Prediction of Children’s Blood Lead Levels from Exposure to Lead in Schools’ Drinking Water—A Case Study in Tennessee, USA


Abstract
:1. Introduction
2. Methods
2.1. Data Collection
2.2. Risk Modeling
2.2.1. IEUBK Model
2.2.2. Bowers’ Model
2.2.3. Estimating At-Risk Students
3. Results
3.1. Investigation of Lead in Schools’ Drinking Water
3.2. Elementary Schools Assessment
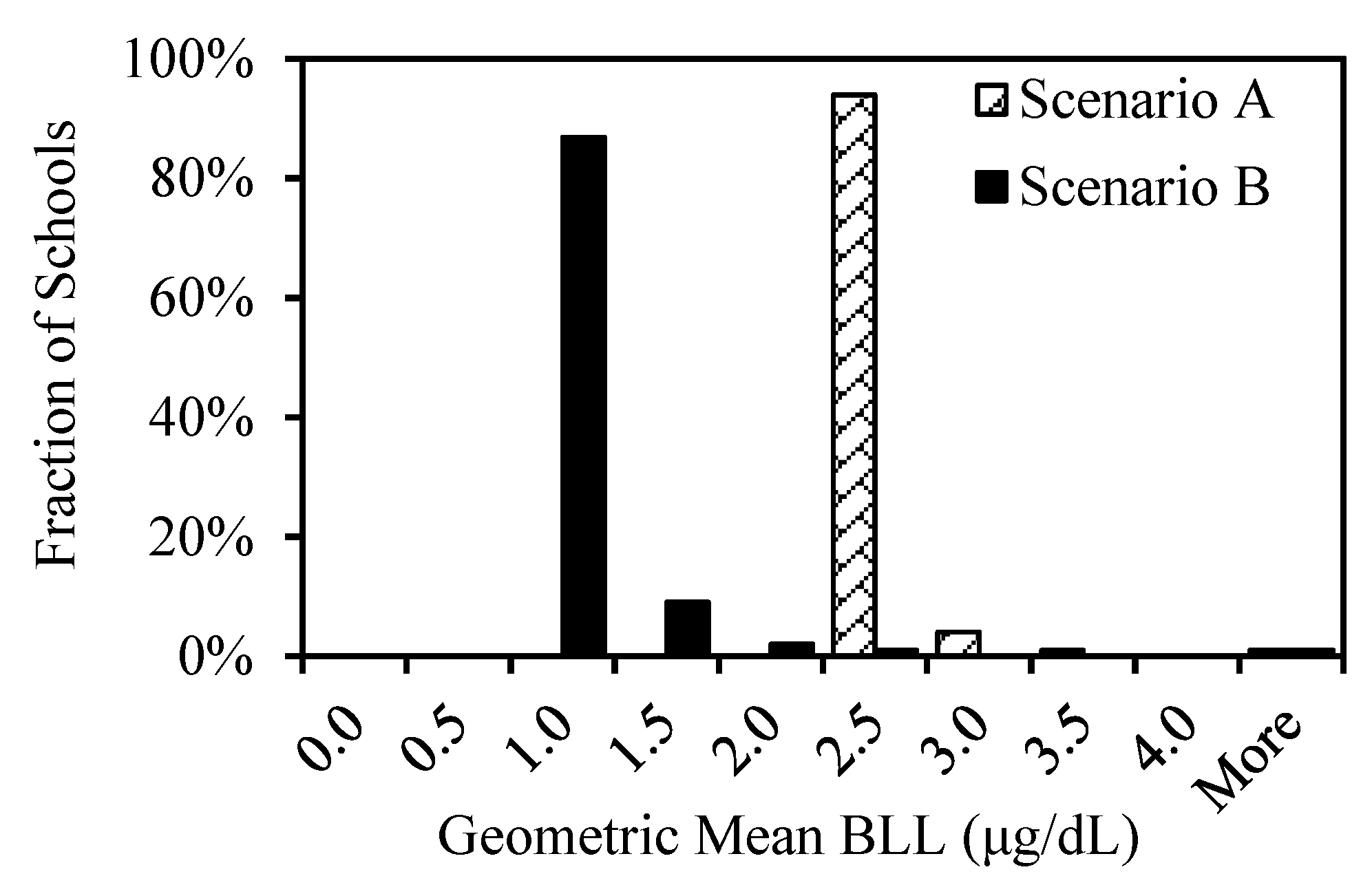
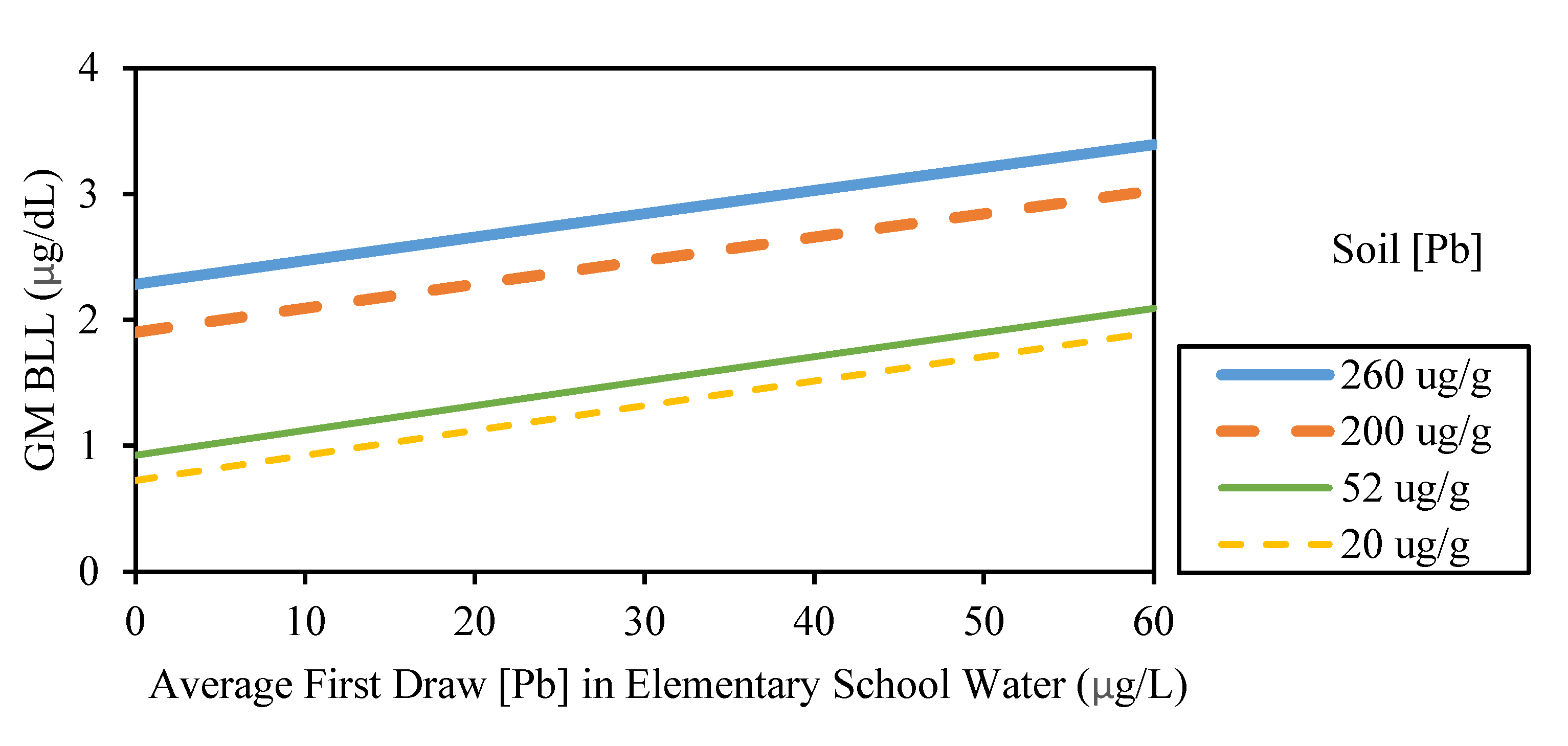
3.2.1. Geometric Mean BLL
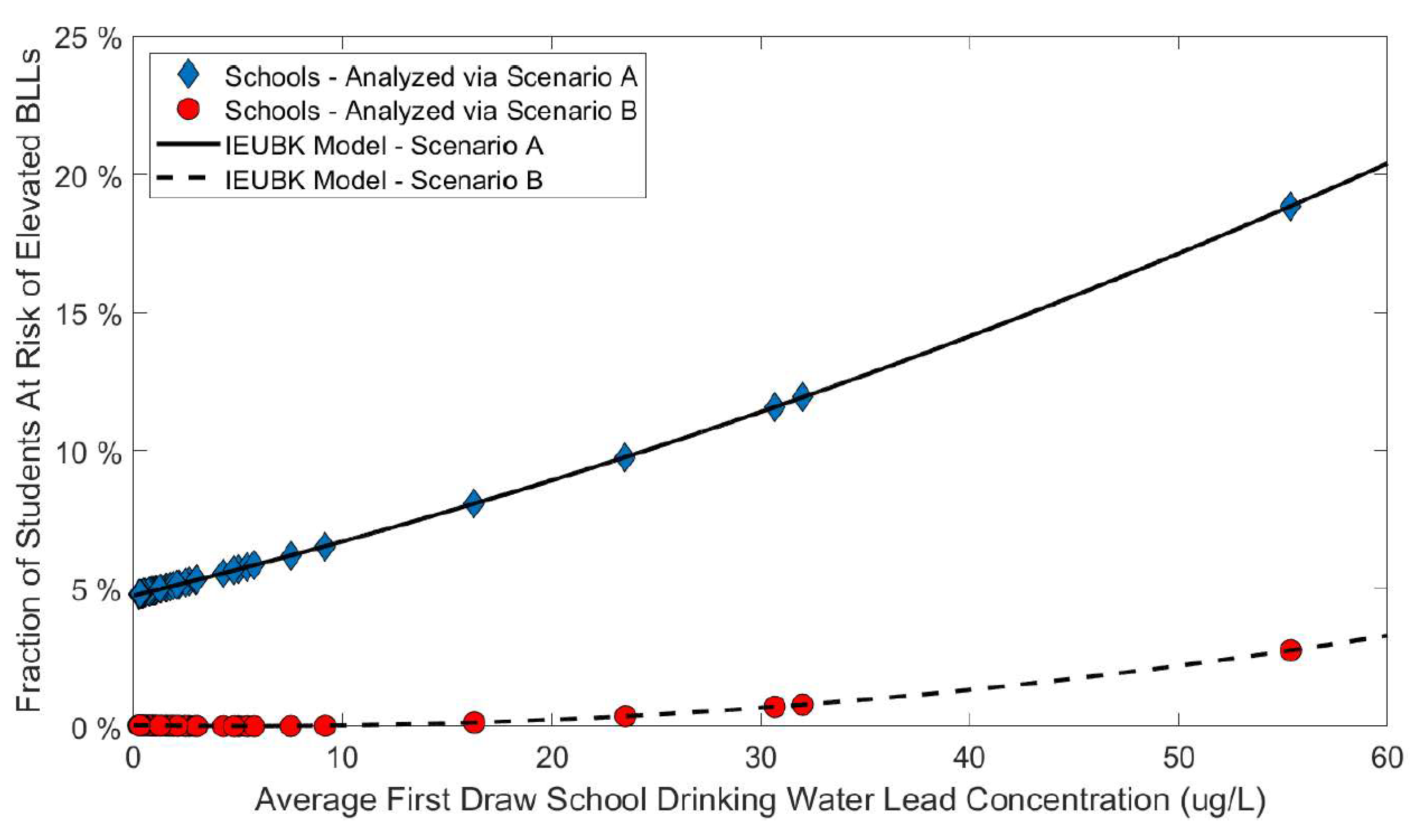
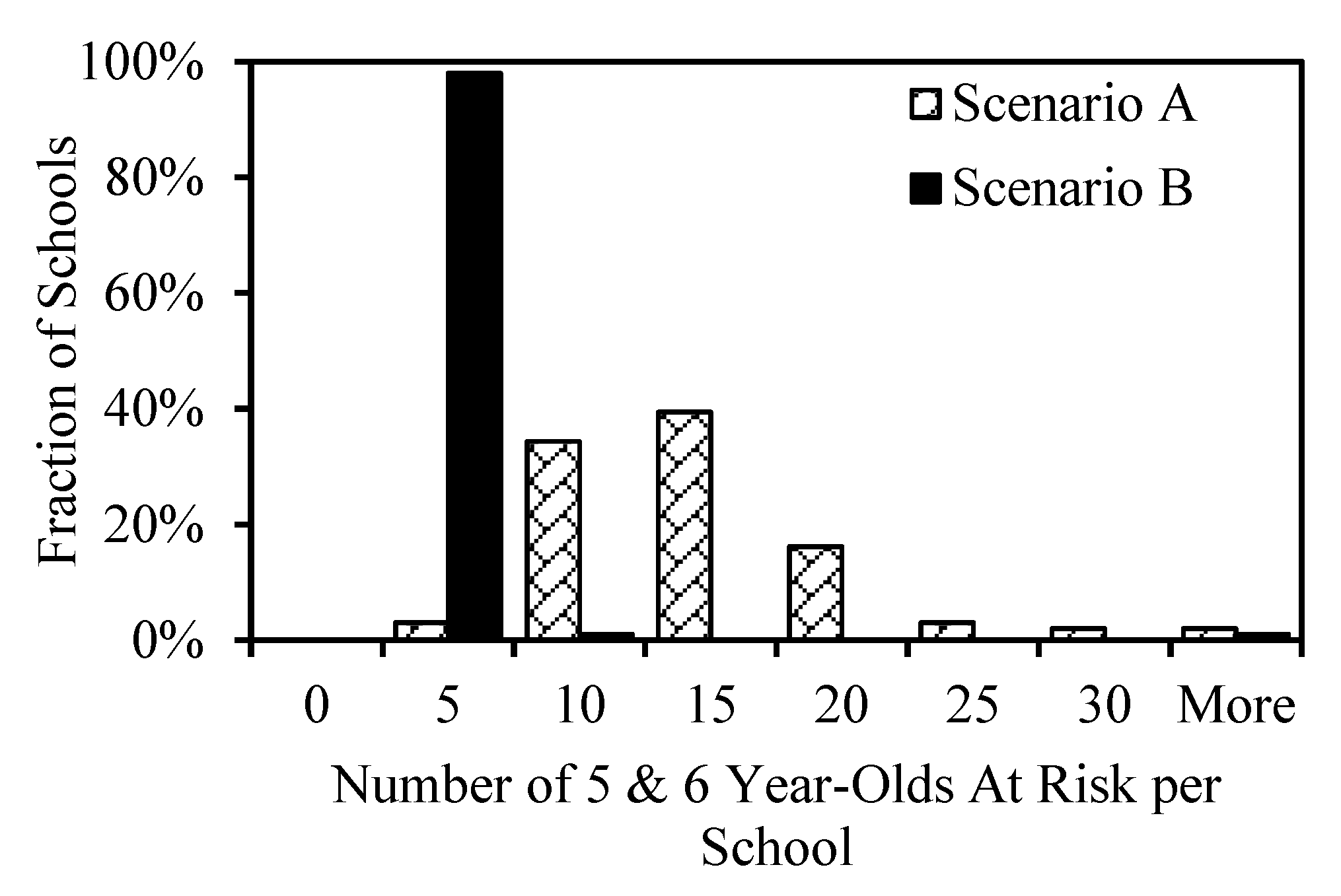
3.2.2. Percentage and Number of At-Risk Students
3.3. Secondary School Assessment
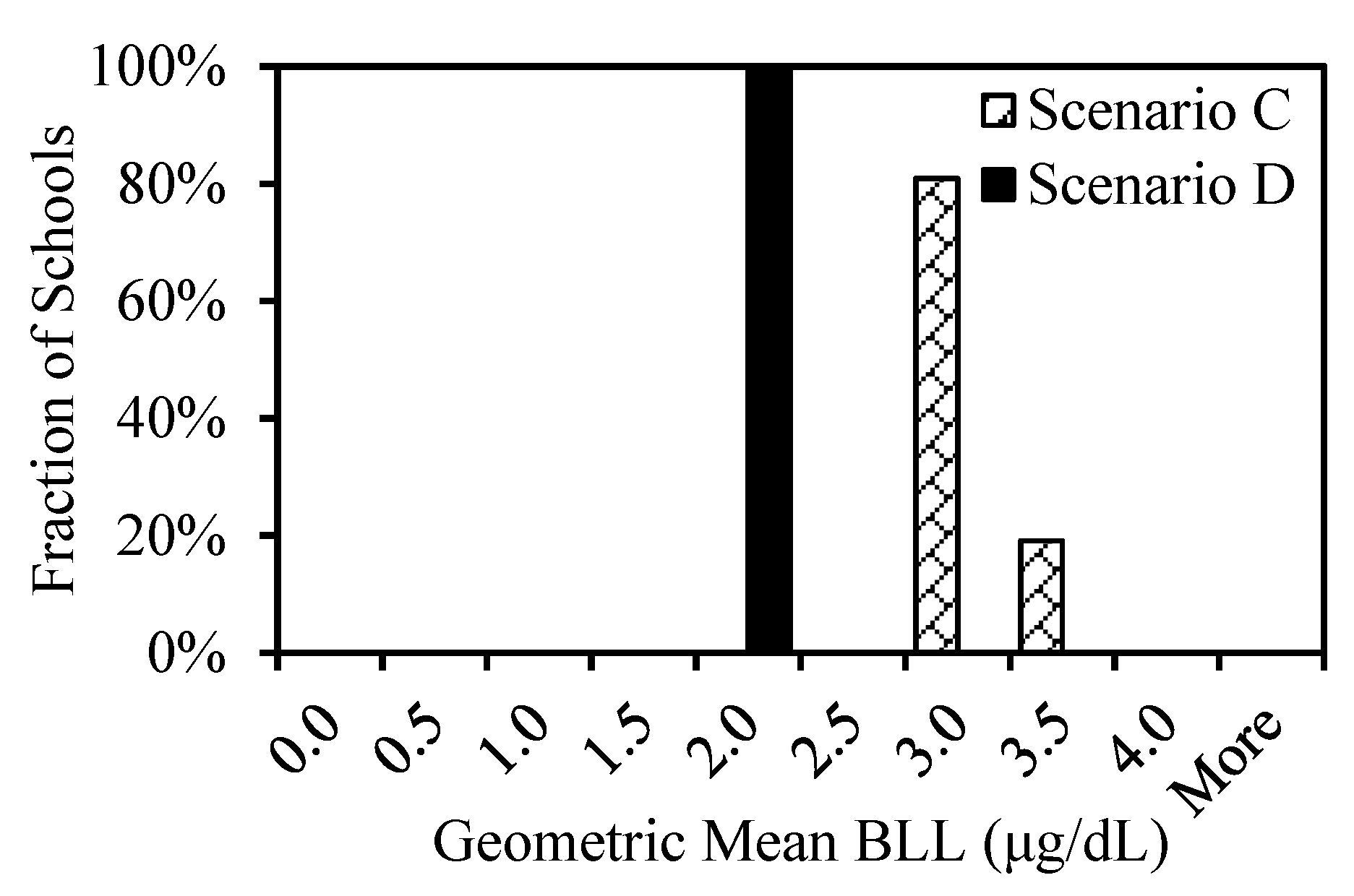
3.3.1. Geometric Mean BLL
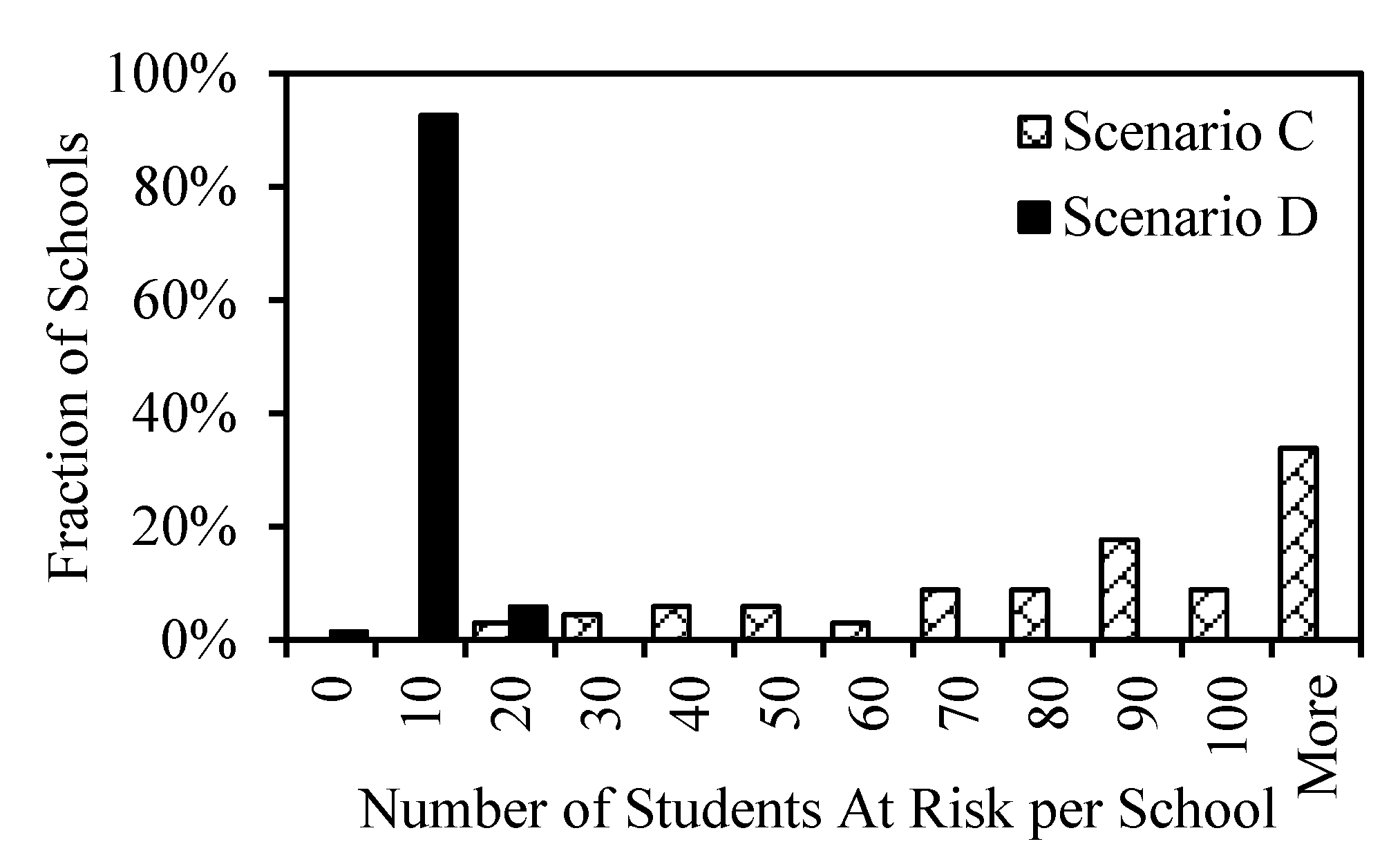
3.3.2. Percentage and Number of At-Risk Students
4. Discussion
4.1. Elementary School Assessment
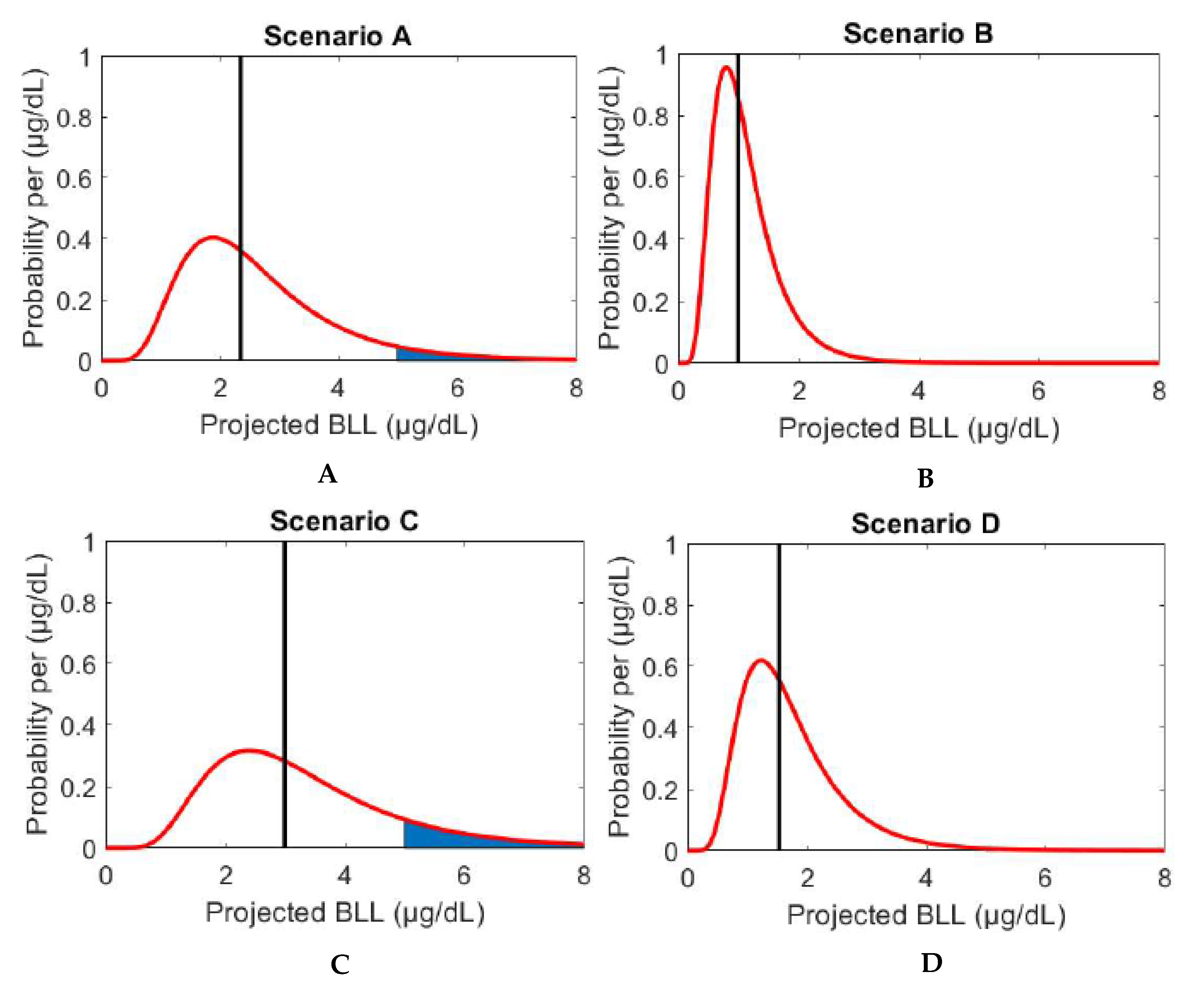
4.1.1. Scenario A
4.1.2. Scenario B
4.1.3. Comparison of Scenarios A & B
4.2. Secondary School Assessment
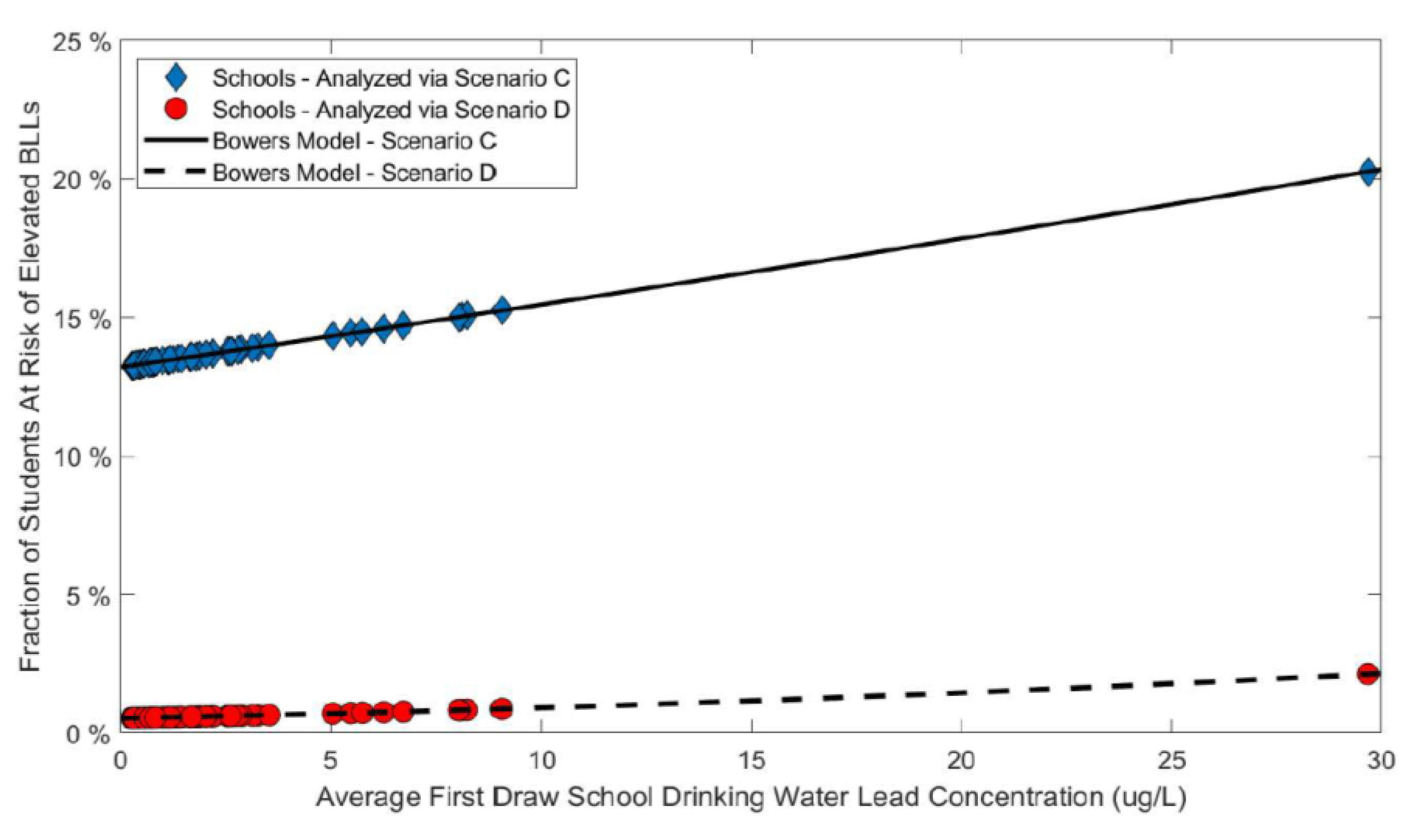
4.2.1. Scenario C
4.2.2. Scenario D
4.2.3. Comparison of Scenarios C & D
4.3. Sensitivity Analysis
4.3.1. IEUBK Model
4.3.2. Bowers’ Model
