1. Introduction
Immune checkpoint blockade is a rapidly expanding modality of cancer treatment and continues to gain approval for more cancer indications. This class of immunotherapy encompasses drugs with mechanisms that include antagonizing programmed death-ligand 1 (PD-L1), programmed cell death protein 1 (PD-1), cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), and, most recently, lymphocyte-activation gene 3 (LAG-3) [
1,
2]. The blockade of these checkpoints on cancer cells induces the immune system recognition of the cells as foreign and prompts anticancer activity, thus leading to the eventual death of malignant cells. However, this mechanism also poses a risk to healthy cells, as breaks in immune tolerance lead to autoimmune and autoinflammatory side effects, which are known as immune-related adverse events (irAEs), which can occur in most organ systems [
3].
Checkpoint inhibitor diabetes mellitus (CPI-DM) is a severe and highly morbid irAE caused by the collateral damage from autoimmune activation targeting pancreatic beta cells. It occurs in 0.2–1.9% of patients using CPIs, is predominantly in those exposed to PD-1 and PD-L1 inhibitors, and it is not seen in CTLA-4 inhibitor monotherapy [
4]. Phase 2 and 3 clinical trials for the only LAG-3 inhibitor available in the US did not list CPI-DM as an irAE that occurred in ≥1% of study participants [
5]. The autoantibodies usually present in type 1 diabetes (T1DM) such as GAD65, IA-2 (also known as ICA-512), insulin auto-antibodies, and ZnT8 are positive in some cases but not all [
6]. While the mechanism is unknown currently, this suggests that it differs from traditional T1DM. For example, in studies where GAD65 is measured, less than half of patients with CPI-DM show GAD65 positivity [
4,
7,
8].
In nearly all cases of CPI-DM, presentation involves a precipitous and significant increase in blood glucose levels, with low or undetectable C-peptide levels present in 73–91% of cases, and positive autoantibodies associated with type 1 diabetes such as GAD65 seen in 48–52% of patients [
9,
10]. In 59–71% of cases, depending on the study, patients will develop potentially life-threatening diabetic ketoacidosis (DKA), which requires hospitalization to initiate insulin therapy and replete fluids [
8,
11,
12]. Diagnosis is often made with standard lab values such as blood glucose, urine, or serum ketones, and blood pH and treatment is similar to T1DM with short and long-acting insulin. Auto-antigen, auto-antibody, insulin, and C-peptide levels are not routinely measured as they are not necessary to treat the patient, although they can sometimes help to confirm the diagnosis. The discontinuation of CPI therapy almost never reverses CPI-DM, and treatment requires lifelong insulin therapy [
3,
4,
8,
13]. Due to the dramatic consequences and often severe presentation of this irAE, patients and physicians may be fearful of resuming CPI treatment due to the risk of additional irAEs, while others may continue treatment due to the irreversible and medically manageable nature of CPI-DM. These decisions have the potential to impact the patient’s cancer outcomes and possibly put the patient at risk for future morbidities.
Several studies have described the clinical syndrome of CPI-DM and theorized its pathophysiologic mechanism related to checkpoint blockade but none, to our knowledge, have explored the implication of the clinical decision of either resuming or discontinuing CPI treatment following the diagnosis of CPI-DM. Thus, there has been no guidance to help decide whether to discontinue or resume CPI therapy. To date, this decision is often made by assessing a variety of factors, including the cancer’s response to treatment and patient preference. To provide guidance when faced with similar situations, this study evaluated the incidence of additional irAEs and cancer outcomes in patients who have either resumed or discontinued CPI therapy after developing CPI-DM.
2. Materials and Methods
This is a single-institution retrospective cohort study including patients who developed CPI-DM between 1 July 2015 to 5 July 2023 while being treated with a PD-1 or PD-L1 inhibitor alone or in combination with other cancer therapies. CPI-DM is defined as a loss of insulin production, as defined by low C-peptide and presentation in DKA [
8,
14,
15]. All of the patients in the study required prolonged basal–bolus insulin administration. The positive autoantibodies typically present in T1DM were not required to be included in the study. This study was approved by the UCSF Institutional Review Board.
