
Incidence and Risk Factors for Extremity Osteoradionecrosis after Limb-Sparing Surgery and Adjuvant Radiotherapy
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
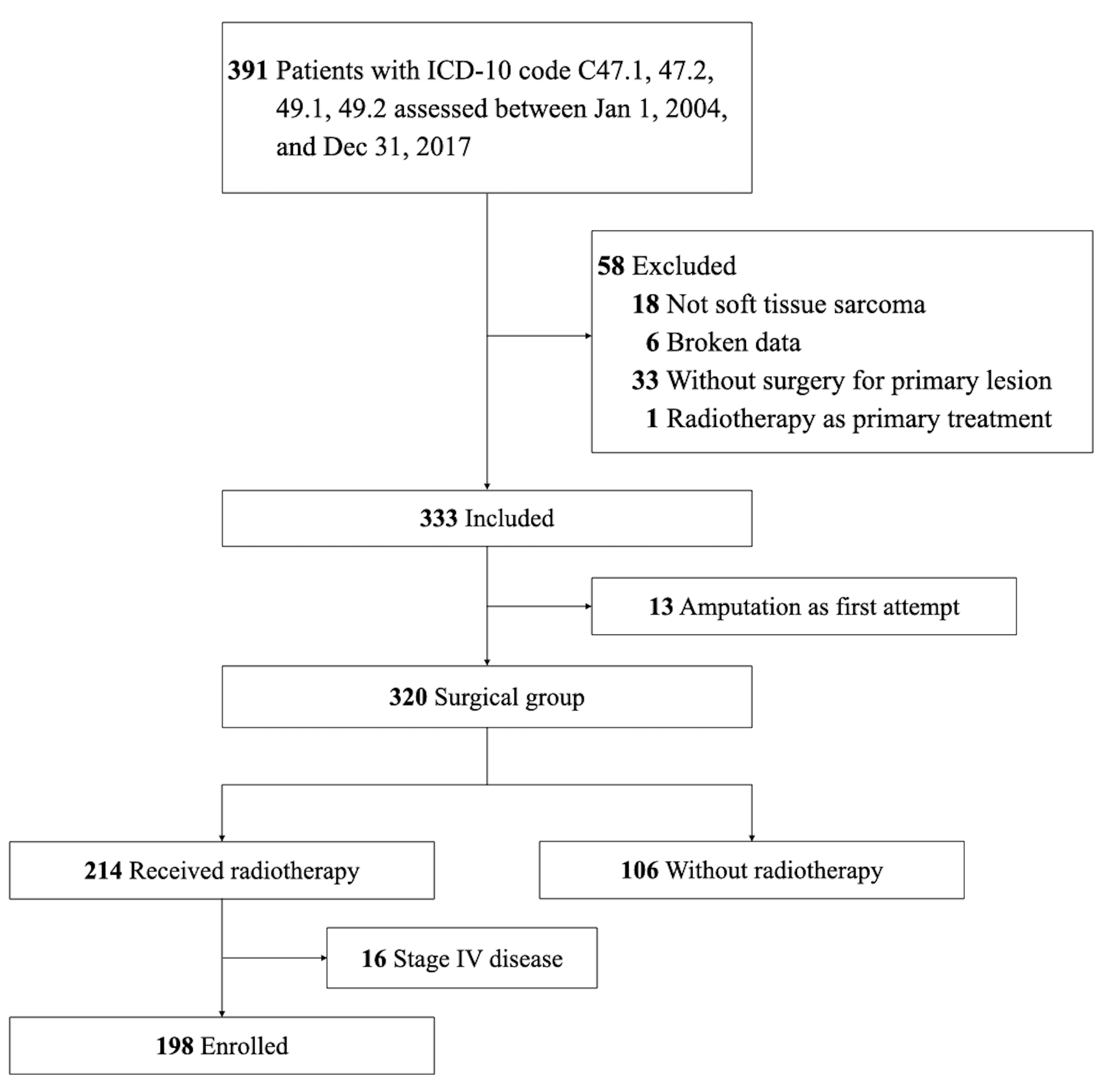
2. Materials and Methods
2.1. ORN Identification
2.2. Statistical Analysis
3. Results
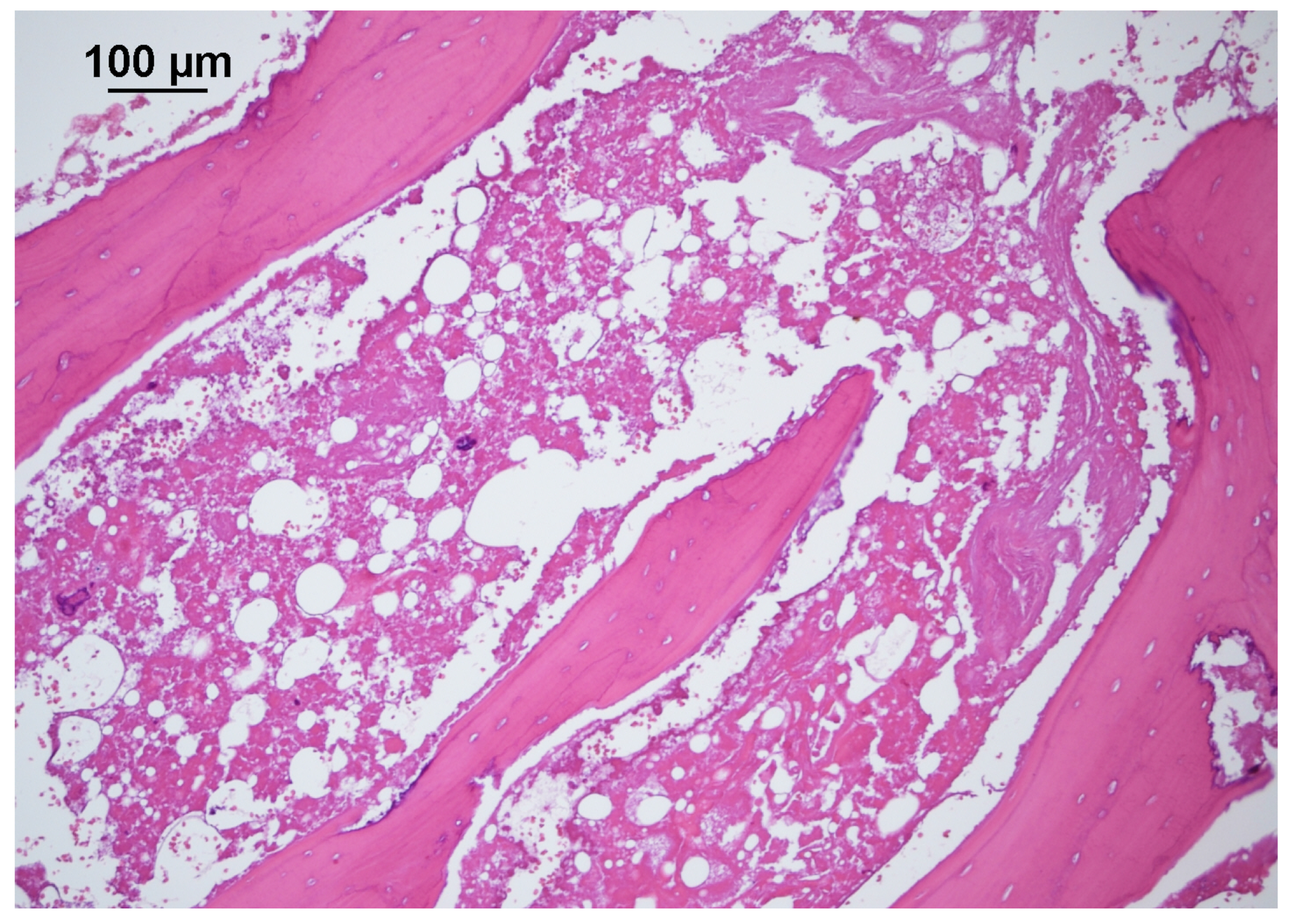
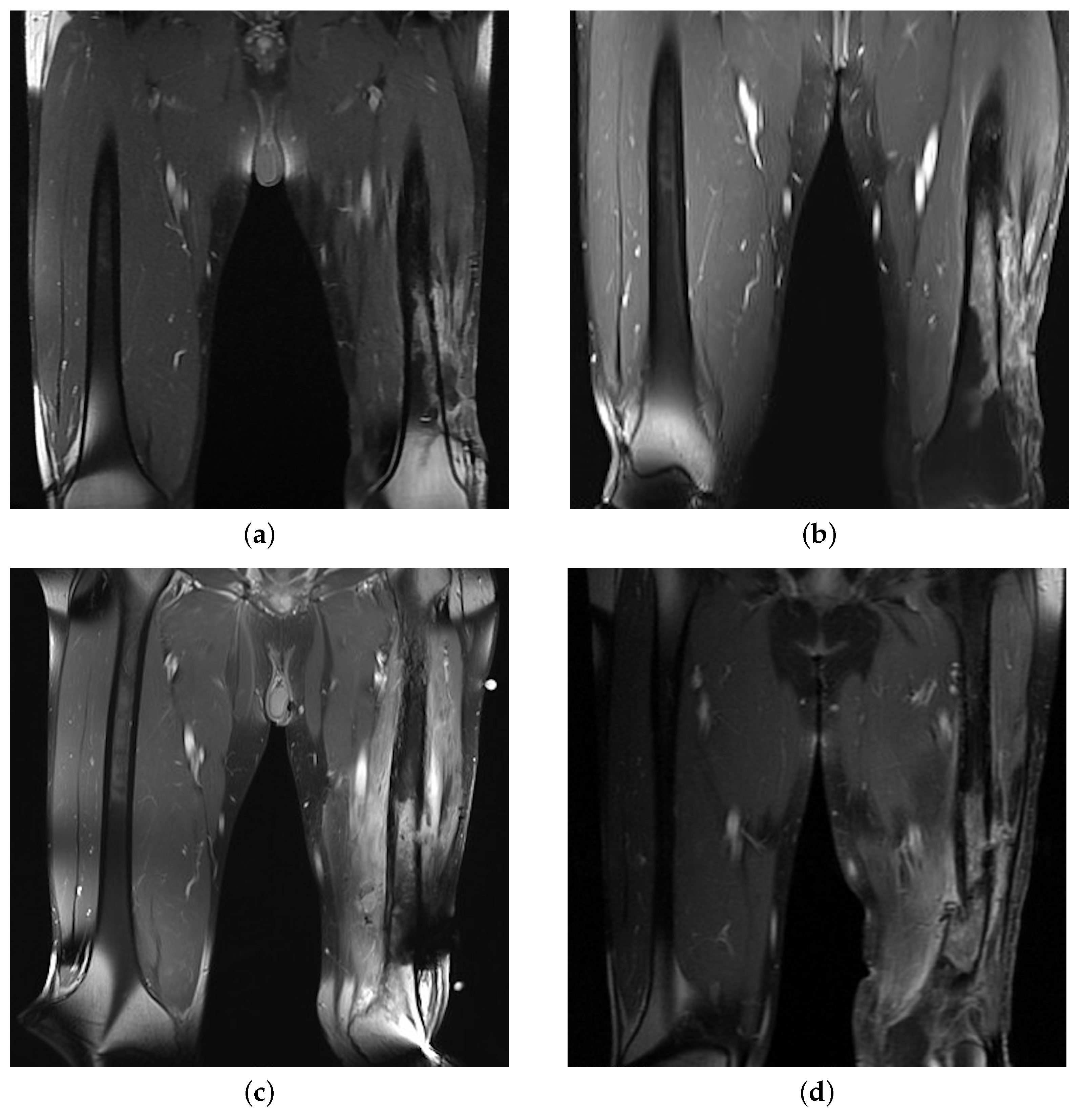
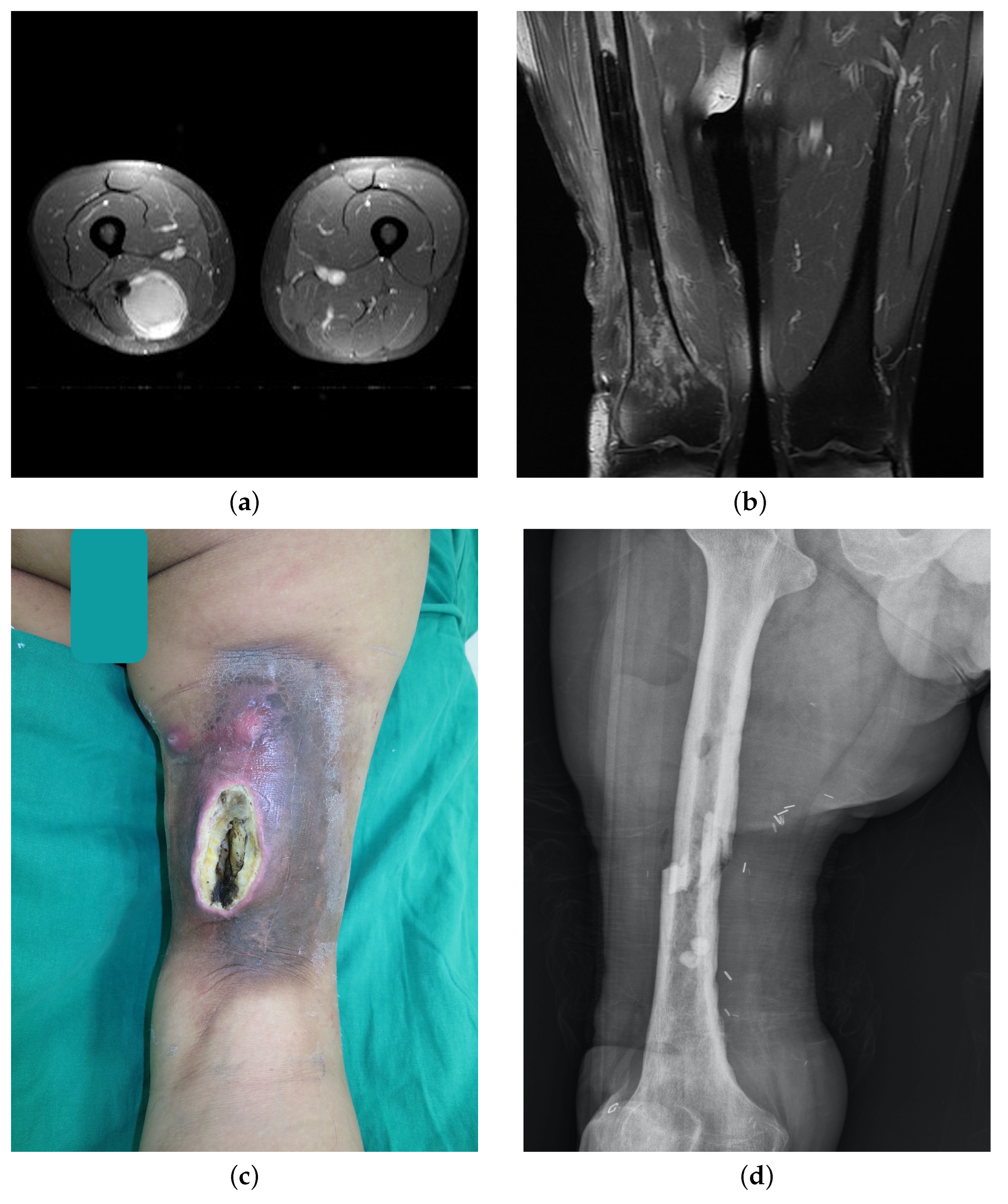
ORN Case Presentations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hung, G.Y.; Yen, C.C.; Horng, J.L.; Liu, C.Y.; Chen, W.M.; Chen, T.H.; Liu, C.L. Incidences of primary soft tissue sarcoma diagnosed on extremities and trunk wall: A population-based study in Taiwan. Medicine 2015, 94, e1696. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.; Bridge, J.; Hogendoorn, P.; Martens, F. Soft Tissue and Bone Tumours: WHO Classification of Tumours, 5th ed.; IARC Press: Lyon, France, 2020. [Google Scholar]
- Alektiar, K.M.; Brennan, M.F.; Healey, J.H.; Singer, S. Impact of intensity-modulated radiation therapy on local control in primary soft-tissue sarcoma of the extremity. J. Clin. Oncol. 2008, 26, 3440–3444. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Osteoradionecrosis: A new concept of its pathophysiology. J. Oral Maxillofac. Surg. 1983, 41, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Chronopoulos, A.; Zarra, T.; Ehrenfeld, M.; Otto, S. Osteoradionecrosis of the jaws: Definition, epidemiology, staging and clinical and radiological findings. A concise review. Int. Dent. J. 2018, 68, 22–30. [Google Scholar] [CrossRef]
- Edge, S.; Edge, S. American Joint Committee on C. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Choi, J.H.; Ro, J.Y. The 2020 WHO classification of tumors of soft tissue: Selected changes and new entities. Adv. Anat. Pathol. 2021, 28, 44–58. [Google Scholar] [CrossRef]
- Miyamoto, I.; Tanaka, R.; Kogi, S.; Yamaya, G.; Kawai, T.; Ohashi, Y.; Takahashi, N.; Izumisawa, M.; Yamada, H. Clinical Diagnostic Imaging Study of Osteoradionecrosis of the Jaw: A Retrospective Study. J. Clin. Med. 2021, 10, 4704. [Google Scholar] [CrossRef]
