
Efficacy of Lymph Node Location-Number Hybrid Staging System on the Prognosis of Gastric Cancer Patients
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Follow Up
2.3. Statistics Analysis
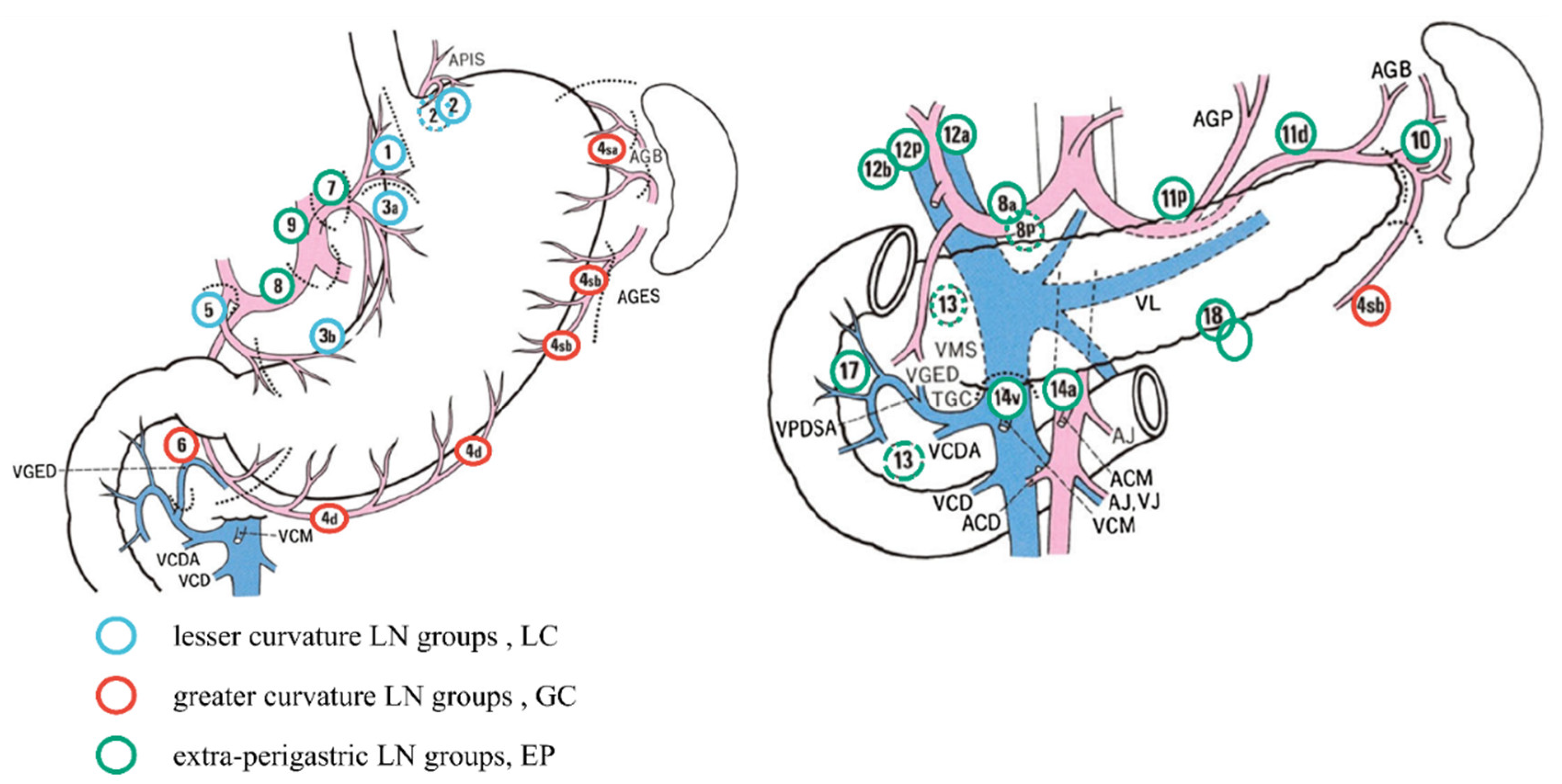
2.4. Lymph Nodes Location-Number Hybrid Staging System Criteria
- hN0: No positive lymph nodes.
- hN1: LC/GC had positive lymph nodes irrespective of the number, or EP had positive lymph nodes, and the number of positive lymph nodes in the EP group was ≤4.
- hN2: Two groups of LC/GC/EP had positive lymph nodes, regardless of the number. EP had positive lymph nodes, and the number of lymph nodes was >4.
- hN3a: LC + GC + EP all had positive lymph nodes, and the total number of positive lymph nodes was ≤14.
- hN3b: LC + GC + EP all had positive lymph nodes, and the total number of positive lymph nodes was >14.
