Fuzzy-Based Symmetrical Multi-Criteria Decision-Making Procedure for Evaluating the Impact of Harmful Factors of Healthcare Information Security

 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
1.1. Past Research Initiatives
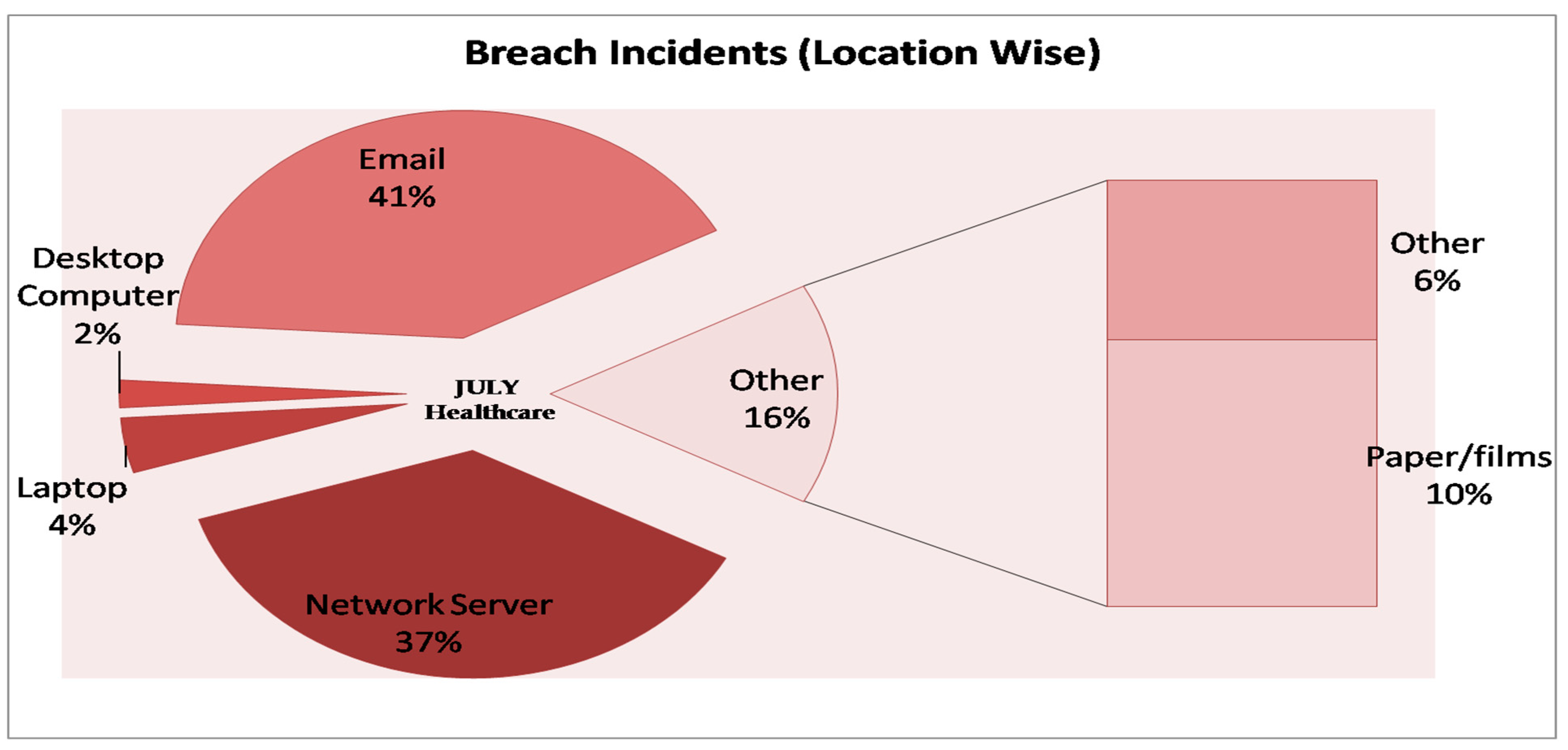
1.2. Previous Attack Trends on Healthcare
2. Materials and Methods
2.1. Classical Layered Healthcare Model: Information Perspective
2.2. Various Factors: Affecting Healthcare Data Security
2.3. Methodology
3. Data Analysis and Results
3.1. Sensitivity Analysis
3.2. Comparison with the Classical AHP-TOPSIS Method
4. Discussion
- Results of the proposed study will provide a constructive and a secure path for the experts and researchers to prepare their prevention strategies according to the evaluated result.
- Results of the proposed paper will help the experts in enhancing the current security scenario of healthcare information security by providing a scientifically evaluated priority list of affecting factors. An expert can use that result and enhance the security by preventing the factors one by one according to the results.
- The most prioritized factor is the Human Error in evaluated results, this type of evaluation attempts to draw the attention of experts and researchers on the factor and thus create future research possibilities for them.
