
Effect on Germline Mutation Rate in a High-Risk Chinese Breast Cancer Cohort after Compliance with The National Comprehensive Cancer Network (NCCN) 2023 v.1 Testing Criteria
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Selection Criteria
2.2. DNA Extraction and Sequencing
2.3. Variant Interpretation and Annotation
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics of the Cohorts
3.2. NCCN Testing Guideline 2022 v.2 vs. 2023 v.1
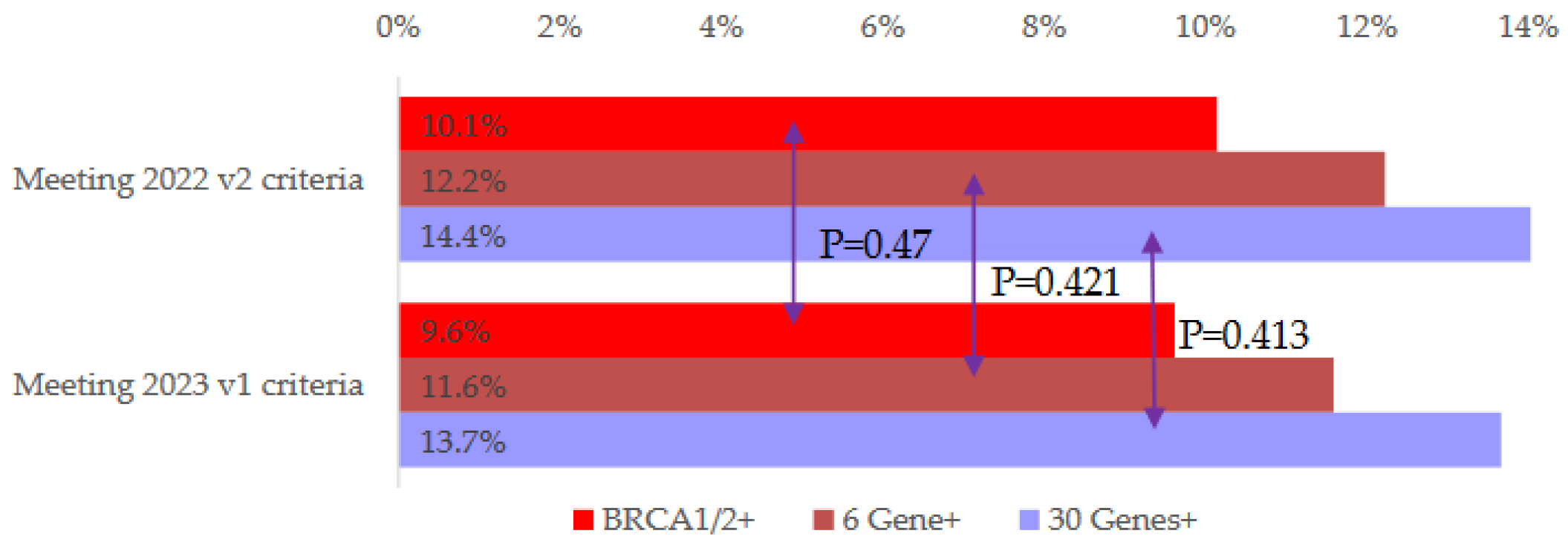
3.3. Germline Mutation Detection Rate
3.4. Patients who Met 2023 v.1 Criteria Only
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fearon, E.R.; Vogelstein, B. A genetic model for colorectal tumorigenesis. Cell 1990, 61, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Vogelstein, B.; Kinzler, K.W. The multistep nature of cancer. Trends Genet. 1993, 9, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Espinel, W.; Champine, M.; Hampel, H.; Jeter, J.; Sweet, K.; Pilarski, R.; Pearlman, R.; Shane, K.; Brock, P.; Westman, J.A.; et al. Clinical Impact of Pathogenic Variants in DNA Damage Repair Genes beyond BRCA1 and BRCA2 in Breast and Ovarian Cancer Patients. Cancers 2022, 14, 2426. [Google Scholar] [CrossRef] [PubMed]
- Brandão, A.; Paulo, P.; Teixeira, M.R. Hereditary Predisposition to Prostate Cancer: From Genetics to Clinical Implications. Int. J. Mol. Sci. 2020, 21, 5036. [Google Scholar] [CrossRef] [PubMed]
- Paduano, F.; Colao, E.; Fabiani, F.; Rocca, V.; Dinatolo, F.; Dattola, A.; D’antona, L.; Amato, R.; Trapasso, F.; Baudi, F.; et al. Germline Testing in a Cohort of Patients at High Risk of Hereditary Cancer Predisposition Syndromes: First Two-Year Results from South Italy. Genes 2022, 13, 1286. [Google Scholar] [CrossRef] [PubMed]
- Graffeo, R.; Rana, H.; Conforti, F.; Bonanni, B.; Cardoso, M.; Paluch-Shimon, S.; Pagani, O.; Goldhirsch, A.; Partridge, A.; Lambertini, M.; et al. Moderate penetrance genes complicate genetic testing for breast cancer diagnosis: ATM, CHEK2, BARD1 and RAD51D. Breast 2022, 65, 32–40. [Google Scholar] [CrossRef]
- Jung, K.; Lee, S.; Na, H.Y.; Kim, J.-W.; Lee, J.-C.; Hwang, J.-H.; Kim, J. NGS-based targeted gene mutational profiles in Korean patients with pancreatic cancer. Sci. Rep. 2022, 12, 20937. [Google Scholar] [CrossRef]
