
Expression and Clinical Significance of Androgen Receptor in Triple-Negative Breast Cancer

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Background
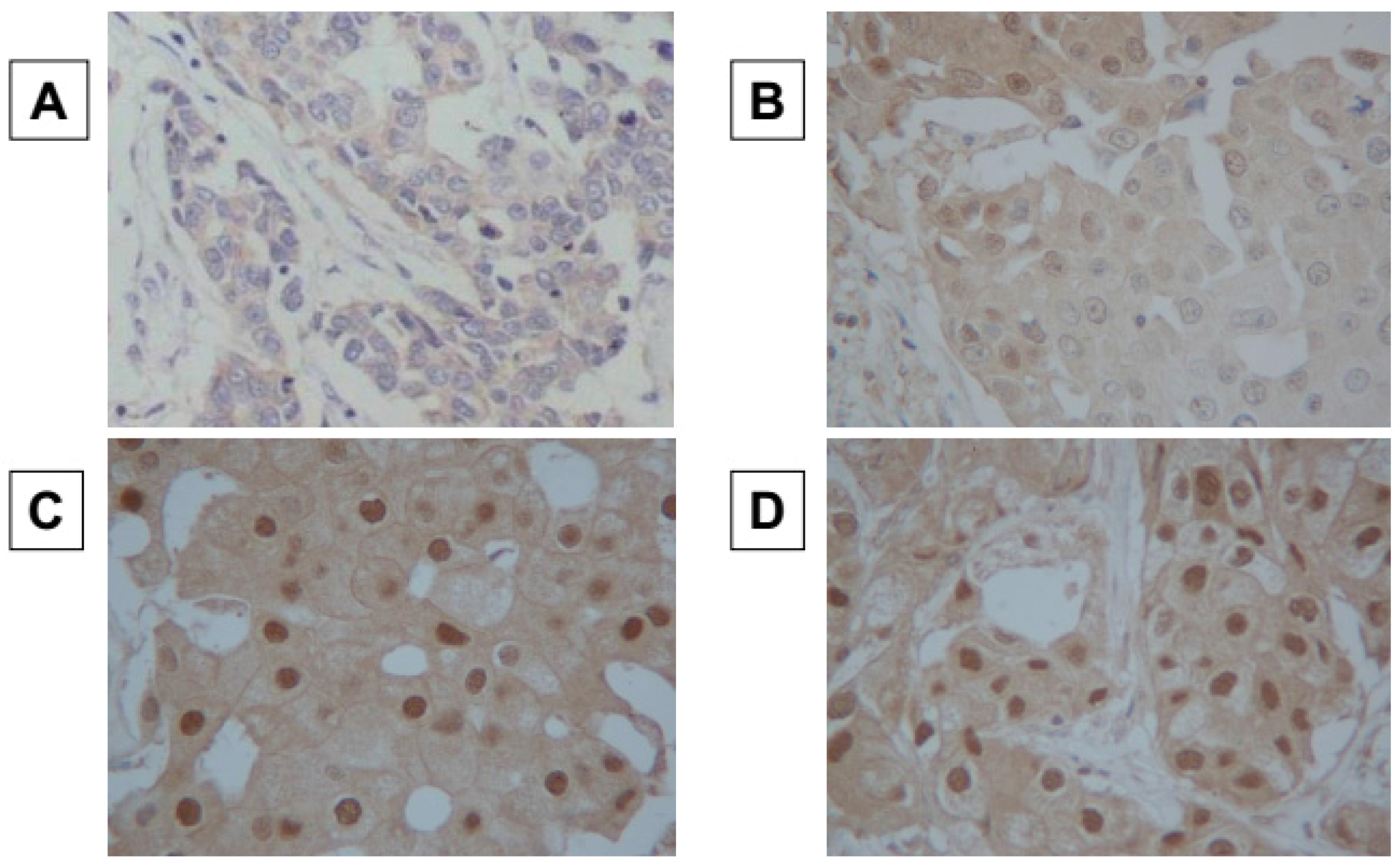
2.2. Immunohistochemistry
2.3. Immunohistochemical Scoring
2.4. Statistical Analysis
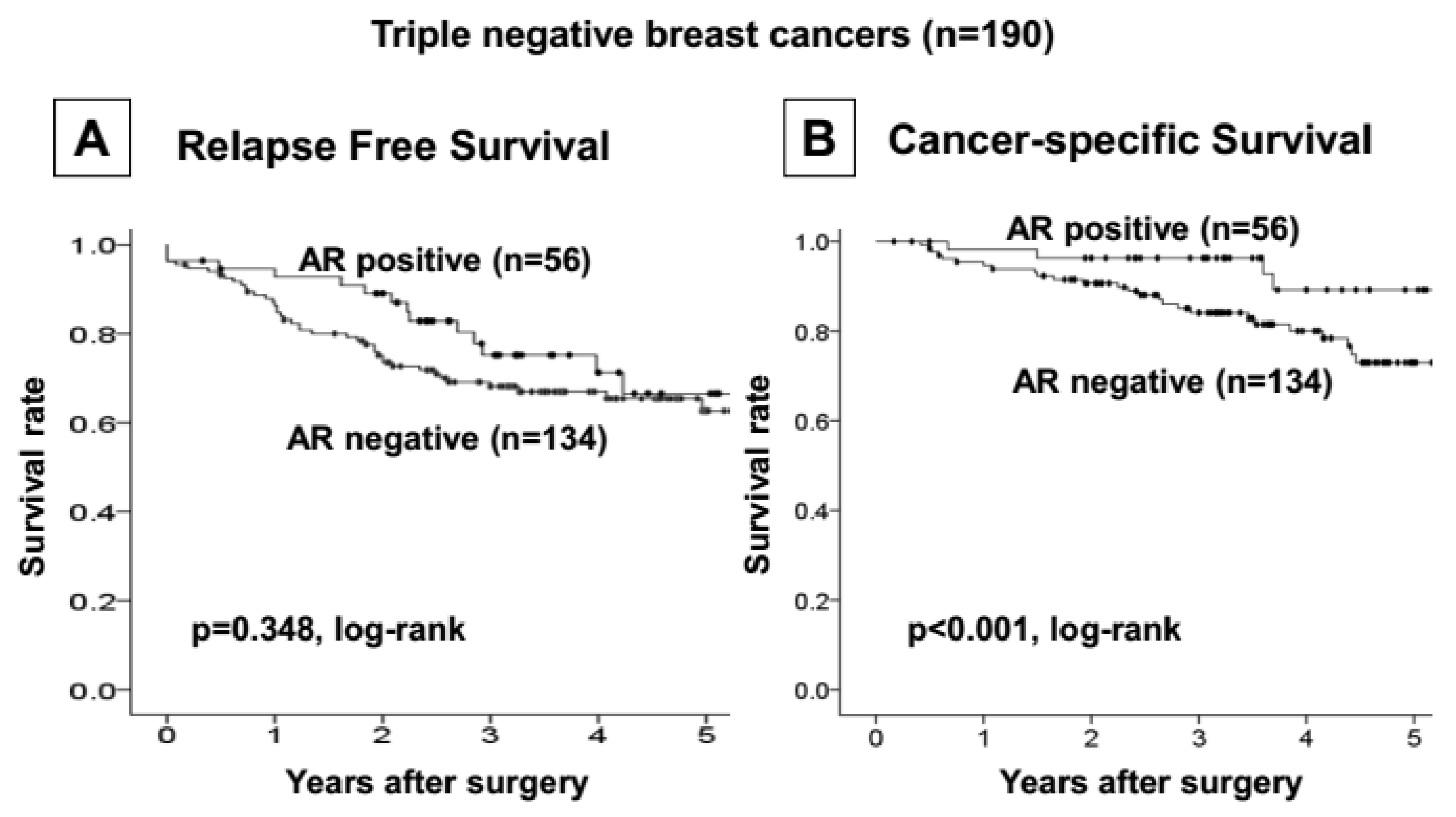
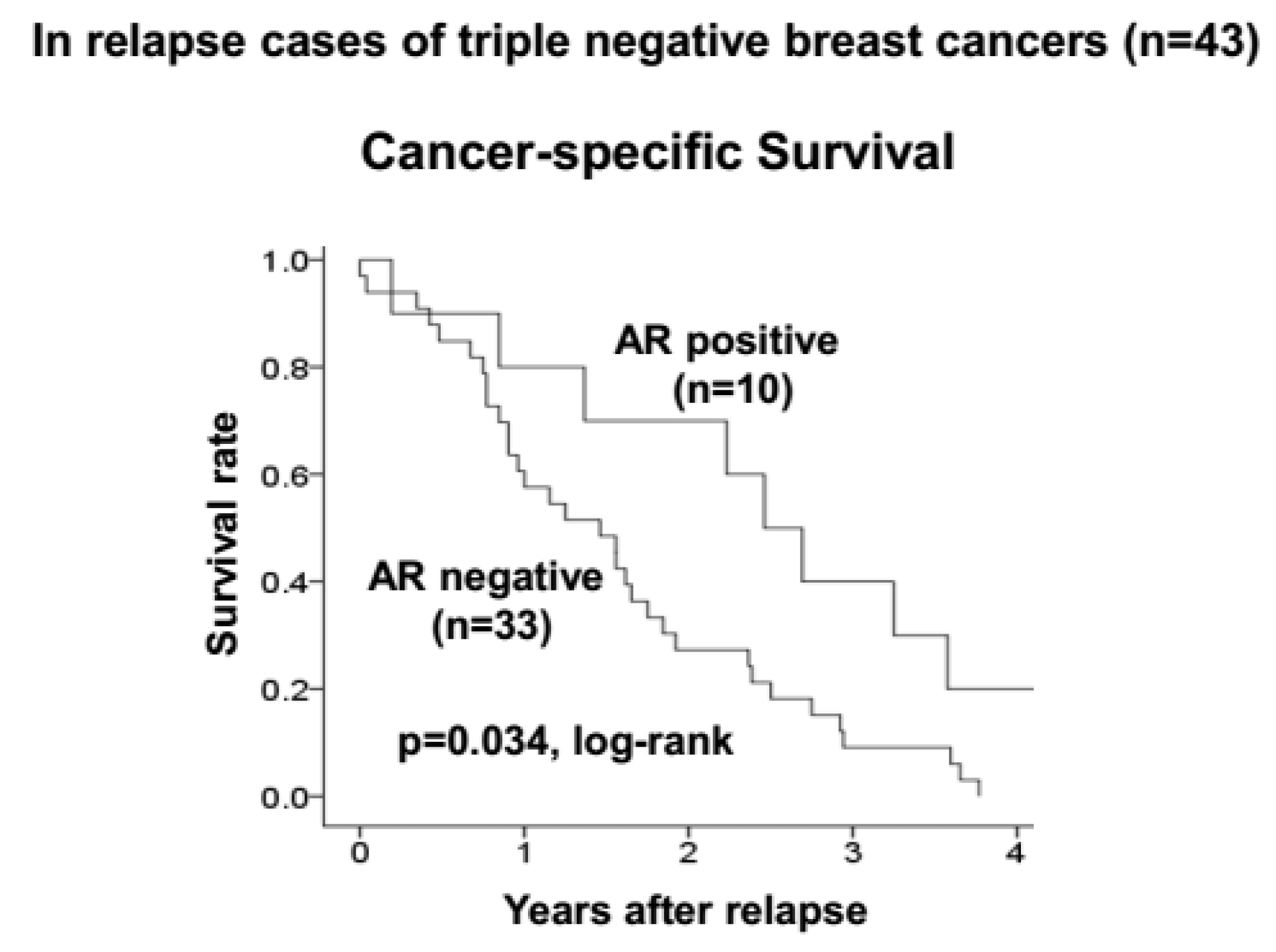
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Abd El-Rehim, D.M.; Ball, G.; Pinder, S.E.; Rakha, E.; Paish, C.; Robertson, J.F.; Macmillan, D.; Blamey, R.W.; Ellis, I.O. High-throughput protein expression analysis using tissue microarray technology of a large well-characterised series identifies biologically distinct classes of breast cancer confirming recent cDNA expression analyses. Int. J. Cancer 2005, 116, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Mattie, M.D.; Benz, C.C.; Bowers, J.; Sensinger, K.; Wong, L.; Scott, G.K.; Fedele, V.; Ginzinger, D.; Getts, R.; Haqq, C. Optimized high-throughput microRNA expression profiling provides novel biomarker assessment of clinical prostate and breast cancer biopsies. Mol. Cancer 2006, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- Perou, C.M.; Sorlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Sorlie, T.; Perou, C.M.; Tibshirani, R.; Aas, T.; Geisler, S.; Johnsen, H.; Hastie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl. Acad. Sci. USA 2001, 98, 10869–10874. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, T.O.; Hsu, F.D.; Jensen, K.; Cheang, M.; Karaca, G.; Hu, Z.; Hernandez-Boussard, T.; Livasy, C.; Cowan, D.; Dressler, L.; et al. Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin. Cancer Res. 2004, 10, 5367–5374. [Google Scholar] [CrossRef] [PubMed]
- Perou, C.M. Molecular stratification of triple-negative breast cancers. Oncologist 2011, 16, S61–S70. [Google Scholar] [CrossRef] [PubMed]