3. Results
3.1. Patient Baseline Characteristics
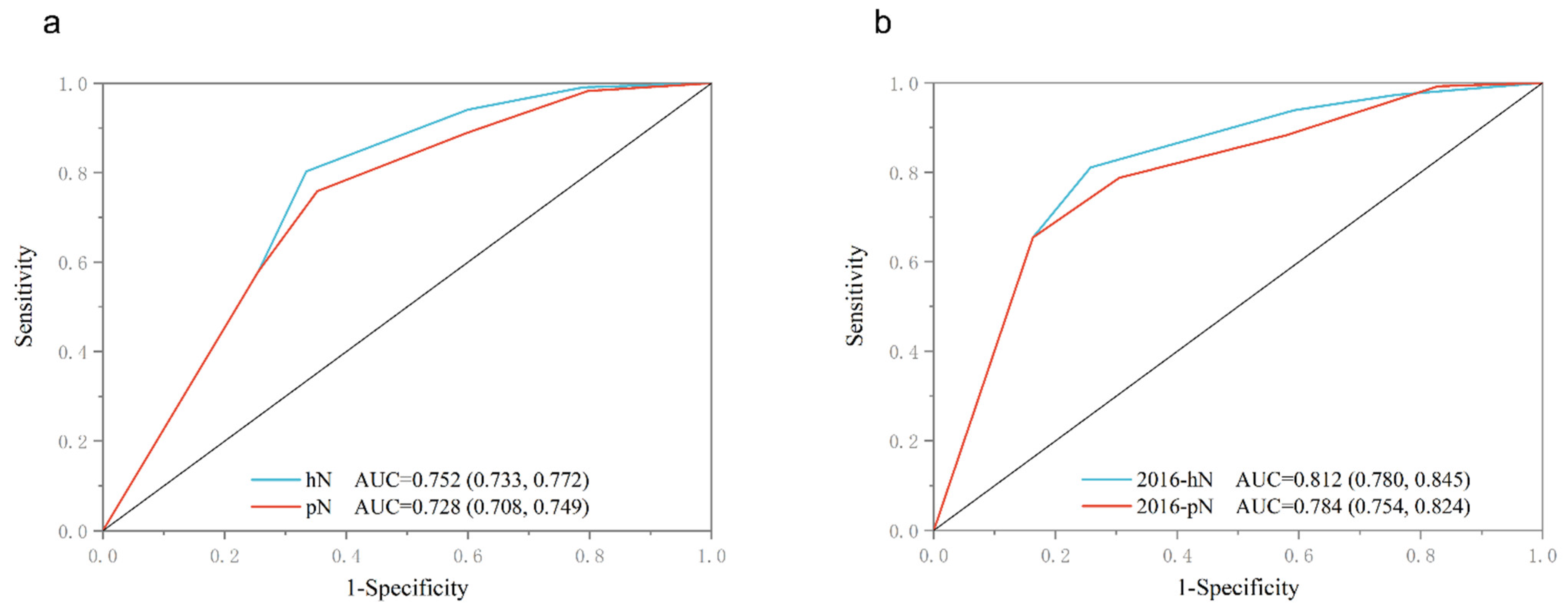
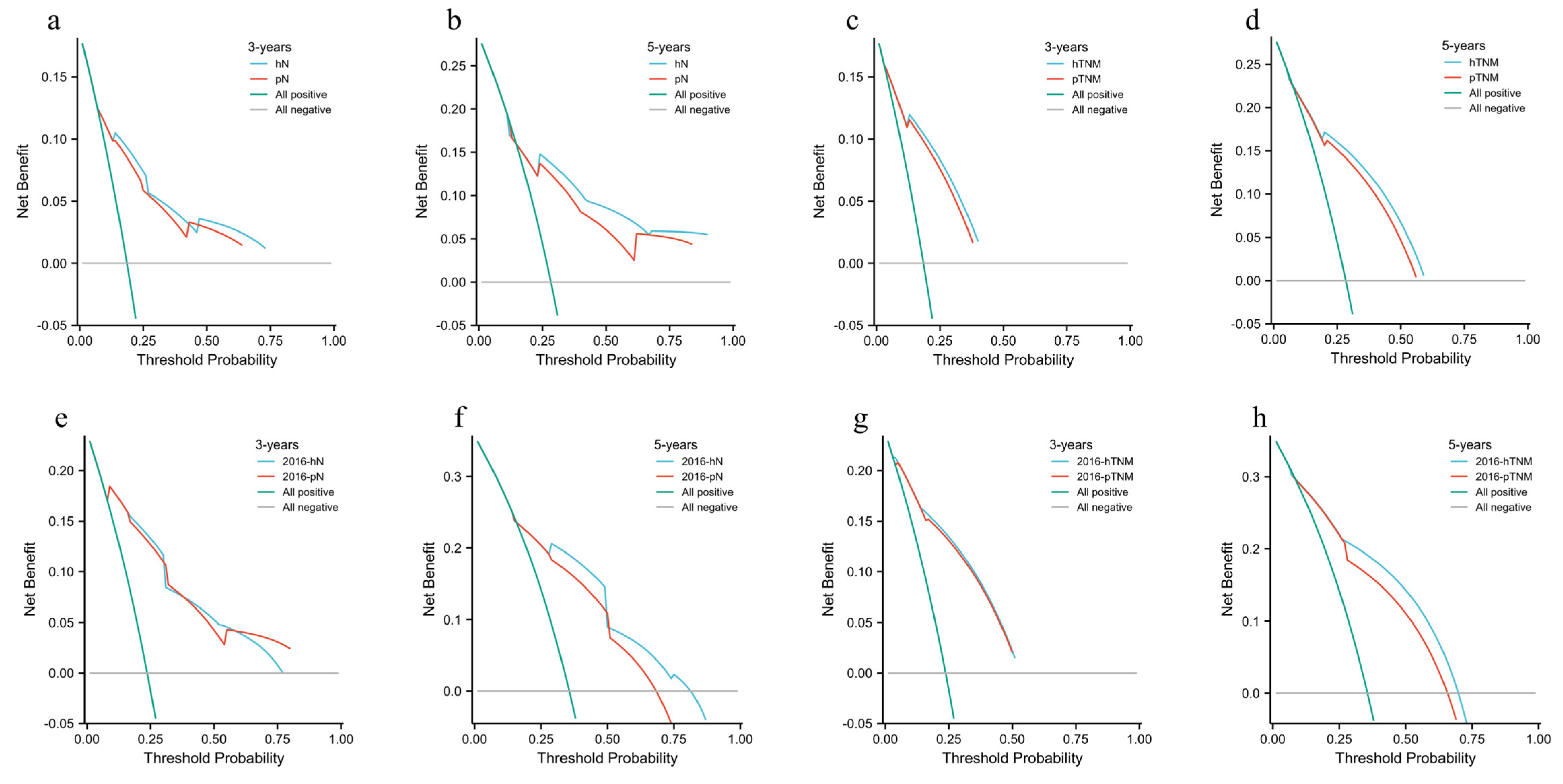
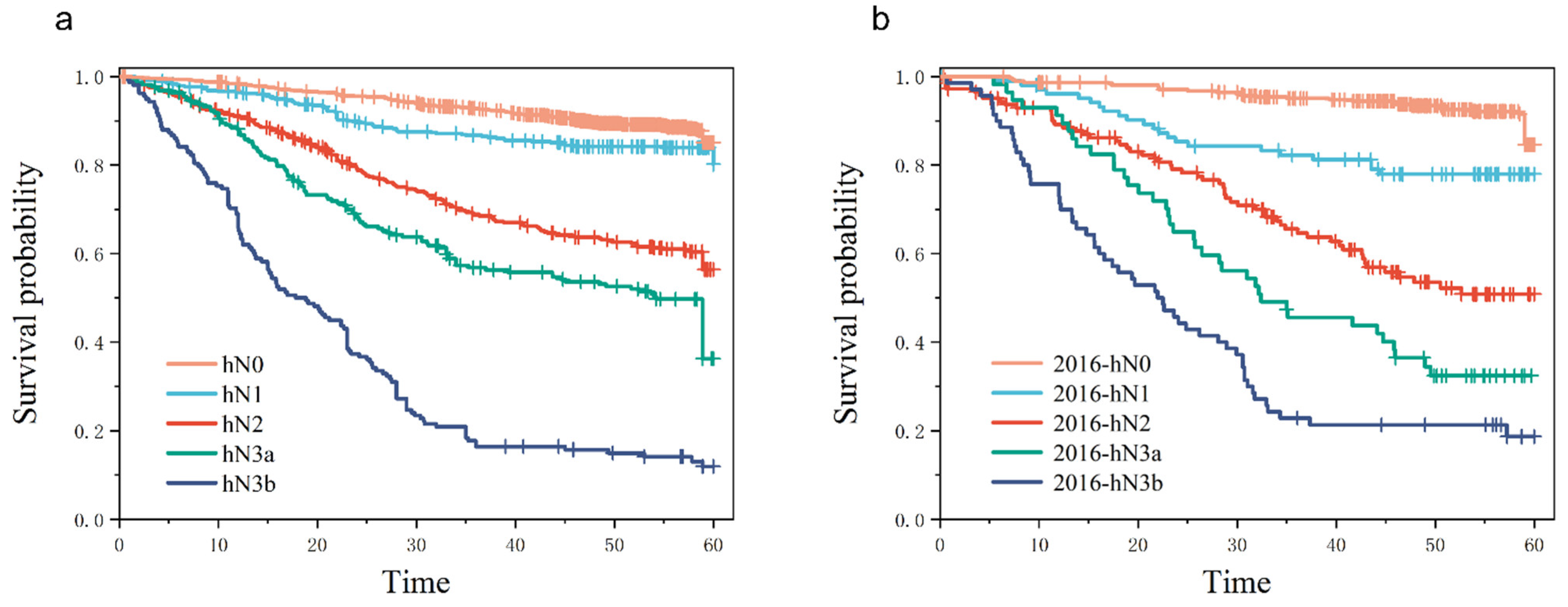
3.2. Evaluation of the Predictive Ability of hN Staging
3.3. Univariate and Multivariate Analysis of Prognostic Factors in Patients with hN Staging
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Biondi, A.; Hyung, W.J. Seventh edition of TNM classification for gastric cancer. J. Clin. Oncol. 2011, 29, 4338–4339. [Google Scholar] [CrossRef] [PubMed]
- Kutlu, O.C.; Watchell, M.; Dissanaike, S. Metastatic lymph node ratio successfully predicts prognosis in western gastric cancer patients. Surg. Oncol. 2015, 24, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Kooby, D.A.; Suriawinata, A.; Klimstra, D.S.; Brennan, M.F.; Karpeh, M.S. Biologic predictors of survival in node-negative gastric cancer. Ann. Surg. 2003, 237, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Behrns, K.E.; Dalton, R.R.; van Heerden, J.A.; Sarr, M.G. Extended lymph node dissection for gastric cancer. Is it of value? Surg. Clin. N. Am. 1992, 72, 433–443. [Google Scholar] [CrossRef]
- Cuschieri, A.; Weeden, S.; Fielding, J.; Bancewicz, J.; Craven, J.; Joypaul, V.; Sydes, M.; Fayers, P. Patient survival after D1 and D2 resections for gastric cancer: Long-term results of the MRC randomized surgical trial. Surgical Co-operative Group. Br. J. Cancer 1999, 79, 1522–1530. [Google Scholar] [CrossRef]
- Siewert, J.R.; Böttcher, K.; Stein, H.J.; Roder, J.D. Relevant prognostic factors in gastric cancer: Ten-year results of the German Gastric Cancer Study. Ann. Surg. 1998, 228, 449–461. [Google Scholar] [CrossRef]
- Maruyama, K.; Gunvén, P.; Okabayashi, K.; Sasako, M.; Kinoshita, T. Lymph node metastases of gastric cancer. General pattern in 1931 patients. Ann. Surg. 1989, 210, 596–602. [Google Scholar] [CrossRef]
- Martinez-Ramos, D.; Calero, A.; Escrig-Sos, J.; Mingol, F.; Daroca-Jose, J.M.; Sauri, M.; Arroyo, A.; Salvador-Sanchis, J.L.; de Juan, M.; Calpena, R.; et al. Prognosis for gastric carcinomas with an insufficient number of examined negative lymph nodes. Eur. J. Surg. Oncol. 2014, 40, 358–365. [Google Scholar] [CrossRef]
- He, X.; Wu, W.; Lin, Z.; Ding, Y.; Si, J.; Sun, L.M. Validation of the American Joint Committee on Cancer (AJCC) 8th edition stage system for gastric cancer patients: A population-based analysis. Gastric Cancer 2018, 21, 391–400. [Google Scholar] [CrossRef]
- Marrelli, D.; Ferrara, F.; Giacopuzzi, S.; Morgagni, P.; Di Leo, A.; De Franco, L.; Pedrazzani, C.; Saragoni, L.; De Manzoni, G.; Roviello, F. Incidence and Prognostic Value of Metastases to "Posterior" and Para-aortic Lymph Nodes in Resectable Gastric Cancer. Ann. Surg. Oncol. 2017, 24, 2273–2280. [Google Scholar] [CrossRef]
- Choi, Y.Y.; An, J.Y.; Katai, H.; Seto, Y.; Fukagawa, T.; Okumura, Y.; Kim, D.W.; Kim, H.I.; Cheong, J.H.; Hyung, W.J.; et al. A Lymph Node Staging System for Gastric Cancer: A Hybrid Type Based on Topographic and Numeric Systems. PLoS ONE 2016, 11, e0149555. [Google Scholar] [CrossRef]
- Rosa, F.; Costamagna, G.; Doglietto, G.B.; Alfieri, S. Classification of nodal stations in gastric cancer. Transl. Gastroenterol. Hepatol. 2017, 2, 2. [Google Scholar] [CrossRef]
- Karavokyros, I.; Michalinos, A. Favoring D(2)-Lymphadenectomy in Gastric Cancer. Front. Surg. 2018, 5, 42. [Google Scholar] [CrossRef]