- Kwong, A.; Shin, V.Y.; Chen, J.; Cheuk, I.W.-Y.; Ho, C.Y.; Au, C.H.; Chan, K.K.; Ngan, H.Y.S.; Chan, T.L.; Ford, J.M.; et al. Germline Mutation in 1338 BRCA-Negative Chinese Hereditary Breast and/or Ovarian Cancer Patients: Clinical Testing with a Multigene Test Panel. J. Mol. Diagn. 2020, 22, 544–554. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Genetic/Familial High-Risk Assessment: Breast and Ovarian; Version 2.2022; NCCN: Plymouth Meeting, PA, USA, 2022. [Google Scholar]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Genetic/Familial High-Risk Assessment: Breast and Ovarian; Version 1.2023; NCCN: Plymouth Meeting, PA, USA, 2023. [Google Scholar]
- Andoni, T.; Wiggins, J.; Robinson, R.; Charlton, R.; Sandberg, M.; Eeles, R. Half of germline pathogenic and likely pathogenic variants found on panel tests do not fulfil NHS testing criteria. Sci. Rep. 2022, 12, 2507. [Google Scholar] [CrossRef]
- King, M.-C.; Levy-Lahad, E.; Lahad, A. Population-Based Screening for BRCA1 and BRCA2: 2014 Lasker Award. JAMA 2014, 312, 1091–1092. [Google Scholar] [CrossRef]
- Pal, T.; Agnese, D.; Daly, M.; La Spada, A.; Litton, J.; Wick, M.; Klugman, S.; Esplin, E.D.; Jarvik, G.P.; Professional Practice and Guidelines Committee. Points to consider: Is there evidence to support BRCA1/2 and other inherited breast cancer genetic testing for all breast cancer patients? A statement of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2020, 22, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Manahan, E.R.; Kuerer, H.M.; Sebastian, M.; Hughes, K.S.; Boughey, J.C.; Euhus, D.M.; Boolbol, S.K.; Taylor, W.A. Consensus Guidelines on Genetic‘ Testing for Hereditary Breast Cancer from the American Society of Breast Surgeons. Ann. Surg. Oncol. 2019, 26, 3025–3031. [Google Scholar] [CrossRef] [PubMed]
- Kwong, A.; Shin, V.Y.; Au, C.H.; Law, F.B.; Ho, D.N.; Ip, B.K.; Wong, A.T.; Lau, S.S.; To, R.M.; Choy, G.; et al. Detection of Germline Mutation in Hereditary Breast and/or Ovarian Cancers by Next-Generation Sequencing on a Four-Gene Panel. J. Mol. Diagn. 2016, 18, 580–594. [Google Scholar] [CrossRef]
- Manickam, K.; Buchanan, A.H.; Schwartz, M.L.B.; Hallquist, M.L.G.; Williams, J.L.; Rahm, A.K.; Rocha, H.; Savatt, J.M.; Evans, A.E.; Butry, L.M.; et al. Exome Sequencing–Based Screening for BRCA1/2 Expected Pathogenic Variants Among Adult Biobank Participants. JAMA Netw. Open 2018, 1, e182140. [Google Scholar] [CrossRef]
- 1000 Genomes Project Consortium; Auton, A.; Brooks, L.D.; Durbin, R.M.; Garrison, E.P.; Kang, H.M.; Korbel, J.O.; Marchini, J.L.; McCarthy, S.; McVean, G.A.; et al. A global reference for human genetic variation. Nature 2015, 526, 68–74. [Google Scholar] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 1 February 2023).