- Contributors of this study have found six factors that affect the healthcare information security on various layers. By adopting this assessment, the future researchers can assess the web application security affecting factors and evaluate their respective weights.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pandey, A.K.; Tripathi, A.K.; Kapil, G.; Singh, V.; Khan, M.W.; Agrawal, A.; Kumar, R.; Khan, R.A. Trends in Malware Attacks. In Critical Concepts, Standards, and Techniques in Cyber Forensics; IGI Global: Hershey, PA, USA, 2020; pp. 47–60. [Google Scholar] [CrossRef]
- Appari, A.; Johnson, M.E. Information security and privacy in healthcare: Current state of research. Int. J. Internet Enterp. Manag. 2010, 6, 279. [Google Scholar] [CrossRef]
- Kruse, C.; Smith, B.; Vanderlinden, H.; Nealand, A. Security Techniques for the Electronic Health Records. J. Med. Syst. 2017, 41, 127. [Google Scholar] [CrossRef] [Green Version]
- Slamanig, D.; Stingl, C. The Degree of Privacy in Web-based Electronic Health Records. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering, Seoul, Korea, 27 August–1 Septmber 2006; Springer: Berlin/Heidelberg, Germany, 2009; Volume 22, pp. 974–977. [Google Scholar]
- Toll, E.T.; A Alkureishi, M.; Lee, W.W.; Babbott, S.F.; A Bain, P.; Beasley, J.W.; Frankel, R.M.; A Loveys, A.; Wald, H.S.; Woods, S.S.; et al. Protecting healing relationships in the age of electronic health records: Report from an international conference. JAMIA Open 2019, 2, 282–290. [Google Scholar] [CrossRef]
- Al-Zubaidie, M.; Zhang, Z.; Zhang, J. PAX: Using Pseudonymization and Anonymization to Protect Patients’ Identities and Data in the Healthcare System. Int. J. Environ. Res. Public Health 2019, 16, 1490. [Google Scholar] [CrossRef] [Green Version]
- Señor, I.C.; Fernández-Alemán, J.L.; Toval, A. Usable Privacy and Security in Personal Health Records. In Computer Vision; Springer: Berlin/Heidelberg, Germany, 2011; Volume 6949, pp. 36–43. [Google Scholar] [CrossRef]
- Thigpen, B.L. Strategies to Lower Security Risks Involving Medical Devices in Patient Care. 2020. Available online: https://scholarworks.waldenu.edu/cgi/viewcontent.cgi?article=9698&context=dissertations (accessed on 15 February 2020).
- Ronquillo, J.G.; Winterholler, J.E.; Cwikla, K.; Szymanski, R.; Levy, C. Health IT, hacking, and cybersecurity: National trends in data breaches of protected health information. JAMIA Open 2018, 1, 15–19. [Google Scholar] [CrossRef]
- Hai, N.K.; Lawpoolsri, S.; Jittamala, P.; Huong, P.T.T.; Kaewkungwal, J. Practices in security and confidentiality of HIV/AIDS patients’ information: A national survey among staff at HIV outpatient clinics in Vietnam. PLoS ONE 2017, 12, e0188160. [Google Scholar] [CrossRef]
- Sahu, K.; Srivastava, R.K. Needs and Importance of Reliability Prediction: An Industrial Perspective. Inf. Sci. Lett. Natural Sci. Publ. 2020, 9, 33–37. [Google Scholar]
- Peikari, H.R.; Ramayah, T.; Shah, M.H.; Lo, M.C. Patients’ perception of the information security management in health centers: The role of organizational and human factors. BMC Med. Inform. Decis. Mak. 2018, 18, 102. [Google Scholar] [CrossRef]
- Lyon, A.R.; Lewis, C.C.; Melvin, A.; Boyd, M.; Nicodimos, S.; Liu, F.F.; Jungbluth, N. Health Information Technologies—Academic and Commercial Evaluation (HIT-ACE) methodology: Description and application to clinical feedback systems. Implement Sci. 2015, 11, 128. [Google Scholar] [CrossRef] [Green Version]
- Sahu, K.; Srivastava, R.K. Revisiting Software Reliability. In Advances in Intelligent Systems and Computing; Springer: Berlin/Heidelberg, Germany, 2018; pp. 221–235. [Google Scholar] [CrossRef]
- Yeratziotis, A.; Pottas, D.; Van Greunen, D. A Usable Security Heuristic Evaluation for the Online Health Social Networking Paradigm. Int. J. Hum.-Comput. Interact. 2012, 28, 678–694. [Google Scholar] [CrossRef]
- Sahu, K.; Rajshree, P.; Kumar, R. Risk management perspective in SDLC. Int. J. Adv. Res. Comput. Sci. Softw. Eng. 2014, 4, 1247–1251. [Google Scholar]
- Kumar, R.; Khan, A.I.; Abushark, Y.B.; Alam, M.; Agrawal, A.; Khan, R.A. A Knowledge-Based Integrated System of Hesitant Fuzzy Set, AHP and TOPSIS for Evaluating Security-Durability of Web Applications. IEEE Access 2020, 8, 48870–48885. [Google Scholar] [CrossRef]
- Kumar, R.; Khan, A.I.; Abushark, Y.B.; Alam, M.; Agrawal, A.; Khan, R.A. An Integrated Approach of Fuzzy Logic, AHP and TOPSIS for Estimating Usable-Security of Web Applications. IEEE Access 2020, 8, 50944–50957. [Google Scholar] [CrossRef]
- Teles, S.; Napolskij, M.S.; Paúl, C.; Ferreira, A.; Seeher, K. Training and support for caregivers of people with dementia: The process of culturally adapting the World Health Organization iSupportprogramme to Portugal. Dementia. Dementia 2020. [Google Scholar] [CrossRef]
- Kumar, R.; Zarour, M.; Alenezi, M.; Agrawal, A.; Khan, R.A. Measuring Security Durability of Software through Fuzzy-Based Decision-Making Process. Int. J. Comput. Intell. Syst. 2019, 12, 627–642. [Google Scholar] [CrossRef] [Green Version]
- Peng, P. A Measurement Approach to Understanding the Data Flow of Phishing from Attacker and Defender Perspectives (Doctoral Dissertation, Virginia Tech). 2019. Available online: https://vtechworks.lib.vt.edu/bitstream/handle/10919/96401/Peng_P_T_2020.pdf?sequence=1&isAllowed=y (accessed on 22 March 2020).
