
Revealing an Abundance of Microbial Fecal Contamination and Multidrug Resistant Bacteria in the Mississippi Gulf Coast

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Sample Collection
2.3. Temperature, pH, and Salinity Measurements
2.4. E. coli and Enterococcus Enumeration, Isolation and Archiving
2.5. Antibiotic Resistance Analysis and Multidrug Resistance Analysis
2.6. Statistical Analyses
3. Results
3.1. Analysis of Microbial Contamination
3.1.1. E. coli Contamination Measurements
3.1.2. Enterococcus Contamination Measurements
3.2. Antimicrobial Resistance (AMR) Patterns for Individual Antibiotic Tested
3.2.1. E. coli AMR Patterns
3.2.2. Enterococcus AMR Patterns
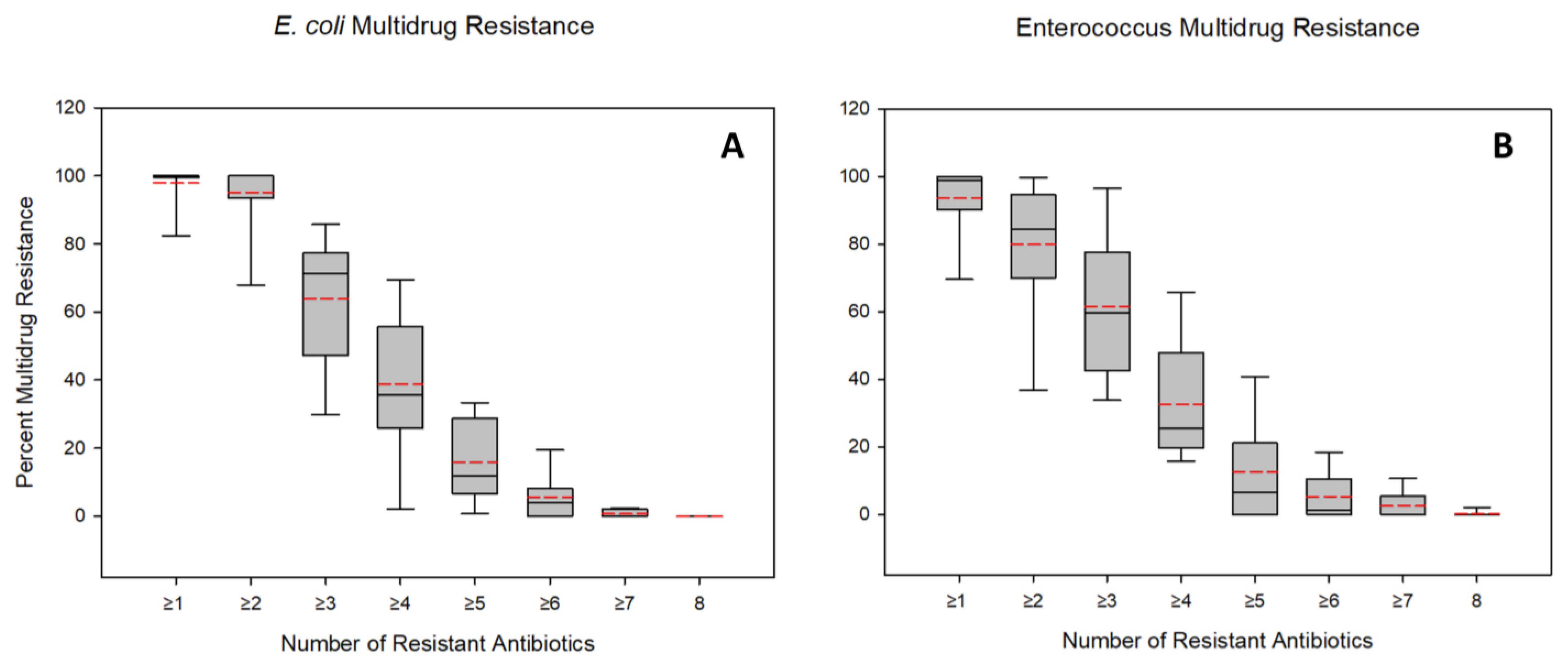
3.3. Multidrug Resistance Patterns
3.3.1. E. coli MDR Patterns
3.3.2. Enterococcus MDR Patterns
3.4. Variations in Physical Parameters in Relation to E. coli and Enterococcus Numbers
4. Discussion
4.1. FIB Contamination in the Mississippi Gulf Coast
4.2. Antimicrobial Resistance Patterns along the Mississippi Gulf Coast
4.3. Multidrug Resistance Patterns along the Mississippi Gulf Coast
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- USEPA (United States Environmental Protection Agency) Recreational Water Quality Criteria and Methods. 2013. Available online: https://www.epa.gov/wqc/recreational-water-quality-criteria-and-methods (accessed on 7 February 2022).