- Meixel, A.J.; Hauswald, H.; Delorme, S.; Jobke, B. From radiation osteitis to osteoradionecrosis: Incidence and MR morphology of radiation-induced sacral pathologies following pelvic radiotherapy. Eur. Radiol. 2018, 28, 3550–3559. [Google Scholar] [CrossRef]
- Deshpande, S.; Thakur, M.; Dholam, K.; Mahajan, A.; Arya, S.; Juvekar, S. Osteoradionecrosis of the mandible: Through a radiologist’s eyes. Clin. Radiol. 2015, 70, 197–205. [Google Scholar] [CrossRef]
- Marx, R.; Tursun, R. Suppurative osteomyelitis, bisphosphonate induced osteonecrosis, osteoradionecrosis: A blinded histopathologic comparison and its implications for the mechanism of each disease. Int. J. Oral Maxillofac. Surg. 2012, 41, 283–289. [Google Scholar] [CrossRef]
- Shuster, A.; Reiser, V.; Trejo, L.; Ianculovici, C.; Kleinman, S.; Kaplan, I. Comparison of the histopathological characteristics of osteomyelitis, medication-related osteonecrosis of the jaw, and osteoradionecrosis. Int. J. Oral Maxillofac. Surg. 2019, 48, 17–22. [Google Scholar] [CrossRef]
- Kammeijer, Q.; van Spronsen, E.; Mirck, P.G.; Dreschler, W.A. Treatment outcomes of temporal bone osteoradionecrosis. Otolaryngol. Head Neck Surg. 2015, 152, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Youn, D.G.; Hwang, K.T.; Kim, J.T.; Kim, Y.H. Reconstruction of severely infected gluteal osteoradionecrosis using negative-pressure wound therapy and latissimus dorsi musculocutaneous flaps. Microsurgery 2016, 36, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Raz, D.J.; Clancy, S.L.; Erhunmwunsee, L.J. Surgical management of the radiated chest wall and its complications. Thorac. Surg. Clin. 2017, 27, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Nadella, K.R.; Kodali, R.M.; Guttikonda, L.K.; Jonnalagadda, A. Osteoradionecrosis of the jaws: Clinico-therapeutic management: A literature review and update. J. Maxillofac. Oral Surg. 2015, 14, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Kuo, T.J.; Leung, C.M.; Chang, H.S.; Wu, C.N.; Chen, W.L.; Chen, G.J.; Lai, Y.C.; Huang, W.C. Jaw osteoradionecrosis and dental extraction after head and neck radiotherapy: A nationwide population-based retrospective study in Taiwan. Oral Oncol. 2016, 56, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Moon, D.H.; Moon, S.H.; Wang, K.; Weissler, M.C.; Hackman, T.G.; Zanation, A.M.; Thorp, B.D.; Patel, S.N.; Zevallos, J.P.; Marks, L.B.; et al. Incidence of, and risk factors for, mandibular osteoradionecrosis in patients with oral cavity and oropharynx cancers. Oral Oncol. 2017, 72, 98–103. [Google Scholar] [CrossRef]