- Park, E.H.; Kim, J.; Wiles, L.L.; Park, Y.S.; Wile, L.L. Factors affecting intention to disclose patients’ health information. Comput. Secur. 2019, 87, 101340. [Google Scholar] [CrossRef]
- Kessler, S.R.; Pindek, S.; Kleinman, G.; A Andel, S.; Spector, P.E. Information security climate and the assessment of information security risk among healthcare employees. Heal. Inform. J. 2019. [Google Scholar] [CrossRef]
- Alipour, J.; Mehdipour, Y.; Karimi, A. Factors Affecting Acceptance of Hospital Information Systems in Public Hospitals of Zahedan University of Medical Sciences: A Cross-Sectional Study. J. Med. Life 2020, 12, 403–410. [Google Scholar]
- Shirdeli, M.; Zare, S.; Kharazmi, E.; Rezaee, R.; Maher, M.H. Presenting a Model to Evaluate Factors Affecting Outsourcing of Health Information Technology Services. Acta Inform. Medica 2018, 26, 190–194. [Google Scholar] [CrossRef]
- McLeod, A.; Dolezel, D. Cyber-analytics: Modeling factors associated with healthcare data breaches. Decis. Support Syst. 2018, 108, 57–68. [Google Scholar] [CrossRef]
- Priestman, W.; Anstis, T.; Sebire, I.G.; Sridharan, S.; Sebire, N.J. Phishing in healthcare organisations: Threats, mitigation and approaches. BMJ Health Care Inform. 2019, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healthcare Data Breach Statistics. Available online: https://www.hipaajournal.com/healthcare-data-breach-statistics/ (accessed on 11 January 2020).
- Healthcare Data Breach Report. 2019. Available online: https://www.hipaajournal.com/july-2019-healthcare-data-breach-report/ (accessed on 11 January 2020).
- Palanisamy, V.; Thirunavukarasu, R. Implications of big data analytics in developing healthcare frameworks–A review. J. King Saud Univ.-Comput. Inf. Sci. 2017, 31, 415–425. [Google Scholar] [CrossRef]
- El Aboudi, N.; Benhlima, L. Big Data Management for Healthcare Systems: Architecture, Requirements, and Implementation. Adv. Bioinform. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.; Bourn, S.; Skoufalos, A.; Beck, E.H.; Castillo, D.J. An Innovative Approach to Health Care Delivery for Patients with Chronic Conditions. Popul. Health Manag. 2016, 20, 23–30. [Google Scholar] [CrossRef] [Green Version]
- University Repositorty. 2019. Available online: http://www.bbau.ac.in/new/index.aspx (accessed on 1 March 2020).
- Dang, L.M.; Piran, J.; Han, D.; Min, K.; Moon, H. A Survey on Internet of Things and Cloud Computing for Healthcare. Electronics 2019, 8, 768. [Google Scholar] [CrossRef] [Green Version]
- Vimalachandran, P.; Wang, H.; Zhang, Y.; Heyward, B.; Zhao, Y. Preserving patient-centered controls in electronic health record systems: A reliance-based model implication. In Proceedings of the 2017 International Conference on Orange Technologies (ICOT), Singapore, 8–10 December 2017; Available online: https://arxiv.org/ftp/arxiv/papers/1802/1802.00575.pdf (accessed on 11 January 2020).
- Health Industry Cybersecurity Practices: Managing Threats and Protecting Patients; Department of Health and Human Services: USA. 2018. Available online: https://www.phe.gov/Preparedness/planning/405d/Pages/hic-practices.aspx (accessed on 1 March 2020).
- Pandey, A.K.; Khan, A.I.; Abushark, Y.B.; Alam, M.; Agrawal, A.; Kumar, R.; Khan, R.A. Key Issues in Healthcare Data Integrity: Analysis and Recommendations. IEEE Access 2020, 8, 40612–40628. [Google Scholar] [CrossRef]
- MEDJACK. Medical Device Hijacking; TrapX Research Lab. 2018. Available online: https://www.trustdimension.com/wp-content/uploads/2015/02/MedJack.4-ilovepdf-compressed.pdf (accessed on 1 March 2020).
- Saaty, T.L. How to make a decision: The analytic hierarchy process. Eur. J. Oper. Res. 1990, 48, 9–26. [Google Scholar] [CrossRef]
- Saaty, T.L. Transport planning with multiple criteria: The analytic hierarchy process applications and progress review. J. Adv. Transp. 1995, 29, 81–126. [Google Scholar] [CrossRef]
- Hahn, W.J.; Seaman, S.L.; Bikel, R. Making decisions with multiple attributes: A case in sustainability planning. Graziadio Bus. Rev. 2012, 15, 365–381. [Google Scholar]
- Zavadskas, E.K.; Govindan, K.; Antuchevičienė, J.; Turskis, Z. Hybrid multiple criteria decision-making methods: A review of applications for sustainability issues. Econ. Res.-Ekon. Istraživanja 2016, 29, 857–887. [Google Scholar] [CrossRef] [Green Version]
- Syamsuddin, I. Multicriteria Evaluation and Sensitivity Analysis on Information Security. Int. J. Comput. Appl. 2013, 69, 22–25. [Google Scholar] [CrossRef] [Green Version]
- Mi, X.; Wu, X.; Tang, M.; Liao, H.; Al-Barakati, A.; Altalhi, A.H.; Herrera, F. Hesitant Fuzzy Linguistic Analytic Hierarchical Process with Prioritization, Consistency Checking, and Inconsistency Repairing. IEEE Access 2019, 7, 44135–44149. [Google Scholar] [CrossRef]
- Srivastava, P.R.; Singh, A.P.; Vageesh, V.K. Assessment of Software Quality: A Fuzzy Multi-Criteria Approach. In Evolutionary Computation and Optimization Algorithms in Software Engineering; IGI Global: Hershey, PA, USA, 2010; pp. 200–219. [Google Scholar] [CrossRef]
- How to Build a Sustainable Cyber Security Plan. 2019. Available online: https://www.cigniti.com/blog/sustainable-cybersecurity-strategy-plan/ (accessed on 7 February 2020).
- Mikhailov, L. Deriving priorities from fuzzy pairwise comparison judgements. Fuzzy Sets Syst. 2003, 134, 365–385. [Google Scholar] [CrossRef]
- Dymova, L.; Sevastjanov, P.; Tikhonenko, A. An interval type-2 fuzzy extension of the TOPSIS method using alpha cuts. Knowl.-Based Syst. 2015, 83, 116–127. [Google Scholar] [CrossRef]
- Pearson Product-Moment Correlation. 2017. Available online: https://statistics.laerd.com/statistical-guides/pearson-correlation-coefficient-statistical-guide.php (accessed on 1 March 2020).