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Li, Y.; Hu, J.; Wu, W.; Liu, S.; Li, M.; Yao, N.; Chen, J.; Ye, L.; Wang, Q.; Zhou, Y. Application of IEUBK model in lead risk assessment of children aged 61-84 months old in central China. Sci.Total Environ. 2016, 541, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Jusko, T.; Henderson, C.R., Jr.; Lanphear, B.P.; Cory-Slechta, D.A.; Parsons, P.J.; Canfield, R.L. Blood Lead Concentrations <10 microg/dL and Child Intelligence at 6 Years of Age. Environ. Health Perspect. 2008, 116, 243–248. [Google Scholar] [CrossRef]
- Kwong, W.T.; Friello, P.; Semba, R. Interactions between iron deficiency and lead poisoning: Epidemiology and pathogenesis. Sci.Total Environ. 2004, 330, 21–37. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.S.; Koplewicz, H.S.; Klein, R.G. Teacher Ratings of Hyperactivity, Inattention, and Conduct Problems in Preschoolers. J. Abnorm. Child Psychol. 1997, 25, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Lanphear, B.P.; Dietrich, K.; Auinger, P.; Cox, C. Cognitive Deficits Associated with Blood Lead Concentrations <10 microg/dL in US Children and Adolescents. Public Health Rep. 2000, 115, 521. