
Selective Axillary Dissection after Neoadjuvant Chemotherapy in Patients with Lymph-Node-Positive Breast Cancer (CLYP Study): The Radio-Guided Occult Lesion Localization Technique for Biopsy-Proven Metastatic Lymph Nodes
 , , ,
, , ,  ,
, 
 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
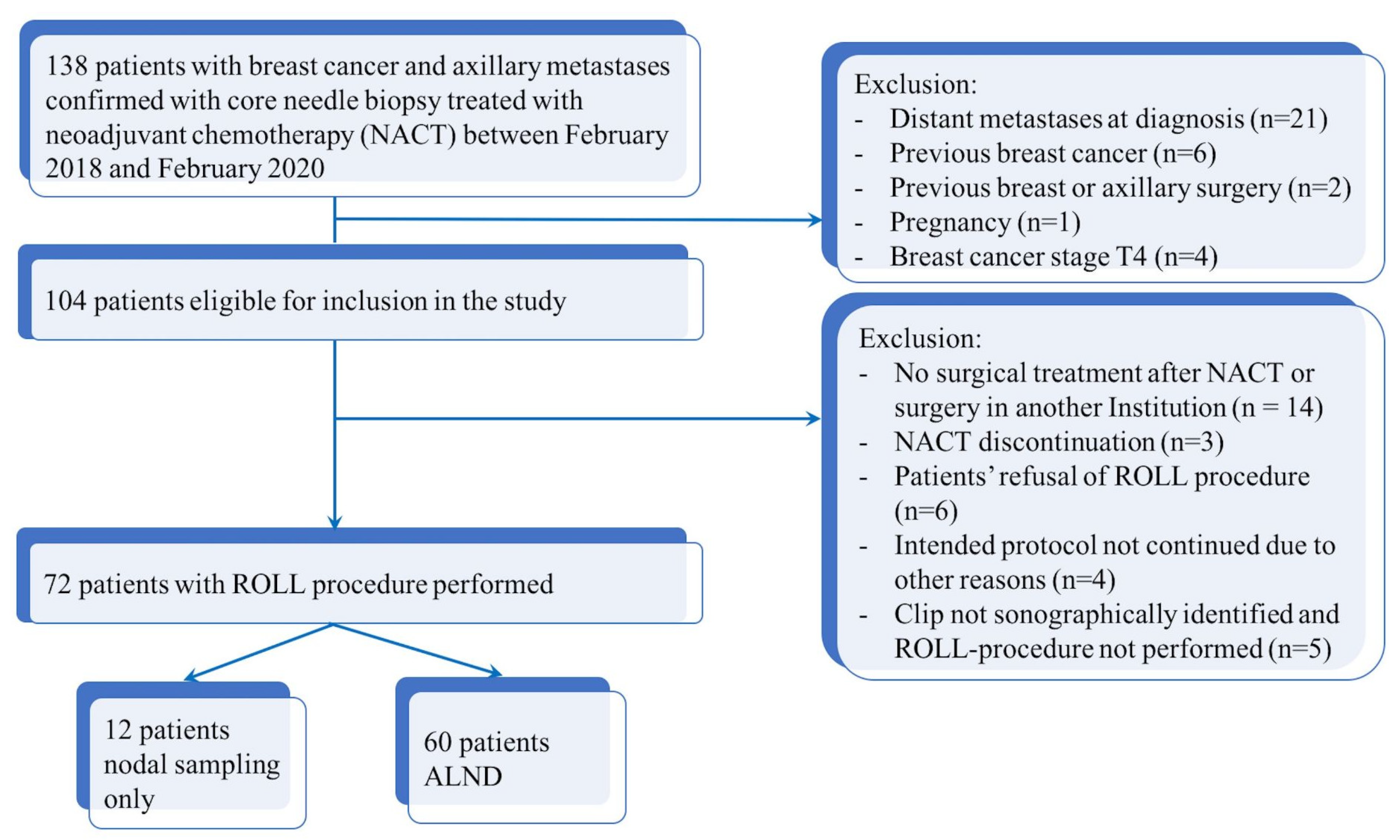
2.1. Study Population
2.2. Pathological Evaluation
2.3. Statistical Analysis
3. Results
3.1. CLN and SLNs and the Prediction of the Nodal Status
3.2. Factors Contributing to Prediction of Nodal Status for CLN and SLNs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beenken, S.W.; Urist, M.M.; Zhang, Y.; Desmond, R.; Krontiras, H.; Medina, H.; Bland, K.I. Axillary lymph node status, but not tumor size, predicts locoregional recurrence and overall survival after mastectomy for breast cancer. Ann. Surg. 2003, 237, 732–738, discussion 738–739. [Google Scholar] [CrossRef]
- Caudle, A.S.; Cupp, J.A.; Kuerer, H.M. Management of axillary disease. Surg. Oncol. Clin. N. Am. 2014, 23, 473–486. [Google Scholar] [CrossRef]
- Gandhi, A.; Coles, C.; Makris, A.; Provenzano, E.; Goyal, A.; Maxwell, A.J.; Doughty, J.; Gandhi, A.; Coles, C.; Makris, A.; et al. Axillary surgery following neoadjuvant chemotherapy-multidisciplinary guidance from the association of breast surgery, faculty of clinical oncology of the royal college of radiologists, UK breast cancer group, national coordinating committee for breast pathology and British society of breast radiology. Clin. Oncol. 2019, 31, 664–668. [Google Scholar]
- Dominici, L.S.; Gonzalez, V.M.N.; Buzdar, A.U.; Lucci, A.; Mittendorf, E.A.; Le-Petross, H.T.; Babiera, G.V.; Meric-Bernstam, F.; Hunt, K.K.; Kuerer, H.M. Cytologically proven axillary lymph node metastases are eradicated in patients receiving preoperative chemotherapy with concurrent trastuzumab for HER2-positive breast cancer. Cancer 2010, 116, 2884–2889. [Google Scholar] [CrossRef]
- Lucci, A.; McCall, L.M.; Beitsch, P.D.; Whitworth, P.W.; Reintgen, D.S.; Blumencranz, P.W.; Leitch, A.M.; Saha, S.; Hunt, K.K.; Giuliano, A.E. American College of Surgeons Oncology Group: Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J. Clin. Oncol. 2007, 25, 3657–3663. [Google Scholar] [CrossRef]
- Boughey, J.C.; Suman, V.J.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Leitch, A.M.; Kuerer, H.M.; Bowling, M.; Flippo-Morton, T.S.; et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: The ACOSOG Z1071 (Alliance) clinical trial. JAMA 2013, 310, 1455–1461. [Google Scholar] [CrossRef] [Green Version]
- Kuehn, T.; Bauerfeind, I.; Fehm, T.; Fleige, B.; Hausschild, M.; Helms, G.; Lebeau, A.; Liedtke, C.; Minckwitz, P.G.; Nekljudova, V.; et al. Sentinel lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): A prospective, multicentre cohort study. Lancet Oncol. 2013, 14, 609–618. [Google Scholar] [CrossRef]
