
MRI-Based Assessment of Brain Tumor Hypoxia: Correlation with Histology
 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. MR Data Acquisition
2.3. MR Data Analysis
2.4. Volume of Interest (VOI) Segmentation
2.5. VOI-Based MRI Data Evaluation
2.6. Image-Guided Biopsy Procedure
2.7. Histological Analysis
2.8. MRI Measurements in the Target Voxels
2.9. Statistical Analysis
3. Results
3.1. Patient and Biopsy Characteristics
3.2. Characteristics of the FLAIR-ASE Signal
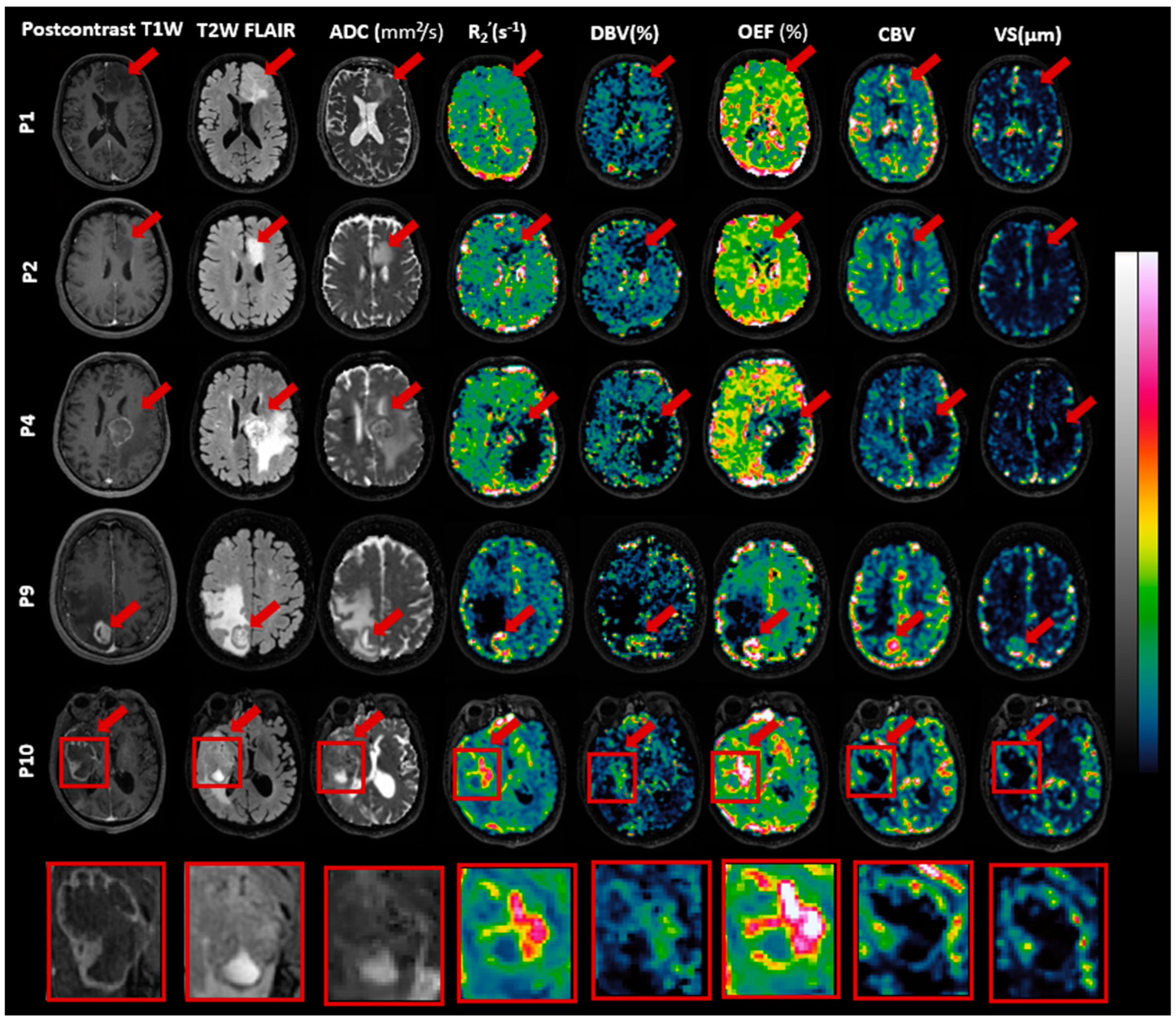
3.3. Features of MRI Parametric Maps
3.4. Histological Findings
3.5. Correlation between MRI and Histology
4. Discussion
4.1. Correlation between MRI and Histology
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Mendichovszky, I.; Jackson, A. Imaging Hypoxia in Gliomas. Br. J. Radiol. 2011, 84, S145–S158. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.L. Brain Tumor Hypoxia: Tumorigenesis, Angiogenesis, Imaging, Pseudoprogression, and as a Therapeutic Target. J. Neurooncol. 2009, 92, 317–335. [Google Scholar] [CrossRef] [PubMed]
- Gerstner, E.R.; Zhang, Z.; Fink, J.R.; Muzi, M.; Hanna, L.; Greco, E.; Prah, M.; Schmainda, K.M.; Mintz, A.; Kostakoglu, L.; et al. ACRIN 6684: Assessment of Tumor Hypoxia in Newly Diagnosed Glioblastoma Using 18F-FMISO PET and MRI. Clin. Cancer Res. 2016, 22, 5079–5086. [Google Scholar] [CrossRef]
- Li, H.; Wang, C.; Yu, X.; Luo, Y.; Wang, H. Measurement of Cerebral Oxygen Extraction Fraction Using Quantitative BOLD Approach: A Review. Phenomics 2023, 3, 101–118. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Yablonskiy, D.A. Quantitative BOLD: Mapping of Human Cerebral Deoxygenated Blood Volume and Oxygen Extraction Fraction: Default State. Magn. Reson. Med. 2007, 57, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Ni, W.; Christen, T.; Zun, Z.; Zaharchuk, G. Comparison of R2′ Measurement Methods in the Normal Brain at 3T. Magn. Reson. Med. 2015, 73, 1228–1236. [Google Scholar] [CrossRef]
- Stadlbauer, A.; Mouridsen, K.; Doerfler, A.; Bo Hansen, M.; Oberndorfer, S.; Zimmermann, M.; Buchfelder, M.; Heinz, G.; Roessler, K. Recurrence of Glioblastoma Is Associated with Elevated Microvascular Transit Time Heterogeneity and Increased Hypoxia. J. Cereb. Blood Flow. Metab. 2018, 38, 422–432. [Google Scholar] [CrossRef]
- Stadlbauer, A.; Zimmermann, M.; Doerfler, A.; Oberndorfer, S.; Buchfelder, M.; Coras, R.; Kitzwögerer, M.; Roessler, K. Intratumoral Heterogeneity of Oxygen Metabolism and Neovascularization Uncovers 2 Survival-Relevant Subgroups of IDH1 Wild-Type Glioblastoma. Neuro Oncol. 2018, 20, 1536–1546. [Google Scholar] [CrossRef]
