
Pediatric Patients with Stage IV Rhabdomyosarcoma Significantly Benefit from Long-Term Maintenance Therapy: Results of the CWS-IV 2002 and the CWS DOK IV 2004-Trials

 , , , , , , ,
, , , , , , ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Eligible Patients
2.2. Treatment Schedule According to CWS-IV 2002 and CWS 2002 Doku-Trial
2.3. Statistical Methods
3. Results
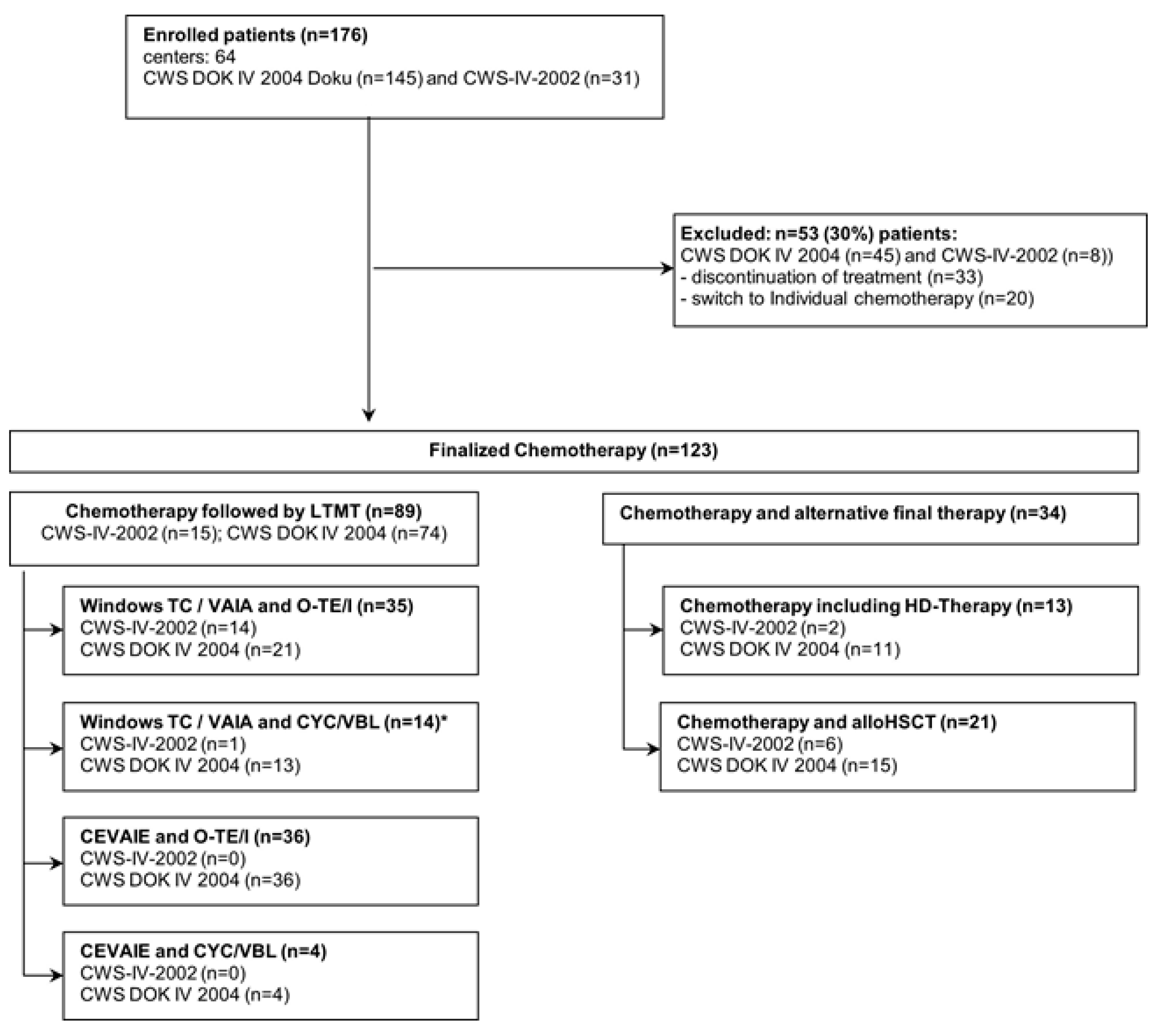
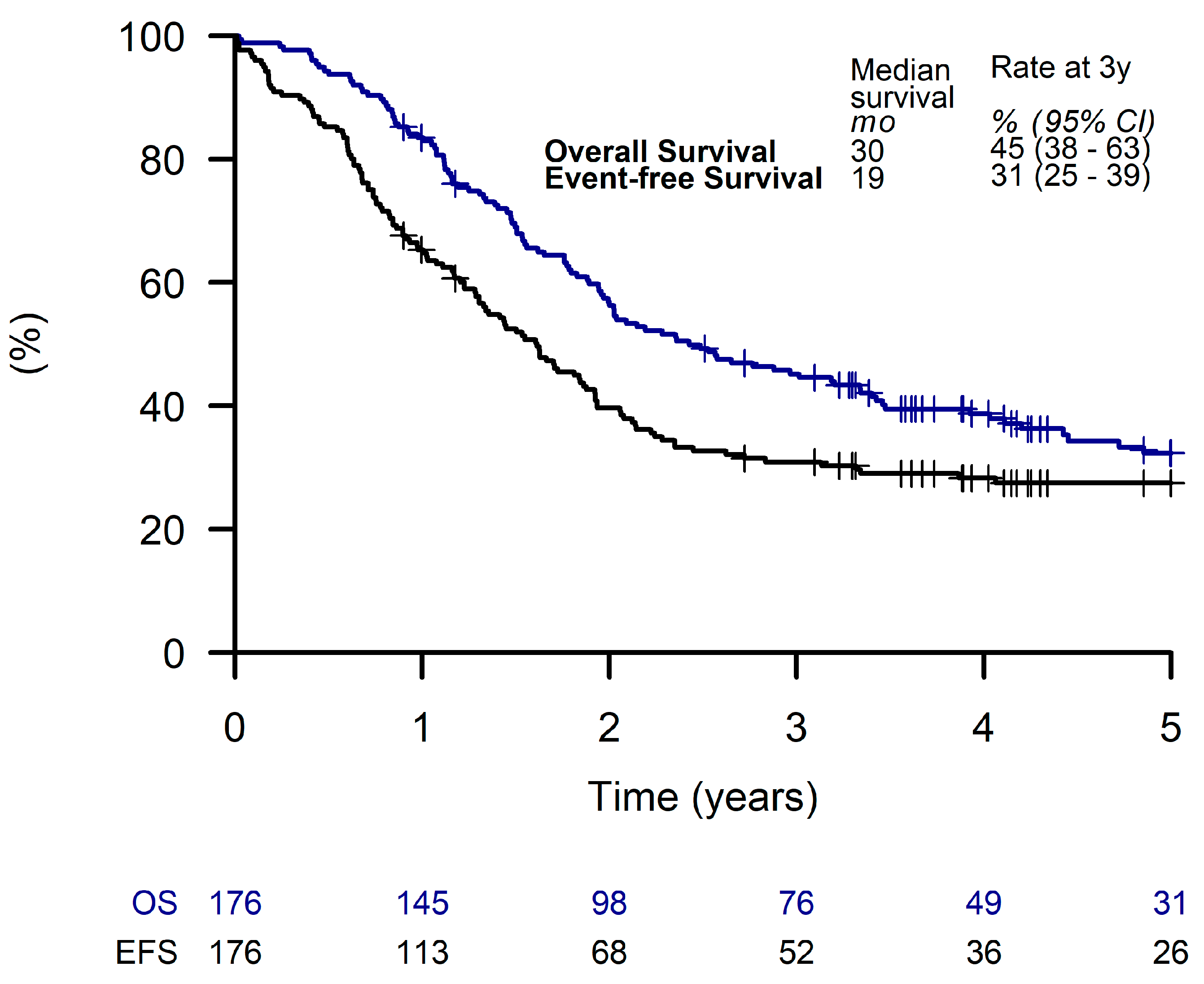
3.1. Patient Characteristics
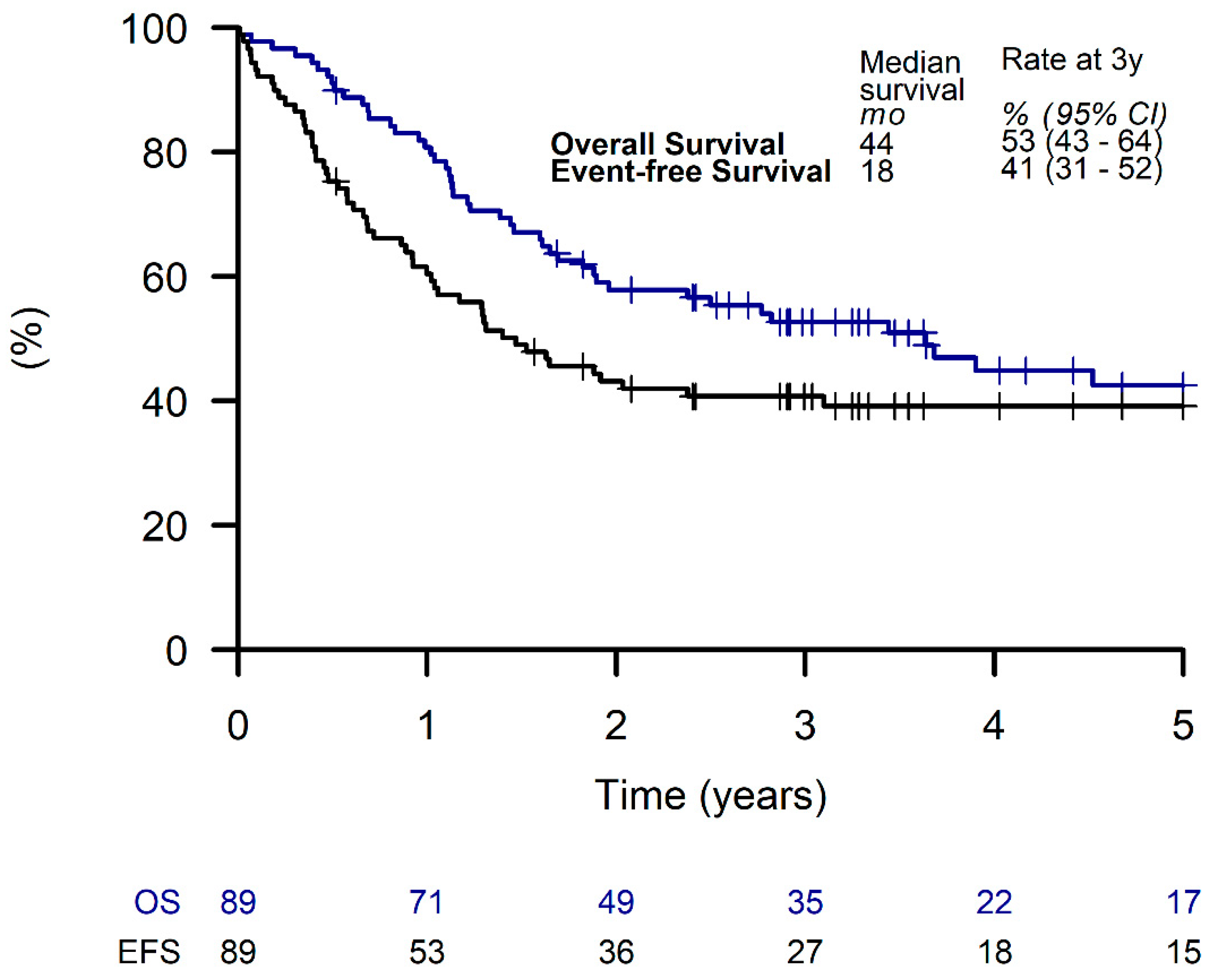
3.2. Outcome of Patients Receiving LTMT
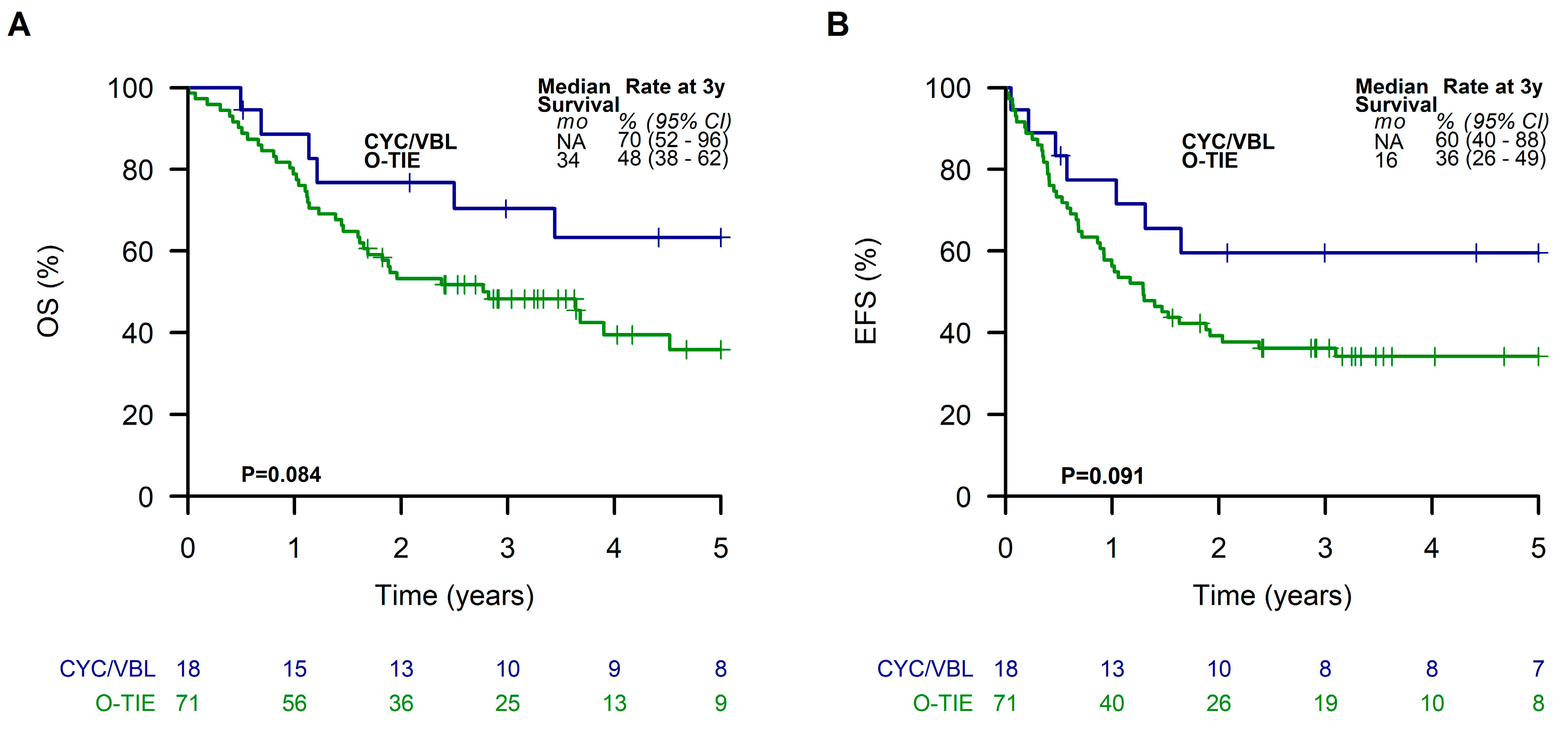
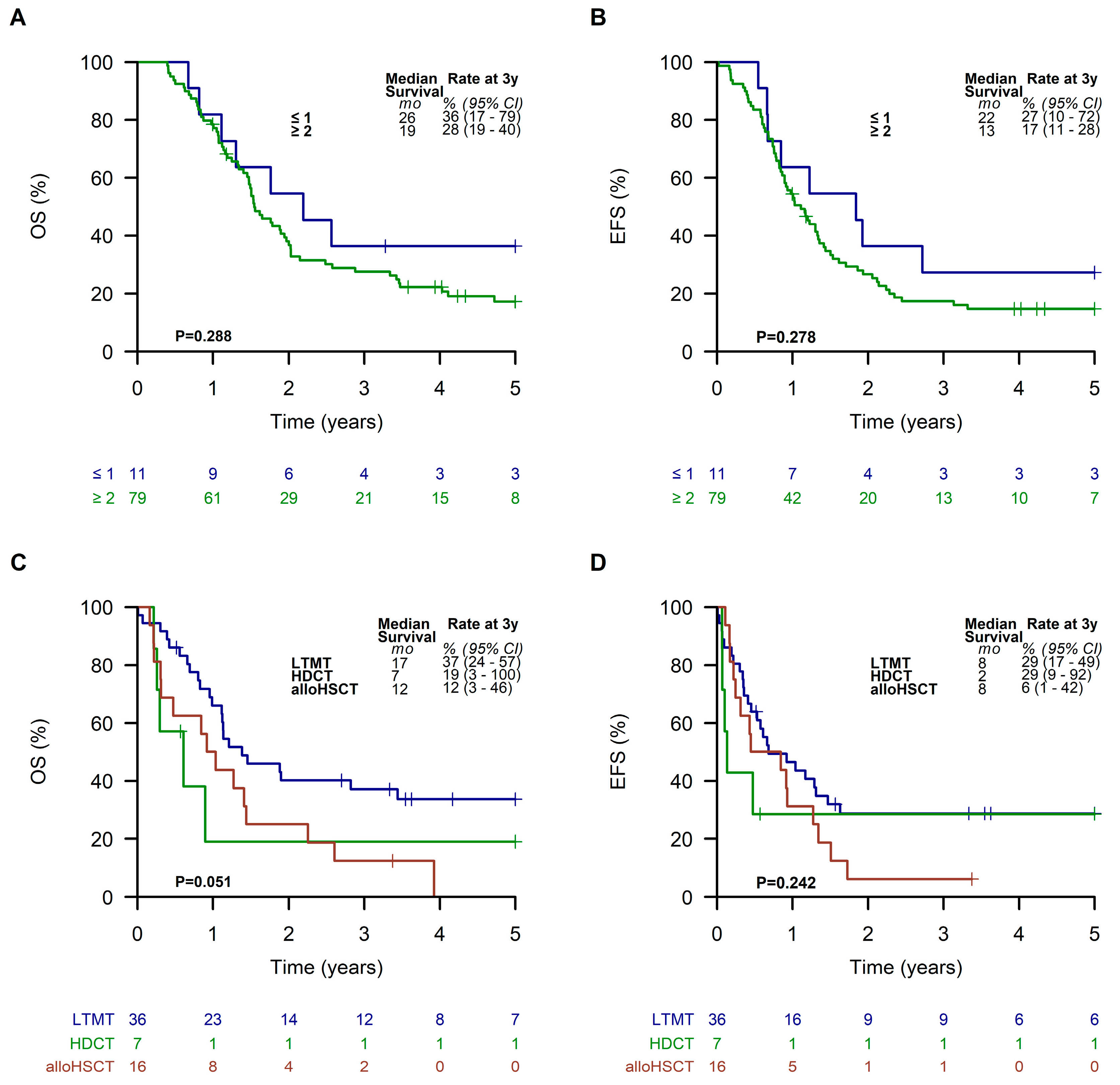
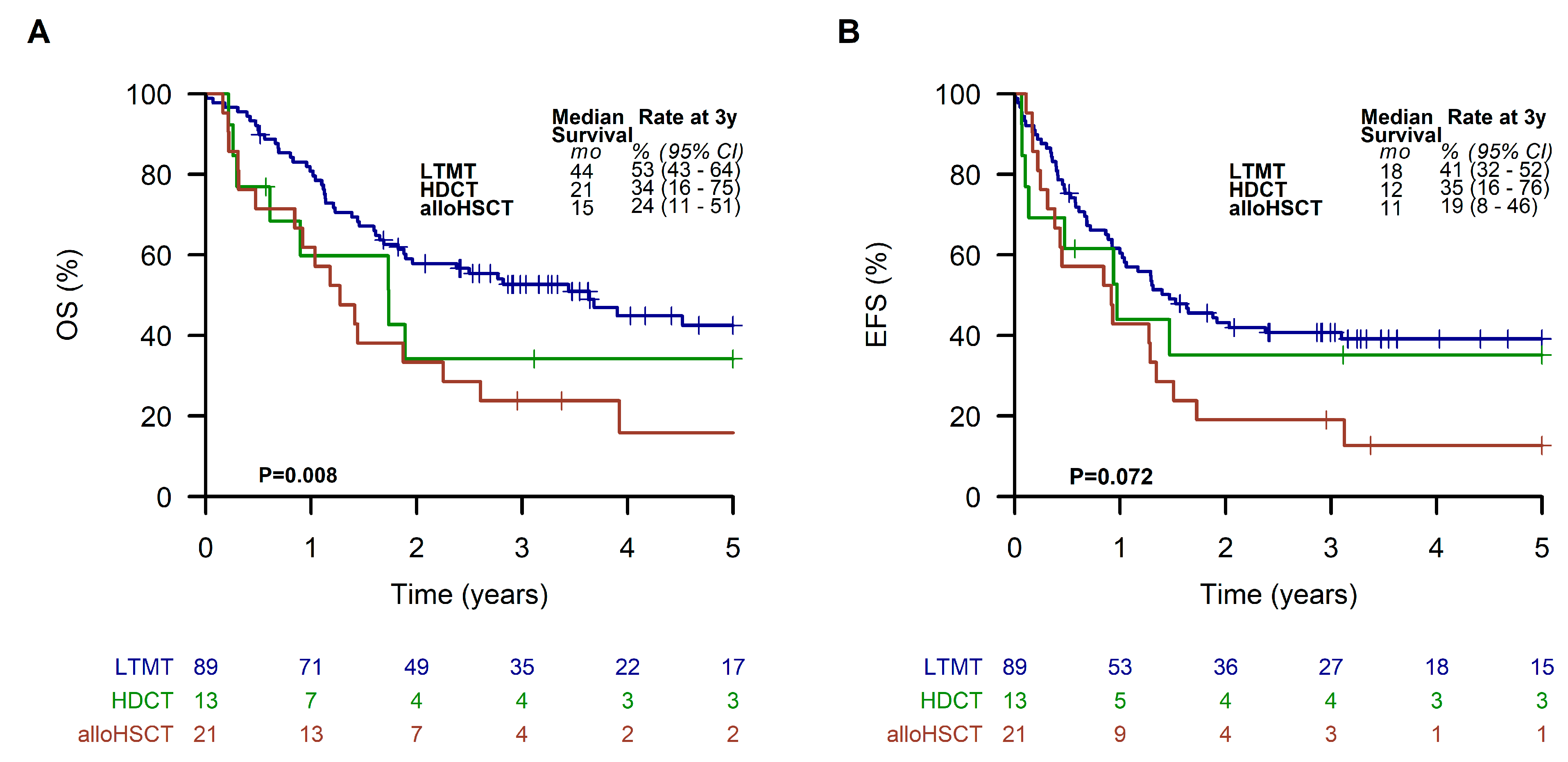
3.3. Outcome Depending on Treatment Strategies after Intensive Chemotherapy
3.4. Toxicity
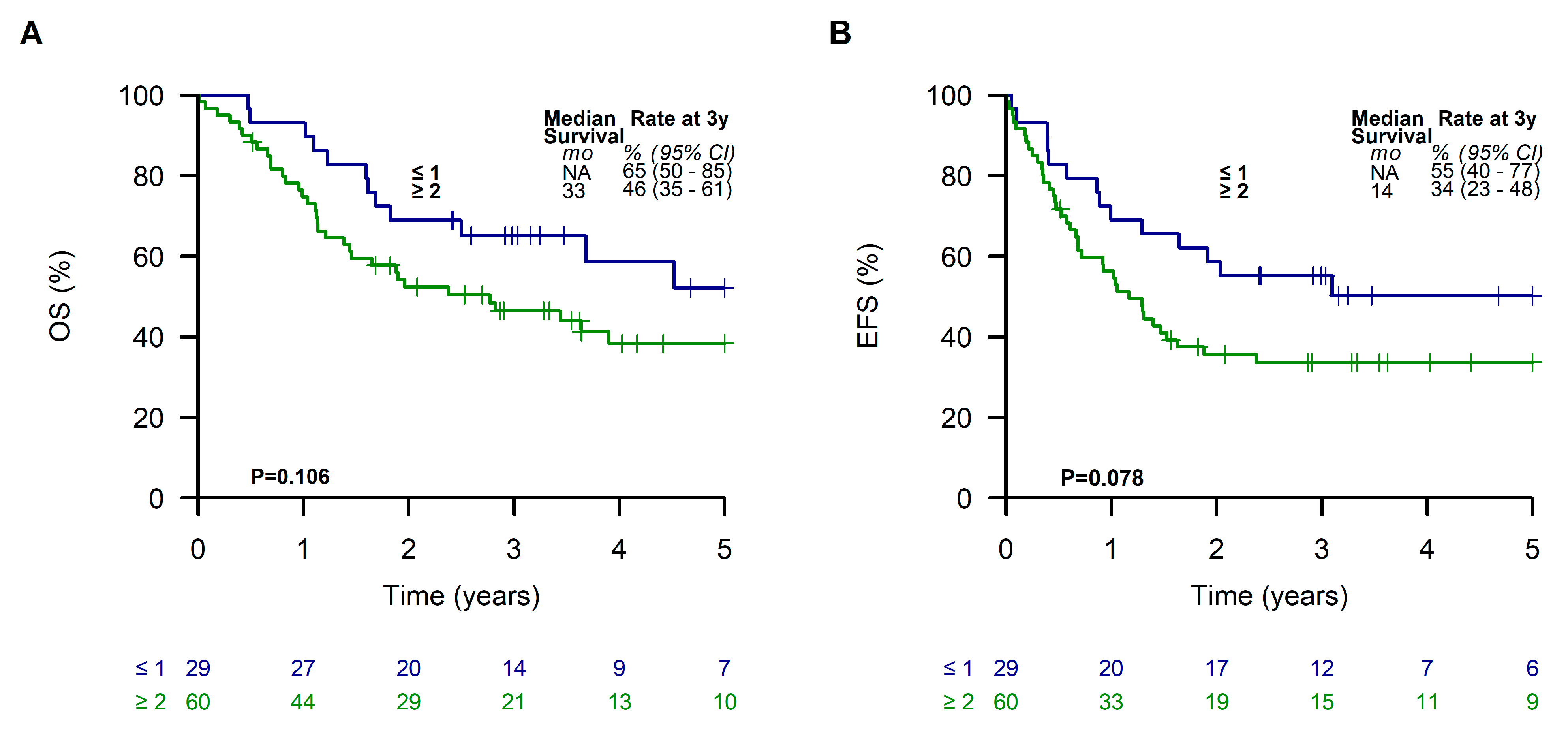
3.5. Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weihkopf, T.; Blettner, M.; Dantonello, T.; Jung, I.; Klingebiel, T.; Koscielniak, E.; Luckel, M.; Spix, C.; Kaatsch, P. Incidence and time trends of soft tissue sarcomas in German children 1985–2004—A report from the population-based German Childhood Cancer Registry. Eur. J. Cancer 2008, 44, 432–440. [Google Scholar] [CrossRef]
- Sultan, I.; Qaddoumi, I.; Yaser, S.; Rodriguez-Galindo, C.; Ferrari, A. Comparing adult and pediatric rhabdomyosarcoma in the surveillance, epidemiology and end results program, 1973 to 2005: An analysis of 2600 patients. J. Clin. Oncol. 2009, 27, 3391–3397. [Google Scholar] [CrossRef] [PubMed]
- Stevens, M.C.; Rey, A.; Bouvet, N.; Ellershaw, C.; Flamant, F.; Habrand, J.L.; Marsden, H.B.; Martelli, H.; Sanchez de Toledo, J.; Spicer, R.D.; et al. Treatment of nonmetastatic rhabdomyosarcoma in childhood and adolescence: Third study of the International Society of Paediatric Oncology--SIOP Malignant Mesenchymal Tumor 89. J. Clin. Oncol. 2005, 23, 2618–2628. [Google Scholar] [CrossRef] [PubMed]
