. Sports Med. 2012, 46, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opar, D.; Williams, M.; Morgan, D.; Shield, A. Hamstring Strain Injuries: Factors That Lead to Injury and Re-Injury. Sport. Med. 2012, 42, 209–226. [Google Scholar] [CrossRef]
- Bolívar, Y.; Munuera, P. Relationship Between Tightness of the Posterior Muscles of the Lower Limb and Plantar Fasciitis. Foot Ankle Int. 2013, 34, 42–48. [Google Scholar] [CrossRef]
- Witvrouw, E.; Bellemans, J.; Lysens, R.; Danneels, L.; Cambier, D. Intrinsic Risk Factors for the Development of Patellar Tendinitis in an Athletic Population. Am. J. Sports Med. 2001, 29, 190–195. [Google Scholar] [CrossRef]
- Witvrouw, E.; Van Tiggelen, D.; Willems, T. Risk Factors and Prevention of Anterior Knee Pain. In Anterior Knee Pain and Patellar Instability; Springer: London, UK, 2006. [Google Scholar]
- Stutchfield, B.; Coleman, S. The Relationships between Hamstring Flexibility, Lumbar Flexion, and Low Back Pain in Rowers. Eur. J. Sport Sci. 2006, 6, 255–260. [Google Scholar] [CrossRef]
- Biering-Sorensen, F. A One-Year Prospective Study of Low Back Trouble in a General Population: The Prognostic Value of Low Back History and Physical Measurements. Dan. Med. Bull. 1984, 31, 362–375. [Google Scholar]
- McGill, S. Low Back Disorders: Evidence-Based Prevention and Rehabilitation; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Standaert, C.; Herring, S. Spondylolysis: A Critical Review. Br. J. Sports Med. 2000, 34, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Mase, Y.; Sairyo, K. Active Stretching for Lower Extremity Muscle Tightness in Pediatric Patients with Lumbar Spondylolysis. J. Med. Investig. 2017, 64, 136–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brodersen, A.; Pedersen, B.; Reimers, J. Incidence of Complaints about Heel-, Knee-and Back-Related Discomfort among Danish Children, Possible Relation to Short Muscles. Ugeskr. Laeger 1994, 156, 2243–2245. [Google Scholar]
- Zhu, Q.; Gu, R.; Yang, X.; Lin, Y.; Gao, Z.; Tanaka, Y. Adolescent Lumbar Disc Herniation and Hamstring Tightness: Review of 16 Cases. Spine (Phila. Pa. 1976) 2006, 31, 1810–1814. [Google Scholar] [CrossRef]