- Devine, J. Testing the Waters 2014: A Guide to Water Quality at Vacation Beaches. 2014. Available online: https://www.nrdc.org/resources/testing-waters-2014-guide-water-quality-vacation-beaches (accessed on 16 November 2022).
- Garrido-Pérez, M.; Anfuso, E.; Acevedo, A.; Perales-Vargas-Machuca, J. Microbial indicators of faecal contamination in waters and sediments of beach bathing zones. Int. J. Hyg. Environ. Health 2008, 211, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Halliday, E.; Gast, R.J. Bacteria in Beach Sands: An Emerging Challenge in Protecting Coastal Water Quality and Bather Health. Environ. Sci. Technol. 2010, 45, 370–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korajkic, A.; McMinn, B.R.; Harwood, V.J. Relationships between Microbial Indicators and Pathogens in Recreational Water Settings. Int. J. Environ. Res. Public Health 2018, 15, 2842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klevens, R.M.; Edwards, J.R.; Richards, C.L., Jr.; Horan, T.C.; Gaynes, R.P.; Pollock, D.A.; Cardo, D.M. Estimating Health Care-Associated Infections and Deaths in U.S. Hospitals, 2002. Public Health Rep. 2007, 122, 160–166. [Google Scholar] [CrossRef]
- Baquero, F.; Martinez, J.L.; Cantón, R. Antibiotics and antibiotic resistance in water environments. Curr. Opin. Biotechnol. 2008, 19, 260–265. [Google Scholar] [CrossRef]
- Zhang, X.-X.; Zhang, T.; Fang, H.H.P. Antibiotic resistance genes in water environment. Appl. Microbiol. Biotechnol. 2009, 82, 397–414. [Google Scholar] [CrossRef]
- Allen, H.K.; Donato, J.; Wang, H.H.; Cloud-Hansen, K.A.; Davies, J.; Handelsman, J. Call of the wild: Antibiotic resistance genes in natural environments. Nat. Rev. Genet. 2010, 8, 251–259. [Google Scholar] [CrossRef]
- Bush, K.; Courvalin, P.; Dantas, G.; Davies, J.; Eisenstein, B.; Huovinen, P.; Jacoby, G.A.; Kishony, R.; Kreiswirth, B.N.; Kutter, E.; et al. Tackling antibiotic resistance. Nat. Rev. Microbiol. 2011, 9, 894–896. [Google Scholar] [CrossRef] [Green Version]
- Wellington, E.M.H.; Boxall, A.B.A.; Cross, P.; Feil, E.J.; Gaze, W.H.; Hawkey, P.M.; Johnson-Rollings, A.S.; Jones, D.L.; Lee, N.M.; Otten, W.; et al. The role of the natural environment in the emergence of antibiotic resistance in Gram-negative bacteria. Lancet Infect. Dis. 2013, 13, 155–165. [Google Scholar] [CrossRef]
- Ventola, C.L. The Antibiotic Resistance Crisis. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- Spellberg, B.; Guidos, R.; Gilbert, D.; Bradley, J.; Boucher, H.W.; Scheld, W.M.; Bartlett, J.G.; Edwards, J., Jr. The Infectious Diseases Society of America. The Epidemic of Antibiotic-Resistant Infections: A Call to Action for the Medical Community from the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 46, 155–164. [Google Scholar] [CrossRef] [Green Version]
- Pruden, A. Balancing Water Sustainability and Public Health Goals in the Face of Growing Concerns about Antibiotic Resistance. Environ. Sci. Technol. 2014, 48, 5–14. [Google Scholar] [CrossRef]
- CDC’s Antibiotic Resistance Threats in the United States (2019 AR Threats Report). 2019. Available online: https://www.cdc.gov/drugresistance/biggest-threats.html (accessed on 14 December 2021).
