
Paradigm Shift in Radiation Biology/Radiation Oncology—Exploitation of the “H2O2 Effect” for Radiotherapy Using Low-LET (Linear Energy Transfer) Radiation such as X-rays and High-Energy Electrons


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Beam Radiation Therapy
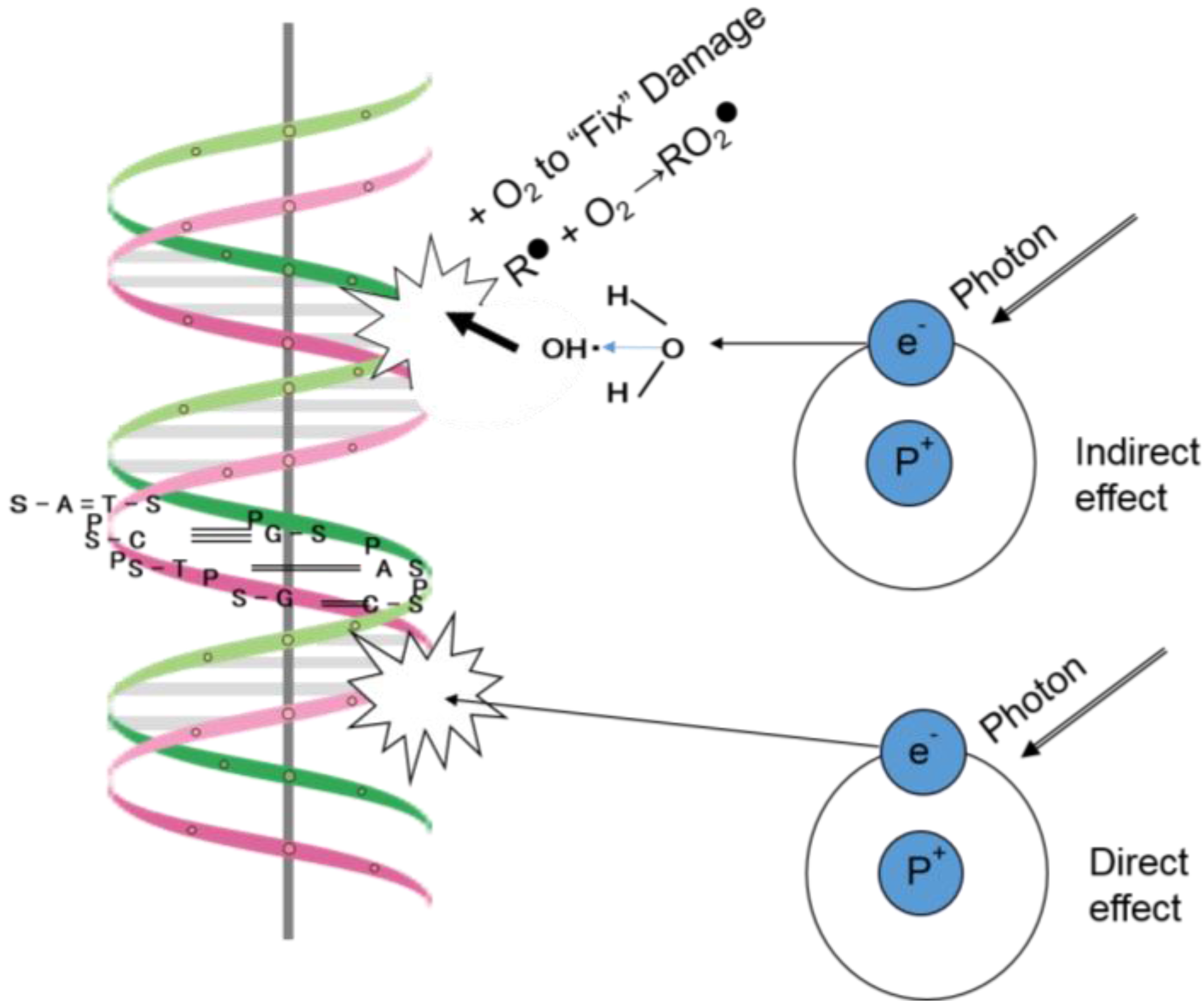
3. Interaction of Low-LET (Linear Energy Transfer) Radiation with Cancerous and Normal Tissues
4. Significance of Oxygen Molecules in the Interaction between Radiation and Cancers