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, L.M.; Minter, M.L.; Cobb, K.A.; Scott, A.A.; German, V.F. Lead hazards for pregnant women and children: Part 1: Immigrants and the poor shoulder most of the burden of lead exposure in this country. Part 1 of a two-part article details how exposure happens, whom it affects, and the harm it can do. Am. J. Nurs. 2008, 108, 40–49. [Google Scholar] [CrossRef]
- Bowers, T.S.; Beck, B.D.; Karam, H.S. Assessing the Relationship Between Environmental Lead Concentrations and Adult Blood Lead Levels. Risk Anal. 1994, 14, 183–189. [Google Scholar] [CrossRef]
- Salehi, M.; Jafvert, C.T.; Howarter, J.A.; Whelton, A.J. Investigation of the factors that influence lead accumulation onto polyethylene: Implication for potable water plumbing pipes. J. Hazard. Mater. 2018, 347, 242–251. [Google Scholar] [CrossRef]
- Jain, N.B.; Laden, F.; Guller, U.; Shankar, A.; Kazani, S.; Garshick, E. Relation between blood lead levels and childhood anemia in India. Am. J. Epidemiol. 2005, 161, 968–973. [Google Scholar] [CrossRef] [Green Version]
- Bryant, S.D. Lead-Contaminated Drinking Waters in the Public Schools of Philadelphia. J. Toxicol. Clin. Toxicol. 2004, 42, 287–294. [Google Scholar] [CrossRef]