- Wright, G.D. Antibiotic resistance in the environment: A link to the clinic? Curr. Opin. Microbiol. 2010, 13, 589–594. [Google Scholar] [CrossRef]
- Davison, J. Genetic Exchange between Bacteria in the Environment. Plasmid 1999, 42, 73–91. [Google Scholar] [CrossRef]
- Pepper, I.L.; Gentry, T.J. Microorganisms Found in the Environment. In Environmental Microbiology; Elsevier Inc.: Amsterdam, The Netherlands, 2015; pp. 9–36. [Google Scholar] [CrossRef]
- Pepper, I.L.; Gerba, C.P.; Gentry, T.J. Global Emerging Microbial Issues in the Anthropocene Era. In Environmental Microbiology; Elsevier Inc.: Amsterdam, The Netherlands, 2015; pp. 677–688. [Google Scholar] [CrossRef]
- Vaz-Moreira, I.; Nunes, O.C.; Manaia, C.M. Bacterial diversity and antibiotic resistance in water habitats: Searching the links with the human microbiome. FEMS Microbiol. Rev. 2014, 38, 761–778. [Google Scholar] [CrossRef]
- Alm, E.W.; Zimbler, D.; Callahan, E.; Plomaritis, E. Patterns and persistence of antibiotic resistance in faecal indicator bacteria from freshwater recreational beaches. J. Appl. Microbiol. 2014, 117, 273–285. [Google Scholar] [CrossRef]
- Blaak, H.; Lynch, G.; Italiaander, R.; Hamidjaja, R.A.; Schets, F.M.; de Roda Husman, A.M. Multidrug-Resistant and Extended Spectrum Beta-Lactamase-Producing Escherichia coli in Dutch Surface Water and Wastewater. PLoS ONE 2015, 10, e0127752. [Google Scholar] [CrossRef] [Green Version]
- Böckelmann, U.; Dörries, H.-H.; Ayuso-Gabella, M.N.; de Marçay, M.S.; Tandoi, V.; Levantesi, C.; Masciopinto, C.; Van Houtte, E.; Szewzyk, U.; Wintgens, T.; et al. Quantitative PCR Monitoring of Antibiotic Resistance Genes and Bacterial Pathogens in Three European Artificial Groundwater Recharge Systems. Appl. Environ. Microbiol. 2009, 75, 154–163. [Google Scholar] [CrossRef] [Green Version]
- Cooke, M.D. Antibiotic Resistance among Coliform and Fecal Coliform Bacteria Isolated from Sewage, Seawater, and Marine Shellfish. Antimicrob. Agents Chemother. 1976, 9, 879–884. [Google Scholar] [CrossRef] [Green Version]
- Di Cesare, A.; Vignaroli, C.; Luna, G.M.; Pasquaroli, S.; Biavasco, F. Antibiotic-Resistant Enterococci in Seawater and Sediments from a Coastal Fish Farm. Microb. Drug Resist. 2012, 18, 502–509. [Google Scholar] [CrossRef]
- Griffin, D.W.; Banks, K.; Gregg, K.; Shedler, S.; Walker, B.K. Antibiotic Resistance in Marine Microbial Communities Proximal to a Florida Sewage Outfall System. Antibiotics 2020, 9, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibekwe, A.M.; Murinda, S.E.; Graves, A.K. Genetic Diversity and Antimicrobial Resistance of Escherichia coli from Human and Animal Sources Uncovers Multiple Resistances from Human Sources. PLoS ONE 2011, 6, e20819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knapp, C.; Dolfing, J.; Ehlert, P.A.I.; Graham, D.W. Evidence of Increasing Antibiotic Resistance Gene Abundances in Archived Soils since 1940. Environ. Sci. Technol. 2010, 44, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, M.; Gentry, T.; Mjelde, H.; Brooks, J.P.; Harmel, D.; Gregory, L.; Wagner, K. Escherichia coli Antimicrobial Resistance Variability in Water Runoff and Soil from a Remnant Native Prairie, an Improved Pasture, and a Cultivated Agricultural Watershed. Water 2020, 12, 1251. [Google Scholar] [CrossRef]