5. History of the Development of Methods to Overcome Tumor Hypoxia and the Need to Reconsider Current Approaches
6. Do the Therapeutic Effects of X-rays and Electrons Produced by a Linac Involve DNA Damage?
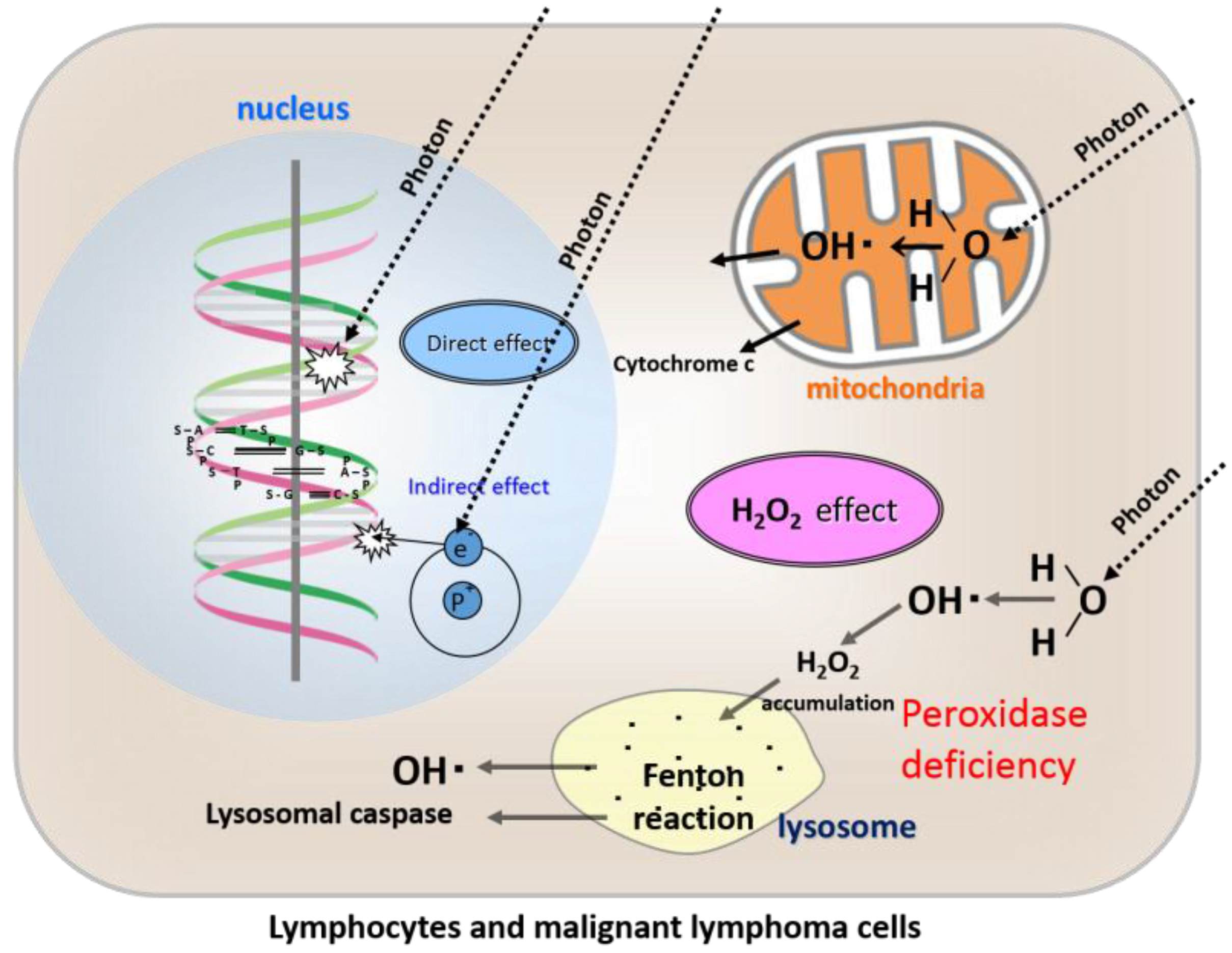
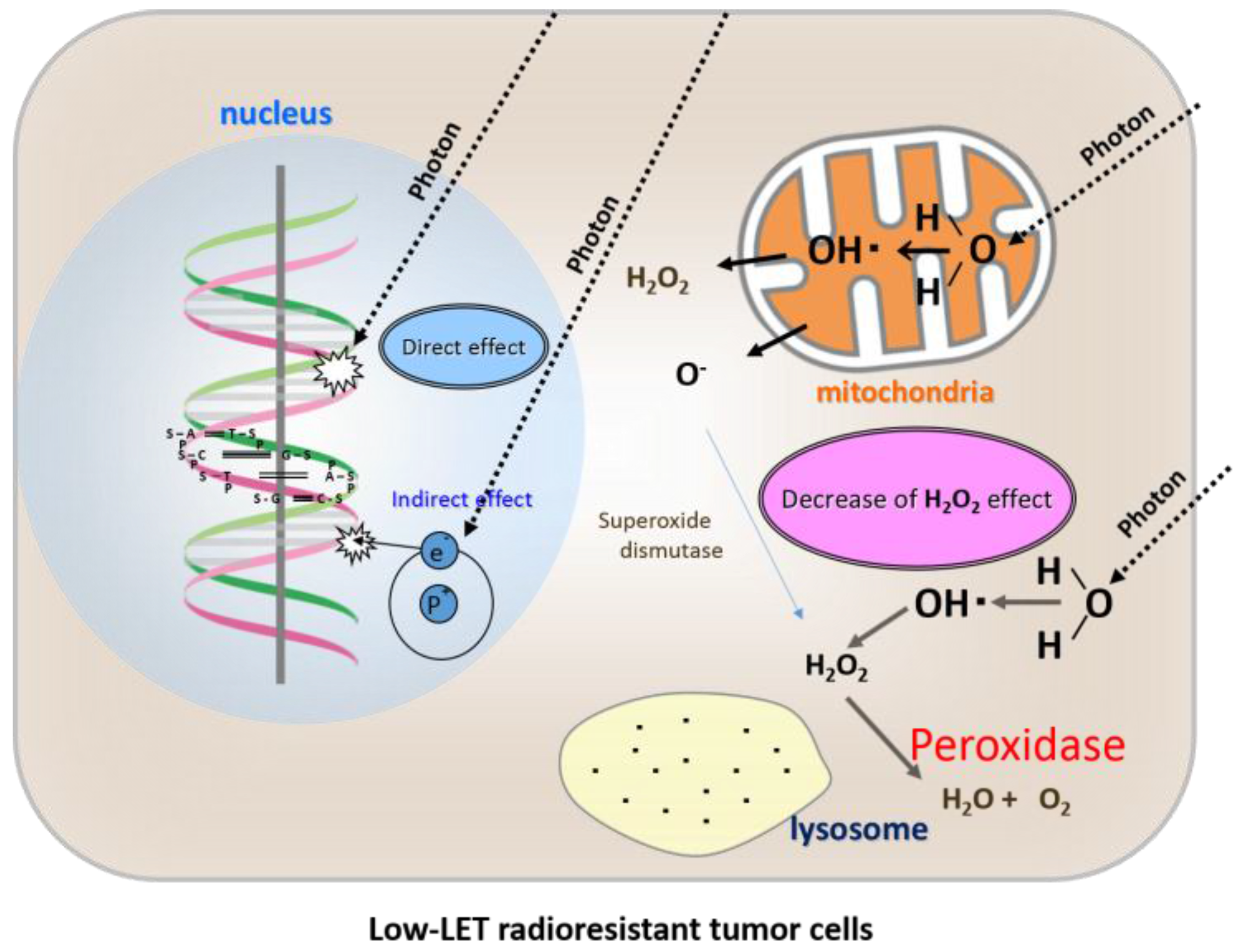