- Chen, M.W.; Chan, C.P.; Lin, Y.J.; Yen, H.H. Anatomical location-based nodal staging system is superior to the 7th edition of the American Joint Committee on Cancer staging system among patients with surgically resected, histologically low-grade gastric cancer: A single institutional experience. PLoS ONE 2019, 14, e0211836. [Google Scholar] [CrossRef]
- Lauricella, S.; Caricato, M.; Mascianà, G.; Carannante, F.; Carnazza, M.; Bonaccorso, A.; Angeletti, S.; Ciccozzi, M.; Coppola, R.; Capolupo, G.T. Topographic lymph node staging system shows prognostic superiority compared to the 8th edition of AJCC TNM in gastric cancer. A western monocentric experience. Surg. Oncol. 2020, 34, 223–233. [Google Scholar] [CrossRef]
- Sano, T.; Coit, D.G.; Kim, H.H.; Roviello, F.; Kassab, P.; Wittekind, C.; Yamamoto, Y.; Ohashi, Y. Proposal of a new stage grouping of gastric cancer for TNM classification: International Gastric Cancer Association staging project. Gastric Cancer 2017, 20, 217–225. [Google Scholar] [CrossRef]
- Abdel-Rahman, O. Validation of the 8th AJCC staging system for gastric cancer in a population-based setting. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 525–530. [Google Scholar] [CrossRef]
- Huang, S.F.; Chien, T.H.; Fang, W.L.; Wang, F.; Tsai, C.Y.; Hsu, J.T.; Yeh, C.N.; Chen, T.C.; Wu, R.C.; Chiu, C.T.; et al. The 8th edition American Joint Committee on gastric cancer pathological staging classification performs well in a population with high proportion of locally advanced disease. Eur. J. Surg. Oncol. 2018, 44, 1634–1639. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 2011, 14, 101–112. [Google Scholar] [CrossRef]
- Mine, S.; Yamada, K.; Grabsch, H.; Sano, T.; Ishiyama, A.; Hirasawa, T.; Yamamoto, N.; Hiki, N.; Yamaguchi, T. The prognostic significance of tumor laterality in patients with esophageal squamous cell carcinoma. J. Surg. Oncol. 2012, 105, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.J.; Seo, H.S.; Kim, J.H.; Park, C.H.; Lee, H.H. Cross-Sectional Location of Gastric Cancer Affects the Long-Term Survival of Patients as Tumor Invasion Deepens. Ann. Surg. Oncol. 2017, 24, 3947–3953. [Google Scholar] [CrossRef] [PubMed]
- Shida, A.; Mitsumori, N.; Fujioka, S.; Takano, Y.; Fujisaki, M.; Hashizume, R.; Takahashi, N.; Ishibashi, Y.; Yanaga, K. Sentinel Node Navigation Surgery for Early Gastric Cancer: Analysis of Factors Which Affect Direction of Lymphatic Drainage. World J. Surg. 2018, 42, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Du, Y.; Xu, Z.; Huang, L.; Cheng, X. Comparison of D2 and D2 plus radical surgery for advanced distal gastric cancer: A randomized controlled study. World J. Surg. Oncol. 2019, 17, 28. [Google Scholar] [CrossRef]
- Han, W.H.; Joo, J.; Eom, B.W.; Ryu, K.W.; Kim, Y.W.; Kook, M.C.; Yoon, H.M. Factors associated with metastasis in superior mesenteric vein lymph node in subtotal gastrectomy for gastric cancer: Retrospective case control study. Chin. J. Cancer Res. 2020, 32, 43–50. [Google Scholar] [CrossRef]
- Hayashi, H.; Ochiai, T.; Suzuki, T.; Shimada, H.; Hori, S.; Takeda, A.; Miyazawa, Y. Superiority of a new UICC-TNM staging system for gastric carcinoma. Surgery 2000, 127, 129–135. [Google Scholar] [CrossRef]
- Lu, J.; Zheng, C.H.; Cao, L.L.; Li, P.; Xie, J.W.; Wang, J.B.; Lin, J.X.; Chen, Q.Y.; Lin, M.; Tu, R.H.; et al. Comparison of the 7th and 8th editions of the American joint committee on cancer TNM classification for patients with stage III gastric cancer. Oncotarget 2017, 8, 83555–83562. [Google Scholar] [CrossRef]
- Wu, C.W.; Hsiung, C.A.; Lo, S.S.; Hsieh, M.C.; Chen, J.H.; Li, A.F.; Lui, W.Y.; Whang-Peng, J. Nodal dissection for patients with gastric cancer: A randomised controlled trial. Lancet Oncol. 2006, 7, 309–315. [Google Scholar] [CrossRef]