- Mukherjee, M.; Laird, E.; Gentry, T.J.; Brooks, J.P.; Karthikeyan, R. Increased Antimicrobial and Multidrug Resistance Downstream of Wastewater Treatment Plants in an Urban Watershed. Front. Microbiol. 2021, 12, 657353. [Google Scholar] [CrossRef]
- Mukherjee, M.; Marie, L.; Liles, C.; Mustafa, N.; Bullerjahn, G.; Gentry, T.J.; Brooks, J.P. Elevated Incidences of Antimicrobial Resistance and Multidrug Resistance in the Maumee River (Ohio, USA), a Major Tributary of Lake Erie. Microorganisms 2021, 9, 911. [Google Scholar] [CrossRef]
- Zou, S.; Xu, W.; Zhang, R.; Tang, J.; Chen, Y.; Zhang, G. Occurrence and distribution of antibiotics in coastal water of the Bohai Bay, China: Impacts of river discharge and aquaculture activities. Environ. Pollut. 2011, 159, 2913–2920. [Google Scholar] [CrossRef]
- USCDC (United States Centers for Disease Control and Prevention). Antibiotic Resistance Threats in the United Stated. 2019. Available online: https://www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf (accessed on 11 November 2022).
- Weisman, G. Safe for Swimming? Water Quality at Our Beaches. Environment America Research and Policy Center. 2019. Available online: https://policycommons.net/artifacts/1767748/safe-for-swimming/2499394/ (accessed on 16 November 2022).
- DiRienzo, D. Mississippi has Some of the Dirtiest Beaches in the Nation Due to Fecal Bacteria. 2019. Available online: https://www.onlyinyourstate.com/mississippi/fecal-bacteria-beaches-ms/ (accessed on 15 November 2022).
- Mississippi Department of Environmental Quality (MDEQ). 11 Beach Water Contact Advisories in Effect. 2020. Available online: https://www.mdeq.ms.gov/11-beach-water-contact-advisories-in-effect/ (accessed on 16 November 2022).
- Quyyumi, F. Swim at Your Own Risk: State Issues Bacteria Warnings for 17 Coastal Beaches. Sunherald. 2021. Available online: http://www.sunherald.com/news/local/article251750823.html (accessed on 16 November 2022).
- Armstrong, B.N.; Cambazoglu, M.K.; Wiggert, J.D. Modeling the impact of the 2019 Bonnet Carré Spillway Opening and Local River Flooding on the Mississippi Sound. In OCEANS 2021: San Diego—Porto; IEEE: Piscataway, NJ, USA, 2021; pp. 1–7. [Google Scholar] [CrossRef]
- Parton, A. NOAA Launches Investigation into Dolphin Deaths. Supertalk Mississippi Media. 2019. Available online: https://www.supertalk.fm/noaa-launches-investigation-into-dolphin-deaths/ (accessed on 17 March 2022).
- Rozier, A. A Flood of Catastrophe: How a Warming Climate and the Bonnet Carre Spillway Threaten the Survival of Coast Fishermen. 2020. Available online: https://pulitzercenter.org/stories/flood-catastrophe-how-warming-climate-and-bonnet-carre-spillway-threaten-survival-coast (accessed on 16 November 2022).
- Gauntt, B. Mississippi Lt Gov: Corps Ignored Spillway Operating Manual. Clarion Ledger. 2021. Available online: https://www.clarionledger.com/story/news/2021/07/21/mississippi-lt-gov-army-corps-of-engineers-ignored-spillway-operating-manual/8039050002/ (accessed on 11 March 2022).
- Herbert, G. Mississippi Cities, Counties Sue Over Damages from Freshwater Dumping from La Spillway. Clarion Ledger. 2019. Available online: https://www.clarionledger.com/story/news/local/2019/12/27/bonnet-carre-spillway-mississippi-cities-counties-file-lawsuit/2755596001/ (accessed on 16 November 2022).