- Stone, A.J.; Blockley, N.P. A Streamlined Acquisition for Mapping Baseline Brain Oxygenation Using Quantitative BOLD. Neuroimage 2017, 147, 79–88. [Google Scholar] [CrossRef]
- Stone, A.J.; Harston, G.W.J.; Carone, D.; Okell, T.W.; Kennedy, J.; Blockley, N.P. Prospects for Investigating Brain Oxygenation in Acute Stroke: Experience with a Non-Contrast Quantitative BOLD Based Approach. Hum. Brain Mapp. 2019, 40, 2853–2866. [Google Scholar] [CrossRef]
- Arzanforoosh, F.; Berman, A.J.L.; Smits, M.; Warnert, E.A.H. Streamlined Quantitative BOLD for Detecting Visual Stimulus-Induced Changes in Oxygen Extraction Fraction in Healthy Participants: Toward Clinical Application in Human Glioma. Magn. Reson. Mater. Phys. Biol. Med. 2023, 36, 975–984. [Google Scholar] [CrossRef] [PubMed]
- Kiselev, V.G.; Strecker, R.; Ziyeh, S.; Speck, O.; Hennig, J. Vessel Size Imaging in Humans. Magn. Reson. Med. 2005, 53, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Tóth, V.; Förschler, A.; Hirsch, N.M.; Den Hollander, J.; Kooijman, H.; Gempt, J.; Ringel, F.; Schlegel, J.; Zimmer, C.; Preibisch, C. MR-Based Hypoxia Measures in Human Glioma. J. Neurooncol. 2013, 115, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Chakhoyan, A.; Yao, J.; Leu, K.; Pope, W.B.; Salamon, N.; Yong, W.; Lai, A.; Nghiemphu, P.L.; Everson, R.G.; Prins, R.M.; et al. Validation of Vessel Size Imaging (VSI) in High-Grade Human Gliomas Using Magnetic Resonance Imaging, Image-Guided Biopsies, and Quantitative Immunohistochemistry. Sci. Rep. 2019, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.J.L.; Mazerolle, E.L.; MacDonald, M.E.; Blockley, N.P.; Luh, W.M.; Pike, G.B. Gas-Free Calibrated FMRI with a Correction for Vessel-Size Sensitivity. Neuroimage 2018, 169, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, P.F.; Gatehouse, P.D.; Firmin, D.N. Myocardial First-Pass Perfusion Imaging with Hybrid-EPI: Frequency-Offsets and Potential Artefacts. J. Cardiovasc. Magn. Reson. 2012, 14, 44. [Google Scholar] [CrossRef] [PubMed]
- Arzanforoosh, F.; van der Voort, S.R.; Incekara, F.; Vincent, A.; Van den Bent, M.; Kros, J.M.; Smits, M.; Warnert, E.A.H. Microvasculature Features Derived from Hybrid EPI MRI in Non-Enhancing Adult-Type Diffuse Glioma Subtypes. Cancers 2023, 15, 2135. [Google Scholar] [CrossRef]
- Jenkinson, M. Improved Optimization for the Robust and Accurate Linear Registration and Motion Correction of Brain Images. Neuroimage 2002, 17, 825–841. [Google Scholar] [CrossRef]