- Kim, E.Y.; Song, K.Y.; Lee, J. Does Hospital Volume Really Affect the Surgical and Oncological Outcomes of Gastric Cancer in Korea? J. Gastric Cancer 2017, 17, 246–254. [Google Scholar] [CrossRef]
- Maruyama, K.; Katai, H. Surgical treatment of gastric cancer in Japan, trend from standardization to individualization. Chirurgia 2014, 109, 722–730. [Google Scholar]
- Katai, H.; Ishikawa, T.; Akazawa, K.; Isobe, Y.; Miyashiro, I.; Oda, I.; Tsujitani, S.; Ono, H.; Tanabe, S.; Fukagawa, T.; et al. Five-year survival analysis of surgically resected gastric cancer cases in Japan: A retrospective analysis of more than 100,000 patients from the nationwide registry of the Japanese Gastric Cancer Association (2001–2007). Gastric Cancer 2018, 21, 144–154. [Google Scholar] [CrossRef]
- Faiz, Z.; Hayashi, T.; Yoshikawa, T. Lymph node dissection for gastric cancer: Establishment of D2 and the current position of splenectomy in Europe and Japan. Eur. J. Surg. Oncol. 2021, 47, 2233–2236. [Google Scholar] [CrossRef]
- Wen, J.; Yang, Y.; Liu, P.; Ye, F.; Tang, H.; Huang, X.; Zhong, S.; Xie, X. Development and validation of a nomogram for predicting survival on the base of modified lymph node ratio in breast cancer patients. Breast 2017, 33, 14–22. [Google Scholar] [CrossRef]
- Wang, J.; Dang, P.; Raut, C.P.; Pandalai, P.K.; Maduekwe, U.N.; Rattner, D.W.; Lauwers, G.Y.; Yoon, S.S. Comparison of a lymph node ratio-based staging system with the 7th AJCC system for gastric cancer: Analysis of 18,043 patients from the SEER database. Ann. Surg. 2012, 255, 478–485. [Google Scholar] [CrossRef]
- Marchet, A.; Mocellin, S.; Ambrosi, A.; Morgagni, P.; Garcea, D.; Marrelli, D.; Roviello, F.; de Manzoni, G.; Minicozzi, A.; Natalini, G.; et al. The ratio between metastatic and examined lymph nodes (N ratio) is an independent prognostic factor in gastric cancer regardless of the type of lymphadenectomy: Results from an Italian multicentric study in 1853 patients. Ann. Surg. 2007, 245, 543–552. [Google Scholar] [CrossRef]
- Xie, J.; Pang, Y.; Li, X.; Wu, X. The log odds of negative lymph nodes/T stage: A new prognostic and predictive tool for resected gastric cancer patients. J. Cancer Res. Clin. Oncol. 2021, 147, 2259–2269. [Google Scholar] [CrossRef]
- Li, G.C.; Jia, X.C.; Zhao, Q.C.; Zhang, H.W.; Yang, P.; Xu, L.L.; Pang, F.N.; Sun, J.B. The expression of epidermal growth factor receptor 1 and human epidermal growth factor receptor 2 based on tumor location affect survival in gastric cancer. Medicine 2020, 99, e20460. [Google Scholar] [CrossRef]
- Eom, B.W.; Jung, K.W.; Won, Y.J.; Yang, H.; Kim, Y.W. Trends in Gastric Cancer Incidence According to the Clinicopathological Characteristics in Korea, 1999–2014. Cancer Res. Treat. 2018, 50, 1343–1350. [Google Scholar] [CrossRef]
- Yao, K.; Uedo, N.; Kamada, T.; Hirasawa, T.; Nagahama, T.; Yoshinaga, S.; Oka, M.; Inoue, K.; Mabe, K.; Yao, T.; et al. Guidelines for endoscopic diagnosis of early gastric cancer. Dig. Endosc. 2020, 32, 663–698. [Google Scholar] [CrossRef]
- Verlato, G.; Marrelli, D.; Accordini, S.; Bencivenga, M.; Di Leo, A.; Marchet, A.; Petrioli, R.; Zoppini, G.; Muggeo, M.; Roviello, F.; et al. Short-term and long-term risk factors in gastric cancer. World J. Gastroenterol. 2015, 21, 6434–6443. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (%) | Training Cohort hN | Validation Cohort hN | p |
|---|---|---|---|---|
| n | 3354 | 2598 | 756 | |