- Cornelis, C.; Berghmans, P.; van Sprundel, M.; Van der Auwera, J. Use of the IEUBK Model for Determinination of Exposure Routes in View of Site Remediation. Hum. Ecol. Risk Assess. 2006, 12, 963–982. [Google Scholar] [CrossRef]
- Boyd, G.R.; Pierson, G.L.; Kirmeyer, G.J.; English, R.J. Lead variability testing in Seattle Public Schools. JAWWA 2008, 100, 53–64. [Google Scholar] [CrossRef]
- Subramanian, K.S.; Sastri, V.S.; Elboujdaini, M.; Connor, J.W.; Davey, A.B.C. Water Contamination: Impact of tin-lead solder. Water Res. 1995, 29, 1827–1836. [Google Scholar] [CrossRef]
- Ahamed, T.; Brown, S.P.; Salehi, M. Investigate the Role of Biofilm and Water Chemistry on Lead Deposition onto and Release from Polyethylene: An Implication for Potable Water Pipes. J. Hazard. Mater. 2020. [Google Scholar] [CrossRef]
- Salehi, M.; Li, X.; Whelton, A. Metal Accumulation in Representative Plastic Drinking Water Plumbing Systems. JAWWA 2017, 109, E479–E493. [Google Scholar] [CrossRef] [Green Version]
- Salehi, M.; Odimayomi, T.; Ra, K.; Ley, C.; Julien, R.; Nejadhashemi, A.P.; Hernandez-Suare, J.S.; Mitchell, J.; Shah, A.D.; Whelton, A. An investigation of spatial and temporal drinking water quality variation in green residential plumbing. Build. Environ. 2020, 169, 106566. [Google Scholar] [CrossRef]