Study endpoints included the development of new irAEs and cancer outcomes after CPI-DM diagnosis in those who discontinued CPIs compared to those who resumed. Patients were categorized into three groups: those who resumed CPIs within 90 days after DM diagnosis (prompt restart), those who resumed CPIs after 90 days (delayed restart), and those who permanently discontinued CPI therapy (
Figure 1). New irAEs were defined as symptoms or syndromes that were either biopsy-proven or clinically determined to be due to CPI therapy by the treating physician(s) after ruling out other attributing causes. Progression was determined in accordance with Response Evaluation Criteria in Solid Tumors (RECIST) guidelines [
16]. Patient data were collected until either death, loss to institution-specific follow-up, or 9 October 2023, whichever came first.
Baseline demographic data, including age, sex, type of cancer, prior lines of cancer therapy, prior irAEs, and personal or family history of DM, as well as other autoimmune conditions, were collected (
Table 1). The date of CPI-DM diagnosis was recorded along with presenting symptoms, presence of diabetic ketoacidosis, and insulin requirement. After CPI-DM diagnosis, new irAEs were documented for all patients, including the respective irAE treatments required. Outcome data were collected for all patients, including response at CPI-DM diagnosis, progression, and death.
Additional analysis was performed comparing the incidence rate of new irAEs based on the time the patient was on and off CPI treatment (
Figure 2). On-treatment time was defined as the time from CPI-DM diagnosis to the date of the patients last CPI cycle in those who resumed CPI. Off-treatment time began on the date of the CPI-DM diagnosis, and it was calculated with three different end dates to examine the effect of delayed irAEs. The first approach used the time from CPI-DM diagnosis to either the date of death or last point of contact. The second approach limited the time off treatment post-CPI exposure to one year (365 days) maximum, and the third approach limited the time off treatment post-CPI exposure to six months (180 days) maximum. In patients who had a prolonged delay between CPI-DM diagnosis and resumption of CPI therapy, the delayed time to resumption was considered time off-treatment.
Baseline characteristics, new irAEs, and cancer outcomes were summarized using descriptive statistics, such as medians, ranges, counts, and percentages, and they were compared by CPI use after CPI-DM diagnosis using binomial tests, t-tests, and Fisher’s exact tests, as appropriate. The time-to-event data were summarized with Cox regression and log-rank tests, and they were visualized with Kaplan–Meier methods. Analyses were performed using the R statistical program version 4.3.1.
3. Results
Forty-three patients that developed CPI-DM during the study period were identified. Among those who died, the median follow-up time was 535 (51–2525) days, while all other patients were followed with at 1368 (96–2784) days.
3.1. Baseline Demographics
Of the 43 patients with CPI-DM, 19 (44%) discontinued CPIs after diagnosis, 20 (47%) had a prompt restart within 90 days, and 4 (9%) had a delayed CPI restart (
Figure 1). Delays in restarting CPIs were either due to patient preference (
n = 1) or disease progression (
n = 3). Patients were treated for a variety of cancers, with melanoma being the most common (
n = 11, 26%), followed by non-small cell lung cancer and breast cancer (both with
n = 4, 9%). The most common CPIs used prior to CPI-DM onset were pembrolizumab (
n = 23, 53%) and nivolumab (
n = 14, 33%). A total of 40 patients (93%) received PD-1 or PD-L1 blockades, while the remaining 3 (7%) received a combination of PD-1 and CTLA-4 inhibitor. Furthermore, 9 (21%) patients had a history of pre-diabetes and 3 (7%) had controlled type 2 diabetes mellitus (T2DM). Patients with a history of pre-CPI prediabetes or diabetes were more likely to resume CPIs after CPI-DM diagnosis. In addition, 4 (9%) patients had a family history of type 1 diabetes mellitus (T1DM). Prior thyroid disease was present in 21 (49%) of patients. Moreover, 5 patients (12%) had autoimmune thyroid diseases diagnosed and 16 (37%) had already developed CPI-induced thyroid dysfunction. Dermatitis (
n = 10, 23%), arthritis (
n = 6, 14%), and colitis (
n = 5, 12%) were among the most common non-endocrine irAEs that occurred prior to CPI-DM onset. Overall, only 28 (65%) of the patients had any irAEs before CPI-DM was diagnosed (
Table 1). The time from the beginning to the last CPI therapy to diagnosis CPI-DM was not significantly associated with the decision to resume or discontinue CPI therapy (
p = 0.078) (
Figure 3A). Furthermore, 20 out of 24 patients (83%) resumed CPI therapy within the first three months after CPI-DM diagnosis (
Figure 3B).