- Owosho, A.A.; Tsai, C.J.; Lee, R.S.; Freymiller, H.; Kadempour, A.; Varthis, S.; Sax, A.Z.; Rosen, E.B.; Yom, S.K.; Randazzo, J.; et al. The prevalence and risk factors associated with osteoradionecrosis of the jaw in oral and oropharyngeal cancer patients treated with intensity-modulated radiation therapy (IMRT): The Memorial Sloan Kettering Cancer Center experience. Oral Oncol. 2017, 64, 44–51. [Google Scholar] [CrossRef]
- Mendenhall, W.M.; Suárez, C.; Genden, E.M.; de Bree, R.; Strojan, P.; Langendijk, J.A.; Mäkitie, A.A.; Smee, R.; Eisbruch, A.; Lee, A.W.; et al. Parameters associated with mandibular osteoradionecrosis. Am. J. Clin. Oncol. 2018, 41, 1276–1280. [Google Scholar] [CrossRef]
- Haas, R.L.; DeLaney, T.F.; O’Sullivan, B.; Keus, R.B.; Le Pechoux, C.; Olmi, P.; Poulsen, J.P.; Seddon, B.; Wang, D. Radiotherapy for management of extremity soft tissue sarcomas: Why, when, and where? Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 572–580. [Google Scholar] [CrossRef]
- Pisters, P.W.; O’Sullivan, B.; Maki, R.G. Evidence-based recommendations for local therapy for soft tissue sarcomas. J. Clin. Oncol. 2007, 25, 1003–1008. [Google Scholar] [CrossRef]
- Pisters, P.W.; Pollock, R.E.; Lewis, V.O.; Yasko, A.W.; Cormier, J.N.; Respondek, P.M.; Feig, B.W.; Hunt, K.K.; Lin, P.P.; Zagars, G.; et al. Long-term results of prospective trial of surgery alone with selective use of radiation for patients with T1 extremity and trunk soft tissue sarcomas. Ann. Surg. 2007, 246, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Pan, E.; Goldberg, S.I.; Chen, Y.L.; Giraud, C.; Hornick, J.L.; Nielsen, G.P.; Hornicek, F.J.; Raut, C.P.; DeLaney, T.F.; Baldini, E.H. Role of post-operative radiation boost for soft tissue sarcomas with positive margins following pre-operative radiation and surgery. J. Surg. Oncol. 2014, 110, 817–822. [Google Scholar] [CrossRef] [PubMed]