- Boileau, J.-F.; Poirier, B.; Basik, M.; Holloway, C.M.; Gaboury, L.; Sideris, L.; Meterissian, S.; Arnaout, A.; Brackstone, M.; McCready, D.R.; et al. Sentinel node biopsy after neoadjuvant chemotherapy in biopsy-proven node-positive breast cancer: The SN FNAC study. J. Clin. Oncol. 2015, 33, 258–264. [Google Scholar] [CrossRef]
- Classe, J.-M.; Loaec, C.; Gimbergues, P.; Alran, S.; de Lara, C.T.; Dupre, P.F.; Rouzier, R.; Faure, C.; Paillocher, N.; Chauvet, M.P.; et al. Sentinel lymph node biopsy without axillary lymphadenectomy after neoadjuvant chemotherapy is accurate and safe for selected patients: The GANEA 2 study. Breast Cancer Res. Treat. 2019, 173, 343–352. [Google Scholar] [CrossRef]
- Goyal, A.; Newcombe, R.G.; Chhabra, A.; E Mansel, R.; on behalf of the ALMANAC Trialists Group. Factors affecting failed localisation and false-negative rates of sentinel node biopsy in breast cancer—Results of the ALMANAC validation phase. Breast Cancer Res. Treat. 2006, 99, 203–208. [Google Scholar] [CrossRef]
- Boughey, J.C.; Ballman, K.V.; Le-Petross, H.T.; McCall, L.M.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Feliberti, E.C.; Hunt, K.K. Identification and resection of clipped node decreases the false-negative rate of sentinel lymph node surgery in patients presenting with node-positive breast cancer (T0-T4, N1-N2) who receive neoadjuvant chemotherapy: Results from ACOSOG Z1071 (Alliance). Ann. Surg. 2016, 263, 802–807. [Google Scholar] [CrossRef] [Green Version]
- Caudle, A.S.; Yang, W.T.; Krishnamurthy, S.; Mittendorf, E.A.; Black, D.M.; Gilcrease, M.Z.; Bedrosian, I.; Hobbs, B.P.; DeSnyder, S.M.; Hwang, R.F.; et al. Improved axillary evaluation following neoadjuvant therapy for patients with node-positive breast cancer using selective evaluation of clipped nodes: Implementation of targeted axillary dissection. J. Clin. Oncol. 2016, 34, 1072–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, N.; Moon, W.K.; Han, W.; Park, I.A.; Cho, J.; Noh, D.-Y. Preoperative sonographic classification of axillary lymph nodes in patients with breast cancer: Node-to-node correlation with surgical histology and sentinel node biopsy results. Am. J. Roentgenol. 2009, 193, 1731–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trinh, L.; Miyake, K.K.; Dirbas, F.M.; Kothary, N.; Horst, K.C.; Lipson, J.A.; Carpenter, C.; Thompson, A.C.; Ikeda, D.M. CT-Guided wire localization for involved axillary lymph nodes after neo-adjuvant chemotherapy in patients with initially node-positive breast cancer. Breast J. 2016, 22, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Siso, C.; De Torres, J.; Esgueva-Colmenarejo, A.; Espinosa-Bravo, M.; Rus, N.; Cordoba, O.; Rodriguez, R.; Peg, V.; Rubio, I.T. Intraoperative ultrasound-guided excision of axillary clip in patients with node-positive breast cancer treated with neoadjuvant therapy (ILINA trial): A new tool to guide the excision of the clipped node after neoadjuvant treatment. Ann. Surg. Oncol. 2018, 25, 784–791. [Google Scholar] [CrossRef]