| Age, n (%) | 0.060 | |||
| ≤60 | 1899 (56.62%) | 1494 (44.5%) | 405 (12.1%) | |
| >60 | 1455 (43.38%) | 1104 (32.9%) | 351 (10.5%) | |
| Gender, n (%) | 0.153 | |||
| Male | 2444 (72.87%) | 1909 (56.9%) | 535 (16%) | |
| Female | 910 (27.13%) | 689 (20.5%) | 221 (6.6%) | |
| Tumor location, n (%) | 0.383 | |||
| L | 2419 (72.13%) | 1890 (56.4%) | 529 (15.8%) | |
| M | 530 (15.80%) | 403 (12%) | 127 (3.8%) | |
| U | 354 (10.55%) | 269 (8%) | 85 (2.5%) | |
| LMU | 51 (1.52%) | 36 (1.1%) | 15 (0.4%) | |
| hN, n (%) | <0.001 | |||
| hN0 | 1671 (49.82%) | 1291 (38.5%) | 380 (11.3%) | |
| hN1 | 587 (17.50%) | 483 (14.4%) | 104 (3.1%) | |
| hN2 | 588 (17.53%) | 443 (13.2%) | 145 (4.3%) | |
| hN3a | 280 (8.35%) | 223 (6.6%) | 57 (1.7%) | |
| hN3b | 228 (6.80%) | 158 (4.7%) | 70 (2.1%) | |
| pT stage, n (%) | <0.001 | |||
| T1 | 854 (25.47%) | 656 (19.6%) | 198 (5.9%) | |
| T2 | 527 (15.71%) | 417 (12.4%) | 110 (3.3%) | |
| T3 | 1218 (36.31%) | 901 (26.9%) | 317 (9.5%) | |
| T4 | 755 (22.51%) | 624 (18.6%) | 131 (3.9%) | |
| hTNM, n (%) | 0.316 | |||
| Ⅰ | 1154 (34.41%) | 885 (26.4%) | 269 (8%) | |
| Ⅱ | 1029 (30.68%) | 814 (24.3%) | 215 (6.4%) | |
| Ⅲ | 1171 (34.91%) | 899 (26.8%) | 272 (8.1%) | |
| Histological type, n (%) | 0.037 | |||
| Adenocarcinoma | 2679 (79.87%) | 2090 (62.3%) | 589 (17.6%) | |
| Low adhesion adenocarcinoma | 460 (13.71%) | 347 (10.3%) | 113 (3.4%) | |
| mucoid adenocarcinoma | 151 (4.50%) | 120 (3.6%) | 31 (0.9%) | |
| Signet-ring cell carcinoma | 64 (1.92%) | 41 (1.2%) | 23 (0.7%) | |
| Differentiation degree, n (%) | 0.031 | |||
| G1 | 298 (8.88%) | 221 (6.6%) | 77 (2.3%) | |
| G2 | 1736 (51.76%) | 1325 (39.5%) | 411 (12.3%) | |
| G3 | 1320 (39.36%) | 1052 (31.4%) | 268 (8%) | |
| HER-2, n (%) | <0.001 | |||
| 0 | 1772 (52.83%) | 1303 (38.8%) | 469 (14%) | |
| 1+ | 926 (27.61%) | 758 (22.6%) | 168 (5%) | |
| 2+ | 434 (12.94%) | 356 (10.6%) | 78 (2.3%) | |
| 3+ | 222 (6.62%) | 181 (5.4%) | 41 (1.2%) | |
| BMI, median (IQR) | 22.59 (20.42, 24.8) | 23.04 (20.76, 25.09) | 0.029 | |
| CEA, median (IQR) | 2.03 (1.2, 3.3) | 1.89 (1.07, 3.04) | 0.005 | |
| CA-199, median (IQR) | 9.09 (5.6, 16.89) | 10.02 (6, 16.89) | 0.183 | |
| MLNs, median (IQR) | 1 (0, 4) | 0 (0, 5) | 0.653 | |
| RLNs, median (IQR) | 27 (20, 35) | 27 (21, 34) | 0.995 | |
| LNRS, median (IQR) | 0.02 (0, 0.17) | 0 (0, 0.19) | 0.556 | |
| Tumor size, median (IQR) | 40 (30, 60) | 45 (30, 60) | 0.042 |
| Characteristics | Patients, n (%) | hN0, n (%) | hN1, n (%) | hN2, n (%) | hN3a, n (%) | hN3b, n (%) | p |
|---|---|---|---|---|---|---|---|
| n | 2598 | 1291 (49.69%) | 483 (18.59%) | 443 (17.05%) | 223 (8.58%) | 158 (6.08%) | |
| Age, Mean ± SD | 57.97 ± 10.05 | 57.61 ± 9.93 | 59.43 ± 10.02 | 57.79 ± 10.91 | 57.67 ± 9.23 | 57.42 ± 9.40 | 0.009 |
| BMI, Mean ± SD | 22.75 ± 3.22 | 23.12 ± 3.21 | 22.59 ± 3.15 | 22.37 ± 3.17 | 22.18 ± 3.19 | 22.18 ± 3.42 | <0.001 |
| CEA, Mean ± SD | 6.64 ± 39.56 | 3.63 ± 14.93 | 6.45 ± 46.37 | 8.87 ± 42.58 | 7.45 ± 20.97 | 24.36 ± 106.42 | <0.001 |
| CA-199, Mean ± SD | 30.78 ± 102.63 | 17.47 ± 58.88 | 26.04 ± 82.77 | 38.62 ± 113.76 | 55.37 ± 151.21 | 97.39 ± 225.42 | <0.001 |
| RLNs, Mean ± SD | 28.21 ± 11.88 | 25.65 ± 10.83 | 27.84 ± 11.96 | 31.47 ± 12.47 | 29.73 ± 10.96 | 38.96 ± 11.04 | <0.001 |
| MLNs, Mean ± SD | 3.62 ± 6.68 | 0 | 2.21 ± 2.08 | 6.87 ± 6.16 | 7.47 ± 2.77 | 22.97 ± 8.03 | <0.001 |
| LNRs, Mean ± SD | 0.12 ± 0.19 | 0 | 0.09 ± 0.08 | 0.24 ± 0.20 | 0.28 ± 0.14 | 0.61 ± 0.18 | <0.001 |
| Age, n (%) | 0.087 | ||||||