- Koscielniak, E.; Blank, B.; Vokuhl, C.; Kazanowska, B.; Ladenstein, R.; Niggli, F.; Ljungman, G.; Handgretinger, R.; Seitz, G.; Fuchs, J.; et al. Long-Term Clinical Outcome and Prognostic Factors of Children and Adolescents with Localized Rhabdomyosarcoma Treated on the CWS-2002P Protocol. Cancers 2022, 14, 899. [Google Scholar] [CrossRef] [PubMed]
- Bisogno, G.; Minard-Colin, V.; Zanetti, I.; Ferrari, A.; Gallego, S.; Davila Fajardo, R.; Mandeville, H.; Kelsey, A.; Alaggio, R.; Orbach, D.; et al. Nonmetastatic Rhabdomyosarcoma in Children and Adolescents: Overall Results of the European Pediatric Soft Tissue Sarcoma Study Group RMS2005 Study. J. Clin. Oncol. 2023, JCO2202093. [Google Scholar] [CrossRef]
- Breneman, J.C.; Lyden, E.; Pappo, A.S.; Link, M.P.; Anderson, J.R.; Parham, D.M.; Qualman, S.J.; Wharam, M.D.; Donaldson, S.S.; Maurer, H.M.; et al. Prognostic factors and clinical outcomes in children and adolescents with metastatic rhabdomyosarcoma—A report from the Intergroup Rhabdomyosarcoma Study IV. J. Clin. Oncol. 2003, 21, 78–84. [Google Scholar] [CrossRef]
- Malempati, S.; Hawkins, D.S. Rhabdomyosarcoma: Review of the Children’s Oncology Group (COG) Soft-Tissue Sarcoma Committee experience and rationale for current COG studies. Pediatr. Blood Cancer 2012, 59, 5–10. [Google Scholar] [CrossRef]
- Koscielniak, E.; Rodary, C.; Flamant, F.; Carli, M.; Treuner, J.; Pinkerton, C.R.; Grotto, P. Metastatic rhabdomyosarcoma and histologically similar tumors in childhood: A retrospective European multi-center analysis. Med. Pediatr. Oncol. 1992, 20, 209–214. [Google Scholar] [CrossRef]
- Oberlin, O.; Rey, A.; Lyden, E.; Bisogno, G.; Stevens, M.C.; Meyer, W.H.; Carli, M.; Anderson, J.R. Prognostic factors in metastatic rhabdomyosarcomas: Results of a pooled analysis from United States and European cooperative groups. J. Clin. Oncol. 2008, 26, 2384–2389. [Google Scholar] [CrossRef]