- Blockley, N.P.; Stone, A.J. Improving the Specificity of R2′ to the Deoxyhaemoglobin Content of Brain Tissue: Prospective Correction of Macroscopic Magnetic Field Gradients. Neuroimage 2016, 135, 253–260. [Google Scholar] [CrossRef]
- Cherukara, M.T.; Stone, A.J.; Chappell, M.A.; Blockley, N.P. Model-Based Bayesian Inference of Brain Oxygenation Using Quantitative BOLD. Neuroimage 2019, 202, 116106. [Google Scholar] [CrossRef]
- Spees, W.M.; Yablonskiy, D.A.; Oswood, M.C.; Ackerman, J.J.H. Water Proton MR Properties of Human Blood at 1.5 Tesla: Magnetic Susceptibility,T1,T2,T*2, and Non-Lorentzian Signal Behavior. Magn. Reson. Med. 2001, 45, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Boxerman, J.L.; Schmainda, K.M.; Weisskoff, R.M. Relative Cerebral Blood Volume Maps Corrected for Contrast Agent Extravasation Significantly Correlate with Glioma Tumor Grade, Whereas Uncorrected Maps Do Not. Am. J. Neuroradiol. 2006, 27, 859–867. [Google Scholar] [PubMed]
- Arzanforoosh, F.; Croal, P.L.; van Garderen, K.A.; Smits, M.; Chappell, M.A.; Warnert, E.A.H. Effect of Applying Leakage Correction on RCBV Measurement Derived From DSC-MRI in Enhancing and Nonenhancing Glioma. Front. Oncol. 2021, 11, 648528. [Google Scholar] [CrossRef] [PubMed]
- Isensee, F.; Jaeger, P.F.; Kohl, S.A.A.; Petersen, J.; Maier-Hein, K.H. NnU-Net: A Self-Configuring Method for Deep Learning-Based Biomedical Image Segmentation. Nat. Methods 2021, 18, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Kickingereder, P.; Isensee, F.; Tursunova, I.; Petersen, J.; Neuberger, U.; Bonekamp, D.; Brugnara, G.; Schell, M.; Kessler, T.; Foltyn, M.; et al. Automated Quantitative Tumour Response Assessment of MRI in Neuro-Oncology with Artificial Neural Networks: A Multicentre, Retrospective Study. Lancet Oncol. 2019, 20, 728–740. [Google Scholar] [CrossRef] [PubMed]
- McKinley, R.; Rebsamen, M.; Dätwyler, K.; Meier, R.; Radojewski, P.; Wiest, R. Uncertainty-Driven Refinement of Tumor-Core Segmentation Using 3D-to-2D Networks with Label Uncertainty. In Brainlesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries: 6th International Workshop, BrainLes 2020, Held in Conjunction with MICCAI 2020, Lima, Peru, 4 October 2020, Revised Selected Papers, Part I; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; Volume 6, pp. 401–411. [Google Scholar]
- Isensee, F.; Schell, M.; Pflueger, I.; Brugnara, G.; Bonekamp, D.; Neuberger, U.; Wick, A.; Schlemmer, H.; Heiland, S.; Wick, W.; et al. Automated Brain Extraction of Multisequence MRI Using Artificial Neural Networks. Hum. Brain Mapp. 2019, 40, 4952–4964. [Google Scholar] [CrossRef]