| ≤60 | 1494 (57.51%) | 766 (59.33%) | 254 (52.59%) | 246 (55.53%) | 134 (60.09%) | 94 (59.49%) | |
| >60 | 1104 (42.49%) | 525 (40.67%) | 229 (47.41%) | 197 (44.47%) | 89 (39.91%) | 64 (40.51%) | |
| Gender, n (%) | 0.567 | ||||||
| Male | 1909 (73.48%) | 943 (73.04%) | 362 (74.95%) | 316 (71.33%) | 166 (74.44%) | 122 (77.22%) | |
| Female | 689 (26.52%) | 348 (26.96%) | 121 (25.05%) | 127 (28.67%) | 57 (25.56%) | 36 (22.78%) | |
| Tumor location, n (%) | <0.001 | ||||||
| L | 1890 (72.75%) | 974 (75.45%) | 367 (75.98%) | 311 (70.20%) | 146 (65.47%) | 92 (58.23%) | |
| M | 403 (15.51%) | 185 (14.33%) | 60 (12.42%) | 74 (16.70%) | 50 (22.42%) | 34 (21.52%) | |
| U | 269 (10.35%) | 123 (9.53%) | 53 (10.97%) | 45 (10.17%) | 24 (10.76%) | 24 (15.19%) | |
| LMU | 36 (1.39%) | 9 (0.70%) | 3 (0.62%) | 13 (2.93%) | 3 (1.34%) | 8 (5.07%) | |
| T stage, n (%) | <0.001 | ||||||
| T1 | 656 (25.25%) | 570 (44.15%) | 61 (12.63%) | 22 (4.97%) | 3 (1.35%) | 0 (0%) | |
| T2 | 417 (16.05%) | 254 (19.67%) | 85 (17.60%) | 52 (11.74%) | 21 (9.42%) | 5 (3.16%) | |
| T3 | 901 (34.68%) | 326 (25.25%) | 197 (40.79%) | 212 (47.86%) | 104 (46.64%) | 62 (39.24%) | |
| T4 | 624 (24.02%) | 141 (10.92%) | 140 (28.98%) | 157 (35.43%) | 95 (42.59%) | 91 (57.60%) | |
| TNM stage, n (%) | <0.001 | ||||||
| I | 885 (34.06%) | 824 (63.83%) | 61 (12.63%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| II | 814 (31.33%) | 453 (35.09%) | 282 (58.39%) | 76 (17.16%) | 3 (1.35%) | 0 (0%) | |
| III | 899 (34.61%) | 14 (1.08%) | 140 (29.98%) | 367 (82.84%) | 220 (98.65%) | 158 (100%) | |
| Histological type, n (%) | <0.001 | ||||||
| Adenocarcinoma | 2090 (80.45%) | 1051 (81.41%) | 396 (81.99%) | 358 (80.81%) | 170 (76.23%) | 115 (72.78%) | |
| Low adhesion adenocarcinoma | 347 (13.36%) | 187 (14.48%) | 51 (10.56%) | 50 (11.51%) | 32 (14.35%) | 27 (17.09%) | |
| Mucoid adenocarcinoma | 120 (4.62%) | 50 (3.87%) | 21 (4.35%) | 24 (5.42%) | 16 (7.17%) | 9 (5.70%) | |
| Signet-ring cell carcinoma | 41 (1.57%) | 3 (0.24%) | 15 (3.10%) | 11 (2.48%) | 5 (2.24%) | 7 (4.43%) | |
| Differentiation degree, n (%) | <0.001 | ||||||
| G1 | 221 (8.51%) | 144 (11.15%) | 37 (7.66%) | 23 (5.19%) | 11 (4.93%) | 6 (3.80%) | |
| G2 | 1325 (51.00%) | 740 (57.32%) | 223 (46.17%) | 212 (47.86%) | 101 (45.29%) | 49 (31.01%) | |
| G3 | 1052 (40.49%) | 407 (31.53%) | 223 (46.17%) | 208 (46.95%) | 111 (49.78%) | 103 (65.19%) | |
| HER-2, n (%) | 0.028 | ||||||
| 0 | 1303 (50.15%) | 686 (53.14%) | 241 (49.90%) | 197 (44.47%) | 109 (48.88%) | 70 (44.30%) | |
| 1+ | 758 (29.18%) | 364 (28.20%) | 136 (28.16%) | 136 (30.70%) | 67 (30.04%) | 55 (34.81%) | |
| 2+ | 356 (13.70%) | 172 (13.32%) | 71 (14.70%) | 67 (15.12%) | 28 (12.56%) | 18 (11.39%) | |
| 3+ | 181 (6.97%) | 69 (5.34%) | 35 (7.24%) | 43 (9.71%) | 19 (8.52%) | 15 (9.50%) |
| Characteristics | Patients, n (%) | 2016-hN0, n (%) | 2016-hN1, n (%) | 2016-hN2, n (%) | 2016-hN3a, n (%) | 2016-hN3b, n (%) | p |
|---|---|---|---|---|---|---|---|
| n | 756 | 380 (50.26%) | 104 (13.76%) | 145 (19.18%) | 57 (7.54%) | 70 (9.26%) | |
| Age, Mean ± SD | 59.10 ± 9.82 | 58.53 ± 9.99 | 60.34 ± 9.90 | 59.23 ± 9.81 | 60.46 ± 9.09 | 58.93 ± 9.40 | 0.398 |
| BMI, Mean ± SD | 23.01 ± 3.27 | 22.24 ± 3.06 | 23.36 ± 3.88 | 22.79 ± 3.27 | 23.18 ± 3.09 | 21.57 ± 3.17 | 0.001 |
| CEA, Mean ± SD | 4.80 ± 15.49 | 3.53 ± 12.36 | 3.66 ± 7.91 | 5.84 ± 11.78 | 5.54 ± 17.02 | 10.62 ± 33.42 | 0.022 |
| CA-199, Mean ± SD | 32.31 ± 112.96 | 18.65 ± 68.42 | 12.90 ± 54.05 | 45.01 ± 148.12 | 53.48 ± 147.16 | 75.23 ± 205.81 | 0.021 |