3.2. New irAEs Diagnosed after CPI-DM
Of the 43 patients with CPI-DM, 12 (28%) developed new irAEs after being diagnosed with CPI-DM, regardless of whether CPIs were resumed or not (
Figure 1). Moreover, 7 (35%) patients who promptly resumed, 2 (50%) of those who delayed resuming (both of which occurred after resuming CPIs), and 3 (16%) of those who permanently stopped CPI had subsequent irAEs after being diagnosed with CPI-DM. Resuming CPI therapy was not associated with the development of new irAEs (38% resuming CPI and 16% permanently stopping CPI,
p = 0.17). Factors that may be signs of increased autoimmunity such as prior irAEs and a family history of autoimmune disease did not predict new irAE development (
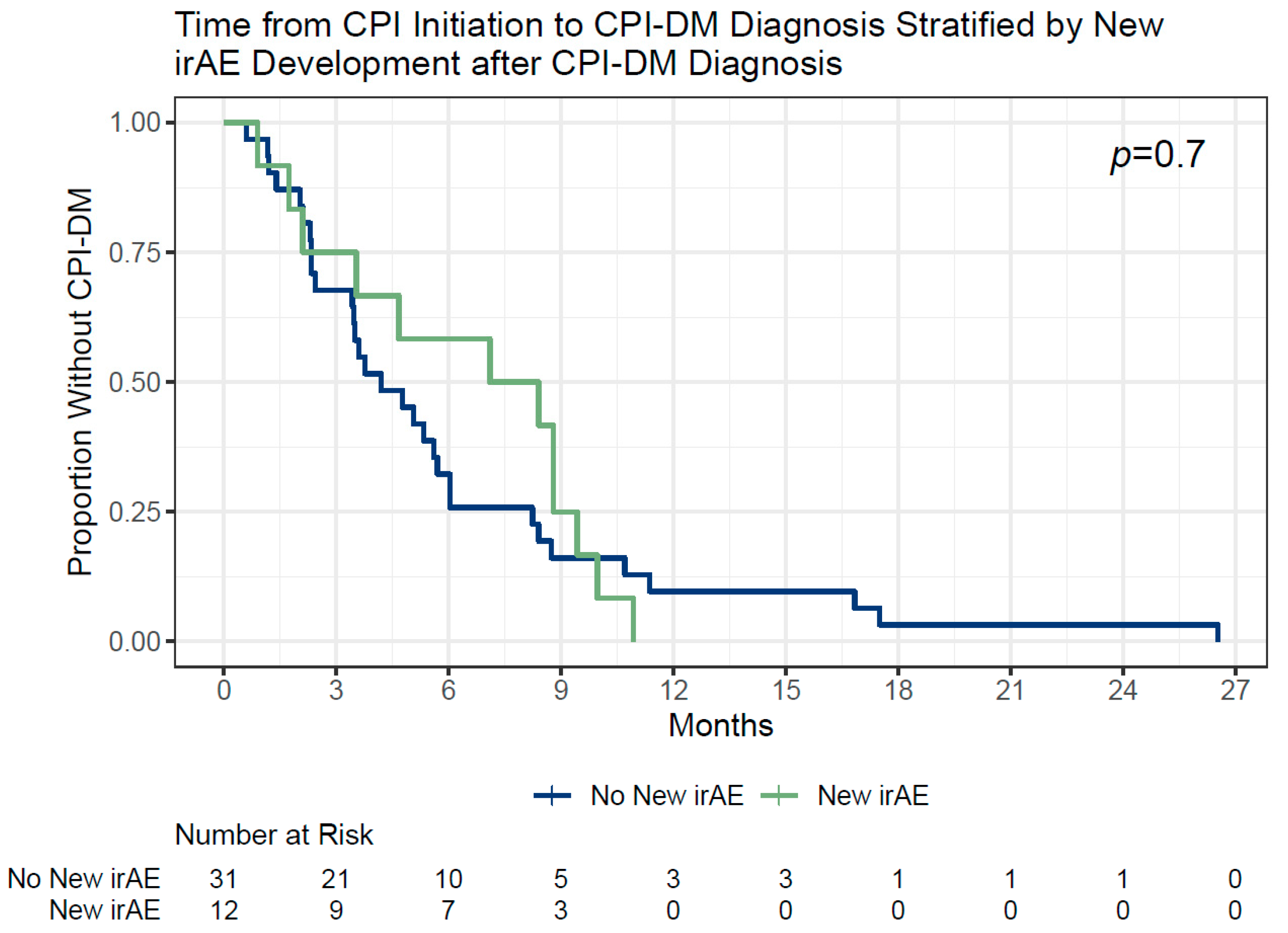
Table 2). The development of new irAEs was not influenced by the time from CPI initiation to CPI-DM diagnosis (
Figure 4). Among the patients who developed CPI-DM within 3, 3–6, 6–12, and over 12 months from starting CPI therapy, 3/13 (23%), 2/13 (15%), 7/14 (50%), and 0/3 (0%) developed a subsequent irAE, respectively (
p = 0.17). This association with time to CPI-DM diagnosis remained non-significant regardless of whether the first exposure to CPI was used as the starting point or the start date of the CPI that the patient was on when CPI-DM diagnosis was considered (Kaplan–Meier, log rank
p = 0.8 and 0.7, respectively).
3.3. Cancer Outcomes