7. Anti-Oxidative Enzymes in the Therapeutic Effects of X-rays and Electrons Produced by Linac
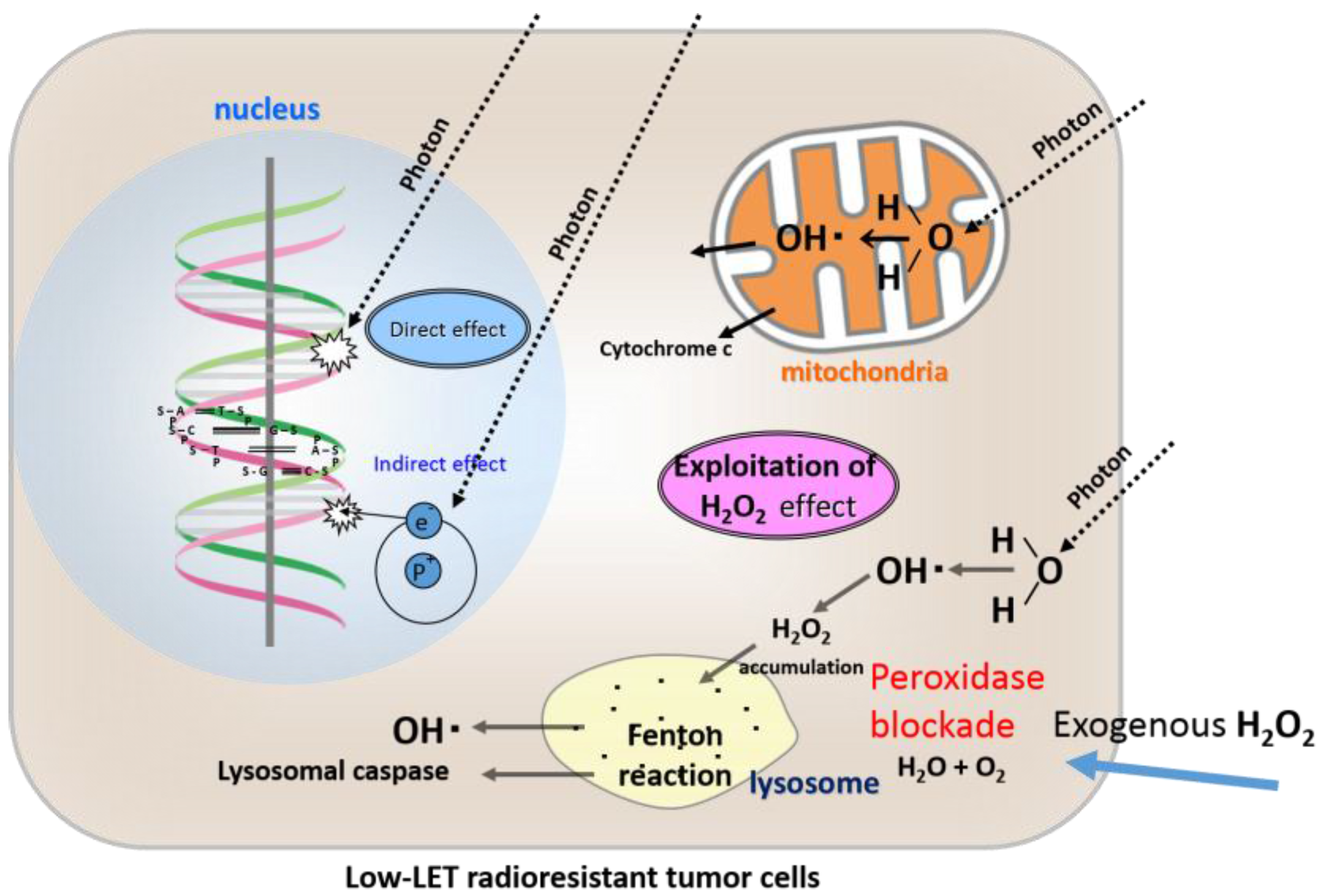
8. Possible Mechanism of Radiosensitivity Augmentation—Special Reference to “Peroxidase Blockade” as a Model of Radiosensitization