- Bauer, C.; Peigne, V.; Gisselbrecht, M. Unusual presentation of myeloma in an elderly woman: Breast and cutaneous involvement. Eur. J. Intern. Med. 2008, 19, 150–151. [Google Scholar] [CrossRef] [PubMed]
- Rakha, E.A.; El-Sayed, M.E.; Green, A.R.; Lee, A.H.; Robertson, J.F.; Ellis, I.O. Prognostic markers in triple-negative breast cancer. Cancer 2007, 109, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Sorlie, T.; Tibshirani, R.; Parker, J.; Hastie, T.; Marron, J.S.; Nobel, A.; Deng, S.; Johnsen, H.; Pesich, R.; Geisler, S.; et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc. Natl. Acad. Sci. USA 2003, 100, 8418–8423. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J. Clin. Investig. 2011, 121, 2750–2767. [Google Scholar] [CrossRef] [PubMed]
- Metzger-Filho, O.; Tutt, A.; de Azambuja, E.; Saini, K.S.; Viale, G.; Loi, S.; Bradbury, I.; Bliss, J.M.; Azim, H.A., Jr.; Ellis, P.; et al. Dissecting the heterogeneity of triple-negative breast cancer. J. Clin. Oncol. 2012, 30, 1879–1887. [Google Scholar] [CrossRef] [PubMed]
- Gucalp, A.; Traina, T.A. Triple-negative breast cancer: Role of the androgen receptor. Cancer J. 2010, 16, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Gucalp, A.; Tolaney, S.; Isakoff, S.J.; Ingle, J.N.; Liu, M.C.; Carey, L.A.; Blackwell, K.; Rugo, H.; Nabell, L.; Forero, A.; et al. Phase II trial of bicalutamide in patients with androgen receptor-positive, estrogen receptor-negative metastatic Breast Cancer. Clin. Cancer Res. 2013, 19, 5505–5512. [Google Scholar] [CrossRef] [PubMed]
- Kuenen-Boumeester, V.; Van der Kwast, T.H.; Claassen, C.C.; Look, M.P.; Liem, G.S.; Klijn, J.G.; Henzen-Logmans, S.C. The clinical significance of androgen receptors in breast cancer and their relation to histological and cell biological parameters. Eur. J. Cancer 1996, 32A, 1560–1565. [Google Scholar] [CrossRef] [Green Version]
- Ando, S.; De Amicis, F.; Rago, V.; Carpino, A.; Maggiolini, M.; Panno, M.L.; Lanzino, M. Breast cancer: From estrogen to androgen receptor. Mol. Cell. Endocrinol. 2002, 193, 121–128. [Google Scholar] [CrossRef]