When considering cancer outcomes, patients who had a delayed resumption of CPIs (>90 days after CPI-DM diagnosis) were grouped with those who discontinued CPIs as this was in line with the treating physician’s intent at CPI-DM diagnosis. The patient cancer response at CPI-DM diagnosis did not significantly impact whether the patients resumed CPI or stopped/delayed resuming them (p = 0.16). However, there was a tendency for more patients with PR or SD to promptly resume CPI therapy (16/20, 75%) compared to stopping or delaying CPI resumption (11/23, 48%) (p = 0.06).
Furthermore, 6 (32%) patients who stopped/delayed resuming CPIs and 7 (29%) patients who promptly resumed CPIs died during the study period (p = 0.74). Among the patients who died from non-cancer related causes, 3 (16%) had stopped/delayed CPIs and 1 (4%) had promptly resumed CPIs. The alternate causes of death included hip fracture, gastrointestinal stromal tumor progression (which was different from the initial malignancy requiring CPI use), aspiration pneumonia, and a surgical complication. When limiting the analysis to cancer-attributable deaths, 3 (7.7%) and 6 (15%) of the patients who stopped and resumed CPIs died from their original cancer (p = 0.71). Moreover, 8 (35%) patients who stopped/delayed CPIs and 9 (45%) patients who resumed them had a progression of their disease (p = 0.55). All of the patients who had a prolonged pause (>90 days) in restarting CPI therapy had either no evidence of disease, stable disease, or, in one subject, a partial response at CPI-DM diagnosis that converted to a complete response in the coming months.