- Beitsch, P.D.; Whitworth, P.W.; Hughes, K.; Patel, R.; Rosen, B.; Compagnoni, G.; Baron, P.; Simmons, R.; Smith, L.A.; Grady, I.; et al. Underdiagnosis of Hereditary Breast Cancer: Are Genetic Testing Guidelines a Tool or an Obstacle? J. Clin. Oncol. 2019, 37, 453–460. [Google Scholar] [CrossRef]
- Buys, S.S.; Sandbach, J.F.; Gammon, A.; Patel, G.; Kidd, J.; Brown, K.L.; Sharma, L.; Saam, J.; Lancaster, J.; Daly, M.B. A study of over 35,000 women with breast cancer tested with a 25-gene panel of hereditary cancer genes. Cancer 2017, 123, 1721–1730. [Google Scholar] [CrossRef]
- Susswein, L.R.; Marshall, M.L.; Nusbaum, R.; Postula, K.J.V.; Weissman, S.M.; Yackowski, L.; Vaccari, E.M.; Bissonnette, J.; Booker, J.K.; Cremona, M.L.; et al. Pathogenic and likely pathogenic variant prevalence among the first 10,000 patients referred for next-generation cancer panel testing. Genet. Med. 2016, 18, 823–832. [Google Scholar] [CrossRef]
- Kurian, A.W.; Bernhisel, R.; Larson, K.; Caswell-Jin, J.; Shadyab, A.H.; Ochs-Balcom, H.; Stefanick, M.L. Prevalence of Pathogenic Variants in Cancer Susceptibility Genes Among Women With Postmenopausal Breast Cancer. JAMA 2020, 323, 995–997. [Google Scholar] [CrossRef]
- Chavarri-Guerra, Y.; Hendricks, C.B.; Brown, S.; Marcum, C.; Hander, M.; Segota, Z.E.; Hake, C.; Sand, S.; Slavin, T.P.; Hurria, A.; et al. The Burden of Breast Cancer Predisposition Variants across the Age Spectrum among 10,000 Patients. J. Am. Geriatr. Soc. 2019, 67, 884–888. [Google Scholar] [CrossRef]
- Yadav, S.; Hu, C.; Hart, S.N.; Boddicker, N.; Polley, E.C.; Na, J.; Gnanaolivu, R.; Lee, K.Y.; Lindstrom, T.; Armasu, S.; et al. Evaluation of Germline Genetic Testing Criteria in a Hospital-Based Series of Women With Breast Cancer. J. Clin. Oncol. 2020, 38, 1409–1418. [Google Scholar] [CrossRef]
- Samadder, N.J.; Riegert-Johnson, D.; Boardman, L.; Rhodes, D.; Wick, M.; Okuno, S.; Kunze, K.L.; Golafshar, M.; Uson, P.L.S.; Mountjoy, L.; et al. Comparison of Universal Genetic Testing vs Guideline-Directed Targeted Testing for Patients With Hereditary Cancer Syndrome. JAMA Oncol. 2021, 7, 230–237. [Google Scholar] [CrossRef]
- Stanislaw, C.; Xue, Y.; Wilcox, W.R. Genetic evaluation and testing for hereditary forms of cancer in the era of next-generation sequencing. Cancer Biol. Med. 2016, 13, 55–67. [Google Scholar] [CrossRef]
- Burke, W. Genetic Tests: Clinical Validity and Clinical Utility. Curr. Protoc. Hum. Genet. 2014, 81, 9.15.1–9.15.8. [Google Scholar] [CrossRef] [PubMed]
- Weber-Lassalle, N.; Hauke, J.; Ramser, J.; Richters, L.; Groß, E.; Blümcke, B.; Gehrig, A.; Kahlert, A.-K.; Müller, C.R.; Hackmann, K.; et al. BRIP1 loss-of-function mutations confer high risk for familial ovarian cancer, but not familial breast cancer. Breast Cancer Res. 2018, 20, 7. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Hart, S.N.; Gnanaolivu, R.; Huang, H.; Lee, K.Y.; Na, J.; Gao, C.; Lilyquist, J.; Yadav, S.; Boddicker, N.J.; et al. A Population-Based Study of Genes Previously Implicated in Breast Cancer. N. Engl. J. Med. 2021, 384, 440–451. [Google Scholar] [CrossRef]