- DeLaney, T.F.; Kepka, L.; Goldberg, S.I.; Hornicek, F.J.; Gebhardt, M.C.; Yoon, S.S.; Springfield, D.S.; Raskin, K.A.; Harmon, D.C.; Kirsch, D.G.; et al. Radiation therapy for control of soft-tissue sarcomas resected with positive margins. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Holt, G.E.; Griffin, A.M.; Pintilie, M.; Wunder, J.S.; Catton, C.; O’Sullivan, B.; Bell, R.S. Fractures following radiotherapy and limb-salvage surgery for lower extremity soft-tissue sarcomas: A comparison of high-dose and low-dose radiotherapy. JBJS 2005, 87, 315–319. [Google Scholar] [CrossRef]
- Zagars, G.K.; Ballo, M.T.; Pisters, P.W.; Pollock, R.E.; Patel, S.R.; Benjamin, R.S. Surgical margins and reresection in the management of patients with soft tissue sarcoma using conservative surgery and radiation therapy. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2003, 97, 2544–2553. [Google Scholar] [CrossRef] [PubMed]
- Strander, H.; Turesson, I.; Cavallin-Ståhl, E. A systematic overview of radiation therapy effects in soft tissue sarcomas. Acta Oncol. 2003, 42, 516–531. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, R.; Jacobson, A.; Hornicek, F.; Haynes, A.B.; Choy, E.; Cote, G.; Nielsen, G.P.; Chen, Y.L.; DeLaney, T.F.; Mullen, J.T. The width of the surgical margin does not influence outcomes in extremity and truncal soft tissue sarcoma treated with radiotherapy. Oncologist 2016, 21, 1269–1276. [Google Scholar] [CrossRef]
- Lin, P.P.; Schupak, K.D.; Boland, P.J.; Brennan, M.F.; Healey, J.H. Pathologic femoral fracture after periosteal excision and radiation for the treatment of soft tissue sarcoma. Cancer Interdiscip. Int. J. Am. Cancer Soc. 1998, 82, 2356–2365. [Google Scholar] [CrossRef]
- Yuhan, B.T.; Nguyen, B.K.; Svider, P.F.; Raza, S.N.; Hotaling, J.; Chan, E.; Hong, R.S. Osteoradionecrosis of the temporal bone: An evidence-based approach. Otol. Neurotol. 2018, 39, 1172–1183. [Google Scholar] [CrossRef]
- Thorn, J.J.; Hansen, H.S.; Specht, L.; Bastholt, L. Osteoradionecrosis of the jaws: Clinical characteristics and relation to the field of irradiation. J. Oral Maxillofac. Surg. 2000, 58, 1088–1093. [Google Scholar] [CrossRef]