The median time to death was 1139 days and 805 days in patients who stopped and resumed CPIs (
p = 0.36), while the median time to progression was 566 and 492 days in both groups (
p = 0.47), respectively (
Table 3).
4. Discussion
In our review of 43 patients with CPI-DM, there was no difference in the incidence of new irAEs or an effect on mortality and progression between those that stopped and resumed CPIs.
Patients with CPI-DM remained at risk for subsequent irAEs both on and off CPI therapy. In our study, 38% of patients who resumed therapy and 16% who discontinued CPI developed new irAEs. Risk of irAEs after resuming CPI therapy in the context of CPI-DM may be slightly lower than resuming CPIs after other irAEs. In similar studies, 52–55% of patients develop new or recurrent irAEs when CPIs are rechallenged after any irAE and higher severity irAEs (like CPI-DM), which carry a non-significant but higher risk of additional irAEs upon CPI resumption compared to lower severity irAEs [
17,
18]. Importantly, unlike irAEs such as colitis, inflammatory arthritis, or dermatitis, CPI-DM is nearly always a permanent irAE that cannot recur or worsen during the CPI treatment course. Since CPI-DM typically has a longer range of time to presentation compared to other irAEs, the lower incidence of new irAEs in our study may be explained by the fact that many patients will have already experienced other irAEs that they are most susceptible to prior to the onset of CPI-DM [
19,
20]. This is reflected in our study with 65% of patients having experienced another irAE prior to developing CPI-DM. In summary, resuming CPIs does not seem to put patients at additional risk compared to having developed other irAEs, but further study is needed to determine if this risk is higher than patients who have continued on therapy without a history of severe irAE.
An important finding in this study is the confirmation that patients remain at risk for irAEs after discontinuation of CPIs, which is consistent with a prolonged alteration in immune tolerance. The occurrence of delayed irAEs is mechanistically supported by Phase I pharmacodynamic studies showing PD-1 receptor occupancy remains at a plateau of 72% for ≥ 57 days, despite the serum half-life of the drug being 12–20 days [
21]. A more recent study on the receptor occupancy (RO) of PD-1 drugs showed a two-fold reduction in antibody binding capacity in patients exposed to CPIs within the last 14 weeks, presumably due to interfering RO from prior anti-PD1 drugs [
22]. Furthermore, a study on delayed irAEs after CPI discontinuation showed a median time to delayed irAE of 6 months in a cohort of 23 patients [
23]. Our sensitivity analysis showed that the rate of irAEs does decrease with the passage of time after CPI discontinuation and that patients are statistically less likely to obtain new irAEs somewhere between 6–12 months after their last CPI exposure. This highlights the persistent effect of CPIs on immune tolerance and supports the need to remain vigilant for irAEs post-CPI cessation for at least 6 months (but possibly longer).
This study did not reveal a significant effect on cancer progression and cancer-related mortality when discontinuing CPIs. The trend toward significantly more patients with PR or SD promptly resuming CPI therapy (p = 0.06) suggests that cancer providers may have been more likely to continue treatment if patients seemed to have tenuous control over their cancer. This is clinically reasonable and reflects the complexity of treatment decisions made during cancer care that includes a careful analysis of risks, benefits, the current state of the patient’s cancer control, and their functional status.
A limitation in this study is the small sample size, which has possibly prevented the detection of significant differences in the outcomes and incidence of irAEs. Additionally, there are likely confounding factors surrounding the cancer outcomes that have not been captured in this study, including cancer grade, cytogenetics, stage at diagnosis, and patient performance status, among others. Furthermore, the heterogeneity of cancer types in our relatively small patient population may mask the inherent differences in the expected response to immunotherapy and expected rates of progression and death. Thus, cancer characteristics could be more meaningful, and the differences in cancer outcomes could be more interpretable when examining large cohorts with more patients with a single tumor type. Therefore, future research should focus on recruiting a larger cohort of patients or combining data across institutions to increase study power. Additionally, other endpoints should be explored, such as quality-adjusted life year analyses to better understand patient perspectives in addition to clinical endpoints. The authors of this study hope to update this article when more patients are received with CPI-DM at the institution where this study was conducted.