- Hall, M.J.; Forman, A.D.; Pilarski, R.; Wiesner, G.; Giri, V.N. Gene Panel Testing for Inherited Cancer Risk. J. Natl. Compr. Cancer Netw. 2014, 12, 1339–1346. [Google Scholar] [CrossRef]
- Fanale, D.; Incorvaia, L.; Filorizzo, C.; Bono, M.; Fiorino, A.; Calò, V.; Brando, C.; Corsini, L.R.; Barraco, N.; Badalamenti, G.; et al. Detection of Germline Mutations in a Cohort of 139 Patients with Bilateral Breast Cancer by Multi-Gene Panel Testing: Impact of Pathogenic Variants in Other Genes beyond BRCA1/2. Cancers 2020, 12, 2415. [Google Scholar] [CrossRef]
- Fu, E.A.F.; Zhang, D.; Hu, L.; Sundaram, S.; Ying, D.; Zhang, Y.; Fu, S.; Zhang, J.; Yao, L.; Xu, Y.; et al. Association between 15 known or potential breast cancer susceptibility genes and breast cancer risks in Chinese women. Cancer Biol. Med. 2021, 19, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Desai, N.V.; Yadav, S.; Batalini, F.; Couch, F.J.; Tung, N.M. Germline genetic testing in breast cancer: Rationale for the testing of all women diagnosed by the age of 60 years and for risk-based testing of those older than 60 years. Cancer 2021, 127, 828–833. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n = 3797 | % | ||
|---|---|---|---|
| Sex | F | 3713 | 97.8% |
| M | 84 | 2.2% | |
| First diagnosis age | Mean | 45.5 | (SD) 11.5 |
| Median | 44 | (Range) 18–95 | |
| Personal multiple cancers | 305 | 8.0% | |
| Bilateral breast | 747 | 19.7% | |
| Pathology (primary tumors = 4544) | |||
| Histology | Ductal | 3212 | 72.7% |
| In situ | 721 | 16.3% | |
| Others | 485 | 11.0% | |
| NS | 126 | ||
| Stage | 0 | 775 | 18.1% |
| I | 1573 | 36.8% | |
| II | 1307 | 30.5% | |
| III | 471 | 11.0% | |
| IV | 154 | 3.6% | |
| Not stated | 264 | ||
| Grade (invasive) | 1 | 564 | 17.9% |
| 2 | 1437 | 45.7% | |
| 3 | 1146 | 36.4% | |
| Not stated | 676 | ||
| Breast cancer subtype | Luminal type | 2699 | 75.5% |
| TNBC | 573 | 15.8% | |
| HER2+ | 305 | 8.5% | |
| Not stated | 246 | ||
| Family history in 1st–3rd degrees | Breast cancer | 1655 | 43.6% |
| Ovarian cancer | 202 | 5.3% | |
| Prostate cancer | 201 | 5.3% | |
| Pancreatic cancer | 186 | 4.9% | |
| Proband’s Breast Cancer Diagnosis Age | |||
|---|---|---|---|
| Testing Criteria | 2022 v2 | 2023 v1 | |
| Personal breast cancer | Diagnosis age | ≤45 y | ≤50 y |
| Multiple primary breast cancers (Synchronous or metachronous) | 46–50 y | Any age | |
| Family history (≥1 close relative ^ with) | Breast cancer at any age | 46–50 y | - |
| Breast cancer at age ≤50 y | ≥51 y | Any age | |
| Male breast cancer at any age | ≥51 y | Any age | |
| Ovarian, pancreatic, or metastatic/high-risk group of prostate cancer at any age | 46–50 y | Any age | |
| Family history (≥2 close relative ^ with) | Breast or prostate cancer at any age | ≥51 y | Any age |
| Family history (≥3 in patient and/or close relative ^ with) | Breast cancer at any age | ≥51 y | Any age |
| Mutation Positive | Negative | Grand Total | |||
|---|---|---|---|---|---|
| BRCA1/2+ | 6 Gene+ | 30 Genes+ | |||