- De Launoit, Y.; Veilleux, R.; Dufour, M.; Simard, J.; Labrie, F. Characteristics of the biphasic action of androgens and of the potent antiproliferative effects of the new pure antiestrogen EM-139 on cell cycle kinetic parameters in LNCaP human prostatic cancer cells. Cancer Res. 1991, 51, 5165–5170. [Google Scholar] [PubMed]
- Poulin, R.; Baker, D.; Labrie, F. Androgens inhibit basal and estrogen-induced cell proliferation in the ZR-75–1 human breast cancer cell line. Breast Cancer Res. Treat. 1988, 12, 213–225. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Peng, R.; Yuan, Z.; Wang, S.; Peng, J.; Lin, G.; Jiang, X.; Qin, T. Prognostic value of androgen receptor expression in operable triple-negative breast cancer: A retrospective analysis based on a tissue microarray. Med. Oncol. 2012, 29, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.; Dawood, S.; Holmes, M.D.; Collins, L.C.; Schnitt, S.J.; Cole, K.; Marotti, J.D.; Hankinson, S.E.; Colditz, G.A.; Tamimi, R.M. Androgen receptor expression and breast cancer survival in postmenopausal women. Clin. Cancer Res. 2011, 17, 1867–1874. [Google Scholar] [CrossRef] [PubMed]
- McGhan, L.J.; McCullough, A.E.; Protheroe, C.A.; Dueck, A.C.; Lee, J.J.; Nunez-Nateras, R.; Castle, E.P.; Gray, R.J.; Wasif, N.; Goetz, M.P.; et al. Androgen receptor-positive triple negative breast cancer: A unique breast cancer subtype. Ann. Surg. Oncol. 2014, 21, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Mrklic, I.; Pogorelic, Z.; Capkun, V.; Tomic, S. Expression of androgen receptors in triple negative breast carcinomas. Acta Histochem. 2013, 115, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.L.; Macarthur, S.; Ross-Innes, C.S.; Tilley, W.D.; Neal, D.E.; Mills, I.G.; Carroll, J.S. Androgen receptor driven transcription in molecular apocrine breast cancer is mediated by FoxA1. EMBO J. 2011, 30, 3019–3027. [Google Scholar] [CrossRef] [PubMed]