9. Mechanism of Radiation-Induced Apoptosis of Lymphocytes
10. The Low-LET Radioresistant Osteosarcoma Cell Line, HS-Os-1
11. What Is KORTUC I: Kochi Oxydol-Radiation Therapy for Unresectable Carcinomas, Type I?
12. Intra-Tumoral Injection of H2O2
13. Confirmation of the Safety of Intra-Tumoral Injection of H2O2 with Various Viscosity-Increasing Agents Using a Mouse Tumor Model
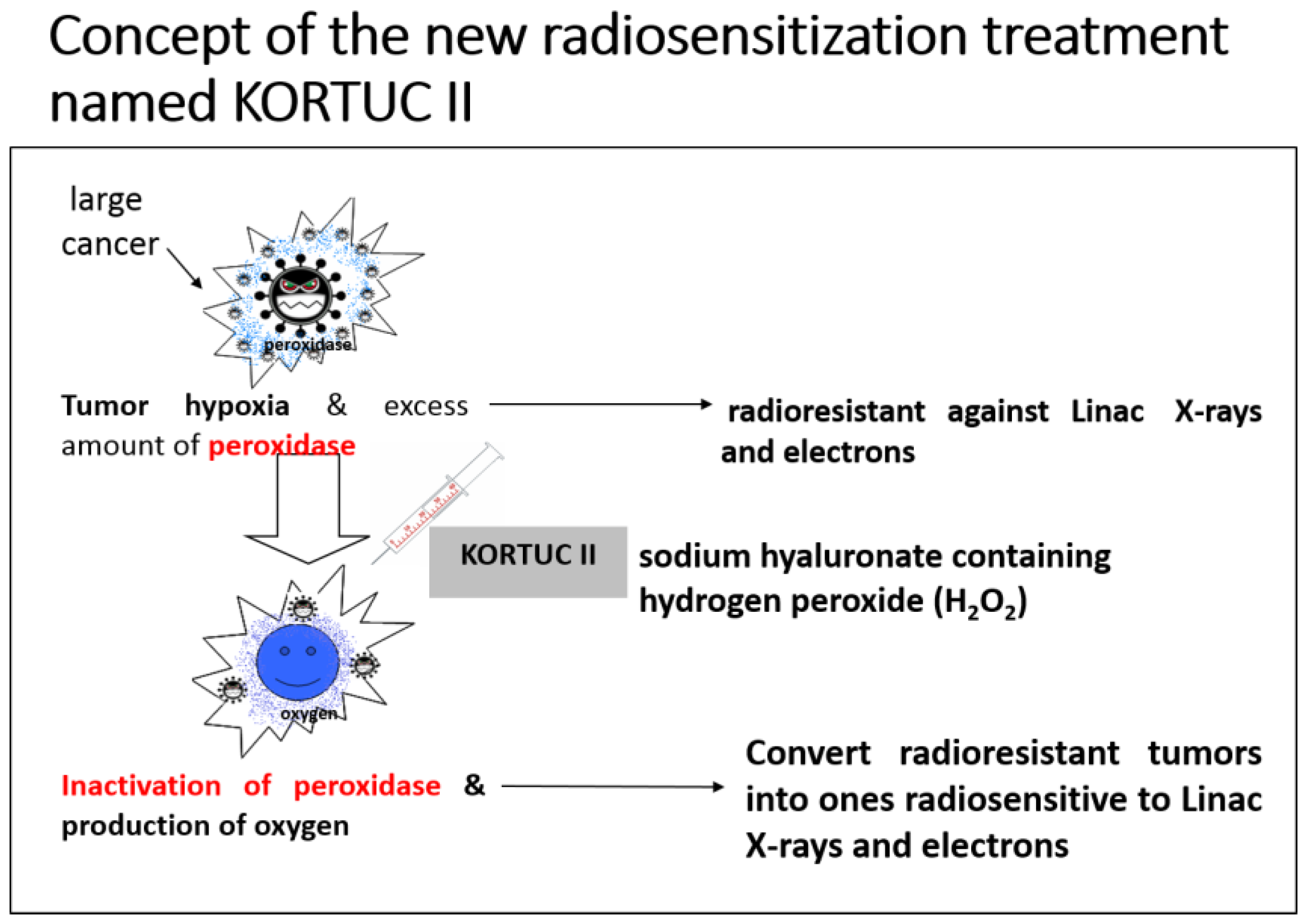
14. Development of the KORTUC II Radiosensitization Method
Formulation Example
15. Conclusions
Acknowledgments
Conflicts of Interest
References
- Hall, E.J.; Giaccia, A.J. Physics and chemistry of radiation absorption. In Radiobiology for the Radiologist, 7th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; pp. 3–11. [Google Scholar]
- Jette, D.C.; Wiebe, L.I.; Chapman, J.D. Synthesis and in vivo studies of the radiosensitizer 4-[82Br]bromomisonidazole. Int. J. Nuclear Med. 1983, 10, 205–210. [Google Scholar] [CrossRef]
- Coleman, C.N. Hypoxic cell radiosensitizers: Expectations and progress in drug development. Int. J. Radiat. Oncol. Biol. Phys. 1985, 11, 323–329. [Google Scholar] [CrossRef]
- Overgaard, J. Clinical evaluation of nitroimidazoles as modifiers of hypoxia in solid tumors. Oncol. Res. 1994, 6, 509–518. [Google Scholar] [PubMed]
- Overgaard, J. Hypoxic radiosensitization: Adored and ignored. J. Clin. Oncol. 2007, 25, 4066–4074. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Nishioka, A.; Hamada, N.; Terashima, M.; Inomata, T.; Yoshida, S.; Seguchi, H.; Kishimoto, S. Immunohistochemical study of c-fos-positive lymphocytes infiltrated into human squamous cell carcinomas of the head and neck during radiation therapy and its clinical significance. Clin. Cancer Res. 1997, 3, 2301–2307. [Google Scholar] [PubMed]
- Ogawa, Y.; Nishioka, A.; Hamada, N.; Terashima, M.; Inomata, T.; Yoshida, S.; Seguchi, H.; Kishimoto, S. Expression of Fas (CD95/APO-1) antigen induced by radiation therapy for diffuse B-cell lymphoma: Immunohistochemical study. Clin. Cancer Res. 1997, 3, 2211–2216. [Google Scholar] [PubMed]
- Izawa, S.; Kono, K.; Mimura, K.; Kawaguchi, Y.; Watanabe, M.; Maruyama, T.; Fujii, H. H2O2 production within tumor microenvironment inversely correlated with infiltration of CD56dim NK cells in gastric and esophageal cancer: Possible mechanism of NK cell dysfunction. Cancer Immunol. Immunother. 2011, 60, 1801–1810. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Outschoorn, U.E.; Lin, Z.; Trimmer, C.; Flomenberg, N.; Wang, C.; Pavlides, S.; Pestell, R.G.; Howell, A.; Sotgia, F.; Lisanti, M.P. Cancer cells metabolically “fertilize” the tumor microenvironment with hydrogen peroxide, driving the Warburg effect: Implications for PET imaging of human tumors. Cell Cycle 2011, 10, 2504–2520. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Nishioka, A.; Inomata, T.; Yoshida, S.; Nakayama, K.; Kataoka, S. Radiation kills human peripheral T cells by a Fas-independent mechanism. Int. J. Mol. Med. 1998, 2, 403–408. [Google Scholar] [PubMed]