- Green, D. The 2019–2020 Bonnet Carre Spillway Opening. ArcGIS StoryMaps. 2020. Available online: https://storymaps.arcgis.com/stories/2558ee4ef8314cb9ab95cd31670783c4 (accessed on 9 February 2022).
- McCormack, F. State of Mississippi Sues over Bonnet Carrey. The Waterways Journal. 2020. Available online: https://www.waterwaysjournal.net/2020/01/03/state-of-mississippi-sues-over-bonnet-carre/ (accessed on 16 November 2022).
- Parra, S.M.; Sanial, V.; Boyette, A.D.; Cambazoglu, M.K.; Soto, I.M.; Greer, A.T.; Chiaverano, L.M.; Hoover, A.; Dinniman, M.S. Bonnet Carré Spillway freshwater transport and corresponding biochemical properties in the Mississippi Bight. Cont. Shelf Res. 2020, 199, 104114. [Google Scholar] [CrossRef]
- Lee, A. ‘Unlawful’ Operation of Bonnet Carré Prompts MS Secretary of State to Sue US Army Corps. Clarion Ledger. Available online: https://www.clarionledger.com/story/news/2019/12/31/bonnet-carre-spillway-lawsuit/2782429001/ (accessed on 9 February 2022).
- Schleifstein, M. Environmentalists Plan to Sue over Harm to Endangered Species from Bonnet Carre Spillway. 2020. Available online: https://www.nola.com/news/courts/article_27ca454e-4157-11ea-8e2c-97e7195fce75.html (accessed on 11 March 2022).
- Schleifstein, M. What the Bonnet Carre Spillway Opening Means for Lake Pontchartrain. Nola. com. 2019. Available online: https://www.nola.com/news/environment/article_42887d20-14ba-5900-ae2c-c3f4faefa265.html (accessed on 16 November 2022).
- USEPA (United Stated Environmental Protection Agency). Method 1600: Enterococci in Water by Membrane Filtration Using Membrane-Enterococcus Indoxyl-β-D-Glucoside Agar (mEI). 2002. Available online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.epa.gov/sites/default/files/2015-08/documents/method_1600_2009.pdf (accessed on 16 November 2022).
- USEPA (United Stated Environmental Protection Agency). Method 1603: Escherichia coli (E. coli) in Water by Membrane Filtration Using Modified Membrane-Thermotolerant Escherichia coli Agar (Modified mTEC). 2002. Available online: https://www.epa.gov/sites/default/files/2015-08/documents/method_1603_2009.pdf (accessed on 20 June 2023).
- Bauer, A.W.; Kirby, W.M.; Sherris, J.C.; Turck, M. Antibiotic susceptibility testing by a standardized single disk method. Am. J. Clin. Pathol. 1966, 45, 493–496. [Google Scholar] [CrossRef]
- Agudelo Higuita, N.I.; Huycke, M.M. Enterococcal Disease, Epidemiology, and Implications for Treatment. In Enterococci: From Commensals to Leading Causes of Drug Resistant Infection; Massachusetts Eye and Ear Infirmary: Boston, MA, USA, 2014; pp. 1–35. [Google Scholar]
- Byappanahalli, M.; Nevers, M.; Korajkic, A.; Staley, Z.R.; Harwood, V.J. Enterococci in the Environment. Microbiol. Mol. Biol. Rev. 2012, 76, 685–706. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira, D.M.P.; Forde, B.M.; Kidd, T.J.; Harris, P.N.A.; Schembri, M.A.; Beatson, S.A.; Paterson, D.L.; Walker, M.J. Antimicrobial Resistance in ESKAPE Pathogens. Clin. Microbiol. Rev. 2020, 33, e00181-19. [Google Scholar] [CrossRef]
- Jang, J.; Hur, H.-G.; Sadowsky, M.; Byappanahalli, M.; Yan, T.; Ishii, S. Environmental Escherichia coli: Ecology and public health implications-a review. J. Appl. Microbiol. 2017, 123, 570–581. [Google Scholar] [CrossRef] [Green Version]
- Vila, J.; Sáez-López, E.; Johnson, J.R.; Römling, U.; Dobrindt, U.; Cantón, R.; Giske, C.G.; Naas, T.; Carattoli, A.; Martínez-Medina, M. Escherichia coli: An old friend with new tidings. FEMS Microbiol. Rev. 2016, 40, 437–463. [Google Scholar] [CrossRef] [Green Version]