- Sutton, L.M.; Cao, D.; Sarode, V.; Molberg, K.H.; Torgbe, K.; Haley, B.; Peng, Y. Decreased androgen receptor expression is associated with distant metastases in patients with androgen receptor-expressing triple-negative breast carcinoma. Am. J. Clin. Pathol. 2012, 138, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Fioretti, F.M.; Sita-Lumsden, A.; Bevan, C.L.; Brooke, G.N. Revising the role of the androgen receptor in breast cancer. J. Mol. Endocrinol. 2014, 52, R257–R265. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, S.; Yashiro, M.; Takashima, T.; Aomatsu, N.; Kawajiri, H.; Ogawa, Y.; Onoda, N.; Ishikawa, T.; Wakasa, K.; Hirakawa, K. c-Kit expression as a prognostic molecular marker in patients with basal-like breast cancer. Br. J. Surg. 2013, 100, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef] [PubMed]
- Goldhirsch, A.; Wood, W.C.; Coates, A.S.; Gelber, R.D.; Thurlimann, B.; Senn, H.J. Panel members. Strategies for subtypes—Dealing with the diversity of breast cancer: Highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann. Oncol. 2011, 22, 1736–1747. [Google Scholar] [CrossRef] [PubMed]
- Asano, Y.; Kashiwagi, S.; Onoda, N.; Kurata, K.; Morisaki, T.; Noda, S.; Takashima, T.; Ohsawa, M.; Kitagawa, S.; Hirakawa, K. Clinical verification of sensitivity to preoperative chemotherapy in cases of androgen receptor-expressing positive breast cancer. Br. J. Cancer 2016, 114, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Castellano, I.; Allia, E.; Accortanzo, V.; Vandone, A.M.; Chiusa, L.; Arisio, R.; Durando, A.; Donadio, M.; Bussolati, G.; Coates, A.S.; et al. Androgen receptor expression is a significant prognostic factor in estrogen receptor positive breast cancers. Breast Cancer Res. Treat. 