- Ogawa, Y.; Nishioka, A.; Kobayashi, T.; Kariya, S.; Hamasato, S.; Saibara, T.; Nakayama, K.; Seguchi, H.; Yoshida, S. Mitochondrial cytochrome c release in radiation-induced apoptosis of human peripheral T cells. Int. J. Mol. Med. 2002, 10, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Nishioka, A.; Kobayashi, T.; Kariya, S.; Hamasato, S.; Saibara, T.; Seguchi, H.; Yoshida, S. Radiation-induced apoptosis of human peripheral T cells: Analyses with c DNA expression arrays and mitochondrial membrane potential assay. Int. J. Mol. Med. 2001, 7, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Kobayashi, T.; Nishioka, A.; Kariya, S.; Hamasato, S.; Seguchi, H.; Yoshida, S. Radiation-induced oxidative DNA damage, 8-oxoguanine, in human peripheral T cells. Int. J. Mol. Med. 2003, 11, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Kobayashi, T.; Nishioka, A.; Kariya, S.; Hamasato, S.; Seguchi, H.; Yoshida, S. Radiation-induced reactive oxygen species (ROS) formation prior to oxidative DNA damage in human peripheral T cells. Int. J. Mol. Med. 2003, 11, 149–152. [Google Scholar] [PubMed]
- Ogawa, Y.; Kobayashi, T.; Nishioka, A.; Kariya, S.; Ohnishi, T.; Hamasato, S.; Seguchi, H.; Yoshida, S. Reactive oxygen species-producing site in radiation-induced apoptosis of human peripheral T cells: Involvement of lysosomal membrane destabilization. Int. J. Mol. Med. 2004, 13, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Takahashi, T.; Kobayashi, T.; Kariya, S.; Nishioka, A.; Hamasato, S.; Moriki, T.; Seguchi, H.; Yoshida, S.; Sonobe, H. Immunocytochemical characteristics of human osteosarcoma cell line HS-Os-1: Possible implication in apoptotic resistance against irradiation. Int. J. Mol. Med. 2004, 14, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Takahashi, T.; Kobayashi, T.; Kariya, S.; Nishioka, A.; Ohnishi, T.; Saibara, T.; Hamasato, S.; Tani, T.; Seguchi, H.; et al. Apoptotic resistance of the human osteosarcoma cell line HS-Os-1 to irradiation is converted to apoptotic-susceptibility by hydrogen peroxide: A potent role of hydrogen peroxide as a new radiosensitizer. Int. J. Mol. Med. 2003, 12, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Takahashi, T.; Kobayashi, T.; Kariya, S.; Nishioka, A.; Mizobuchi, H.; Noguchi, M.; Hamasato, S.; Tani, T.; Seguchi, H.; et al. Mechanism of apoptotic resistance of human osteosarcoma cell line, HS-Os-1, against irradiation. Int. J. Mol. Med. 2003, 12, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Kariya, S.; Sawada, K.; Kobayashi, T.; Karashima, T.; Shuin, T.; Nishioka, A.; Ogawa, Y. Combination treatment of hydrogen peroxide and X-rays induces apoptosis in human prostate cancer PC-3 cells. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Takahashi, T.; Kobayashi, T.; Toda, M.; Nishioka, A.; Kariya, S.; Seguchi, H.; Yamamoto, H.; Yoshida, S. Comparison of radiation-induced reactive oxygen species formation in adult articular chondrocytes and that in human peripheral T cells: Possible implication in radiosensitivity. Int. J. Mol. Med. 2003, 11, 455–459. [Google Scholar] [PubMed]