Immunotherapy has been an important recent discovery that has provided a major tool toward fighting cancer. It offers life-saving treatment for patients who would otherwise have no options. However, it is crucial to continue expanding our understanding of the irAEs associated with this therapy so we may better serve our patients in mitigating them and making treatment more tolerable [
24,
25]. As such, both future clinical, basic science, and translational research should work toward understanding irAE mechanisms and providing treatment or prevention strategies [
26,
27].
5. Conclusions
In conclusion, this study demonstrated no significant difference in the risk of additional irAEs and progression or death for patients who decide to stop or continue CPI therapy after CPI-DM. However, this remains a challenging clinical decision and further research is needed to provide clearer guidance to clinicians when making individualized decisions for their patients. Nevertheless, these data may provide clinicians and patients with an additional piece of information when considering the difficult decision of whether to resume CPI therapy. Most importantly, providers should counsel that discontinuing CPIs may not prevent all additional irAEs, especially in the immediate three-month period after the last dose.
Author Contributions
All authors contributed to study design. E.D. and Z.Q. completed the data abstraction and analyses. The interpretation of the results was performed by all authors. E.D. wrote the manuscript with support from Z.Q. Substantial review of the manuscript was conducted by S.B., M.S.A. and R.J.R. All authors have read and agreed to the published version of the manuscript.
Funding
Z.Q. was supported NIDDK DiabDocs K12DK133995, the Larry L Hillblom Foundation Start Up Grant, and by an American Diabetes Association Grant (1–19-PDF-131).
Institutional Review Board Statement
This study was approved by the UCSF Institutional Review Board; approval number 10-02467. All patient data were obtained with the consent of the patients.
Informed Consent Statement
Patient consent was waived due to only requiring chart review to complete the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding authors.
Conflicts of Interest
S.B., R.J.R. and E.D. declare no conflicts of interest. Z.Q. has worked as a consultant for Sanofi and Novartis. M.A. has worked as a consultant for Sanofi and Imcyse and has stock in Merck.
References
- Abdou, Y.; Pandey, M.; Sarma, M.; Shah, S.; Baron, J.; Ernstoff, M.S. Mechanism-based treatment of cancer with immune checkpoint inhibitor therapies. Br. J. Clin. Pharmacol. 2020, 86, 1690–1702. [Google Scholar] [CrossRef] [PubMed]
- Andrews, L.P.; Cillo, A.R.; Karapetyan, L.; Kirkwood, J.M.; Workman, C.J.; Vignali, D.A.A. Molecular Pathways and Mechanisms of LAG3 in Cancer Therapy. Clin. Cancer Res. 2022, 28, 5030–5039. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Abu-Sbeih, H.; Ascierto, P.A.; Brufsky, J.; Cappelli, L.C.; Cortazar, F.B.; Gerber, D.E.; Hamad, L.; Hansen, E.; Johnson, D.B.; et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immune checkpoint inhibitor-related adverse events. J. Immunother. Cancer 2021, 9, e002435. [Google Scholar] [CrossRef] [PubMed]