2010, 124, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Shi, Y.X.; Li, Z.M.; Jiang, W.Q. Expression and clinical significance of androgen receptor in triple negative breast cancer. Chin. J. Cancer 2010, 29, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Masuda, H.; Baggerly, K.A.; Wang, Y.; Zhang, Y.; Gonzalez-Angulo, A.M.; Meric-Bernstam, F.; Valero, V.; Lehmann, B.D.; Pietenpol, J.A.; Hortobagyi, G.N.; et al. Differential response to neoadjuvant chemotherapy among 7 triple-negative breast cancer molecular subtypes. Clin. Cancer Res. 2013, 19, 5533–5540. [Google Scholar] [CrossRef] [PubMed]
- Gasparini, P.; Fassan, M.; Cascione, L.; Guler, G.; Balci, S.; Irkkan, C.; Paisie, C.; Lovat, F.; Morrison, C.; Zhang, J.; et al. Androgen receptor status is a prognostic marker in non-basal triple negative breast cancers and determines novel therapeutic options. PLoS ONE 2014, 9, e88525. [Google Scholar] [CrossRef] [PubMed]
- McNamara, K.M.; Yoda, T.; Miki, Y.; Chanplakorn, N.; Wongwaisayawan, S.; Incharoen, P.; Kongdan, Y.; Wang, L.; Takagi, K.; Mayu, T.; et al. Androgenic pathway in triple negative invasive ductal tumors: Its correlation with tumor cell proliferation. Cancer Sci. 2013, 104, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Mohammadizadeh, F.; Sajadieh, S.; Sajjadieh, H.; Kasaei, Z. Androgen receptor expression and its relationship with clinicopathological parameters in an Iranian population with invasive breast carcinoma. Adv. Biomed. Res. 2014, 3, 132. [Google Scholar] [PubMed]
- Greeve, M.A.; Allan, R.K.; Harvey, J.M.; Bentel, J.M. Inhibition of MCF-7 breast cancer cell proliferation by 5alpha-dihydrotestosterone; a role for p21(Cip1/Waf1). J. Mol. Endocrinol. 2004, 32, 793–810. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, R.; Dalton, J.T. Androgen receptor: A complex therapeutic target for breast cancer. Cancers 2016, 8, 108. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, D.R.; Bernales, S.; Jacobsen, B.M.; Cittelly, D.M.; Howe, E.N.; D’Amato, N.C.; Spoelstra, N.S.; Edgerton, S.M.; Jean, A.; Guerrero, J.; et al. Role of the androgen receptor in breast cancer and preclinical analysis of enzalutamide. Breast Cancer Res. 2014, 16, R7. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Androgen Receptor | p Value | |