- Hancock, L.E.; Murray, B.E.; Sillanpää, J. Enterococcal Cell Wall Components and Structures. In Enterococci: From Commensals to Leading Causes of Drug Resistant Infection; Massachusetts Eye and Ear Infirmary: Boston, MA, USA, 2014; pp. 1–35. [Google Scholar]
- Whitman, R.L.; Harwood, V.J.; Edge, T.A.; Nevers, M.B.; Byappanahalli, M.N.; Vijayavel, K.; Brandão, J.; Sadowsky, M.J.; Alm, E.W.; Crowe, A.; et al. Microbes in beach sands: Integrating environment, ecology and public health. Rev. Environ. Sci. Bio. Technol. 2014, 13, 329–368. [Google Scholar] [CrossRef] [Green Version]
- Flood, C.; Ufnar, J.; Wang, S.; Johnson, J.; Carr, M.; Ellender, R. Lack of correlation between enterococcal counts and the presence of human specific fecal markers in Mississippi creek and coastal waters. Water Res. 2011, 45, 872–878. [Google Scholar] [CrossRef]
- Pachepsky, Y.A.; Shelton, D.R. Escherichia coli and Fecal Coliforms in Freshwater and Estuarine Sediments. Crit. Rev. Environ. Sci. Technol. 2011, 41, 1067–1110. [Google Scholar] [CrossRef]
- Singh, R.; Singh, A.P.; Kumar, S.; Giri, B.S.; Kim, K.-H. Antibiotic resistance in major rivers in the world: A systematic review on occurrence, emergence, and management strategies. J. Clean. Prod. 2019, 234, 1484–1505. [Google Scholar] [CrossRef]
- Sabater, J.K. Antibiotic-resistant Escherichia coli and Enterococcus spp. in Sand and Water at Tampa Bay Beaches. Ph.D. Thesis, University of South Florida, Tampa, FL, USA, 2022. Available online: https://digitalcommons.usf.edu/etd/9452/ (accessed on 20 June 2023).
- McGowan, E. Comment on “Antibiotic Resistance Genes as Emerging Contaminants: Studies in Northern Colorado”. Environ. Sci. Technol. 2007, 41, 2651–2652. [Google Scholar] [CrossRef]
- Overbey, K.N.; Hatcher, S.M.; Stewart, J.R. Water quality and antibiotic resistance at beaches of the Galápagos Islands. Front. Environ. Sci. 2015, 3, 64. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Gallard, J.; Wu, B.; Harwood, V.J.; Sadowsky, M.J.; Hamilton, K.A.; Ahmed, W. Synergy between quantitative microbial source tracking (qMST) and quantitative microbial risk assessment (QMRA): A review and prospectus. Environ. Int. 2019, 130, 104703. [Google Scholar] [CrossRef]
- Nappier, S.P.; Liguori, K.; Ichida, A.M.; Stewart, J.R.; Jones, K.R. Antibiotic Resistance in Recreational Waters: State of the Science. Int. J. Environ. Res. Public Health 2020, 17, 8034. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, L.; Manaia, C.; Merlin, C.; Schwartz, T.; Dagot, C.; Ploy, M.C.; Michael, I.; Fatta-Kassinos, D. Urban wastewater treatment plants as hotspots for antibiotic resistant bacteria and genes spread into the environment: A review. Sci. Total Environ. 2013, 447, 345–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinos, G.P. The macrolide antibiotic renaissance. Br. J. Pharmacol. 2017, 174, 2967–2983. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.; Markham, A.; Balfour, J.A. Ciprofloxacin, an updated review of its pharmacology, therapeutic efficacy, and tolerability. Drugs 1996, 51, 1019–1074. [Google Scholar] [CrossRef] [PubMed]
- Peechakara, B.V.; Basit, H.; Gupta, M. Ampicillin. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2022. Available online: https://pubmed.ncbi.nlm.nih.gov/30137853/ (accessed on 20 June 2023).