- Ogawa, Y.; Ue, H.; Tsuzuki, K.; Tadokoro, M.; Miyatake, K.; Sasaki, T.; Yokota, N.; Hamada, N.; Kariya, S.; Hitomi, J.; et al. New radiosensitization treatment (KORTUC I) using hydrogen peroxide solution soaked gauze bolus for unresectable and superficially exposed neoplasms. Oncol. Rep. 2008, 19, 1389–1394. [Google Scholar] [PubMed]
- Lichtenbaum, R.; de Souza, A.A.; Jafar, J.J. Intratumoral hydrogen peroxide injection during meningioma resection. Neurosurgery 2006, 59, S470–S473. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Kubota, K.; Ue, H.; Tsuzuki, K.; Tadokoro, M.; Miyatake, K.; Sasaki, T.; Yokota, N.; Hamada, N.; Kariya, S.; et al. Development and clinical application of a new radiosensitizer containing hydrogen peroxide and hyaluronic acid sodium for topical tumor injection—A new enzyme-targeting radiosensitization treatment, KORTUC II (Kochi Oxydol-Radiation Therapy for Unresectable Carcinomas, Type II). Strahlenther. Onkol. 2007, 183, 100–101. [Google Scholar]
- Tokuhiro, S.; Ogawa, Y.; Tsuzuki, K.; Akima, R.; Ue, H.; Kariya, S.; Nishioka, A. Development of a new enzyme-targeting radiosensitizer (KORTUC) containing hydrogen peroxide for intratumoral injection for patients with low linear energy transfer (LET) radioresistant neoplasms. Oncol. Lett. 2010, 1, 1025–1028. [Google Scholar] [PubMed]
- Ogawa, Y.; Kubota, K.; Ue, H.; Kataoka, Y.; Tadokoro, M.; Miyatake, K.; Tsuzuki, K.; Yamanishi, T.; Itoh, S.; Hitomi, J.; et al. Phase I study of a new radiosensitizer containing hydrogen peroxide and sodium hyaluronate for topical tumor injection: A new enzyme-targeting radiosensitization treatment, Kochi Oxydol-Radiation Therapy for Unresectable Carcinomas, Type II (KORTUC II). Int. J. Oncol. 2009, 34, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Prada, P.J.; Fernandez, J.; Martinez, A.A.; de la Rua, A.; Gonzalez, J.M.; Fernandez, J.M.; Juan, G. Transperineal injection of hyaluronic acid in anterior perirectal fat to decrease rectal toxicity from radiation delivered with intensity-modulated brachytherapy or EBRT for prostate cancer patients. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Kubota, K.; Ue, H.; Tadokoro, M.; Matsui, R.; Yamanishi, T.; Hamada, N.; Kariya, S.; Nishioka, A.; Nakajima, H.; et al. Safety and effectiveness of a new enzyme-targeting radiosensitization treatment (KORTUC II) for intratumoral injection for low-LET radioresistant tumors. Int. J. Oncol. 2011, 39, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Chasin, W.D.; Gross, C.C.; Wang, C.C. Hydrogen peroxide and irradiation of tumors. Arch. Otolaryngol. 1967, 85, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Tsuzuki, A.; Ogawa, Y.; Kubota, K.; Tokuhiro, S.; Akima, R.; Yaogawa, S.; Itoh, K.; Yamada, Y.; Sasaki, T.; Onogawa, M.; et al. Evaluation of changes in tumor shadows and microcalcifications on mammography following KORTUC II, a new radiosensitization treatment without any surgical procedure for elderly patients with stage I and II breast cancer. Cancers 2011, 3, 3496–3505. [Google Scholar] [CrossRef] [PubMed]