- Perret, C.; Poiraudeau, S.; Fermanian, J.; Colau, M.; Benhamou, M.; Revel, M. Validity, Reliability, and Responsiveness of the Fingertip-to-Floor Test. Arch. Phys. Med. Rehabil. 2001, 82, 1566–1570. [Google Scholar] [CrossRef]
- Gogia, P.; Braatz, J.; Rose, S.; Norton, B. Reliability and Validity of Goniometric Measurements at the Knee. Phys. Ther. 1987, 67, 192–195. [Google Scholar] [CrossRef]
- Cejudo, A.; Sainz de Baranda, P.; Ayala, F.; Santonja, F. Test-Retest Reliability of Seven Common Clinical Tests for Assessing Lower Extremity Muscle Flexibility in Futsal and Handball Players. Phys. Ther. Sport 2015, 16, 107–113. [Google Scholar] [CrossRef]
- Ayala, F.; Sainz de Baranda, P.; De Ste Croix, M.; Santonja, F. Absolute Reliability of Five Clinical Tests for Assessing Hamstring Flexibility in Professional Futsal Players. J. Sci. Med. Sport 2012, 15, 142–147. [Google Scholar] [CrossRef]
- Moreno-Alcaraz, V.; Cejudo, A.; Sainz de Baranda, P. Injury Types and Frequency in Spanish Inline Hockey Players. Phys. Ther. Sport 2020, 42, 91–99. [Google Scholar] [CrossRef]
- Sainz de Baranda, P.; Rodríguez-Iniesta, M.; Ayala, F.; Santonja, F.; Cejudo, A. Determination of the Criterion-Related Validity of Hip Joint Angle Test for Estimating Hamstring Flexibility Using a Contemporary Statistical Approach. Clin. Sports Med. 2014, 24, 320–325. [Google Scholar] [CrossRef]
- Santonja, F.; Sainz De Baranda, P.; García, P.; López-Miñarro, P.; Jordana, M. Effects of Frequency of Static Stretching on Straight-Leg Raise in Elementary School Children. J. Sport. Med. Phys. Fit. 2007, 47, 304–308. [Google Scholar]
- Fasuyi, F.; Fabunmi, A.; Adegoke, B. Hamstring Muscle Length and Pelvic Tilt Range among Individuals with and without Low Back Pain. J. Bodyw. Mov. Ther. 2017, 21, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Alshammari, F.; Alzoghbieh, E.; Abu Kabar, M.; Hawamdeh, M. A Novel Approach to Improve Hamstring Flexibility: A Single-Blinded Randomised Clinical Trial. S. Afr. J. Physiother. 