- Koscielniak, E.; Klingebiel, T.H.; Peters, C.; Hermann, J.; Burdach, S.T.; Bender-Gotze, C.; Muller-Weihrich, S.T.; Treuner, J. Do patients with metastatic and recurrent rhabdomyosarcoma benefit from high-dose therapy with hematopoietic rescue? Report of the German/Austrian Pediatric Bone Marrow Transplantation Group. Bone Marrow Transpl. 1997, 19, 227–231. [Google Scholar] [CrossRef]
- Walterhouse, D.O.; Hoover, M.L.; Marymont, M.A.; Kletzel, M. High-dose chemotherapy followed by peripheral blood stem cell rescue for metastatic rhabdomyosarcoma: The experience at Chicago Children’s Memorial Hospital. Med. Pediatr. Oncol. 1999, 32, 88–92. [Google Scholar] [CrossRef]
- Weigel, B.J.; Breitfeld, P.P.; Hawkins, D.; Crist, W.M.; Baker, K.S. Role of high-dose chemotherapy with hematopoietic stem cell rescue in the treatment of metastatic or recurrent rhabdomyosarcoma. J. Pediatr. Hematol. Oncol. 2001, 23, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Soft Tissue Sarcoma Committee of the Children’s Oncology Group; Lager, J.J.; Lyden, E.R.; Anderson, J.R.; Pappo, A.S.; Meyer, W.H.; Breitfeld, P.P. Pooled analysis of phase II window studies in children with contemporary high-risk metastatic rhabdomyosarcoma: A report from the Soft Tissue Sarcoma Committee of the Children’s Oncology Group. J. Clin. Oncol. 2006, 24, 3415–3422. [Google Scholar] [CrossRef] [PubMed]
- Weigel, B.J.; Lyden, E.; Anderson, J.R.; Meyer, W.H.; Parham, D.M.; Rodeberg, D.A.; Michalski, J.M.; Hawkins, D.S.; Arndt, C.A. Intensive Multiagent Therapy, Including Dose-Compressed Cycles of Ifosfamide/Etoposide and Vincristine/Doxorubicin/Cyclophosphamide, Irinotecan, and Radiation, in Patients With High-Risk Rhabdomyosarcoma: A Report From the Children’s Oncology Group. J. Clin. Oncol. 2016, 34, 117–122. [Google Scholar] [CrossRef]