- Sayah, R.S.; Kaneene, J.B.; Johnson, Y.; Miller, R.S. Patterns of antimicrobial resistance observed in Escherichia coli isolates obtained from domestic- and wild-animal fecal samples, human septage, and surface water. Appl. Environ. Microbiol. 2005, 71, 1394–1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolau, D.P.; Carmeli, Y.; Crank, C.W.; Goff, D.A.; Graber, C.J.; Lima, A.L.L.; Goldstein, E.J. Carbapenem stewardship: Does ertapenem affect Pseudomonas susceptibility to other carbapenems? A review of the evidence. Int. J. Antimicrob. Agents 2012, 39, 11–15. [Google Scholar] [CrossRef]
- van Loon, K.; Voor in ‘t holt, A.F.; Vos, M.C. A systematic review and meta-analyses of the clinical epidemiology of carbapenem-resistant enterobacteriaceae. Antimicrob Agents Chemother 2018, 62, 1. [Google Scholar] [CrossRef] [Green Version]
- Cohen, R.; Paikin, S.; Rokney, A.; Rubin-Blum, M.; Astrahan, P. Multidrug-resistant enterobacteriaceae in coastal water: An emerging threat. Antimicrob. Resist. Infect. Control. 2020, 9, 1–9. [Google Scholar] [CrossRef]
- Khan, F.A.; Hellmark, B.; Ehricht, R.; Söderquist, B.; Jass, J. Related carbapenemase-producing Klebsiella isolates detected in both a hospital and associated aquatic environment in Sweden. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 2241–2251. [Google Scholar] [CrossRef] [Green Version]
- Kieffer, N.; Poirel, L.; Bessa, L.J.; Barbosa-Vasconcelos, A.; da Costa, P.M.; Nordmann, P. VIM-1, VIM-34, and IMP-8 Carbapenemase-Producing Escherichia coli Strains Recovered from a Portuguese River. Antimicrob. Agents Chemother. 2016, 60, 2585–2586. [Google Scholar] [CrossRef] [Green Version]
- Kittinger, C.; Lipp, M.; Folli, B.; Kirschner, A.; Baumert, R.; Galler, H.; Grisold, A.J.; Luxner, J.; Weissenbacher, M.; Farnleitner, A.H.; et al. Enterobacteriaceae Isolated from the River Danube: Antibiotic Resistances, with a Focus on the Presence of ESBL and Carbapenemases. PLoS ONE 2016, 11, e0165820. [Google Scholar] [CrossRef] [Green Version]
- Montezzi, L.F.; Campana, E.H.; Corrêa, L.L.; Justo, L.H.; Paschoal, R.P.; da Silva, I.L.V.D.; Souza, M.D.C.M.; Drolshagen, M.; Picão, R.C. Occurrence of carbapenemase-producing bacteria in coastal recreational waters. Int. J. Antimicrob. Agents 2015, 45, 174–177. [Google Scholar] [CrossRef]
- Paschoal, R.P.; Campana, E.H.; Corrêa, L.L.; Montezzi, L.F.; Barrueto, L.R.L.; da Silva, I.R.; Bonelli, R.R.; Castro, L.D.S.; Picão, R.C. Concentration and Variety of Carbapenemase Producers in Recreational Coastal Waters Showing Distinct Levels of Pollution. Antimicrob. Agents Chemother. 2017, 61, e01963-17. [Google Scholar] [CrossRef] [Green Version]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Liu, M.; Liu, L.; Liu, X.; Chen, H.; Yang, J. The antibiotic resistome of free-living and particle-attached bacteria under a reservoir cyanobacterial bloom. Environ. Int. 2018, 117, 107–115. [Google Scholar] [CrossRef]