2019, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bierma-Zeinstra, S.; Van Gool, J.; Bernsen, R.; Njoo, K. Measuring the Sacral Inclination Angle in Clinical Practice: Is There an Alternative to Radiographs? J. Manip. Physiol. Ther. 2001, 24, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.; Gajdosik, R.; LeVeau, B. Relationship of Pelvic and Thigh Motions During Unilateral and Bilateral Hip Flexion. Phys. Ther. 1985, 65, 1501–1504. [Google Scholar] [CrossRef]
- Park, K.; Ha, S.; Kim, S.; Park, K.; Kwon, O.; Oh, J. Effects of the Pelvic Rotatory Control Method on Abdominal Muscle Activity and the Pelvic Rotation during Active Straight Leg Raising. Man. Ther. 2013, 18, 220–224. [Google Scholar] [CrossRef]
- Palmer, M.; Epler, M. Fundamentos de Las Técnicas de Evaluación Musculoesquelética; Paidotribo: Barcelona, Spain, 2002. [Google Scholar]
- Peterson, F.; Kendall, E.; Geise, P. Kendall’s Músculos. Pruebas, Funciones y Dolor Postural; Marbán: Madrid, Spain, 2005. [Google Scholar]
- Cejudo, A.; Robles-Palazón, F.; Ayala, F.; De Ste Croix, M.; Ortega-Toro, E.; Santonja, F.; Sainz de Baranda, P. Age-Related Differences in Flexibility in Soccer Players 8-19 Years Old. PeerJ 2019, 2019, e6236. [Google Scholar] [CrossRef]
- Reese, N.; Bandy, W. Use of an Inclinometer to Measure Flexibility of the Iliotibial Band Using the Ober Test and the Modified Ober Test: Differences in Magnitude and Reliability of Measurements. J. Orthop. Sports Phys. Ther. 2003, 33, 326–330. [Google Scholar] [CrossRef] [Green Version]
- Muir, S.; Corea, C.; Beaupre, L. Evaluating Change in Clinical Status: Reliability and Measures of Agreement for the Assessment of Glenohumeral Range of Motion. North Am. J. Sport. Phys. Ther. NAJSPT 2010, 5, 98. [Google Scholar]
- Ayala, F.; Moreno-Perez, V.; Vera-Garcia, F.; Moya, M.; Sanz-Rivas, D.; Fernandez-Fernandez, J. Acute and Time-Course Effects of Traditional and Dynamic Warm-up Routines in Young Elite Junior Tennis Players. PLoS ONE 2016, 11, e0152790. [Google Scholar] [CrossRef] [Green Version]