|---|---|---|---|
| Positive (n = 56) | Negative (n = 134) | ||
| Age at operation | |||
| ≤55 | 27 (48.2%) | 57 (42.5%) | |
| >55 | 29 (51.8%) | 77 (57.5%) | 0.473 |
| Stage | |||
| 1 | 16 (28.6%) | 43 (32.1%) | |
| 2–4 | 40 (71.4%) | 91 (67.9%) | 0.633 |
| Tumor size (cm) | |||
| ≤2 | 21 (37.5%) | 54 (40.3%) | |
| >2 | 35 (62.5%) | 80 (59.7%) | 0.719 |
| Lymph node status | |||
| Negative | 34 (60.7%) | 81 (60.4%) | |
| Positive | 22 (39.3%) | 53 (39.6%) | 0.973 |
| Lymphatic invasion | |||
| Negative | 44 (78.6%) | 91 (67.9%) | |
| Positive | 12 (21.4%) | 43 (32.1%) | 0.140 |
| Vascular invasion | |||
| Negative | 56 (100.0%) | 129 (96.3%) | |
| Positive | 0 (0%) | 5 (3.7%) | 0.171 |
| Histologic type | |||
| IDC | 48 (85.6%) | 116 (86.6%) | |
| Special type | 8 (14.3%) | 18 (13.4%) | 0.876 |
| Histological grade | |||
| 1–2 | 28 (50.0%) | 55 (41.0%) | |
| 3 | 28 (50.0%) | 79 (59.0%) | 0.257 |
| Ki67 | |||
| Negative | 24 (42.9%) | 57 (42.5%) | |
| Positive | 32 (57.1%) | 77 (57.5%) | 0.968 |
| Parameters | Univarite Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p Value | Hazard Ratio | 95% CI | p Value | |
| Androgen receptor | 0.34 | 0.13–0.87 | 0.025 | 0.36 | 0.14–0.95 | 0.039 |
| Positive vs. Negative | ||||||
| Pathological stage | 2.54 | 1.04–6.22 | 0.041 | 0.40 | 0.62–2.54 | 0.329 |
| I vs. II and III | ||||||
| Tumor size (cm) | 2.46 | 1.11–5.45 | 0.027 | 2.71 | 0.63–11.77 | 0.183 |
| ≤2 vs. >2 | ||||||
| Lymph node status | 3.39 | 1.67–6.88 | 0.001 | 3.30 | 1.32–8.25 | 0.011 |
| n0 vs. n1, n2, n3 | ||||||
| Lymphatic invasion | 1.94 | 0.99–3.75 | 0.054 | 1.23 | 0.65–2.66 | 0.565 |
| ly0 vs. ly1, ly2, ly3 | ||||||
| Histological grade | 2.36 | 1.01–5.21 | 0.034 | 1.78 | 0.79–4.01 | 0.162 |
| 1, 2 vs. 3 | ||||||
| Parameters | Androgen Receptor | p Value | |
|---|---|---|---|
| Positive (n = 10) | Negative (n = 33) | ||
| Age at operation | |||