| Total recruited probands | 361 (9.5%) | 435 (11.5%) | 514 (13.5%) | 3283 | 3797 |
| Meeting 2022 v2 criteria | 351 (10.1%) | 423 (12.2%) | 497 (14.4%) | 2964 | 3461 (91.2%) |
| Meeting 2023 v1 criteria | 356 (9.6%) | 429 (11.6%) | 506 (13.7%) | 3197 | 3703 (97.5%) |
| Meeting 2023 v1 criteria only but not 2022 v.2 | 5 (2.1%) | 6 (2.5%) | 9 (3.7%) | 233 | 242 (6.4%) |
| Not meeting both criteria | 5 (5.3%) | 6 (6.4%) | 8 (8.5%) | 86 | 94 (2.5%) |
| Mutation Positive | Negative | Total | p-Value (30 Genes + vs. Negative) | ||||
|---|---|---|---|---|---|---|---|
| BRCA1/2+ | 6 Gene+ | 30 Genes+ | |||||
| n = 5 | n = 6 | n = 9 | n = 233 | n = 242 | |||
| Diagnosis age | Mean | 51.23 | 50.58 | 50.83 | 56.71 | 56.49 | 0.006 |
| Median | 50.56 | 49.3 | 48.03 | 53.97 | 53.65 | 0.058 | |
| Range | 48–56 | 47–56 | 46–59 | 46–84 | 46–84 | ||
| ≤50 | 3 (3.6%) | 4 (4.8%) | 6 (7.1%) | 78 (92.9%) | 84 (34.7%) | 0.0681 | |
| Bilateral | 2 (1.3%) | 2 (1.3%) | 3 (2%) | 147 (98%) | 150 (62%) | 0.0873 | |
| Histology | Ductal | 4 (1.6%) | 5 (2%) | 7 (2.8%) | 243 (97.2%) | 250 (63.8%) | 0.1066 |
| In situ | 1 (1.1%) | 1 (1.1%) | 3 (3.3%) | 88 (96.7%) | 91 (23.2%) | ||
| Others | 0 | 0 | 0 | 38 (100%) | 38 (9.7%) | ||
| Not stated | 2 | 2 | 2 | 11 | 13 (3.3%) | ||
| Breast cancer subtype | Luminal type | 6 (2.6%) | 7 (3%) | 9 (3.9%) | 223 (96.1%) | 232 (59.2%) | 0.5886 |
| TNBC | 0 | 0 | 0 | 6 (100%) | 6 (1.5%) | ||
| HER2+ | 0 | 0 | 0 | 46 (100%) | 46 (100%) | ||
| Not stated | 0 | 0 | 0 | 17 | 17 (4.3%) | ||
| Grade (invasive) | Low/intermediate | 2 (1.1%) | 2 (1.1%) | 4 (2.1%) | 183 (97.9%) | 187 (47.7%) | 0.3654 |
| High | 2 (3.3%) | 3 (5%) | 3 (5%) | 57 (95%) | 60 (15.3%) | ||
| Not stated | 2 | 3 | 2 | 52 | 54 (13.8%) | ||
| Stage of Breast | 0 | 1 (1%) | 1 (1%) | 3 (3.1%) | 93 (96.9%) | 96 (24.4%) | 0.8773 |
| I | 5 (4%) | 5 (4%) | 6 (4.8%) | 120 (95.2%) | 126 (32.1%) | ||
| II | 1 (1.1%) | 1 (1.1%) | 2 (2.2%) | 87 (97.8%) | 89 (22.7%) | ||
| III | 0 | 1 (2%) | 1 (2%) | 48 (98%) | 49 (12.5%) | ||
| IV | 0 | 0 | 0 | 12 (100%) | 12 (3.1%) | ||
| Not stated | 0 | 0 | 0 | 20 | 20 (5.1%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwong, A.; Ho, C.Y.S.; Luk, W.-P.; Fung, L.-H.; Au, C.-H.; Ma, E.S.K. Effect on Germline Mutation Rate in a High-Risk Chinese Breast Cancer Cohort after Compliance with The National Comprehensive Cancer Network (NCCN) 2023 v.1 Testing Criteria. Cancers 2023, 15, 2635. https://doi.org/10.3390/cancers15092635
Kwong A, Ho CYS, Luk W-P, Fung L-H, Au C-H, Ma ESK. Effect on Germline Mutation Rate in a High-Risk Chinese Breast Cancer Cohort after Compliance with The National Comprehensive Cancer Network (NCCN) 2023 v.1 Testing Criteria. Cancers. 2023; 15(9):2635. https://doi.org/10.3390/cancers15092635
Chicago/Turabian StyleKwong, Ava, Cecilia Y. S. Ho, Wing-Pan Luk, Ling-Hiu Fung, Chun-Hang Au, and Edmond S. K. Ma. 2023. "Effect on Germline Mutation Rate in a High-Risk Chinese Breast Cancer Cohort after Compliance with The National Comprehensive Cancer Network (NCCN) 2023 v.1 Testing Criteria" Cancers 15, no. 9: 2635. https://doi.org/10.3390/cancers15092635