- Kim, W.H.; Kim, H.J.; Kim, S.H.; Jung, J.H.; Park, H.Y.; Lee, J.; Kim, W.W.; Park, J.Y.; Chae, Y.S.; Lee, S.J. Ultrasound-guided dual-localization for axillary nodes before and after neoadjuvant chemotherapy with clip and activated charcoal in breast cancer patients: A feasibility study. BMC Cancer 2019, 19, 859. [Google Scholar] [CrossRef] [Green Version]
- Choy, N.; Lipson, J.; Porter, C.; Ozawa, M.; Kieryn, A.; Pal, S.; Kao, J.; Trinh, L.; Wheeler, A.; Ikeda, D.; et al. Initial results with preoperative tattooing of biopsied axillary lymph nodes and correlation to sentinel lymph nodes in breast cancer patients. Ann. Surg. Oncol. 2015, 22, 377–382. [Google Scholar] [CrossRef]
- Greenwood, H.I.; Wong, J.M.; Mukhtar, R.A.; Alvarado, M.D.; Price, E.R. Feasibility of magnetic seeds for preoperative localization of axillary lymph nodes in breast cancer treatment. Am. J. Roentgenol. 2019, 213, 953–957. [Google Scholar] [CrossRef]
- Cox, C.E.; Russell, S.; Prowler, V.; Carter, E.; Beard, A.; Mehindru, A.; Blumencranz, P.; Allen, K.; Portillo, M.; Whitworth, P.; et al. A Prospective, single arm, multi-site, clinical evaluation of a nonradioactive surgical guidance technology for the location of nonpalpable breast lesions during excision. Ann. Surg. Oncol. 2016, 23, 3168–3174. [Google Scholar] [CrossRef]
- Caudle, A.S.; Yang, W.T.; Mittendorf, E.A.; Black, D.M.; Hwang, R.; Hobbs, B.; Hunt, K.K.; Krishnamurthy, S.; Kuerer, H.M. Selective surgical localization of axillary lymph nodes containing metastases in patients with breast cancer: A prospective feasibility trial. JAMA Surg 2015, 150, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Donker, M.; Straver, M.E.; Wesseling, J.; Loo, C.E.; Schot, M.; Drukker, C.A.; Tinteren, H.; Sonke, G.S.; Rutgers, E.J.; Peeters, M.J.T.V. Marking axillary lymph nodes with radioactive iodine seeds for axillary staging after neoadjuvant systemic treatment in breast cancer patients: The MARI procedure. Ann. Surg. 2015, 261, 378–382. [Google Scholar] [CrossRef] [Green Version]
- Kern, K.A. Sentinel lymph node mapping in breast cancer using subareolar injection of blue dye. J. Am. Coll. Surg. 1999, 189, 539–545. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Hellingman, D.; Donswijk, M.; Winter-Warnars, G.A.O.; De Koekkoek-Doll, P.; Pinas, M.; Namen, Y.B.-V.; Westerga, J.; Peeters, M.-J.T.F.D.V.; Kimmings, N.; Stokkel, M.P.M. Feasibility of radioguided occult lesion localization of clip-marked lymph nodes for tailored axillary treatment in breast cancer patients treated with neoadjuvant systemic therapy. EJNMMI Res. 2019, 9, 94. [Google Scholar] [CrossRef]