- Gortzak, Y.; Lockwood, G.A.; Mahendra, A.; Wang, Y.; Chung, P.W.; Catton, C.N.; O’Sullivan, B.; Deheshi, B.M.; Wunder, J.S.; Ferguson, P.C. Prediction of pathologic fracture risk of the femur after combined modality treatment of soft tissue sarcoma of the thigh. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2010, 116, 1553–1559. [Google Scholar] [CrossRef] [PubMed]
- Bartelstein, M.K.; Yerramilli, D.; Christ, A.B.; Kenan, S.; Ogura, K.; Fujiwara, T.; Fabbri, N.; Healey, J.H. Postradiation fractures after combined modality treatment in extremity soft tissue sarcomas. Sarcoma 2021, 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, S.K. Osteomyelitis. Infect. Dis. Clin. 2017, 31, 325–338. [Google Scholar] [CrossRef] [PubMed]
- Qaisi, M.; Montague, L. Bone margin analysis for osteonecrosis and osteomyelitis of the jaws. Oral Maxillofac. Surg. Clin. 2017, 29, 301–313. [Google Scholar] [CrossRef]
- Wortman, J.R.; Tirumani, S.H.; Jagannathan, J.P.; Rosenthal, M.H.; Shinagare, A.B.; Hornick, J.L.; Baldini, E.H.; Ramaiya, N.H. Radiation therapy for soft-tissue sarcomas: A primer for radiologists. Radiographics 2016, 36, 554–572. [Google Scholar] [CrossRef]
- Bluemke, D.A.; Fishman, E.K.; Scott, W.W., Jr. Skeletal complications of radiation therapy. Radiographics 1994, 14, 111–121. [Google Scholar] [CrossRef]
- Epstein, J.B.; Wong, F.L.; Stevenson-Moore, P. Osteoradionecrosis: Clinical experience and a proposal for classification. J. Oral Maxillofac. Surg. 1987, 45, 104–110. [Google Scholar] [CrossRef]
- Marx, R.E.; Ehler, W.J.; Tayapongsak, P.; Pierce, L.W. Relationship of oxygen dose to angiogenesis induction in irradiated tissue. Am. J. Surg. 1990, 160, 519–524. [Google Scholar] [CrossRef]
- Sultan, A.; Hanna, G.J.; Margalit, D.N.; Chau, N.; Goguen, L.A.; Marty, F.M.; Rabinowits, G.; Schoenfeld, J.D.; Sonis, S.T.; Thomas, T.; et al. The use of hyperbaric oxygen for the prevention and management of osteoradionecrosis of the jaw: A Dana-Farber/Brigham and women’s cancer center multidisciplinary guideline. Oncologist 2017, 22, 343–350. [Google Scholar] [CrossRef]