- Agrawal, A.; Seh, A.H.; Baz, A.; Alhakami, H.; Alhakami, W.; Baz, M.; Kumar, R.; Khan, R.A. Software Security Estimation Using the Hybrid Fuzzy ANP-TOPSIS Approach: Design Tactics Perspective. Symmetry 2020, 12, 598. [Google Scholar] [CrossRef] [Green Version]
- Kumar, R.; Baz, A.; Alhakami, H.; Alhakami, W.; Baz, M.; Agrawal, A.; Khan, R.A. A Hybrid Model of Hesitant Fuzzy Decision- Making Analysis for Estimating Usable- Security of Software. IEEE Access (Early Access) 2020, 8. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Saaty Scale Definition | Fuzzy Triangle Scale | |
|---|---|---|
| 1 | Equally important | (1, 1, 1) |
| 3 | Weakly important | (2, 3, 4) |
| 5 | Fairly important | (4, 5, 6) |
| 7 | Strongly important | (6, 7, 8) |
| 9 | Absolutely important | (9, 9, 9) |
| 2 | Intermittent values between two adjacent scales | (1, 2, 3) |
| 4 | (3, 4, 5) | |
| 6 | (5, 6, 7) | |
| 8 | (7, 8, 9) |
| Linguistic Variable | Corresponding TFN |
|---|---|
| Very Poor | (0, 1, 3) |
| Poor (P) | (1, 3, 5) |
| Fair (F) | (3, 5, 7) |
| Good (G) | (5, 7, 9) |
| Very good (VG) | (7, 9,10) |
| C1 | C2 | C3 | C4 | |
|---|---|---|---|---|
| C1 | 1.00000, 1.00000, 1.00000 | 0.34000, 0.40000, 0.48000 | 0.56000, 0.90000, 1.37000 | 0.39000, 0.43000, 0.47000 |
| C2 | 2.08000, 2.50000, 2.94000 | 1.00000, 1.00000, 1.00000 | 0.80000, 0.97000, 1.20000 | 0.79000, 0.88000, 1.02000 |
| C3 | 0.73000, 1.11000, 1.79000 | 0.83000, 1.03000, 1.25000 | 1.00000, 1.00000, 1.00000 | 0.50000, 0.70000, 0.93000 |
| C4 | 2.13000, 2.33000, 2.57000 | 0.98000, 1.14000, 1.27000 | 1.08000, 1.43000, 2.00000 | 1.00000, 1.00000, 1.00000 |
| C11 | C12 | C13 | |
|---|---|---|---|
| C11 | 1.00000, 1.00000, 1.00000 | 0.41000, 0.55000, 0.79000 | 0.80000, 1.24000, 1.78000 |
| C12 | 1.26000, 1.81000, 2.43000 | 1.00000, 1.00000, 1.00000 | 0.38000, 0.55000, 0.84000 |
| C13 | 0.56000, 0.80000, 1.25000 | 1.19000, 1.81000, 2.63000 | 1.00000, 1.00000, 1.00000 |
| C21 | C22 | C23 | C24 | C25 | |
|---|---|---|---|---|---|
| C21 | 1.00000, 1.00000, 1.00000 | 0.97000, 1.25000, 1.61000 | 1.06000, 1.59000, 2.22000 | 0.77000, 1.01000, 1.29000 | 0.76000, 0.91000, 1.10000 |
| C22 | 0.62100, 0.80000, 1.03000 | 1.00000, 1.00000, 1.00000 | 0.64000, 0.91000, 1.34000 | 0.43000, 0.63000, 0.97000 | 0.35000, 0.49000, 0.87000 |
| C23 | 0.45000, 0.62800, 0.94300 | 0.74600, 1.09800, 1.56000 | 1.00000, 1.00000, 1.00000 | 0.52000, 0.66000, 0.79000 | 0.52000, 0.66000, 0.92000 |
| C24 | 0.77500, 0.99000, 0.29800 | 1.03000, 1.58000, 2.32000 | 1.26000, 1.51000, 1.92000 | 1.00000, 1.00000, 1.00000 | 0.56000, 0.65000, 0.81000 |
| C25 | 0.90000, 1.09800, 1.31000 | 1.14000, 2.04000, 2.85000 | 1.08000, 1.51000, 1.92000 | 1.23000, 1.53000, 1.78000 | 1.00000, 1.00000, 1.00000 |
| C31 | C32 | C33 | C34 | C35 | |
|---|---|---|---|---|---|
| C31 | 1.00000, 1.00000, 1.00000 | 1.87000, 2.60000, 3.21000 | 1.46000, 1.68000, 1.97000 | 1.45000, 2.44000, 3.39000 | 0.48000, 0.57000, 0.79000 |
| C32 | 0.31100, 0.38000, 0.53400 | 1.00000, 1.00000, 1.00000 | 0.61000, 0.78000, 1.0300 | 0.77000, 0.95000, 1.24000 | 0.16000, 0.20000, 0.25000 |
| C33 | 0.50700, 0.59500, 0.68400 | 0.97000, 1.28000, 1.63900 | 1.00000, 1.00000, 1.00000 | 0.77000, 1.05000, 1.36000 | 0.21000, 0.2500, 0.31000 |