| ≤55 | 5 (50.0%) | 20 (60.6%) | |
| >55 | 5 (50.0%) | 13 (39.4%) | 0.551 |
| Stage | |||
| 1 | 2 (20.0%) | 8 (24.2%) | |
| 2–4 | 8 (80.0%) | 25 (75.8%) | 0.575 |
| Tumor size (cm) | |||
| ≤2 | 3 (30.0%) | 9 (27.3%) | |
| >2 | 7 (70.0%) | 24 (72.3%) | 0.579 |
| Lymph node status | |||
| Negative | 5 (50.0%) | 14 (42.4%) | |
| Positive | 5 (50.0%) | 19 (57.6%) | 0.673 |
| Lymphatic invasion | |||
| Negative | 6 (60.0%) | 14 (42.4%) | |
| Positive | 4 (40.0%) | 19 (57.6%) | 0.269 |
| Vascular invasion | |||
| Negative | 10 (100.0%) | 31 (93.9%) | |
| Positive | 0 (0%) | 2 (6.1%) | 0.585 |
| Histologic type | |||
| IDC | 10 (100.0%) | 28 (84.8%) | |
| Special type | 0 (0.0%) | 5 (15.2%) | 0.247 |
| Histological grade | |||
| 1–2 | 3 (30.0%) | 8 (24.2%) | |
| 3 | 7 (70.0%) | 25 (75.8%) | 0.504 |
| Ki67 | |||
| Negative | 1 (10.0%) | 11 (33.3%) | |
| Positive | 9 (90.0%) | 22 (66.7%) | 0.149 |
| Relapse and metastases | |||
| Locoregional | 6 (60.0%) | 19 (57.6%) | |
| Distant | 4 (40.0%) | 14 (42.4%) | 0.594 |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asano, Y.; Kashiwagi, S.; Goto, W.; Tanaka, S.; Morisaki, T.; Takashima, T.; Noda, S.; Onoda, N.; Ohsawa, M.; Hirakawa, K.; et al. Expression and Clinical Significance of Androgen Receptor in Triple-Negative Breast Cancer. Cancers 2017, 9, 4. https://doi.org/10.3390/cancers9010004
Asano Y, Kashiwagi S, Goto W, Tanaka S, Morisaki T, Takashima T, Noda S, Onoda N, Ohsawa M, Hirakawa K, et al. Expression and Clinical Significance of Androgen Receptor in Triple-Negative Breast Cancer. Cancers. 2017; 9(1):4. https://doi.org/10.3390/cancers9010004
Chicago/Turabian StyleAsano, Yuka, Shinichiro Kashiwagi, Wataru Goto, Sayaka Tanaka, Tamami Morisaki, Tsutomu Takashima, Satoru Noda, Naoyoshi Onoda, Masahiko Ohsawa, Kosei Hirakawa, and et al. 2017. "Expression and Clinical Significance of Androgen Receptor in Triple-Negative Breast Cancer" Cancers 9, no. 1: 4. https://doi.org/10.3390/cancers9010004