- Gerhardt, J.; Cocchiarella, L.; Lea, R. The Practical Guide to Range of Motion Assessment; American Medical Association: Chicago, IL, USA, 2002. [Google Scholar]
- Boland, R.; Adams, R. Effects of Ankle Dorsiflexion on Range and Reliability of Straight Leg Raising. Aust. J. Physiother. 2000, 46, 191–200. [Google Scholar] [CrossRef] [Green Version]
- Cejudo, A.; Robles-Palazón, F.; Sainz De Baranda, P. Fútbol Sala de Élite: Diferencias de Flexibilidad Según Sexo. E-Balonmano.com Rev. Ciencias Deport. 2019, 15, 37–48. [Google Scholar]
- Reese, N.; Bandy, W. Joint Range of Motion and Muscle Length Testing-E-Book; Elsevier Health Sciences: St. Louis, MO, USA, 2016. [Google Scholar]
- Cobb, J. Outline for the Study of Scoliosis. Instr. Course Lect. AAOS 1948, 5, 261–275. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Method. 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sport. Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R. Cinematographic Analysis of the Passive Straight-Leg-Raising Test for Hamstring Muscle Length. Phys. Ther. 1982, 62, 1269–1274. [Google Scholar] [CrossRef]
- Bohannon, R.; Gajdosik, R.; Leveau, B. Contribution of Pelvic and Lower Limb Motion to Increases in the Angle of Passive Straight Leg Raising. Phys. Ther. 1985, 65, 474–476. [Google Scholar] [CrossRef]
- Milne, R.; Mierau, D. Hamstring Distensibility in the General Population: Relationship to Pelvic and Back Stresses. J. Manip. Physiol. Ther. 1979, 2, 146–150. [Google Scholar]
- Ekstrand, J.; Wiktorsson, M.; Oberg, B.; Gillquist, J. Lower Extremity Goniometric Measurements: A Study to Determine Their Reliability. Arch. Phys. Med. Rehabil. 1982, 63, 171–175. [Google Scholar]
- Cameron, D.; Bohannon, R.; Owen, S. Influence of Hip Position on Measurements of the Straight Leg Raise Test. J. Orthop. Sports Phys. Ther. 1994, 19, 168–172. [Google Scholar] [CrossRef] [Green Version]
- Gajdosik, R.; Rieck, M.; Sullivan, D.; Wightman, S. Comparison of Four Clinical Tests for Assessing Hamstring Muscle Length. J. Orthop. Sports Phys. Ther. 1993, 18, 614–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisk, J. The Passive Hamstring Stretch Test: Clinical Evaluation. N. Z. Med. J. 1979, 89, 209–211. [Google Scholar] [PubMed]