- Salehi, M.; Abouali, M.; Wang, M.; Zhou, Z.; Nejadhashemi, A.P.; Mitchell, J.; Caskey, S.; Whelton, A.J. Case Study: Fixture Water Use and Drinking Water Quality in a New Residential Green Building. Chemosphere 2018, 195, 80–89. [Google Scholar] [CrossRef]
- Control of Lead and Copper. In 40 CFR 141.80-General Requirements; Legal Information Institute: Ithaca, NY, USA, 1991.
- Council on Environmental Health. Prevention of Childhood Lead Toxicity. In Pediatrics; American Association of Pediatrics: Itasca, IL, USA, 2016. [Google Scholar]
- EPA U.S. Guidance Manual for the Integrated Exposure Uptake Biokinetic Model for Lead in Children; US Environmental Protection Agency: Washington, DC, USA, 1994.
- Albalak, R.; Noonan, G.; Buchanan, S.; Flanders, W.D.; Gotway-Crawford, C.; Kim, D.; Jones, R.L.; Sulaiman, R.; Blumenthal, W.; Tan, R.; et al. Blood lead levels and risk factors for lead poisoning among children in Jakarta, Indonesia. Sci. Total Environ. 2003, 301, 75–85. [Google Scholar] [CrossRef]
- Schwartz, J. Low-level lead exposure and children’s IQ: A meta-analysis and search for a threshold. Environ. Res. 1994, 65, 42–55. [Google Scholar] [CrossRef]