- Klingebiel, T.; Boos, J.; Beske, F.; Hallmen, E.; Int-Veen, C.; Dantonello, T.; Treuner, J.; Gadner, H.; Marky, I.; Kazanowska, B.; et al. Treatment of children with metastatic soft tissue sarcoma with oral maintenance compared to high dose chemotherapy: Report of the HD CWS-96 trial. Pediatr. Blood Cancer 2008, 50, 739–745. [Google Scholar] [CrossRef]
- Merker, M.; Meister, M.T.; Rettinger, E.; Jarisch, A.; Soerensen, J.; Willasch, A.; Huenecke, S.; Cappel, C.; Bremm, M.; Salzmann-Manrique, E.; et al. Haploidentical allogeneic hematopoietic stem cell transplantation in patients with high-risk soft tissue sarcomas: Results of a single-center prospective trial. Bone Marrow Transpl. 2018, 53, 891–894. [Google Scholar] [CrossRef]
- Schober, S.J.; Hallmen, E.; Ressle, F.; Gassmann, H.; Prexler, C.; Wawer, A.; von Luettichau, I.; Ladenstein, R.; Kazanowska, B.; Ljungman, G.; et al. No Improvement of Survival for Alveolar Rhabdomyosarcoma Patients After HLA-Matched Versus -Mismatched Allogeneic Hematopoietic Stem Cell Transplantation Compared to Standard-of-Care Therapy. Front. Oncol. 2022, 12, 878367. [Google Scholar] [CrossRef]
- Eichholz, T.; Doring, M.; Giardino, S.; Gruhn, B.; Seitz, C.; Flaadt, T.; Schwinger, W.; Ebinger, M.; Holzer, U.; Mezger, M.; et al. Haploidentical hematopoietic stem cell transplantation as individual treatment option in pediatric patients with very high-risk sarcomas. Front. Oncol. 2023, 13, 1064190. [Google Scholar] [CrossRef]
- Casanova, M.; Ferrari, A.; Bisogno, G.; Merks, J.H.; De Salvo, G.L.; Meazza, C.; Tettoni, K.; Provenzi, M.; Mazzarino, I.; Carli, M. Vinorelbine and low-dose cyclophosphamide in the treatment of pediatric sarcomas: Pilot study for the upcoming European Rhabdomyosarcoma Protocol. Cancer 2004, 101, 1664–1671. [Google Scholar] [CrossRef] [PubMed]