- Pinkney, D.M.; Mychajlowycz, M.; A Shah, B. A prospective comparative study to evaluate the displacement of four commercially available breast biopsy markers. Br. J. Radiol. 2016, 89, 20160149. [Google Scholar] [CrossRef] [Green Version]
- Lim, G.H.; Teo, S.Y.; Gudi, M.; Ng, R.P.; Pang, J.; Tan, Y.S.; Lee, Y.S.; Allen, J.C.; Leong, L.C.H. Initial results of a novel technique of clipped node localization in breast cancer patients postneoadjuvant chemotherapy: Skin Mark clipped Axillary nodes Removal Technique (SMART trial). Cancer Med. 2020, 9, 1978–1985. [Google Scholar] [CrossRef] [Green Version]
- Porpiglia, M.; Borella, F.; Chieppa, P.; Brino, C.; Ala, A.; Marra, V.; Castellano, I.; Benedetto, C. Carbon tattooing of axillary lymph nodes in breast cancer patients before neoadjuvant chemotherapy: A retrospective analysis. Tumori J. 2022. [Google Scholar] [CrossRef]
- Pilewskie, M.; Morrow, M. Axillary nodal management following neoadjuvant chemotherapy: A review. JAMA Oncol. 2017, 3, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Kuemmel, S.; Heil, J.; Rueland, A.; Seiberling, C.; Harrach, H.; Schindowski, D.; Lubitz, J.; Hellerhoff, K.; Ankel, C.; Graßhoff, S.-T.; et al. A prospective, multicenter registry study to evaluate the clinical feasibility of targeted axillary dissection (TAD) in node-positive breast cancer patients. Ann. Surg. 2022, 276, e553–e562. [Google Scholar] [CrossRef]
- Simons, J.M.; van Nijnatten, T.J.A.; van der Pol, C.C.; van Diest, P.J.; Jager, A.; van Klaveren, D.; Kam, B.L.R.; Lobbes, M.B.I.; de Boer, M.; Verhoef, C.; et al. Diagnostic accuracy of radioactive iodine seed placement in the axilla with sentinel lymph node biopsy after neoadjuvant chemotherapy in node-positive breast cancer. JAMA Surg. 2022, 157, 991–999. [Google Scholar] [CrossRef]
- Kedrzycki, M.S.; Leiloglou, M.; Ashrafian, H.; Jiwa, N.; Thiruchelvam, P.T.R.; Elson, D.S.; Leff, D.R. Meta-analysis Comparing Fluorescence Imaging with Radioisotope and Blue Dye-Guided Sentinel Node Identification for Breast Cancer Surgery. Ann. Surg. Oncol. 2021, 28, 3738–3748. [Google Scholar] [CrossRef] [PubMed]
- Almhanedi, H.; McGurk, M.; Wan, S.; Schilling, C. Novel double injection technique for sentinel lymph node biopsy in oral cancer. Br. J. Oral Maxillofac. Surg. 2021, 59, 1296–1301. [Google Scholar] [CrossRef] [PubMed]
- Mamounas, E.P.; Brown, A.; Anderson, S.; Smith, R.; Julian, T.; Miller, B.; Bear, H.D.; Caldwell, C.B.; Walker, A.P.; Mikkelson, W.M.; et al. Sentinel node biopsy after neoadjuvant chemotherapy in breast cancer: Results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J. Clin. Oncol. 2005, 23, 2694–2702, Erratum in J. Clin. Oncol. 2005, 23, 4808. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.; Weaver, O.; Wei, W.; Caudle, A.S.; Kuerer, H.M.; Yang, W.T. Sonographic features of benign and malignant axillary nodes post-neoadjuvant chemotherapy. Breast J. 2020, 26, 182–187. [Google Scholar] [CrossRef]