- Quandt, Z.; Young, A.; Perdigoto, A.L.; Herold, K.C.; Anderson, M.S. Autoimmune Endocrinopathies: An Emerging Complication of Immune Checkpoint Inhibitors. Annu. Rev. Med. 2021, 72, 313–330. [Google Scholar] [CrossRef] [PubMed]
- Tawbi, H.A.; Schadendorf, D.; Lipson, E.J.; Ascierto, P.A.; Matamala, L.; Castillo Gutiérrez, E.; Rutkowski, P.; Gogas, H.J.; Lao, C.D.; De Menezes, J.J.; et al. Relatlimab and Nivolumab versus Nivolumab in Untreated Advanced Melanoma. N. Engl. J. Med. 2022, 386, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Casals, M.; Brahmer, J.R.; Callahan, M.K.; Flores-Chávez, A.; Keegan, N.; Khamashta, M.A.; Lambotte, O.; Mariette, X.; Prat, A.; Suárez-Almazor, M.E. Immune-related adverse events of checkpoint inhibitors. Nat. Rev. Dis. Primers 2020, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Byun, D.J.; Braunstein, R.; Flynn, J.; Zheng, J.; Lefkowitz, R.A.; Kanbour, S.; Girotra, M. Immune Checkpoint Inhibitor–Associated Diabetes: A Single-Institution Experience. Diabetes Care 2020, 43, 3106–3109. [Google Scholar] [CrossRef] [PubMed]
- Stamatouli, A.M.; Quandt, Z.; Perdigoto, A.L.; Clark, P.L.; Kluger, H.; Weiss, S.A.; Gettinger, S.; Sznol, M.; Young, A.; Rushakoff, R.; et al. Collateral Damage: Insulin-Dependent Diabetes Induced With Checkpoint Inhibitors. Diabetes 2018, 67, 1471–1480. [Google Scholar] [CrossRef] [PubMed]
- Perdigoto, A.L.; Quandt, Z.; Anderson, M.; Herold, K.C. Checkpoint inhibitor-induced insulin-dependent diabetes: An emerging syndrome. Lancet Diabetes Endocrinol. 2019, 7, 421–423. [Google Scholar] [CrossRef]
- Tan, M.H.; Iyengar, R.; Mizokami-Stout, K.; Yentz, S.; MacEachern, M.P.; Shen, L.Y.; Redman, B.; Gianchandani, R. Spectrum of immune checkpoint inhibitors-induced endocrinopathies in cancer patients: A scoping review of case reports. Clin. Diabetes Endocrinol. 2019, 5, 1. [Google Scholar] [CrossRef]
- Wu, L.; Tsang, V.H.M.; Sasson, S.C.; Menzies, A.M.; Carlino, M.S.; Brown, D.A.; Clifton-Bligh, R.; Gunton, J.E. Unravelling Checkpoint Inhibitor Associated Autoimmune Diabetes: From Bench to Bedside. Front. Endocrinol. 2021, 12, 764138. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.-S.; Barroso-Sousa, R.; Tolaney, S.M.; Hodi, F.S.; Kaiser, U.B.; Min, L. Endocrine Toxicity of Cancer Immunotherapy Targeting Immune Checkpoints. Endocr. Rev. 2018, 40, 17–65. [Google Scholar] [CrossRef] [PubMed]
- Kotwal, A.; Cheung, Y.-M.M.; Cromwell, G.; Drincic, A.; Leblebjian, H.; Quandt, Z.; Rushakoff, R.J.; McDonnell, M.E. Patient-Centered Diabetes Care of Cancer Patients. Curr. Diab Rep. 2021, 21, 62. [Google Scholar] [CrossRef] [PubMed]
- Tsang, V.H.M.; McGrath, R.T.; Clifton-Bligh, R.J.; Scolyer, R.A.; Jakrot, V.; Guminski, A.D.; Long, G.V.; Menzies, A.M. Checkpoint Inhibitor-Associated Autoimmune Diabetes Is Distinct From Type 1 Diabetes. J. Clin. Endocrinol. Metab. 2019, 104, 5499–5506. [Google Scholar] [CrossRef] [PubMed]