| RLNs, Mean ± SD | 28.10 ± 11.30 | 26.43 ± 11.15 | 27.40 ± 11.38 | 28.92 ± 10.32 | 28.75 ± 11.26 | 36.00 ± 10.73 | <0.001 |
| MLNs, Mean ± SD | 3.63 ± 6.02 | 0 | 1.96 ± 1.54 | 6.05 ± 3.98 | 7.02 ± 1.91 | 18.01 ± 7.00 | <0.001 |
| LNRs, Mean ± SD | 0.12 ± 0.19 | 0 | 0.09 ± 0.08 | 0.22 ± 0.15 | 0.27 ± 0.11 | 0.52 ± 0.17 | <0.001 |
| Age, n (%) | 0.859 | ||||||
| ≤60 | 405 (53.57%) | 208 (54.74%) | 55 (52.88%) | 76 (52.41%) | 27 (47.37%) | 39 (55.71%) | |
| >60 | 351 (46.43%) | 172 (45.26%) | 49 (47.12%) | 69 (47.59%) | 30 (52.63%) | 31 (44.29%) | |
| Gender, n (%) | 0.325 | ||||||
| Male | 535 (70.77%) | 268 (70.53%) | 74 (71.15%) | 98 (67.59%) | 47 (82.46%) | 48 (68.57%) | |
| Female | 221 (29.23%) | 112 (29.47%) | 30 (28.85%) | 47 (32.41%) | 10 (17.54%) | 22 (31.43%) | |
| Tumor location, n (%) | <0.001 | ||||||
| L | 529 (69.97%) | 280 (73.68%) | 75 (72.12%) | 103 (71.03%) | 39 (68.42%) | 32 (45.71%) | |
| M | 127 (16.80%) | 64 (16.84%) | 16 (15.38%) | 22 (15.17%) | 8 (14.04%) | 17 (24.29%) | |
| U | 85 (11.24%) | 35 (9.21%) | 13 (12.50%) | 15 (10.35%) | 10 (17.54%) | 12 (17.14%) | |
| LMU | 15 (1.99%) | 1 (0.27%) | 0 (0%) | 5 (3.45%) | 0 (0%) | 9 (12.86%) | |
| T stage, n (%) | <0.001 | ||||||
| T1 | 198 (26.19%) | 173 (45.53%) | 16 (15.38%) | 7 (4.83%) | 1 (1.75%) | 1 (1.43%) | |
| T2 | 110 (14.55%) | 80 (21.05%) | 11 (10.58%) | 13 (8.97%) | 5 (8.77%) | 1 (1.43%) | |
| T3 | 317 (41.93%) | 93 (24.47%) | 60 (57.69%) | 87 (60.00%) | 35 (61.40%) | 42 (60.00%) | |
| T4 | 131 (17.33%) | 34 (8.95%) | 17 (16.35%) | 38 (26.20%) | 16 (27.08%) | 26 (37.14%) | |
| TNM stage, n (%) | <0.001 | ||||||
| I | 269 (35.58%) | 253 (66.58%) | 16 (15.38%) | 0 (%) | 0 (0%) | 0 (0%) | |
| II | 215 (28.44%) | 123 (32.37%) | 71 (68.27%) | 20 (13.79%) | 1 (1.75%) | 0 (0%) | |
| III | 272 (35.98%) | 4 (1.05%) | 17 (16.35%) | 125 (86.21%) | 56 (98.25%) | 70 (100%) | |
| Histological type, n (%) | 0.045 | ||||||
| Adenocarcinoma | 589 (77.91%) | 310 (81.58%) | 82 (78.85%) | 111 (76.55%) | 42 (73.68%) | 44 (62.86%) | |
| Low adhesion adenocarcinoma | 113 (14.95%) | 48 (12.63%) | 15 (14.42%) | 21(14.48%) | 9 (15.79%) | 20 (28.57%) | |
| Mucoid adenocarcinoma | 31 (4.10%) | 14 (3.68%) | 4 (3.85%) | 8 (5.52%) | 4 (7.02%) | 1 (1.43%) | |
| Signet-ring cell carcinoma | 23 (3.04%) | 8 (2.11%) | 3 (2.88%) | 5 (3.45%) | 2 (3.51%) | 5 (7.14%) | |
| Differentiation degree, n (%) | <0.001 | ||||||
| G1 | 77 (10.19%) | 60 (15.79%) | 9 (8.65%) | 6 (4.14%) | 1 (1.75%) | 1 (1.43%) | |
| G2 | 411 (54.37%) | 212 (55.79%) | 44 (42.31%) | 96 (66.21%) | 26 (45.61%) | 33 (47.14%) | |
| G3 | 268 (35.44%) | 108 (28.42%) | 51 (49.04%) | 43 (29.65%) | 30 (52.64%) | 36 (51.43%) | |
| HER-2, n (%) | 0.384 | ||||||
| 0 | 469 (62.04%) | 242 (63.68%) | 61 (58.65%) | 86 (59.31%) | 33 (57.89%) | 47 (67.14%) | |
| 1+ | 168 (22.22%) | 87 (22.89%) | 24 (23.08%) | 33 (22.76%) | 10 (17.54%) | 14 (20.00%) | |
| 2+ | 78 (10.32%) | 36 (9.47%) | 9 (8.65%) | 16 (11.03%) | 11 (19.30%) | 6 (8.57%) | |
| 3+ | 41 (5.42%) | 15 (3.96%) | 10 (9.62%) | 10 (6.90%) | 3 (5.27%) | 3 (4.29%) |
| (a) | ||||
|---|---|---|---|---|
| N | G1 | G2 | G3 | |
| hN | 0.718 | 0.683 | 0.750 | |
| pN | 0.712 | 0.671 | 0.737 | |
| (b) | ||||
| N | T1 | T2 | T3 | T4 |
| hN | 0.550 | 0.703 | 0.742 | 0.674 |
| pN | 0.531 | 0.648 | 0.689 | 0.660 |
| (c) | ||||
| N | I | II | III | |
| hN | 0.520 | 0.623 | 0.621 | |
| pN | 0.520 | 0.611 | 0.606 | |
| Characteristics | Total (N) | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| Hazard Ratio (95%CI) | p Value | Hazard Ratio (95%CI) | p Value | ||