- Kuo, L.; Chung, W.; Bates, E. The Hamstring Index. J. Pediatr. Orthop. 1997, 17, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Roy, P.; Hebbelinck, M.; Borms, J. Introduction d’un Goniomètre Standard Modifié Avec La Graduation et La Branche Pivotante Montées Sur Un Chariot Déplaçable. Ann. Kinésithérapie 1985, 12, 255–259. [Google Scholar]
- Youdas, J.; Krause, D.; Hollman, J.; Harmsen, W.; Laskowski, E. The Influence of Gender and Age on Hamstring Muscle Length in Healthy Adults. J. Orthop. Sports Phys. Ther. 2005, 35, 246–252. [Google Scholar] [CrossRef]
- Fredriksen, H.; Dagfinrud, H.; Jacobsen, V.; Maehlum, S. Passive Knee Extension Test to Measure Hamstring Muscle Tightness. Scand. J. Med. Sci. Sports 1997, 7, 279–282. [Google Scholar] [CrossRef]
- Wehrenberg, W.; Costello, M. Clinical Evaluation of the BackMate Lower Lumbar Rehabilitation System: Results of a Preliminary Study. J. Orthop. Sports Phys. Ther. 1993, 17, 185–190. [Google Scholar] [CrossRef] [Green Version]
- Enwemeka, C. Radiographic Verification of Knee Goniometry. Scand. J. Rehabil. Med. 1986, 18, 47–49. [Google Scholar]
- Castro-Pinero, J.; Chillon, P.; Ortega, F.; Montesinos, J.; Sjostrom, M.; Ruiz, J. Criterion-Related Validity of Sit-and-Reach and Modified Sit-and-Reach Test for Estimating Hamstring Flexibility in Children and Adolescents Aged 6–17 Years. Int. J. Sports Med. 2009, 30, 658–662. [Google Scholar] [CrossRef]
- Muyor, J.; Arrabal-Campos, F. Effects of Acute Fatigue of the Hip Flexor Muscles on Hamstring Muscle Extensibility. J. Hum. Kinet. 2016, 53, 23–31. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male (n = 10) | Female (n = 13) | Total (n = 23) | ||
|---|---|---|---|---|
| Age (years) | 23.80 ± 1.55 | 23.38 ± 1.71 | 23.57 ± 1.62 | |
| Body mass (kg)* | 77.00 ± 11.28 | 61.22 ± 11.79 | 68.08 ± 13.85 | |
| Height (m)* | 1.73 ± 0.06 | 1.66 ± 0.07 | 1.69 ± 0.07 | |
| BMI (kg/m2)* | 25.66 ± 3.72 | 20.19 ± 6.96 | 22.57 ± 6.31 | |