- Marsiglio, J.; McPherson, J.P.; Kovacsovics-Bankowski, M.; Jeter, J.; Vaklavas, C.; Swami, U.; Grossmann, D.; Erickson-Wayman, A.; Soares, H.P.; Kerrigan, K.; et al. A single center case series of immune checkpoint inhibitor-induced type 1 diabetes mellitus, patterns of disease onset and long-term clinical outcome. Front. Immunol. 2023, 14, 1229823. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Santini, F.C.; Rizvi, H.; Plodkowski, A.J.; Ni, A.; Lacouture, M.E.; Gambarin-Gelwan, M.; Wilkins, O.; Panora, E.; Halpenny, D.F.; Long, N.M.; et al. Safety and Efficacy of Re-treating with Immunotherapy after Immune-Related Adverse Events in Patients with NSCLC. Cancer Immunol. Res. 2018, 6, 1093–1099. [Google Scholar] [CrossRef]
- Simonaggio, A.; Michot, J.M.; Voisin, A.L.; Le Pavec, J.; Collins, M.; Lallart, A.; Cengizalp, G.; Vozy, A.; Laparra, A.; Varga, A.; et al. Evaluation of Readministration of Immune Checkpoint Inhibitors after Immune-Related Adverse Events in Patients with Cancer. JAMA Oncol. 2019, 5, 1310–1317. [Google Scholar] [CrossRef]
- Chan, K.K.; Bass, A.R. Autoimmune complications of immunotherapy: Pathophysiology and management. BMJ 2020, 369, m736. [Google Scholar] [CrossRef]
- Davies, M.; Duffield, E.A. Safety of checkpoint inhibitors for cancer treatment: Strategies for patient monitoring and management of immune-mediated adverse events. ImmunoTargets Ther. 2017, 6, 51–71. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Drake, C.G.; Wollner, I.; Powderly, J.D.; Picus, J.; Sharfman, W.H.; Stankevich, E.; Pons, A.; Salay, T.M.; McMiller, T.L.; et al. Phase I Study of Single-Agent Anti–Programmed Death-1 (MDX-1106) in Refractory Solid Tumors: Safety, Clinical Activity, Pharmacodynamics, and Immunologic Correlates. J. Clin. Oncol. 2010, 28, 3167–3175. [Google Scholar] [CrossRef] [PubMed]
- Junker, F.; Gulati, P.; Wessels, U.; Seeber, S.; Stubenrauch, K.-G.; Codarri-Deak, L.; Markert, C.; Klein, C.; Camillo Teixeira, P.; Kao, H. A human receptor occupancy assay to measure anti-PD-1 binding in patients with prior anti-PD-1. Cytom. Part A 2021, 99, 832–843. [Google Scholar] [CrossRef] [PubMed]
- Couey, M.A.; Bell, R.B.; Patel, A.A.; Romba, M.C.; Crittenden, M.R.; Curti, B.D.; Urba, W.J.; Leidner, R.S. Delayed immune-related events (DIRE) after discontinuation of immunotherapy: Diagnostic hazard of autoimmunity at a distance. J. Immunother. Cancer 2019, 7, 165. [Google Scholar] [CrossRef] [PubMed]
- June, C.H.; Warshauer, J.T.; Bluestone, J.A. Is autoimmunity the Achilles’ heel of cancer immunotherapy? Nat. Med. 2017, 23, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Postow Michael, A.; Sidlow, R.; Hellmann Matthew, D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Young, A.; Quandt, Z.; Bluestone, J.A. The balancing act between cancer immunity and autoimmunity in response to immunotherapy. Cancer Immunol. Res. 2018, 6, 1445–1452. [Google Scholar] [CrossRef]
- Verheijden, R.J.; van Eijs, M.J.M.; May, A.M.; van Wijk, F.; Suijkerbuijk, K.P.M. Immunosuppression for immune-related adverse events during checkpoint inhibition: An intricate balance. NPJ Precis. Oncol. 2023, 7, 41. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).






{kind=link}
{kind=link}
{kind=link}
{kind=link}