- Bisogno, G.; De Salvo, G.L.; Bergeron, C.; Gallego Melcon, S.; Merks, J.H.; Kelsey, A.; Martelli, H.; Minard-Colin, V.; Orbach, D.; Glosli, H.; et al. Vinorelbine and continuous low-dose cyclophosphamide as maintenance chemotherapy in patients with high-risk rhabdomyosarcoma (RMS 2005): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2019, 20, 1566–1575. [Google Scholar] [CrossRef] [PubMed]
- Bisogno, G.; Jenney, M.; Bergeron, C.; Gallego Melcon, S.; Ferrari, A.; Oberlin, O.; Carli, M.; Stevens, M.; Kelsey, A.; De Paoli, A.; et al. Addition of dose-intensified doxorubicin to standard chemotherapy for rhabdomyosarcoma (EpSSG RMS 2005): A multicentre, open-label, randomised controlled, phase 3 trial. Lancet Oncol. 2018, 19, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Chisholm, J.C.; Merks, J.H.M.; Casanova, M.; Bisogno, G.; Orbach, D.; Gentet, J.C.; Thomassin-Defachelles, A.S.; Chastagner, P.; Lowis, S.; Ronghe, M.; et al. Open-label, multicentre, randomised, phase II study of the EpSSG and the ITCC evaluating the addition of bevacizumab to chemotherapy in childhood and adolescent patients with metastatic soft tissue sarcoma (the BERNIE study). Eur. J. Cancer 2017, 83, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Schoot, R.A.; Chisholm, J.C.; Casanova, M.; Minard-Colin, V.; Geoerger, B.; Cameron, A.L.; Coppadoro, B.; Zanetti, I.; Orbach, D.; Kelsey, A.; et al. Metastatic Rhabdomyosarcoma: Results of the European Paediatric Soft Tissue Sarcoma Study Group MTS 2008 Study and Pooled Analysis With the Concurrent BERNIE Study. J. Clin. Oncol. 2022, 40, 3730–3740. [Google Scholar] [CrossRef] [PubMed]
- Bochennek, K.; Dantonello, T.; Koscielniak, E.; Claviez, A.; Dirksen, U.; Sauerbrey, A.; Beilken, A.; Klingebiel, T. Response of children with stage IV soft tissue sarcoma to topotecan and carboplatin: A phase II window trial of the cooperative soft tissue sarcoma group. Klin. Padiatr. 2013, 225, 309–314. [Google Scholar] [CrossRef]