- Brooks, J.; Adeli, A.; McLaughlin, M.R.; Miles, D.M. The effect of poultry manure application rate and AlCl3 treatment on bacterial fecal indicators in runoff. J. Water Heal. 2012, 10, 619–628. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A | |||||||||||
| Sample Site | Sep-20 | Oct-20 | Nov-20 | Dec-20 | Jan-21 | Mar-21 | Apr-21 | May-21 | Jun-21 | Jul-21 | Mean |
| 1-Pass Christian ** | 910 | 800 | 1020 | 440 | 16 | 22 | 660 | 430 | 120 | 400 | 481.8 * |
| 2-Pass Christian | 1060 | 3000 | 940 | 40 | 6 | 110 | 490 | 470 | 310 | 250 | 667.6 * |
| 3-Long Beach | 530 | 110 | 720 | 70 | 2 | 48 | 156 | 320 | 750 | 692 | 339.8 |
| 4-Long Beach | 2750 | 130 | 920 | 106 | 10 | 30 | 32 | 270 | 560 | 5100 | 990.8 * |
| 5-Gulfport | 60 | 26 | 88 | 720 | 0 | 2 | 120 | 360 | 1110 | 2240 | 472.6 |
| 6-Gulfport | 450 | 180 | 340 | 114 | 0 | 148 | 760 | 290 | 2170 | 2240 | 669.2 * |
| 7-Gulfport | 90 | 10 | 98 | 270 | 0 | 10 | 20 | 360 | 230 | 30 | 111.8 |
| 8-Biloxi | 80 | 120 | 104 | 270 | 0 | 22 | 220 | 510 | 190 | 300 | 181.6 |
| 9-Biloxi | 100 | 580 | 780 | 100 | 2 | 110 | 600 | 1560 | 110 | 1730 | 567.2 * |
| 10-Biloxi | 600 | 900 | 1050 | 148 | 4 | 10 | 290 | 1680 | 40 | 380 | 510.2 |
| B | |||||||||||
| Sample Site | Sep-20 | Oct-20 | Nov-20 | Dec-20 | Jan-21 | Mar-21 | Apr-21 | May-21 | Jun-21 | Jul-21 | Mean |
| 1-Pass Christian | 100 | 212 | 0 | 10 | 2 | 80 | 600 | 300 | 20 | 16 | 134 |
| 2-Pass Christian | 100 | 40 | 0 | 10 | 0 | 100 | 210 | 450 | 32 | 10 | 95.2 |
| 3-Long Beach | 100 | 0 | 8 | 4 | 2 | 8 | 28 | 100 | 18 | 24 | 29.2 |
| 4-Long Beach | 220 | 60 | 0 | 20 | 128 | 108 | 6 | 120 | 14 | 40 | 71.6 |
| 5-Gulfport | 0 | 2 | 0 | 110 | 0 | 10 | 2 | 280 | 110 | 32 | 54.6 |
| 6-Gulfport | 10 | 5400 | 0 | 0 | 0 | 20 | 330 | 52 | 540 | 14 | 636.6 |
| 7-Gulfport | 0 | 0 | 0 | 4 | 0 | 8 | 0 | 46 | 6 | 28 | 9.2 |
| 8-Biloxi | 0 | 10 | 2 | 2 | 0 | 28 | 40 | 114 | 10 | 4 | 21 |
| 9-Biloxi | 6100 | 22 | 0 | 2 | 0 | 4 | 58 | 450 | 80 | 30 | 674.6 |
| 10-Biloxi | 10 | 10 | 4 | 10 | 0 | 12 | 50 | 220 | 10 | 6 | 33.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mukherjee, M.; Cuthbert, R.E.; Aitken, E.; Gay, K.A.; McKinney, K.; Brooks, J.P. Revealing an Abundance of Microbial Fecal Contamination and Multidrug Resistant Bacteria in the Mississippi Gulf Coast. Water 2023, 15, 2339. https://doi.org/10.3390/w15132339
Mukherjee M, Cuthbert RE, Aitken E, Gay KA, McKinney K, Brooks JP. Revealing an Abundance of Microbial Fecal Contamination and Multidrug Resistant Bacteria in the Mississippi Gulf Coast. Water. 2023; 15(13):2339. https://doi.org/10.3390/w15132339
Chicago/Turabian StyleMukherjee, Maitreyee, Robyn E. Cuthbert, Emma Aitken, Kristi A. Gay, Katonia McKinney, and John P. Brooks. 2023. "Revealing an Abundance of Microbial Fecal Contamination and Multidrug Resistant Bacteria in the Mississippi Gulf Coast" Water 15, no. 13: 2339. https://doi.org/10.3390/w15132339