- Hitomi, J.; Kubota, K.; Ogawa, Y.; Hamada, N.; Murata, Y.; Nishioka, A. Non-surgical therapy and radiologic assessment of stage I breast cancer treatment with novel enzyme-targeting radiosensitization: Kochi Oxydol-Radiation Therapy for unresectable carcinomas. Exp. Ther. Med. 2010, 1, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Kubota, K.; Aoyama, N.; Yamanishi, T.; Kariya, S.; Hamada, N.; Nogami, M.; Nishioka, A.; Onogawa, M.; Miyamura, M. Non-surgical breast-conserving treatment (KORTUC-BCT) using a new radiosensitization method (KORTUC II) for patients with stage I or II breast cancer. Cancers 2015, 7, 2277–2289. [Google Scholar] [CrossRef] [PubMed]
- Yaogawa, S.; Ogawa, Y.; Morita-Tokuhiro, S.; Tsuzuki, A.; Akima, R.; Itoh, K.; Morio, K.; Yasunami, H.; Onogawa, M.; Kariya, S.; et al. Serial assessment of therapeutic response to a new radiosensitization treatment, Kochi Oxydol-Radiation Therapy for Unresectable Carcinomas, Type II (KORTUC II), in patients with stage I/II breast cancer using breast contrast-enhanced magnetic resonance imaging. Cancers 2016, 8, 1. [Google Scholar]
- Miyatake, K.; Kubota, K.; Ogawa, Y.; Hamada, N.; Murata, Y.; Nishioka, A. Non-surgical care for locally advanced breast cancer: Radiologically assessed therapeutic outcome of a new enzyme-targeting radiosensitization treatment, Kochi Oxydol-Radiation Therapy for Unresectable Carcinomas, Type II (KORTUC II) with systemic chemotherapy. Oncol. Rep. 2010, 24, 1161–1168. [Google Scholar] [PubMed]
- Nishioka, A.; Ogawa, Y.; Mityatake, K.; Tadokoro, M.; Nogami, M.; Hamada, N.; Kubota, K.; Kariya, S.; Kohsaki, T.; Saibara, T.; et al. Safety and efficacy of image-guided enzyme-targeting radiosensitization and intraoperative radiotherapy for locally advanced unresectable pancreatic cancer. Oncol Lett. 2014, 8, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Morita-Tokuhiro, S.; Ogawa, Y.; Yokota, N.; Tsuzuki, A.; Oda, H.; Ishida, N.; Aoyama, N.; Nishioka, A. Development of a novel enzyme-targeting radiosensitizer (New KORTUC) using a gelatin-based hydrogel instead of a sodium hyaluronate. Cancers 2016, 8, 10. [Google Scholar] [CrossRef] [PubMed]





© 2016 by the author; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogawa, Y. Paradigm Shift in Radiation Biology/Radiation Oncology—Exploitation of the “H2O2 Effect” for Radiotherapy Using Low-LET (Linear Energy Transfer) Radiation such as X-rays and High-Energy Electrons. Cancers 2016, 8, 28. https://doi.org/10.3390/cancers8030028
Ogawa Y. Paradigm Shift in Radiation Biology/Radiation Oncology—Exploitation of the “H2O2 Effect” for Radiotherapy Using Low-LET (Linear Energy Transfer) Radiation such as X-rays and High-Energy Electrons. Cancers. 2016; 8(3):28. https://doi.org/10.3390/cancers8030028
Chicago/Turabian StyleOgawa, Yasuhiro. 2016. "Paradigm Shift in Radiation Biology/Radiation Oncology—Exploitation of the “H2O2 Effect” for Radiotherapy Using Low-LET (Linear Energy Transfer) Radiation such as X-rays and High-Energy Electrons" Cancers 8, no. 3: 28. https://doi.org/10.3390/cancers8030028