- Boughey, J.C.; Ballman, K.V.; Hunt, K.K.; McCall, L.M.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Le-Petross, H.T. Axillary ultrasound after neoadjuvant chemotherapy and its impact on sentinel lymph node surgery: Results from the American College of Surgeons Oncology Group Z1071 trial (Alliance). J. Clin. Oncol. 2015, 33, 3386–3393. [Google Scholar] [CrossRef] [Green Version]
- Galimberti, V.; Fontana, S.K.R.; Vicini, E.; Morigi, C.; Sargenti, M.; Corso, G.; Magnoni, F.; Intra, M.; Veronesi, P. This house believes that: Sentinel node biopsy alone is better than TAD after NACT for cN+ patients. Breast 2023, 67, 21–25. [Google Scholar] [CrossRef]
- Banys-Paluchowski, M.; Gasparri, M.L.; de Boniface, J.; Gentilini, O.; Stickeler, E.; Hartmann, S.; Thill, M.; Rubio, I.T.; Di Micco, R.; Bonci, E.-A.; et al. Surgical management of the axilla in clinically node-positive breast cancer patients converting to clinical node negativity through neoadjuvant chemotherapy: Current status, knowledge gaps, and rationale for the EUBREAST-03 AXSANA Study. Cancers 2021, 13, 1565. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N° of Patients | 72 |
| Mean age, years | 51.4 (28–76) |
| Largest tumor diameter on MRI (mm) | 38.3 (12–93) |
| Histologic finding | |
| Invasive ductal carcinoma | 58/72 (80.6%) |
| Invasive lobular carcinoma | 9/72 (12.5%) |
| Other invasive carcinoma | 5/72 (6.9%) |
| Stage at diagnosis | |
| II | 34/72 (47.2%) |
| III | 38/72 (72.8%) |
| IV | 0/72 (0.0%) |
| Phenotype | |
| HR-negative/HER2-negative | 17/72 (23.6%) |
| HR-positive/HER2-positive | 12/72 (16.7%) |
| HR-negative/HER2-positive | 8/72 (11.1%) |
| HR-positive/HER2-positive | 35/72 (48.6%) |
| Histologic grade | |
| Grade I | 3/72 (4.2%) |
| Grade II | 30/72 (41.7%) |
| Grade III | 39/72 (54.1%) |
| Type of surgery | |
| Breast-conserving surgery | 39/72 (54.2%) |
| Mastectomy | 33/72 (45.8%) |
| Neoadjuvant chemotherapy regimen | |
| Anthracycline plus taxane | 26/72 (36.1%) |
| Anthracycline plus taxane plus anti-HER2 | 43/72 (59.7%) |
| Endocrine therapy | 3/72 (4.2%) |
| Identification Technique | Identified | Not Identified | Detection Rate (%) |
|---|---|---|---|
| Blue-dye | 66 | 6 | 91.7 |
| ROLL | 70 | 2 | 97.2 |
| Blue dye + ROLL | 71 | 1 | 98.6 |
| ALND Outcome | |||
|---|---|---|---|
| Residual Disease (n = 32) | No Residual Disease (n = 28) | False Negative Rate (%) | |
| SLN | |||
| Positive | 25 | 0 | |
| Negative | 6 | 24 | |
| Not colored | 1 | 4 | |
| 6/31 (19.35%) | |||
| CLN | |||
| Positive | 31 | 0 | |
| Negative | 1 | 26 | |
| Not identified by ROLL | 0 | 2 | |
| 1/32 (3.13%) | |||
| SNL and CLN | |||