- Zhang, X.-Y.; Carpenter, D.O.; Song, Y.-J.; Chen, P.; Qin, Y.; Wei, N.-Y.; Lin, S.-C. Application of the IEUBK model for linking Children’s blood lead with environmental exposure in a mining site, south China. Environ. Pollut. 2017, 231, 971–978. [Google Scholar] [CrossRef]
- Laidlaw, M.; Mohmmad, S.M.; Gulson, B.L.; Taylor, M.P.; Kristensen, L.J.; Birch, G. Estimates of potential childhood lead exposure from contaminated soil using the US EPA IEUBK Model in Sydney, Australia. Environ. Res. 2017, 156, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Sathyanarayana, S.; Beaudet, N.; Omri, K.; Karr, C. Predicting Children’s Blood Lead Levels from Exposure to School Drinking Water in Seattle, Washington, USA. Ambul. Pediatr. 2006, 6, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Zhong, B.; Giubilato, E.; Critto, A.; Wang, L.; Marcomini, A.; Zhang, J. Probabilistic modeling of aggregate lead exposure in children of urban China using an adapted IEUBK model. Sci. Total Environ. 2017, 584–585, 259–267. [Google Scholar] [CrossRef]
- Triantafyllidou, S.; Le, T.; Gallagher, D.; Edwards, M. Reduced risk estimations after remediation of lead (Pb) in drinking water at two US school districts. Sci. Total Environ. 2014, 466–467, 1011–1021. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Caballero, M.R.; Valles-Aragón, M.C.; Millan, R.; Alarcón-Herrera, M.T. Risk Assessment Through IEUBK Model. in an Inhabited Area Contaminated with Lead. Environ. Prog. Sustain. Energy 2018, 37, 391–398. [Google Scholar] [CrossRef]
- Bowers, T.S.; Cohen, J.T. Blood Lead Slope Factor Models for Adults: Comparisons of Observations and Predictions. Environ. Health Perspect. 1998, 106 (Suppl. S6), 1569–1576. [Google Scholar] [CrossRef] [Green Version]
- Redmon, J.H.; Levine, K.E.; Aceituno, A.M.; Litzenberger, K.; Gibson, J.M. Lead in drinking water at North Carolina childcare centers: Piloting a citizen science-based testing strategy. Environ. Res. 2020, 183, 109126. [Google Scholar] [CrossRef]
- Deshommes, E.; Andrews, R.C.; Gagnon, G.; McCluskey, T.; McIlwain, B.; Doré, E.; Nour, S.; Prévost, M. Evaluation of exposure to lead from drinking water in large buildings. Water Res. 2016, 99, 46–55. [Google Scholar] [CrossRef]
- Costanza-Robinson, M.; Davis, G. Lead Levels in Drinking Water at Salisbury Community School, Salisbury VT. 2019. [Google Scholar]
- 40 CFR 141.86-Monitoring Requirements for Lead and Copper in Tap Water; Cornell Law School: Ithaca, NY, USA, 1991.