- Shaw, R.J.; Butterworth, C.J.; Silcocks, P.; Tesfaye, B.T.; Bickerstaff, M.; Jackson, R.; Kanatas, A.; Nixon, P.; McCaul, J.; Praveen, P.; et al. HOPON (Hyperbaric Oxygen for the Prevention of Osteoradionecrosis): A randomized controlled trial of hyperbaric oxygen to prevent osteoradionecrosis of the irradiated mandible after dentoalveolar surgery. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 530–539. [Google Scholar] [CrossRef]
- Delanian, S.; Lefaix, J.L. The radiation-induced fibroatrophic process: Therapeutic perspective via the antioxidant pathway. Radiother. Oncol. 2004, 73, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Breik, O.; Tocaciu, S.; Briggs, K.; Saief, S.T.; Richardson, S. Is there a role for pentoxifylline and tocopherol in the management of advanced osteoradionecrosis of the jaws with pathological fractures? Case reports and review of the literature. Int. J. Oral Maxillofac. Surg. 2019, 48, 1022–1027. [Google Scholar] [CrossRef] [PubMed]
- Kolokythas, A.; Rasmussen, J.; Reardon, J.; Feng, C. Management of osteoradionecrosis of the jaws with pentoxifylline–tocopherol: A systematic review of the literature and meta-analysis. Int. J. Oral Maxillofac. Surgery 2019, 48, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Chin, R.Y.; Eslick, G.D.; Sritharan, N.; Paramaesvaran, S. Outcomes of microvascular free flap reconstruction for mandibular osteoradionecrosis: A systematic review. J. Cranio-Maxillofac. Surg. 2015, 43, 2026–2033. [Google Scholar] [CrossRef]
- Lu, Y.; Lai, C.Y.; Lai, P.J.; Yu, Y.H. Induced Membrane Technique for the Management of Segmental Femoral Defects: A Systematic Review and Meta-Analysis of Individual Participant Data. Orthop. Surg. 2023, 15, 28–37. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Without ORN | With ORN | p | |
|---|---|---|---|---|
| 198 | 191 | 7 | ||
| Sex | 0.654 | |||
| Male | 113 (57.1%) | 109 (57.1%) | 4 (57.1%) | |
| Female | 85 (42.9%) | 82 (42.9%) | 3 (42.9%) | |
| Age, median (IQR) | 51.5 (28) | 52.0 (28) | 51.0 (33) | 0.971 |
| BMI, median (IQR) | 24.3(5.4) | 24.2 (5.3) | 27.6 (5.3) | 0.121 |
| Smoker | 41 (20.7%) | 38 (19.9%) | 3 (42.8%) | 0.157 |
| Alcohol | 19 (9.6%) | 18 (9.4%) | 1 (14.3%) | 0.512 |
| Betel nuts | 5 (2.5%) | 4 (2.1%) | 1 (14.3%) | 0.166 |
| Hypertension | 64 (32.3%) | 61 (31.9%) | 3 (42.9%) | 0.683 |
| CCI | 0.301 | |||