| BMI | 3354 | 0.934 (0.915–0.954) | <0.001 | 0.971 (0.950–0.991) | 0.006 |
| CEA | 3354 | 1.003 (1.002–1.004) | <0.001 | 1.002 (1.001–1.003) | 0.002 |
| CA-199 | 3354 | 1.002 (1.002–1.002) | <0.001 | 1.001 (1.000–1.001) | <0.001 |
| MLNs | 3354 | 1.075 (1.070–1.080) | <0.001 | 1.017 (0.994–1.041) | 0.149 |
| RLNs | 3354 | 1.018 (1.013–1.023) | <0.001 | 0.991 (0.982–0.999) | 0.030 |
| LNRS | 3354 | 13.647 (11.711–15.902) | <0.001 | 0.907 (0.388–2.122) | 0.822 |
| Tumor size | 3354 | 1.019 (1.017–1.021) | <0.001 | 1.002 (0.999–1.005) | 0.131 |
| Age | 3354 | ||||
| ≤60 | 1899 | Reference | |||
| >60 | 1455 | 1.714 (1.505–1.952) | <0.001 | 1.195 (1.002–1.425) | 0.048 |
| Gender | 3354 | ||||
| Male | 2444 | Reference | |||
| Female | 910 | 0.868 (0.747–1.009) | 0.065 | 1.000 (0.857–1.166) | 0.998 |
| Tumor location | 3354 | ||||
| L | 2419 | Reference | |||
| M | 530 | 1.266 (1.063–1.507) | 0.008 | 1.081 (0.901–1.296) | 0.402 |
| U | 354 | 1.464 (1.205–1.780) | <0.001 | 1.320 (1.078–1.615) | 0.007 |
| LMU | 51 | 3.554 (2.447–5.162) | <0.001 | 0.945 (0.617–1.447) | 0.794 |
| hN | 3354 | ||||
| hN0 | 1671 | Reference | |||
| hN1 | 587 | 1.359 (1.067–1.731) | 0.013 | 0.612 (0.443–0.846) | 0.003 |
| hN2 | 588 | 4.516 (3.759–5.426) | <0.001 | 1.402 (0.945–2.078) | 0.093 |
| hN3a | 280 | 6.890 (5.615–8.453) | <0.001 | 1.854 (1.210–2.843) | 0.005 |
| hN3b | 228 | 16.234 (13.295–19.823) | <0.001 | 3.400 (2.051–5.637) | <0.001 |
| pT stage | 3354 | ||||
| T1 | 854 | Reference | |||
| T2 | 527 | 2.822 (1.922–4.146) | <0.001 | 2.055 (1.339–3.153) | <0.001 |
| T3 | 1218 | 7.811 (5.658–10.784) | <0.001 | 2.619 (1.509–4.546) | <0.001 |
| T4 | 755 | 16.426 (11.921–22.633) | <0.001 | 4.643 (2.635–8.179) | <0.001 |
| hTNM | 3354 | ||||
| I | 1154 | Reference | |||
| II | 1029 | 2.958 (2.255–3.881) | <0.001 | 1.285 (0.783–2.107) | 0.321 |
| III | 1171 | 13.411 (10.526–17.085) | <0.001 | 2.483 (1.249–4.935) | 0.009 |
| Histological type | 3354 | ||||
| Adenocarcinoma | 2679 | Reference | |||
| Low adhesion adenocarcinoma | 460 | 1.367 (1.144–1.633) | <0.001 | 1.547 (1.283–1.866) | <0.001 |
| mucoid adenocarcinoma | 151 | 1.598 (1.220–2.094) | <0.001 | 1.176 (0.892–1.548) | 0.250 |
| Signet-ring cell carcinoma | 64 | 2.610 (1.840–3.701) | <0.001 | 1.565 (1.094–2.239) | 0.014 |
| Differentiation | 3354 | ||||
| G1 | 298 | Reference | |||
| G2 | 1736 | 1.546 (1.151–2.078) | 0.004 | 0.890 (0.659–1.202) | 0.448 |
| G3 | 1320 | 2.223 (1.655–2.987) | <0.001 | 1.009 (0.744–1.369) | 0.953 |
| HER-2 | 3354 | ||||
| 0 | 1772 | Reference | |||
| 1+ | 926 | 1.002 (0.859–1.168) | 0.981 | ||
| 2+ | 434 | 1.042 (0.854–1.271) | 0.688 | ||
| 3+ | 222 | 1.274 (0.996–1.630) | 0.054 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, J.; Wang, H.; Yin, X.; Wang, X.; Wang, Y.; Lu, Z.; Zhang, J.; Zhang, Y.; Xue, Y. Efficacy of Lymph Node Location-Number Hybrid Staging System on the Prognosis of Gastric Cancer Patients. Cancers 2023, 15, 2659. https://doi.org/10.3390/cancers15092659
Wu J, Wang H, Yin X, Wang X, Wang Y, Lu Z, Zhang J, Zhang Y, Xue Y. Efficacy of Lymph Node Location-Number Hybrid Staging System on the Prognosis of Gastric Cancer Patients. Cancers. 2023; 15(9):2659. https://doi.org/10.3390/cancers15092659
Chicago/Turabian StyleWu, Junpeng, Hao Wang, Xin Yin, Xibo Wang, Yufei Wang, Zhanfei Lu, Jiaqi Zhang, Yao Zhang, and Yingwei Xue. 2023. "Efficacy of Lymph Node Location-Number Hybrid Staging System on the Prognosis of Gastric Cancer Patients" Cancers 15, no. 9: 2659. https://doi.org/10.3390/cancers15092659