| C34 | 0.29400, 0.40900, 0.68900 | 0.80600, 1.05200, 1.29800 | 0.73500, 0.95200, 1.29800 | 1.00000, 1.00000, 1.00000 | 0.20000, 0.23000, 0.29000 |
| C35 | 1.26500. 1.75400, 2.08300 | 4.00000, 5.00000, 6.25000 | 3.20000, 4.00000, 4.76000 | 3.44000, 4.34000, 4.00000 | 1.00000, 1.00000, 1.00000 |
| C41 | C42 | C43 | C44 | C45 | |
|---|---|---|---|---|---|
| C41 | 1.00000, 1.00000, 1.00000 | 1.00000, 1.52000, 1.93000 | 0.49000, 0.64000, 1.00000 | 0.42000, 0.57000, 1.00000 | 0.22000, 0.29000, 0.42000 |
| C42 | 0.51800, 0.65700, 1.00000 | 1.00000, 1.00000, 1.00000 | 0.57000, 0.67000, 0.80000 | 0.31000, 0.39000, 0.56000 | 0.27000, 0.35000, 0.52000 |
| C43 | 1.00000, 1.56000, 2.04000 | 1.25000, 1.49000, 1.75000 | 1.00000, 1.00000, 1.00000 | 1.00000, 1.32000, 1.55000 | 0.30000, 0.44000, 0.80000 |
| C44 | 1.00000, 1.75000, 2.38000 | 1.78000, 2.56000, 3.22000 | 0.64500, 0.75000, 1.00000 | 1.00000, 1.00000, 1.00000 | 0.54000, 0.91000, 1.58000 |
| C45 | 2.38000, 3.44000, 4.54000 | 1.92000, 2.85000, 3.70000 | 1.25000, 2.27000, 3.33000 | 0.632000, 1.098000, 1.85000 | 1.00000, 1.00000, 1.00000 |
| The First Level | The Weight of First Level | Best Non-Fuzzy Performance Value (BNP) | The Second Level | Local Weight of Second Level | The Final Weight of the Second Level | Best Non-fuzzy Performance Value (BNP) |
|---|---|---|---|---|---|---|
| C1 | 0.14600, 0.15000, 0.19000 | 0.16200 | C11 | 0.20800, 0.21500, 0.22900 | 0.03000, 0.03200, 0.04300 | 0.03500 |
| C12 | 0.30200, 0.31000, 0.32800 | 0.00500, 0.04600, 0.06200 | 0.03800 | |||
| C13 | 0.45200, 0.46300, 0.48700 | 0.06600, 0.07000, 0.09300 | 0.07600 | |||
| C2 | 0.28900, 0.30000, 0.35100 | 0.31100 | C21 | 0.20200, 0.22500, 0.24000 | 0.05800, 0.06700, 0.08400 | 0.07000 |
| C22 | 0.22000, 0.25100, 0.55500 | 0.06300, 0.07500, 0.19000 | 0.00900 | |||
| C23 | 0.31100, 0.35300, 0.51400 | 0.08900, 0.09900, 0.18000 | 0.09300 | |||
| C24 | 0.11200, 0.16900, 0.21100 | 0.03200, 0.05000, 0.07400 | 0.05200 | |||
| C25 | 0.51000, 0.57100, 0.60400 | 0.04000, 0.07000, 0.09600 | 0.07400 | |||
| C3 | 0.20800, 0.22600, 0.30600 | 0.20000 | C31 | 0.23300, 0.23800, 0.26400 | 0.04800, 0.05300, 0.08000 | 0.06000 |
| C32 | 0.13500, 0.14100, 0.14100 | 0.02800, 0.03100, 0.04000 | 0.03300 | |||
| C33 | 0.12500, 0.13600, 0.17700 | 0.02600, 0.03000, 0.05400 | 0.03700 | |||
| C34 | 0.59200, 0.60200, 0.72700 | 0.12300, 0.13600, 0.22200 | 0.15000 | |||
| C35 | 0.43100, 0.46300, 0.45900, | 0.08900, 0.10000, 0.14000 | 0.01000 | |||
| C4 | 0.32400, 0.34400, 0.40700 | 0.32700 | C41 | 0.23500, 0.25500, 0.26600 | 0.07600, 0.08700, 0.10800 | 0.09000 |
| C42 | 0.52800, 0.53500, 0.54800 | 0.17000, 0.18000, 0.22300 | 0.06500 | |||
| C43 | 0.40200, 0.41400, 0.42800 | 0.13000, 0.14000, 0.17400 | 0.04800 | |||
| C44 | 0.23200, 0.24000, 0.26900 | 0.07500, 0.08000, 0.10900 | 0.04900 | |||
| C45 | 0.27700, 0.28400, 0.28900 | 0.05100, 0.05700, 0.06400 | 0.01100 |
| S. No. | Level 1 Characteristics | Final Weights | Best Non-fuzzy Performance Value (BNP) | Ranks |
|---|---|---|---|---|
| 1 | Data Storage Layer | 0.14600, 0.15000, 0.19000 | 0.16200 | 4 |
| 2 | Data Application Layer | 0.28900, 0.30000, 0.35100 | 0.31100 | 2 |
| 3 | Data Transfer Layer | 0.20800, 0.22600, 0.30600 | 0.20000 | 3 |
| 4 | Data Production Layer | 0.32400, 0.34400, 0.40700 | 0.32700 | 1 |
| S. No. | Level 2 Characteristics | Final Weights | Best Non-fuzzy Performance Value (BNP) | Ranks | |