- Hibbitts, E.; Chi, Y.Y.; Hawkins, D.S.; Barr, F.G.; Bradley, J.A.; Dasgupta, R.; Meyer, W.H.; Rodeberg, D.A.; Rudzinski, E.R.; Spunt, S.L.; et al. Refinement of risk stratification for childhood rhabdomyosarcoma using FOXO1 fusion status in addition to established clinical outcome predictors: A report from the Children’s Oncology Group. Cancer Med. 2019, 8, 6437–6448. [Google Scholar] [CrossRef]
- Shern, J.F.; Selfe, J.; Izquierdo, E.; Patidar, R.; Chou, H.C.; Song, Y.K.; Yohe, M.E.; Sindiri, S.; Wei, J.; Wen, X.; et al. Genomic Classification and Clinical Outcome in Rhabdomyosarcoma: A Report From an International Consortium. J. Clin. Oncol. 2021, 39, 2859–2871. [Google Scholar] [CrossRef]
- Haduong, J.H.; Heske, C.M.; Allen-Rhoades, W.; Xue, W.; Teot, L.A.; Rodeberg, D.A.; Donaldson, S.S.; Weiss, A.; Hawkins, D.S.; Venkatramani, R. An update on rhabdomyosarcoma risk stratification and the rationale for current and future Children’s Oncology Group clinical trials. Pediatr. Blood Cancer 2022, 69, e29511. [Google Scholar] [CrossRef]
- Rudzinski, E.R.; Kelsey, A.; Vokuhl, C.; Linardic, C.M.; Shipley, J.; Hettmer, S.; Koscielniak, E.; Hawkins, D.S.; Bisogno, G. Pathology of childhood rhabdomyosarcoma: A consensus opinion document from the Children’s Oncology Group, European Paediatric Soft Tissue Sarcoma Study Group, and the Cooperative Weichteilsarkom Studiengruppe. Pediatr. Blood Cancer 2021, 68, e28798. [Google Scholar] [CrossRef]
- Carli, M.; Colombatti, R.; Oberlin, O.; Bisogno, G.; Treuner, J.; Koscielniak, E.; Tridello, G.; Garaventa, A.; Pinkerton, R.; Stevens, M. European intergroup studies (MMT4-89 and MMT4-91) on childhood metastatic rhabdomyosarcoma: Final results and analysis of prognostic factors. J. Clin. Oncol. 2004, 22, 4787–4794. [Google Scholar] [CrossRef]