- Klein, S.; Staring, M.; Murphy, K.; Viergever, M.A.; Pluim, J. Elastix: A Toolbox for Intensity-Based Medical Image Registration. IEEE Trans. Med. Imaging 2010, 29, 196–205. [Google Scholar] [CrossRef]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open Source Software for Digital Pathology Image Analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef]
- Preibisch, C.; Shi, K.; Kluge, A.; Lukas, M.; Wiestler, B.; Göttler, J.; Gempt, J.; Ringel, F.; Al Jaberi, M.; Schlegel, J.; et al. Characterizing Hypoxia in Human Glioma: A Simultaneous Multimodal MRI and PET Study. NMR Biomed. 2017, 30, e3775. [Google Scholar] [CrossRef]
- Ahir, B.K.; Engelhard, H.H.; Lakka, S.S. Tumor Development and Angiogenesis in Adult Brain Tumor: Glioblastoma. Mol. Neurobiol. 2020, 57, 2461–2478. [Google Scholar] [CrossRef]
- Yablonskiy, D.A.; Haacke, E.M. Theory of NMR Signal Behavior in Magnetically Inhomogeneous Tissues: The Static Dephasing Regime. Magn. Reson. Med. 1994, 32, 749–763. [Google Scholar] [CrossRef] [PubMed]
- Leu, K.; Ott, G.A.; Lai, A.; Nghiemphu, P.L.; Pope, W.B.; Yong, W.H.; Liau, L.M.; Cloughesy, T.F.; Ellingson, B.M. Perfusion and Diffusion MRI Signatures in Histologic and Genetic Subtypes of WHO Grade II–III Diffuse Gliomas. J. Neurooncol. 2017, 134, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Stadlbauer, A.; Eyüpoglu, I.; Buchfelder, M.; Dörfler, A.; Zimmermann, M.; Heinz, G.; Oberndorfer, S. Vascular Architecture Mapping for Early Detection of Glioblastoma Recurrence. Neurosurg. Focus 2019, 47, E14. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Omuro, A. Glioblastoma and Other Malignant Gliomas. JAMA 2013, 310, 1842. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Chakhoyan, A.; Nathanson, D.A.; Yong, W.H.; Salamon, N.; Raymond, C.; Mareninov, S.; Lai, A.; Nghiemphu, P.L.; Prins, R.M.; et al. Metabolic Characterization of Human IDH Mutant and Wild Type Gliomas Using Simultaneous PH- and Oxygen-Sensitive Molecular MRI. Neuro Oncol. 2019, 21, 1184–1196. [Google Scholar] [CrossRef]
- Hilario, A.; Ramos, A.; Perez-Nuñez, A.; Salvador, E.; Millan, J.M.; Lagares, A.; Sepulveda, J.M.; Gonzalez-Leon, P.; Hernandez-Lain, A.; Ricoy, J.R. The Added Value of Apparent Diffusion Coefficient to Cerebral Blood Volume in the Preoperative Grading of Diffuse Gliomas. Am. J. Neuroradiol. 2012, 33, 701–707. [Google Scholar] [CrossRef]
- Lebelt, A.; Dziecioł, J.; Guzińska-Ustymowicz, K.; Lemancewicz, D.; Zimnoch, L.; Czykier, E. Angiogenesis in Gliomas. Folia Histochem. Cytobiol. 2008, 46, 69–72. [Google Scholar] [CrossRef]
- Stone, A.; Blockley, N. Improving QBOLD Based Measures of Oxygen Extraction Fraction Using Hyperoxia-BOLD Derived Measures of Blood Volume. bioRxiv 2020. [Google Scholar] [CrossRef]