|---|---|---|---|---|---|
| 1 | Medjacking | C11+C21+C31 | 0.13600, 0.15200, 0.20700 | 0.16500 | 6 |
| 2 | Low access control management | C12+C22+C41 | 0.14400, 0.20800, 0.36000 | 0.23600 | 4 |
| 3 | Malware/Ransomware | C35+C45 | 0.14000, 0.15700, 0.20400 | 0.16700 | 5 |
| 4 | Outdated IT Infrastructure | C24+C33+C43 | 0.18800, 0.22000, 0.30200 | 0.23700 | 3 |
| 5 | Human Error | C13+C23+C32+C42 | 0.35300, 0.38000, 0.53600 | 0.42300 | 1 |
| 6 | Social Engineering | C25+C34+C44 | 0.23800, 0.28600, 0.42700 | 0.31700 | 2 |
| A1 | A2 | A3 | A4 | A5 | A6 | A7 | A8 | A9 | A10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Medjacking | 5.36000, 7.36000, 9.00000 | 4.82000, 6.82000, 8.64000 | 3.91000, 5.91000, 7.80020 | 4.27000, 6.27000, 8.27000 | 2.45000, 4.45000, 6.45000 | 2.91000, 4.64000, 6.55000 | 1.45000, 3.00000, 4.91000 | 1.18000, 2.82000, 4.82000 | 4.82000, 6.82000, 8.55000 | 4.82000, 6.82000, 8.73000 |
| Low access control management | 4.27000, 6.27000, 8.09000 | 4.64000, 6.64000, 8.45000 | 4.64000, 6.64000, 8.36000 | 4.27000, 6.27000, 8.00000 | 2.82000, 4.82000, 6.82000 | 3.18000, 5.18000, 7.09000 | 1.45000, 3.00000, 4.91000 | 0.82000, 2.27000, 4.27000 | 5.18000, 7.18000, 8.82000 | 4.82000, 6.82000, 8.64000 |
| Malware/Ransomware | 6.27000, 8.27000, 9.64000 | 2.64000, 4.64000, 6.64000 | 3.18000, 5.18000, 7.09000 | 5.36000, 7.36000, 9.00000 | 3.73000, 5.73000, 7.55000 | 2.45000, 4.45000, 6.45000 | 0.91000, 2.45000, 4.45000 | 2.45000, 4.27000, 6.27000 | 5.18000, 7.18000, 8.91000 | 4.82000, 6.82000, 8.55000 |
| Outdated IT Infrastructure | 4.82000, 6.82000, 8.64000 | 3.09000, 5.00000, 6.91000 | 3.18000, 5.18000, 7.09000 | 4.64000, 6.64000, 8.55000 | 3.00000, 5.00000, 7.00000 | 2.18000, 4.09000, 6.00000 | 2.82000, 4.64000, 6.64000 | 1.91000, 3.73000, 5.73000 | 5.73000, 7.73000, 9.36000 | 5.55000, 7.50500, 9.27000 |
| Human Error | 3.73000, 5.73000, 7.64000 | 3.91000, 5.91000, 7.73000 | 4.27000, 6.27000, 8.18000 | 3.00000, 5.00000, 7.00000 | 2.45000, 4.45000, 6.45000 | 3.55000, 5.55000, 7.45000 | 1.82000, 3.73000, 5.73000 | 1.64000, 3.55000, 5.55000 | 5.73000, 7.73000, 9.27000 | 4.27000, 6.27000, 8.18000 |
| Social Engineering | 4.45000, 6.45000, 8.27000 | 3.55000, 5.55000, 7.45000 | 5.00000, 7.00000, 8.73000 | 5.36000, 7.36000, 9.09000 | 2.64000, 4.64000, 6.64000 | 2.90000, 4.80000, 6.70000 | 2.82000, 4.64000, 6.64000 | 2.55000, 4.45000, 6.45000 | 5.18000, 7.18000, 9.00000 | 4.27000, 6.27000, 8.09000 |
| A1 | A2 | A3 | A4 | A5 | A6 | A7 | A8 | A9 | A10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Medjacking | 0.56000, 0.76000, 0.93000 | 0.52000, 0.74000, 0.93000 | 0.42000, 0.64000, 0.84000 | 0.45000, 0.66000, 0.88000 | 0.33000, 0.59000, 0.86000 | 0.35000, 0.56000, 0.79000 | 0.22000, 0.45000, 0.73000 | 0.18000, 0.42000, 0.72000 | 0.50000, 0.71000, 0.89000 | 0.52000, 0.74000, 0.94000 |
| Low access control management | 0.44000, 0.65000, 0.84000 | 0.50000, 0.72000, 0.91000 | 0.50000, 0.72000, 0.90000 | 0.45000, 0.66000, 0.85000 | 0.37000, 0.64000, 0.90000 | 0.38000, 0.63000, 0.86000 | 0.22000, 0.45000, 0.73000 | 0.12000, 0.34000, 0.64000 | 0.54000, 0.75000, 0.92000 | 0.52000, 0.74000, 0.93000 |