- Thiel, U.; Koscielniak, E.; Blaeschke, F.; Grunewald, T.G.; Badoglio, M.; Diaz, M.A.; Paillard, C.; Prete, A.; Ussowicz, M.; Lang, P.; et al. Allogeneic stem cell transplantation for patients with advanced rhabdomyosarcoma: A retrospective assessment. Br. J. Cancer 2013, 109, 2523–2532. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | ||||
|---|---|---|---|---|
| CWS-IV 2002 | CWS DOK IV 2004 | Total | p | |
| N (%) | 31 (18) | 145 (82) | 176 (100) | |
| Sex, N (%) | 0.825 | |||
| Female | 15 (48) | 67 (46) | 82 (47) | |
| Male | 16 (52) | 78 (54) | 94 (53) | |
| Age, years | ||||
| Median (range) | 15 (2–21) | 12 (0–20) | 12 (0 -21) | 0.048 |
| Age, N (%) | ||||
| ≤1 y | 0 | 4 (3) | 4 (2) | 0.792 |
| 1–9 | 11 (35) | 58 (40) | 69 (39) | |
| ≥10 | 20 (65) | 83 (57) | 103 (59) | |
| Histology, N (%) | 0.617 | |||
| Embryonal RMS | 8 (26) | 50 (35) | 58 (33) | |
| Alveolar RMS | 17 (55) | 73 (50) | 90 (51) | |
| Other | 6 (19) | 22 (15) | 28 (16) | |
| Primary site of tumor, N (%) * | 0.800 | |||
| Favorable | 3 (10) | 12 (8) | 15 (9) | |
| Unfavorable | 28 (90) | 133 (92) | 161 (91) | |
| Tumor size, N (%) | 0.730 | |||
| ≤5 cm | 5 (16) | 25 (17) | 30 (17) | |
| >5 cm | 25 (81) | 110 (76) | 135 (77) | |
| Unknown | 1 (3) | 10 (7) | 11 (6) | |
| Number of metastases, N (%) | 1 | |||
| ≤2 | 21 (68) | 100 (69) | 121 (69) | |
| ≥3 | 10 (32) | 45 (31) | 55 (31) | |
| Bone or bone marrow involvement, N (%) | 0.431 | |||
| Yes | 17 (55) | 67 (46) | 84 (48) | |
| No | 14 (45) | 78 (54) | 92 (52) | |
| Oberlin score, (%) | 0.822 | |||
| ≤1 | 7 (23) | 38 (26) | 45 (26) | |
| ≥2 | 24 (77) | 107 (74) | 131 (74) | |
| Period of start initial chemotherapy | 0.294 | |||
| Median | November 2006 | December 2005 | June 2006 | |
| Range | February 2005–December 2007 | November 2002–July 2010 | November 2002–July 2010 | |
| Initial chemotherapy, N (%) | <0.001 | |||
| Window TC/VAIA | 31 (100) | 70 (48) | 101 (57) | |
| CEVAIE | 0 | 69 (48) | 69 (39) | |