- Sharma, S.; Sharma, M.C.; Sarkar, C. Morphology of Angiogenesis in Human Cancer: A Conceptual Overview, Histoprognostic Perspective and Significance of Neoangiogenesis. Histopathology 2005, 46, 481–489. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No./Sex/Age(y) | Pathologic Diagnosis | # Samples from Necrosis VOI | # Samples from Enhancing VOI | # Samples from Nonenhancing VOI |
|---|---|---|---|---|
| 1/M/56 | Oligodendroglioma (grade 2) | - | - | 4 |
| 2/F/74 | Astrocytoma (grade 2) | - | - | 4 |
| 3/F/52 | Brain Metastasis (lung carcinoma) | - | 2 | - |
| 4/M/57 | Brain Metastasis (adenocarcinoma) | 2 | 1 | - |
| 5/M/72 | Brain Metastasis (adenocarcinoma) | - | - | 2 |
| 6/F/40 | Oligodendroglioma (grade 3) | - | 2 | 1 |
| 7/F/78 | Brain Metastasis (adenocarcinoma) | - | 3 | - |
| 8/M/75 | Glioblastoma (grade 4) | 3 | 1 | - |
| 9/F/68 | Brain Metastasis (melanoma) | 1 | 3 | - |
| 10/M/75 | Glioblastoma (grade 4) | 2 | 2 | - |
| Total: 8 | Total: 14 | Total: 11 |
| VOI | R2′ (s–1) | DBV (%) | OEF (%) | CBV | Vessel Size (µm) |
|---|---|---|---|---|---|
| Contra-GM (n = 10) | 5.13 (1.74) | 4.30 (1.60) | 43.89 (16.88) | 1.66 (0.33) | 16.24 (3.14) |
| Edema (n = 4) | 3.21 (0.58) | 7.43 (2.73) | 21.06 (7.08) | 0.71 (0.13) | 16.78 (5.72) |
| Nonenhancing (n = 4) | 2.56 (0.33) | 7.48 (0.89) | 14.90 (2.08) | 1.04 (0.44) | 12.97 (6.74) |
| Enhancing (n = 8) | 7.90 (5.54) | 6.44 (4.12) | 60.81 (44.88) | 1.78 (1.41) | 25.73 (22.68) |
| Necrosis (n = 5) | 7.36 (6.67) | 6.72 (4.45) | 54.15 (52.34) | 0.70 (0.78) | 16.61 (16.52) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arzanforoosh, F.; Van der Velden, M.; Berman, A.J.L.; Van der Voort, S.R.; Bos, E.M.; Schouten, J.W.; Vincent, A.J.P.E.; Kros, J.M.; Smits, M.; Warnert, E.A.H. MRI-Based Assessment of Brain Tumor Hypoxia: Correlation with Histology. Cancers 2024, 16, 138. https://doi.org/10.3390/cancers16010138
Arzanforoosh F, Van der Velden M, Berman AJL, Van der Voort SR, Bos EM, Schouten JW, Vincent AJPE, Kros JM, Smits M, Warnert EAH. MRI-Based Assessment of Brain Tumor Hypoxia: Correlation with Histology. Cancers. 2024; 16(1):138. https://doi.org/10.3390/cancers16010138
Chicago/Turabian StyleArzanforoosh, Fatemeh, Maaike Van der Velden, Avery J. L. Berman, Sebastian R. Van der Voort, Eelke M. Bos, Joost W. Schouten, Arnaud J. P. E. Vincent, Johan M. Kros, Marion Smits, and Esther A. H. Warnert. 2024. "MRI-Based Assessment of Brain Tumor Hypoxia: Correlation with Histology" Cancers 16, no. 1: 138. https://doi.org/10.3390/cancers16010138