| SLN-positive/CLN-positive | 25 | 0 | |
| SLN-negative/CLN-positive | 5 | 0 | |
| SLN-positive/CLN-negative | 0 | 0 | |
| SLN-negative/CLN-negative | 1 | 22 | |
| SLN not colored/CLN-positive | 1 | 0 | |
| SLN not colored/CLN negative | 0 | 4 | |
| SLN-negative/CLN not identified | 0 | 1 | |
| SLN not colored/CLN not identified | 0 | 1 | |
| 1/32 (3.13%) | |||
| Number of Abnormal Nodes on Initial Staging by US | ||||||
| <4 Abnormal Nodes | ≥4 Abnormal Nodes | |||||
| ALND Outcome | ALND Outcome | |||||
| Residual Disease | No Residual Disease | FNR (%) | Residual Disease | No Residual Disease | FNR (%) | |
| Outcome CLN | ||||||
| Positive | 16 | 0 | 15 | 0 | ||
| Negative | 1 | 18 | 0 | 10 | ||
| 1/17 (5.88%) | 0/15 (0%) | |||||
| Outcome SLNs | ||||||
| Positive | 11 | 0 | 14 | 0 | ||
| Negative | 5 | 17 | 1 | 7 | ||
| Not identified | 1 | 1 | 0 | 3 | ||
| 5/16 (31.25%) | 1/15 (6.67%) | |||||
| Ultrasound Evaluation after NACT | ||||||
| Normal Lymph Node Status | Suspicious Nodal Status | |||||
| Outcome ALND | Outcome ALND | |||||
| Residual Disease | No Residual Disease | FNR (%) | Residual Disease | No Residual Disease | FNR (%) | |
| Outcome CLN | ||||||
| Positive | 10 | 0 | 21 | 0 | ||
| Negative | 1 | 24 | 0 | 4 | ||
| 1/11 (9.09%) | 0/21 (0%) | |||||
| Outcome SLNs | ||||||
| Positive | 7 | 0 | 18 | 0 | ||
| Negative | 3 | 21 | 3 | 3 | ||
| Not identified | 1 | 3 | 0 | 1 | ||
| 3/10 (30.0%) | 3/21 (14.29%) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rella, R.; Conti, M.; Bufi, E.; Trombadori, C.M.L.; Di Leone, A.; Terribile, D.; Masetti, R.; Zagaria, L.; Mulè, A.; Morciano, F.; et al. Selective Axillary Dissection after Neoadjuvant Chemotherapy in Patients with Lymph-Node-Positive Breast Cancer (CLYP Study): The Radio-Guided Occult Lesion Localization Technique for Biopsy-Proven Metastatic Lymph Nodes. Cancers 2023, 15, 2046. https://doi.org/10.3390/cancers15072046
Rella R, Conti M, Bufi E, Trombadori CML, Di Leone A, Terribile D, Masetti R, Zagaria L, Mulè A, Morciano F, et al. Selective Axillary Dissection after Neoadjuvant Chemotherapy in Patients with Lymph-Node-Positive Breast Cancer (CLYP Study): The Radio-Guided Occult Lesion Localization Technique for Biopsy-Proven Metastatic Lymph Nodes. Cancers. 2023; 15(7):2046. https://doi.org/10.3390/cancers15072046
Chicago/Turabian StyleRella, Rossella, Marco Conti, Enida Bufi, Charlotte Marguerite Lucille Trombadori, Alba Di Leone, Daniela Terribile, Riccardo Masetti, Luca Zagaria, Antonino Mulè, Francesca Morciano, and et al. 2023. "Selective Axillary Dissection after Neoadjuvant Chemotherapy in Patients with Lymph-Node-Positive Breast Cancer (CLYP Study): The Radio-Guided Occult Lesion Localization Technique for Biopsy-Proven Metastatic Lymph Nodes" Cancers 15, no. 7: 2046. https://doi.org/10.3390/cancers15072046