| I | T_PSLR (degrees) * | 79.4 ± 11.2 | 96.8 ± 23.6 | 89.2 ± 20.8 |
| N_PSLR (degrees) * | 68.0 ± 11.0 | 80.9 ± 14.5 | 75.3 ± 14.4 | |
| Rx | PT _ neutral position (degrees) | 44.1 ± 11.6 | 40.7 ± 8.0 | 42.2 ± 9.6 |
| PT _ T_PSLR (degrees) | 17.7 ± 11.7 | 19.5 ± 7.9 | 18.7 ± 9.5 | |
| PT _ N_PSLR (degrees) | 27.5 ± 11.5 | 27.5 ± 5.9 | 27.5 ± 8.5 | |
| LL _ neutral position (degrees) | 57.6 ± 15.6 | 58.5 ± 12.9 | 58.1 ± 13.8 | |
| LL_ T_PSLR (degrees) | 24.7 ± 13.3 | 28.5 ± 12.1 | 26.8 ± 12.5 | |
| LL_ N_PSLR (degrees) | 38.4 ± 16.8 | 39.0 ± 8.7 | 38.7 ± 12.5 |
| T_PSLR | N_PSLR | Difference Average | p-Value | d-Value (Qualitative Inference) | |
|---|---|---|---|---|---|
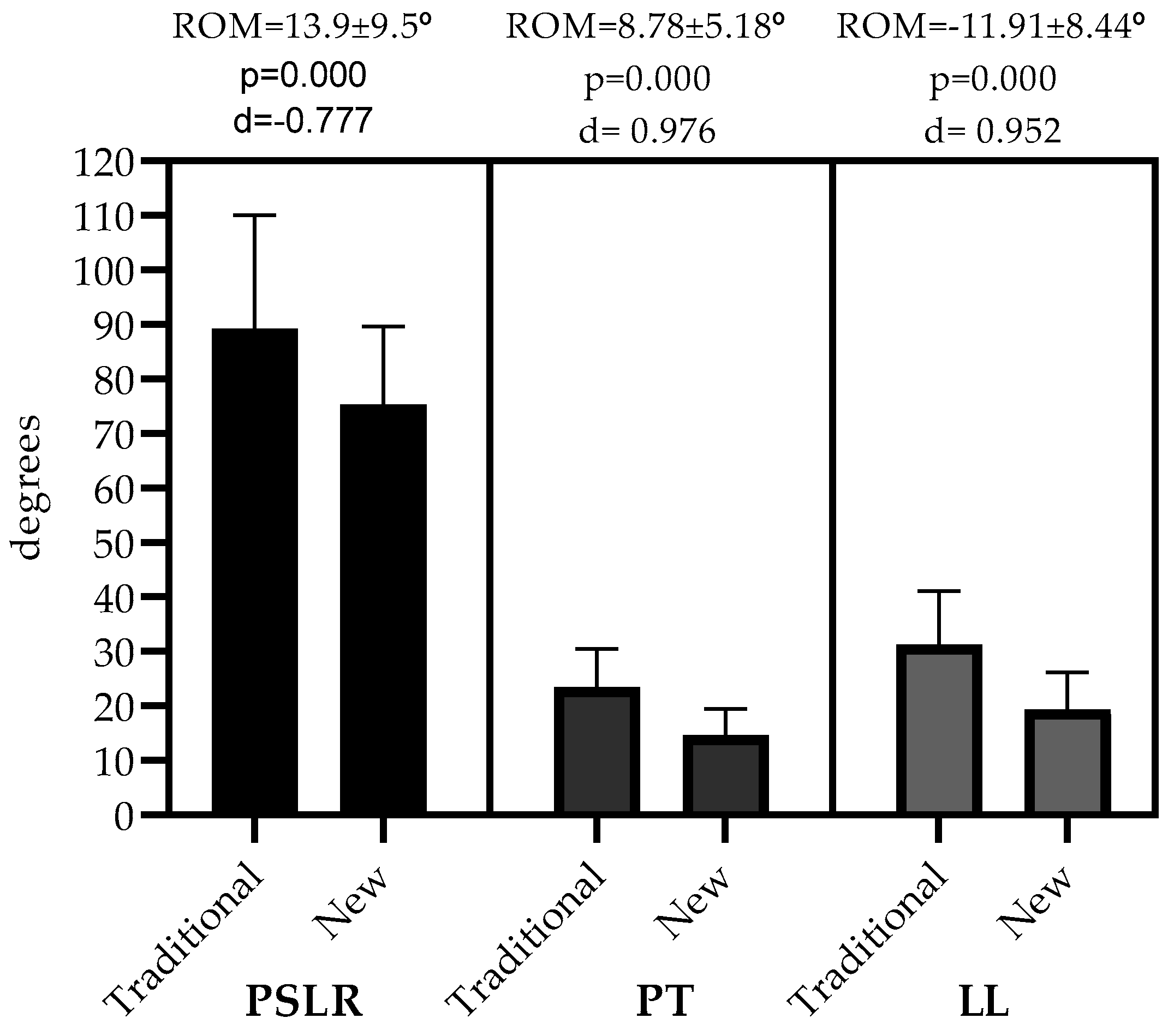
| PSLR (° *) | 89.2 ± 20.8 | 75.3 ± 14.4 | 13.9 ± 9.5 | 0.000 | Moderate (d = −0.777) |
| PT _ neutral position (°) | 42.2 ± 9.6 | 42.2 ± 9.6 | |||
| PT _ PSLR (°) * | 18.7 ± 9.5 | 27.5 ± 8.5 | 8.78 ± 5.18 | 0.000 | Moderate (d = 0.976) |
| LL _ neutral position (°) | 58.1 ± 13.8 | 58.1 ± 13.8 | |||
| LL_ PSLR (°) * | 26.8 ± 12.5 | 38.7 ± 12.5 | −11.91 ± 8.44 | 0.000 | Moderate (d = 0.952) |
| T_PSLR | N_PSLR | Difference Average | p-Value | Qualitative Inference | |
|---|---|---|---|---|---|
| PSLR (degrees) * | 79.4 ± 11.2 | 68.0 ± 11.0 | 11.4 ± 6.3 | 0.005 | Moderate (d = −1.027) |
| PT _ neutral position (degrees) | 44.1 ± 11.6 | ||||
| PT _ PSLR (degrees) * | 17.7 ± 11.7 | 27.5 ± 11.5 | 9.80 ± 5.0 | 0.005 | Moderate (d = 0.845) |
| LL _ neutral position (degrees) | 57.6 ± 15.6 | ||||
| LL_ PSLR (degrees) * | 24.7 ± 13.3 | 38.4 ± 16.8 | -13.7 ± 9.4 | 0.005 | Moderate (d = 0.904) |
| T_PSLR | N_PSLR | Difference Average | p-Value | Qualitative Inference | |
|---|---|---|---|---|---|
| PSLR (degrees) * | 96.8 ± 23.6 | 80.9 ± 14.5 | 15.8 ± 11.2 | 0.001 | Moderate (d = −0.812) |
| PT _ neutral position (degrees) | 40.7 ± 8.0 | ||||
| PT _ PSLR (degrees) * | 19.5 ± 7.9 | 27.5 ± 5.9 | 8.00 ± 5.4 | 0.003 | Moderate (d = 1.147) |
| LL _ neutral position (degrees) | 58.5 ± 12.9 | ||||
| LL_ PSLR (degrees) * | 28.5 ± 12.1 | 39.0 ± 8.7 | −10.5 ± 7.7 | 0.002 | Moderate (d = 0.996) |