| Others | 0 | 6 (4) | 6 (3) | |
| Time between start initial chemotherapy and final treatment, days | 0.431 | |||
| Median | 252 | 254 | 254 | |
| Range | 133–348 | 167–472 | 133–472 | |
| Excluded | 8 | 45 | 53 | |
| Period of start final treatment | 0.768 | |||
| Median | July 2007 | December 2006 | April 2007 | |
| Range | September 2005–Jun 2008 | June 2003–May 2011 | June 2003–May 2011 | |
| Excluded | 8 | 45 | 53 | |
| Final treatment, N (%) | 0.558 | |||
| LTMT | 15 (48) | 74 (51) | 89 (51) | |
| HDC | 2 (6) | 11 (8) | 13 (7) | |
| alloSCT | 6 (19) | 15 (10) | 21 (12) | |
| Excluded | 8 (26) | 45 (31) | 53 (30) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tramsen, L.; Bochennek, K.; Sparber-Sauer, M.; Salzmann-Manrique, E.; Scheer, M.; Dantonello, T.; Borkhardt, A.; Dirksen, U.; Thorwarth, A.; Greiner, J.; et al. Pediatric Patients with Stage IV Rhabdomyosarcoma Significantly Benefit from Long-Term Maintenance Therapy: Results of the CWS-IV 2002 and the CWS DOK IV 2004-Trials. Cancers 2023, 15, 2050. https://doi.org/10.3390/cancers15072050
Tramsen L, Bochennek K, Sparber-Sauer M, Salzmann-Manrique E, Scheer M, Dantonello T, Borkhardt A, Dirksen U, Thorwarth A, Greiner J, et al. Pediatric Patients with Stage IV Rhabdomyosarcoma Significantly Benefit from Long-Term Maintenance Therapy: Results of the CWS-IV 2002 and the CWS DOK IV 2004-Trials. Cancers. 2023; 15(7):2050. https://doi.org/10.3390/cancers15072050
Chicago/Turabian StyleTramsen, Lars, Konrad Bochennek, Monika Sparber-Sauer, Emilia Salzmann-Manrique, Monika Scheer, Tobias Dantonello, Arndt Borkhardt, Uta Dirksen, Anne Thorwarth, Jeanette Greiner, and et al. 2023. "Pediatric Patients with Stage IV Rhabdomyosarcoma Significantly Benefit from Long-Term Maintenance Therapy: Results of the CWS-IV 2002 and the CWS DOK IV 2004-Trials" Cancers 15, no. 7: 2050. https://doi.org/10.3390/cancers15072050