| Malware/Ransomware | 0.65000, 0.86000, 1.00000 | 0.28000, 0.50000, 0.72000 | 0.34000, 0.56000, 0.76000 | 0.57000, 0.78000, 0.95000 | 0.49000, 0.76000, 1.00000 | 0.30000, 0.54000, 0.78000 | 0.140000, 0.36000, 0.66000 | 0.36000, 0.64000, 0.93000 | 0.54000, 0.75000, 0.92000 | 0.52000, 0.74000, 0.92000 |
| Outdated IT Infrastructure | 0.50000, 0.71000, 0.90000 | 0.33000, 0.54000, 0.75000 | 0.34000, 0.56000, 0.76000 | 0.49000, 0.70000, 0.90000 | 0.40000, 0.66000, 0.93000 | 0.26000, 0.49000, 0.73000 | 0.42000, 0.69000, 0.99000 | 0.28000, 0.55000, 0.85000 | 0.59000, 0.80000, 0.97000 | 0.60000, 0.81000, 1.00000 |
| Human Error | 0.39000, 0.59000, 0.79000 | 0.42000, 0.64000, 0.83000 | 0.46000, 0.68000, 0.88000 | 0.32000, 0.53000, 0.74000 | 0.33000, 0.59000, 0.86000 | 0.43000, 0.67000, 0.90000 | 0.27000, 0.55000, 0.80005 | 0.24000, 0.53000, 0.82000 | 0.59000, 0.80000, 0.96000 | 0.46000, 0.68000, 0.88000 |
| Social Engineering | 0.46000, 0.67000, 0.86000 | 0.38000, 0.60000, 0.80000 | 0.54000, 0.75000, 0.94000 | 0.57000, 0.78000, 0.96000 | 0.35000, 0.61000, 0.88000 | 0.35000, 0.58000, 0.81000 | 0.42000, 0.69000, 0.99000 | 0.38000, 0.66000, 0.96000 | 0.54000, 0.75000, 0.93000 | 0.46000, 0.68000, 0.87000 |
| A1 | A2 | A3 | A4 | A5 | A6 | A7 | A8 | A9 | A10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Medjacking | 0.002000, 0.007000, 0.021000 | 0.002000, 0.006000, 0.021000 | 0.001000, 0.006000, 0.019000 | 0.002000, 0.006000, 0.020000 | 0.001000, 0.005000, 0.019000 | 0.001000, 0.005000, 0.018000 | 0.001000, 0.004000, 0.016000 | 0.001000, 0.004000, 0.016000 | 0.004000, 0.014000, 0.043000 | 0.004000, 0.015000, 0.046000 |
| Low access control management | 0.002000, 0.008000, 0.025000 | 0.002000, 0.008000, 0.027000 | 0.002000, 0.008000, 0.027000 | 0.002000, 0.008000, 0.025000 | 0.002000, 0.007000, 0.027000 | 0.002000, 0.007000, 0.025000 | 0.001000, 0.005000, 0.022000 | 0.001000, 0.004000, 0.019000 | 0.002000, 0.006000, 0.019000 | 0.002000, 0.006000, 0.020000 |
| Malware/Ransomware | 0.002000, 0.008000, 0.024000 | 0.001000, 0.005000, 0.017000 | 0.001000, 0.005000, 0.018000 | 0.002000, 0.007000, 0.022000 | 0.002000, 0.007000, 0.024000 | 0.001000, 0.005000, 0.018000 | 0.000000, 0.003000, 0.016000 | 0.001000, 0.006000, 0.022000 | 0.002000, 0.007000, 0.023000 | 0.002000, 0.007000, 0.023000 |
| Outdated IT Infrastructure | 0.002000, 0.007000, 0.023000 | 0.001000, 0.006000, 0.019000 | 0.002000, 0.006000, 0.019000 | 0.002000, 0.007000, 0.023000 | 0.002000, 0.007000, 0.024000 | 0.001000, 0.005000, 0.018000 | 0.002000, 0.007000, 0.025000 | 0.001000, 0.006000, 0.022000 | 0.001000, 0.003000, 0.011000 | 0.001000, 0.004000, 0.011000 |
| Human Error | 0.003000, 0.010000, 0.032000 | 0.003000, 0.011000, 0.034000 | 0.003000, 0.011000, 0.036000 | 0.002000, 0.009000, 0.030000 | 0.002000, 0.010000, 0.035000 | 0.003000, 0.011000, 0.036000 | 0.002000, 0.009000, 0.034000 | 0.002000, 0.009000, 0.033000 | 0.004000, 0.012000, 0.040100 | 0.003000, 0.011000, 0.037000 |
| Social Engineering | 0.004000, 0.014000, 0.044000 | 0.003000, 0.012000, 0.041000 | 0.005000, 0.016000, 0.048000 | 0.005000, 0.016000, 0.049000 | 0.003000, 0.013000, 0.045000 | 0.003000, 0.012000, 0.041000 | 0.004000, 0.014000, 0.050000 | 0.003000, 0.014000, 0.049000 | 0.006000, 0.022000, 0.071000 | 0.005000, 0.020000, 0.066000 |
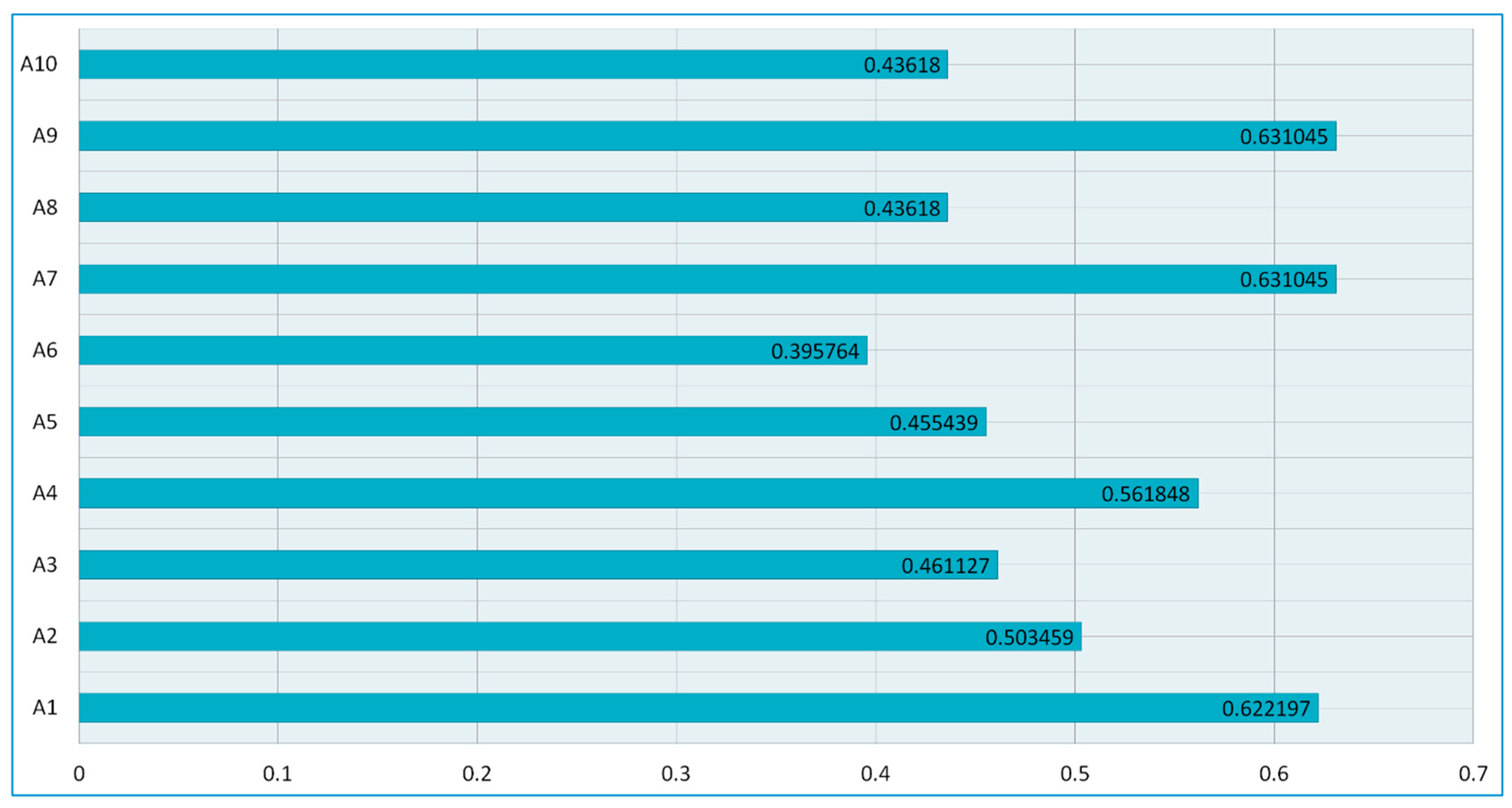
| Alternatives | d+i | d−i | Gap Degree of CC+i | Satisfaction Degree of CC−i | |