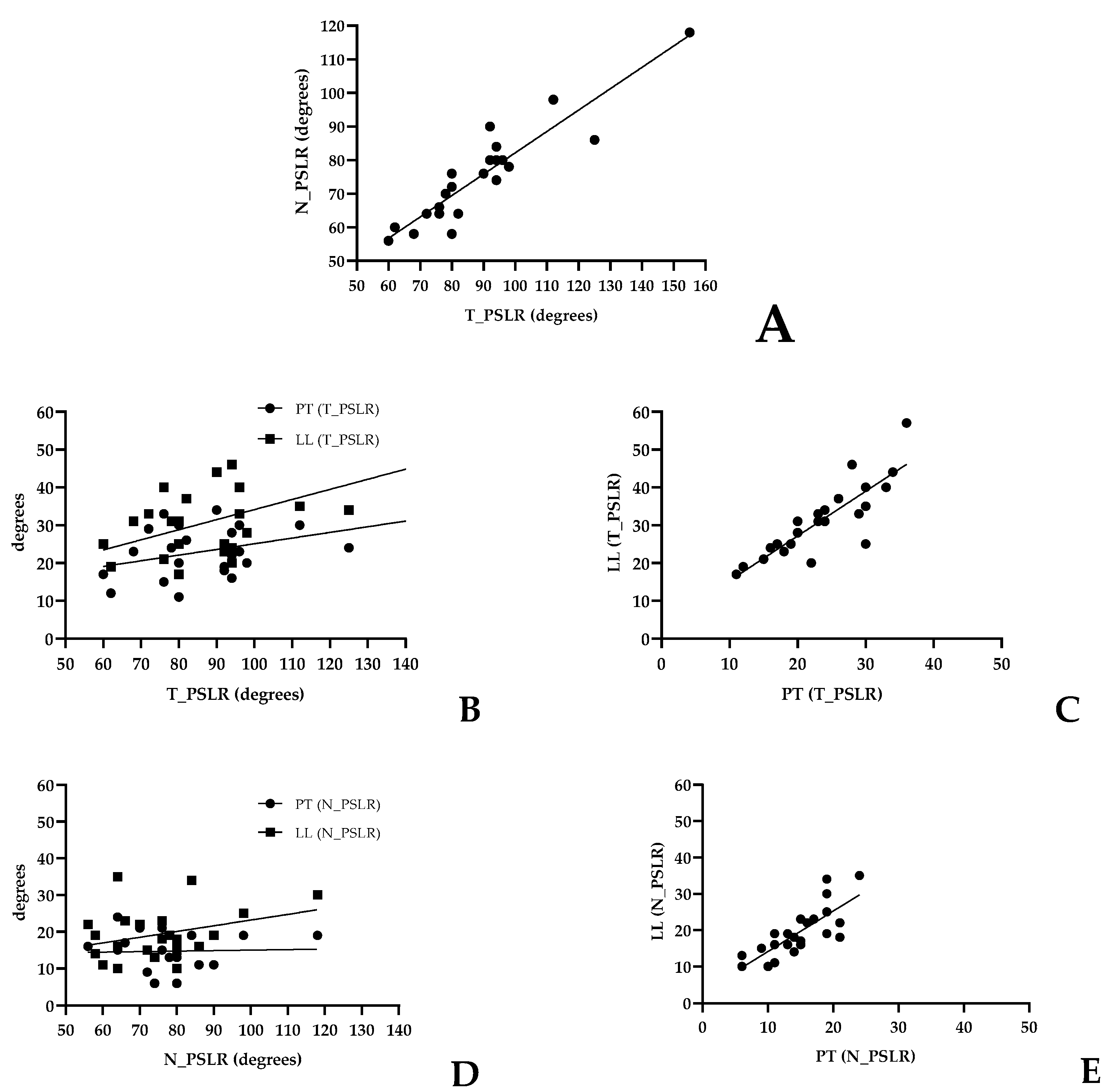
| Tests | Correlation | 90% CI | p Value | Descriptor | R2 | Regression Equation | |||
|---|---|---|---|---|---|---|---|---|---|
| T_PSLR | N_PSLR | 0.877 | 0.704 | to | 0.956 | 0.000 | Very large | 0.8445 | T_PSLR= 18.53 + 0.6363*N_PSLR |
| T_PSLR | PT (T_PSLR) | 0.324 | 0.160 | to | 0.659 | 0.132 | Small | 0.1987 | T_PSLR = 10.09 + 0.1501*PT_T_PSLR |
| LL (T_PSLR) | 0.382 | 0.046 | to | 0.672 | 0.072 | Small | 0.3236 | T_PSLR = 7.457 + −0.2668*LL_T_PSLR | |
| PT vs. LL (T_PSLR) | 0.863 | 0.648 | to | 0.975 | 0.000 | Very large | 0.7206 | LL_T_PSLR= 3.504 + 1.182*PT_T_PSLR | |
| N_PSLR | PT (N_PSLR) | −0.059 | 0.467 | to | 0.332 | 0.788 | Small | 0.0017 | N_PSLR = 13.65 + 0.01385*PT_N_PSLR |
| LL (N_PSLR) | 0.236 | 0.234 | to | 0.625 | 0.279 | Moderate | 0.1082 | N_PSLR = 7.622 + 0.1557*LL_N_PSLR | |
| PT vs. LL (N_PSLR) | 0.801 | 0.543 | to | 0.916 | 0.000 | Very large | 0.6075 | LL_N_PSLR= 2.993 + 1.113*PT_N_PSLR | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santonja-Medina, F.; Santonja-Renedo, S.; Cejudo, A.; Ayala, F.; Ferrer, V.; Pastor, A.; Collazo-Diéguez, M.; Rodríguez-Ferrán, O.; Andújar, P.; Sainz de Baranda, P. Straight Leg Raise Test: Influence of Lumbosant© and Assistant Examiner in Hip, Pelvis Tilt and Lumbar Lordosis. Symmetry 2020, 12, 927. https://doi.org/10.3390/sym12060927
Santonja-Medina F, Santonja-Renedo S, Cejudo A, Ayala F, Ferrer V, Pastor A, Collazo-Diéguez M, Rodríguez-Ferrán O, Andújar P, Sainz de Baranda P. Straight Leg Raise Test: Influence of Lumbosant© and Assistant Examiner in Hip, Pelvis Tilt and Lumbar Lordosis. Symmetry. 2020; 12(6):927. https://doi.org/10.3390/sym12060927
Chicago/Turabian StyleSantonja-Medina, Fernando, Sara Santonja-Renedo, Antonio Cejudo, Francisco Ayala, Vicente Ferrer, Antonio Pastor, Mónica Collazo-Diéguez, Olga Rodríguez-Ferrán, Pilar Andújar, and Pilar Sainz de Baranda. 2020. "Straight Leg Raise Test: Influence of Lumbosant© and Assistant Examiner in Hip, Pelvis Tilt and Lumbar Lordosis" Symmetry 12, no. 6: 927. https://doi.org/10.3390/sym12060927