| ≤3 | 167 (84.3%) | 162 (84.8%) | 5 (71.4%) | |
| >3 | 31 (15.7%) | 29 (15.2%) | 2 (28.6%) | |
| Tumor | 0.203 | |||
| Primary | 174 (87.9%) | 169 (88.5%) | 5 (71.4%) | |
| Recurrent | 24 (12.1%) | 22 (11.5%) | 2 (28.6%) | |
| Location | 0.238 | |||
| Upper limb, proximal | 24 (12.1%) | 22 (11.5%) | 2 (28.6%) | |
| Upper limb, distal | 19 (9.6%) | 19 (9.9%) | 0 | |
| Lower limb, proximal | 107 (54.0%) | 105 (54.9%) | 2 (28.6%) | |
| Lower limb, distal | 48 (24.2%) | 45 (23.6%) | 3 (42.9%) | |
| Depth | 0.452 | |||
| Superficial | 47 (23.7%) | 46 (24.1%) | 1 (14.3%) | |
| Deep | 144 (72.7%) | 138 (72.3%) | 6 (85.7%) | |
| Re-resection | 30 (15.2%) | 29 (15.2) | 1 (14.3%) | 0.713 |
| Periosteal stripping | 14 (7.1%) | 11 (5.8%) | 3 (42.8%) | 0.008 * |
| Lymphovascular invasion | 31 (15.7%) | 29 (15.2%) | 2 (28.6%) | 0.301 |
| Tumor classification | 0.644 | |||
| T1 | 56 (28.3%) | 54 (28.3%) | 2 (28.6%) | |
| T2 | 77 (38.9%) | 74 (38.7%) | 3 (42.8%) | |
| T3 | 30 (15.2%) | 30 (15.7%) | 0 | |
| T4 | 34 (17.2%) | 32 (16.8%) | 2 (28.6%) | |
| Histologic grade | 0.63 | |||
| G1 | 48 (24.2%) | 47 (24.6%) | 1 (14.3%) | |
| G2 | 53 (26.8%) | 50 (26.2%) | 3 (42.8%) | |
| G3 | 86 (43.4%) | 83 (43.5%) | 3 (42.8%) | |
| Margin | 0.242 | |||
| Negative | 33 (16.7%) | 33 (17.3%) | 0 | |
| Close | 80 (40.4%) | 78 (40.8%) | 2 (28.6%) | |
| Positive | 85 (42.9%) | 80 (41.9%) | 5 (71.4%) | |
| Pathology | 0.630 | |||
| Undifferentiated pleomorphic sarcoma | 45 (22.7%) | 42 (21.9%) | 3 (42.8%) | |
| Myxoid liposarcoma | 26 (13.1%) | 25 (13.1%) | 1 (14.3%) | |
| Synovial sarcoma | 25 (12.6%) | 24 (12.6%) | 1 (14.3%) | |
| Myxofibrosarcoma | 24 (12.1%) | 24 (12.6%) | 0 | |
| Leiomyosarcoma | 10 (5.1%) | 9 (4.7%) | 1 (14.3%) | |
| MPNST | 10 (5.1%) | 10 (5.2%) | 0 | |
| Other | 58 (29.3%) | 57 (29.8%) | 1 (14.3%) | |
| Dosage (Gy), median (IQR) | 64.0 (6.0) | 64.0 (6) | 68.0 (6) | 0.048 * |
| Adjuvant chemotherapy | 17 (8.6%) | 16 (8.4%) | 1 (14.3%) | 0.472 |
| Repeated RT | 16 (8.1%) | 13 (6.8%) | 3 (42.8%) | 0.057 |
| Case | Sex | Age | Location | Diagnosis | Margin | Radiation Dose (Gy) | Lag Time (m) | Presentation | Management | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 76 | Left lower leg | Undifferentiated pleomorphic sarcoma | Positive | 66 | 3 | Chronic ulcers, pathological fracture | Debridement, sequestrectomy, bone graft, ORIF, flap reconstruction | Nonunion bone |