- Greatschools. Available online: https://www.greatschools.org/ (accessed on 21 November 2019).
- EPA U.S. IEUBK Model-Windows Version 1.1 Build 11; US Environmental Protection Agency: Washington, DC, USA, 2010.
- EPA U.S. Technical Support Document: Parameters and Equations Used in the Integrated Exposure Uptake Biokinetic Model for Lead in Children (v0.99d); US Environmental Protection Agency: Washington, DC, USA, 1994.
- EPA U.S. User’s Guide for the Integrated Exposure Uptake Biokinetic Model for Lead in Children (IEUBK) Windows; US Environmental Protection Agency: Washington, DC, USA, 2007.
- EPA U.S. Overview of the Clean Air Act and Air Pollution; US Environmental Protection Agency: Washington, DC, USA, 1990.
- MLGW. Memphis Water: Pure and Abundant Water Quality Report 2016; MLGW: Memphis, TN, USA, 2016; pp. 1–8. [Google Scholar]
- EPA U.S. A TRW Report: Review of a Methodology for Establishing Risk-Based Soil Remediation Goals for the Commerical Areas of the California Gulch Site; US Environmental Protection Agency: Washington, DC, USA, 1995.
- EPA U.S. EPA U.S. A TRW Report: Review of the EPA Uptake Biokinetic Model for Lead at the Butte NPL Site; US Environmental Protection Agency: Washington, DC, USA, 1992.
- Zartarian, V.; Xue, J.; Tornero-Velez, R.; Brown, J. Children’s Lead Exposure: A Multimedia Modeling Analysis to Guide Public Health Decision-Making. Environ. Health Perspect. 2017, 125. [Google Scholar] [CrossRef] [Green Version]
- Frederick, T.; Chan, S. EPA Tools and Resources Webinar: Urban. Background Study; US Environmental Protection Agency: Washington, DC, USA, 2018.
- WHO. Childhood Lead Poisoning 2010. Available online: https://www.who.int/ceh/publications/childhoodpoisoning/en/ (accessed on 25 June 2020).
- Lambrinidou, Y.; Triantafyllidou, S.; Edwards, M. Failing Our Children: Lead in U.S. School Drinking Water. New Solut. J. Environ. Occupat. Health Policy 2010, 20, 25–47. [Google Scholar]
- H.R.4939-Lead Contamination Control Act of 1988; United States Congress: Washington, DC, USA, 1988.
- Act to Amend Tennessee Code Annotated, Title 49; Title 68 and Title 69, Relative to Water Quality in Schools; Tennessee General Assembly: Nashville, TN, USA, 2018.
- Smith, D.B.; Cannon, W.F.; Woodruff, L.G.; Solano, F.; Kilburn, J.E.; Fey, D.L. Geochemical and Mineralogical Data for Soils of the Conterminous United States; U.S. Geological Survey: Reston, VA, USA, 2013.
- Proctor, C.; Rhoads, W.; Keane, T.; Salehi, M.; Hamilton, K.; Pieper, K.; Cwiertny, D.; Prevost, M.; Whelton, A. Considerations for Large Building Water Quality after Extended Stagnation. AWWA Water Sci. 2020, e1186. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Schools | Elementary Schools | Middle Schools | High Schools | |||
|---|---|---|---|---|---|---|
| 2017 | 2019 | 2017 | 2019 | 2017 | 2019 | |
| Schools sampled | 39 | 99 | 16 | 25 | 17 | 36 |
| Schools with [Pb] > 1 μg/L | 34 | 90 | 13 | 21 | 13 | 34 |
| Schools with [Pb] > 10 μg/L | 7 | 26 | 0 | 5 | 5 | 18 |
| Schools with [Pb] > 15 μg/L | 5 | 20 | 0 | 5 | 4 | 16 |
| Total sampled | 270 | 1923 | 112 | 613 | 118 | 892 |
| Fixtures with [Pb] > 15 μg/L | 26 | 43 | 0 | 14 | 5 | 19 |
| Maximum [Pb] (μg/L) | 53 | 18,800 | 9 | 140 | 99 | 285 |
| Median [Pb] (μg/L) | 6 | 227 | 3 | 16 | 12 | 30 |
| Range (μg/L) | <0.5–53 | <0.5–18,800 | <0.5–9 | <0.5–140 | <0.5–99 | <0.5–285 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
DeSimone, D.; Sharafoddinzadeh, D.; Salehi, M. Prediction of Children’s Blood Lead Levels from Exposure to Lead in Schools’ Drinking Water—A Case Study in Tennessee, USA. Water 2020, 12, 1826. https://doi.org/10.3390/w12061826
DeSimone D, Sharafoddinzadeh D, Salehi M. Prediction of Children’s Blood Lead Levels from Exposure to Lead in Schools’ Drinking Water—A Case Study in Tennessee, USA. Water. 2020; 12(6):1826. https://doi.org/10.3390/w12061826
Chicago/Turabian StyleDeSimone, Dave, Donya Sharafoddinzadeh, and Maryam Salehi. 2020. "Prediction of Children’s Blood Lead Levels from Exposure to Lead in Schools’ Drinking Water—A Case Study in Tennessee, USA" Water 12, no. 6: 1826. https://doi.org/10.3390/w12061826