|---|---|---|---|---|---|
| Alternative 1 | A1 | 0.043845 | 0.026623 | 0.377803 | 0.622197 |
| Alternative 2 | A2 | 0.036748 | 0.036243 | 0.496541 | 0.503459 |
| Alternative 3 | A3 | 0.035237 | 0.041178 | 0.538873 | 0.461127 |
| Alternative 4 | A4 | 0.034652 | 0.027023 | 0.438152 | 0.561848 |
| Alternative 5 | A5 | 0.038358 | 0.045864 | 0.544561 | 0.455439 |
| Alternative 6 | A6 | 0.030494 | 0.046557 | 0.604236 | 0.395764 |
| Alternative 7 | A7 | 0.043845 | 0.025635 | 0.368955 | 0.631045 |
| Alternative 8 | A8 | 0.032765 | 0.042353 | 0.563820 | 0.436180 |
| Alternative 9 | A9 | 0.043845 | 0.025635 | 0.368955 | 0.631045 |
| Alternative 10 | A10 | 0.032765 | 0.042353 | 0.563820 | 0.436180 |
| Experiments | Weights/Alternatives | A1 | A2 | A3 | A4 | A5 | A6 | A7 | A8 | A9 | A10 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Experiment-0 | Original Weights | Satisfaction Degree (CC-i) | 0.622197 | 0.503459 | 0.461127 | 0.561848 | 0.455439 | 0.395764 | 0.631045 | 0.436180 | 0.631045 | 0.436180 |
| Experiment-1 | Medjacking | 0.711297 | 0.595059 | 0.546727 | 0.642348 | 0.543239 | 0.478764 | 0.656045 | 0.52168 | 0.710545 | 0.53248 | |
| Experiment-2 | Low access control management | 0.663997 | 0.546059 | 0.501927 | 0.599048 | 0.496839 | 0.435064 | 0.668745 | 0.46818 | 0.669045 | 0.48148 | |
| Experiment-3 | Malware/Ransomware | 0.580797 | 0.463059 | 0.424127 | 0.523448 | 0.418039 | 0.359764 | 0.590445 | 0.37798 | 0.597045 | 0.39548 | |
| Experiment-4 | Outdated IT Infrastructure | 0.544797 | 0.423659 | 0.391127 | 0.492048 | 0.385639 | 0.328064 | 0.558045 | 0.34048 | 0.566045 | 0.35948 | |
| Experiment-5 | Human Error | 0.625197 | 0.491459 | 0.468727 | 0.583748 | 0.455239 | 0.406264 | 0.633745 | 0.42918 | 0.629045 | 0.43818 | |
| Experiment-6 | Social Engineering | 0.622897 | 0.496159 | 0.465127 | 0.571748 | 0.455239 | 0.400764 | 0.632045 | 0.44018 | 0.630545 | 0.43678 |
| Methods/Alternatives | A1 | A2 | A3 | A4 | A5 | A6 | A7 | A8 | A9 | A10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Fuzzy-AHP-TOPSIS | 0.622197 | 0.503459 | 0.461127 | 0.561848 | 0.455439 | 0.395764 | 0.631045 | 0.436180 | 0.631045 | 0.436180 |
| Classical-AHP-TOPSIS | 0.637897 | 0.500759 | 0.473127 | 0.602848 | 0.457439 | 0.411764 | 0.640645 | 0.464680 | 0.631045 | 0.441180 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, R.; Pandey, A.K.; Baz, A.; Alhakami, H.; Alhakami, W.; Agrawal, A.; Khan, R.A. Fuzzy-Based Symmetrical Multi-Criteria Decision-Making Procedure for Evaluating the Impact of Harmful Factors of Healthcare Information Security. Symmetry 2020, 12, 664. https://doi.org/10.3390/sym12040664
Kumar R, Pandey AK, Baz A, Alhakami H, Alhakami W, Agrawal A, Khan RA. Fuzzy-Based Symmetrical Multi-Criteria Decision-Making Procedure for Evaluating the Impact of Harmful Factors of Healthcare Information Security. Symmetry. 2020; 12(4):664. https://doi.org/10.3390/sym12040664
Chicago/Turabian StyleKumar, Rajeev, Abhishek Kumar Pandey, Abdullah Baz, Hosam Alhakami, Wajdi Alhakami, Alka Agrawal, and Raees Ahmad Khan. 2020. "Fuzzy-Based Symmetrical Multi-Criteria Decision-Making Procedure for Evaluating the Impact of Harmful Factors of Healthcare Information Security" Symmetry 12, no. 4: 664. https://doi.org/10.3390/sym12040664