| 2 | F | 69 | Left ankle | Leiomyosarcoma | Positive | 60 | 13 | Chronic ulcers, bone exposure | Debridement, flap reconstruction | Healed wound |
| 3 | F | 26 | Left hip | Undifferentiated pleomorphic sarcoma | Positive | 74 | 67 | Periprosthetic fracture, persistent sinus discharge | Debridement, hip joint arthroplasty, flap reconstruction | No infection sign |
| 4 | M | 36 | Left upper arm | Synovial sarcoma | Positive | 70 | 14 | Persistent sinus discharge, wound poor healing | Debridement, synovectomy | Shoulder disarticulation |
| 5 | M | 45 | Left thigh | Myxoid liposarcoma | Close | 70 | 23 | Persistent sinus discharge, wound poor healing, pathological fracture | Debridement, HBO therapy | AK amputation |
| 6 | F | 57 | Left lower leg | Dedifferentiated liposarcoma | Positive | 70 | 3 | Nonunion bone | Debridement, bone graft, HBO therapy, ORIF, flap reconstruction | BK amputation |
| 7 | M | 48 | Right thigh | Undifferentiated pleomorphic sarcoma | Close | 60 | 36 | Persistent sinus discharge, soft tissue necrosis, nonunion bone | Debridement, sequestrectomy, ORIF, flap reconstruction, pentoxifylline, tocopherol | Bone union, wound healed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, Y.-J.; Chen, C.-C.; Chen, S.-H.; Lin, C.-H.; Lin, Y.-T.; Lin, C.-H.; Hsu, C.-C. Incidence and Risk Factors for Extremity Osteoradionecrosis after Limb-Sparing Surgery and Adjuvant Radiotherapy. Cancers 2023, 15, 2339. https://doi.org/10.3390/cancers15082339
Lu Y-J, Chen C-C, Chen S-H, Lin C-H, Lin Y-T, Lin C-H, Hsu C-C. Incidence and Risk Factors for Extremity Osteoradionecrosis after Limb-Sparing Surgery and Adjuvant Radiotherapy. Cancers. 2023; 15(8):2339. https://doi.org/10.3390/cancers15082339
Chicago/Turabian StyleLu, Yun-Jui, Chun-Chieh Chen, Shih-Heng Chen, Cheng-Hung Lin, Yu-Te Lin, Chih-Hung Lin, and Chung-Chen Hsu. 2023. "Incidence and Risk Factors for Extremity Osteoradionecrosis after Limb-Sparing Surgery and Adjuvant Radiotherapy" Cancers 15, no. 8: 2339. https://doi.org/10.3390/cancers15082339